Workaholism, Intensive Smartphone Use, and the Sleep-Wake Cycle: A Multiple Mediation Analysis

 , ,
, ,
Abstract
:1. Introduction
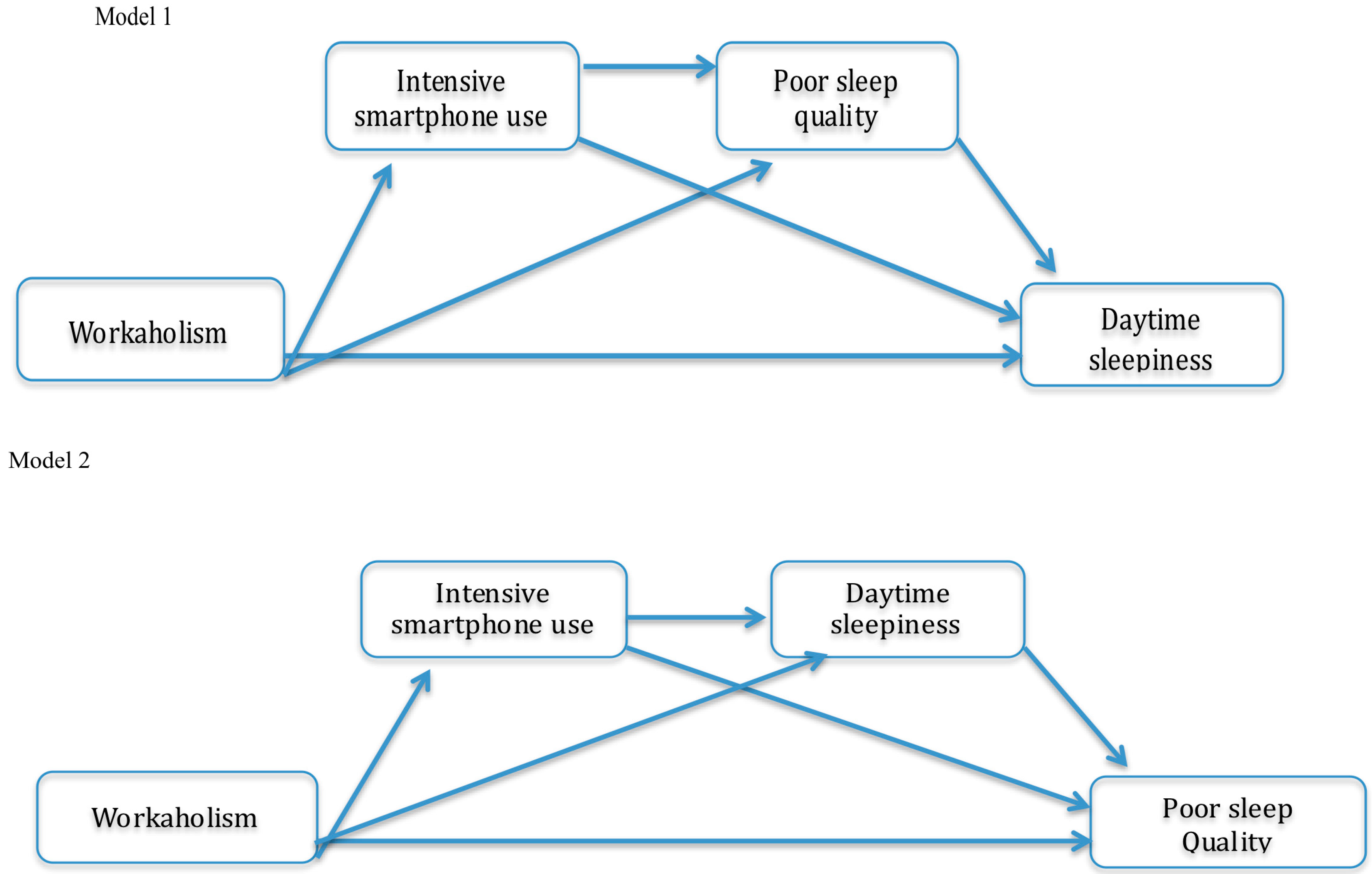
The Mediating Role of Intensive Smartphone Use in the Workaholism–Sleep/Wake Cycle Relationship
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. Workaholism
2.3.2. Intensive Smartphone Use
2.3.3. Sleep-Wake Cycle
2.3.4. Workload
2.4. Statistical Analysis
2.5. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Andreassen, C.S.; Griffiths, M.D.; Hetland, J.; Kravina, L.; Jensen, F.; Pallesen, S. The Prevalence of Workaholism: A Survey Study in a Nationally Representative Sample of Norwegian Employees. PLoS ONE 2014, 9, e102446. [Google Scholar] [CrossRef] [PubMed]
- Balducci, C.; Avanzi, L.; Fraccaroli, F. The individual “costs” of workaholism: An analysis based on multisource and prospective data. J. Manag. 2018, 44, 2961–2986. [Google Scholar] [CrossRef]
- Snir, R.; Harpaz, I. Beyond workaholism: Towards a general model of heavy work investment. Hum. Resour. Manage. Rev. 2012, 22, 232–243. [Google Scholar] [CrossRef]
- Oates, W. Confessions of a Workaholic: The Facts about Work Addiction; World Publishing Company: New York, NY, USA, 1971. [Google Scholar]
- Schaufeli, W.B.; Taris, T.W.; Van Rhenen, W. Workaholism, burnout, and work engagement: Three of a kind or three different kinds of employee well-being? Appl. Psychol. 2008, 57, 173–203. [Google Scholar] [CrossRef]
- Hakanen, J.J.; Peeters, M.C.W.; Schaufeli, W.B. Different types of employee well-being across time and their relationships with job crafting. J. Occup. Health Psych. 2018, 23, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Gillet, N.; Morin, A.J.S.; Cougot, B.; Gagné, M. Workaholism Profiles: Associations with Determinants, Correlates, and Outcomes. J. Occup. Organ. Psychol. 2017, 90, 559–586. [Google Scholar] [CrossRef]
- Birkeland, I.K.; Buch, R. The dualistic model of passion for work: Discriminate and predictive validity with work engagement and workaholism. Motiv. Emot. 2015, 39, 392–408. [Google Scholar] [CrossRef]
- Andreassen, C.S.; Griffiths, M.D.; Hetland, J.; Pallesen, S. Development of a work addiction scale. Scand. J. Psychol. 2012, 53, 265–272. [Google Scholar] [CrossRef]
- Sussman, S.; Lisha, N.; Griffiths, M. Prevalence of the addictions: A problem of the majority or the minority? Eval. Health Prof. 2011, 34, 3–56. [Google Scholar] [CrossRef]
- Clark, M.A.; Michel, J.S.; Zhdanova, L.; Pui, S.Y.; Baltes, B.B. All Work and No Play? A Meta-Analytic Examination of the Correlates and Outcomes of Workaholism. J. Manag. 2016, 42, 1836–1873. [Google Scholar] [CrossRef]
- Andreassen, C.S.; Pallesen, S.; Torsheim, T. Workaholism as a Mediator between Work-Related Stressors and Health Outcomes. Int. J. Environ. Res. Public Health 2018, 15, 73. [Google Scholar] [CrossRef] [PubMed]
- Kubota, K.; Shimazu, A.; Kawakami, N.; Takahashi, M.; Nakata, A.; Schaufeli, W.B. Association between workaholism and sleep problems among hospital nurses. Ind. Health 2010, 48, 864–871. [Google Scholar] [CrossRef] [PubMed]
- Spagnoli, P.; Balducci, C.; Scafuri Kovalchuk, L.; Maiorano, F.; Buono, C. Are Engaged Workaholics Protected against Job-Related Negative Affect and Anxiety before Sleep? A Study of the Moderating Role of Gender. Int. J. Environ. Res. Public Health 2018, 15, 1996. [Google Scholar] [CrossRef] [PubMed]
- Andreassen, C.S.; Hetland, J.; Molde, H.; Pallesen, S. Workaholism and potential outcomes in well-being and health in a cross-occupational sample. Stress Health. 2010, 27, e209–e214. [Google Scholar] [CrossRef]
- Caesens, G.; Stinglhamber, F.; Luypaert, G. The impact of work engagement and workaholism on well-being: The role of work-related social support. Career Dev. Int. 2014, 19, 813–835. [Google Scholar] [CrossRef]
- Kubota, K.; Shimazu, A.; Kawakami, N.; Takahashi, M. Workaholism and sleep quality among Japanese employees: A prospective cohort study. Int. J. Behav. Med. 2014, 21, 66–76. [Google Scholar] [CrossRef] [PubMed]
- Middleton, C. Illusions of balance and control in an always-on environment: A case study of BlackBerry users. Continuum J. Media Cult. Stud. 2007, 21, 165–178. [Google Scholar] [CrossRef]
- Derks, D.; ten Brummelhuis, L.L.; Zecic, D.; Bakker, A.B. Switching on and off: Does smartphone use obstruct the possibility to engage in recovery activities? Eur. J. Work Organ. Psychol. 2014, 23, 80–90. [Google Scholar] [CrossRef]
- Rutland, J.B.; Sheets, T.; Young, T. Development of a scale to measure problem use of short message service: The SMS problem use diagnostic questionnaire. Cyberpsychol. Behav. 2007, 10, 841–843. [Google Scholar] [CrossRef] [PubMed]
- Hyun Ha, J.; Chin, B.; Park, D.H.; Ryu, S.H.; Yu, J. Characteristics of excessive cellular phone use in Korean adolescents. Cyberpsychol. Behav. 2008, 11, 783–784. [Google Scholar] [CrossRef]
- Loscalzo, Y.; Giannini, M. Clinical conceptualization of workaholism: A comprehensive model. Organ. Psychol. Rev. 2017, 7, 306–329. [Google Scholar] [CrossRef]
- Andreassen, C.S. Workaholism: An overview and current status of the research. J. Behav. Addict. 2014, 3, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meijman, T.F.; Mulder, G. Psychological Aspects of Workload—Handbook of Work and Organizational Psychology; Drenth, P.J.D., Thierry, H., Eds.; Psychology Press: Hove, UK, 1998; Volume 2: Work psychology, pp. 5–33. [Google Scholar]
- Bert, F.; Gualano, M.R.; Giacomelli, S.; Martorana, M.; Siliquini, R. Are smartphones and tablets influencing the quality of your sleep? An Italian survey. Epidemiol. Biostat. Public Health 2018, 15, e12808. [Google Scholar] [CrossRef]
- Xie, X.; Dong, Y.; Wang, J. Sleep quality as a mediator of problematic smartphone use and clinical health symptoms. J. Behav. Addict. 2018, 7, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Lanaj, K.; Johnson, R.E.; Barnes, C.M. Beginning the workday yet already depleted? Consequences of late-night smartphone use and sleep. Organ. Behav. Hum. Decis. Process. 2014, 124, 11–23. [Google Scholar] [CrossRef]
- Gradisar, M.; Wolfson, A.M.; Harvey, A.G.; Hale, L.; Rosenberg, R.; Czeisler, C.A. The Sleep and Technology Use of Americans: Findings from the National Sleep Foundation’s 2011 Sleep in America Poll. J. Clin. Sleep Med. 2013, 9, 1291–1299. [Google Scholar] [CrossRef] [PubMed]
- Chinoy, E.D.; Duffy, J.F.; Czeisler, C.A. Unrestricted evening use of light-emitting tablet computers delays self-selected bedtime and disrupts circadian timing and alertness. Physiol. Rep. 2018, 6, e13692. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Dimsdale, J.E. The effect of psychosocial stress on sleep: A review of polysomnographic evidence. Behav. Sleep Med. 2007, 5, 256–278. [Google Scholar] [CrossRef]
- Kobayashi, T.; Ishikawa, T.; Arakawa, K. Effects of daytime activity upon the timing of REM sleep periods during a night. Psychiatry Clin. Neurosci. 1998, 52, 130–131. [Google Scholar] [CrossRef]
- Achermann, P. The two-process model of sleep regulation revisited. Aviat. Space Environ. Med. 2004, 75, 37–43. [Google Scholar]
- Carney, C.E.; Edinger, J.D.; Meyer, B.; Lindman, L.; Istrie, T. Symptom-focused rumination and sleep disturbances. Behav. Sleep Med. 2006, 4, 228–241. [Google Scholar] [CrossRef] [PubMed]
- Garcia, A.N.; Salloum, I.M. Polysomnographic sleep disturbances in nicotine, caffeine, alcohol, cocaine, opioid, and cannabis use: A focused review. Am. J. Addict. 2015, 24, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T. The human sleep project. Nature 2013, 498, 427–428. [Google Scholar] [CrossRef] [PubMed]
- Nose, Y.; Fujinaga, R.; Suzuki, M.; Hayashi, I.; Moritani, T.; Kotani, K.; Nagai, N. Association of evening smartphone use with cardiac autonomic nervous activity after awakening in adolescents living in high school dormitories. Childs Nerv. Syst. 2017, 33, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Taris, T.W.; Van Beek, I.; Schaufeli, W.B. Demographic and occupational correlates of workaholism. Psychol. Rep. 2012, 110, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Balducci, C.; Avanzi, L.; Consiglio, C.; Fraccaroli, F.; Schaufeli, W. A Cross-National Study on the Psychometric Quality of the Italian Version of the Dutch Work Addiction Scale (DUWAS). Eur. J. Psychol. Assess. 2017, 33, 422–428. [Google Scholar] [CrossRef]
- Avanzi, L.; van Dick, R.; Fraccaroli, F.; Sarchielli, G. The downside of organizational identification: Relations between identification, workaholism and well-being. Work Stress 2012, 26, 289–307. [Google Scholar] [CrossRef]
- Natale, V.; Fabbri, M.; Tonetti, L.; Martoni, M. Psychometric goodness of the Mini Sleep Questionnaire. Psychiatry Clin. Neurosci. 2014, 68, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Karasek, R.; Brisson, C.; Kawakami, N.; Houtman, I.; Bongers, P.; Amick, B. The Job Content Questionnaire (JCQ): An instrument for internationally comparative assessments. J. Occup. Health Psychol. 1998, 3, 322–355. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process. Analysis: A Regression-Based Approach, 2nd ed.; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Preacher, J.K.; Hayes, F.A. SPSS and SAS Procedures for Estimating Indirect Effects in Simple Mediation Models. Behav. Res. Methods Instrum. Comp. 2004, 36, 717–731. [Google Scholar] [CrossRef]
- Borbély, A.A.; Daan, S.; Wirz-Justice, A.; Deboer, T. The two-process model of sleep regulation: A reappraisal. J. Sleep Res. 2016, 25, 131–143. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. Bull. World Health Organ. 2001, 79, 373–374. [Google Scholar]
- Cajochen, C.; Münch, M.; Kobialka, S.; Kräuchi, K.; Steiner, R.; Oelhafen, P.; Orgül, S.; Wirz-Justice, A. High sensitivity of human melatonin, alertness, thermoregulation, and heart rate to short wavelength light. J. Clin. Endocrinol. Metab. 2005, 90, 1311–1316. [Google Scholar] [CrossRef] [PubMed]
- Cajochen, C.; Frey, S.; Anders, D.; Späti, J.; Bues, M.; Pross, A.; Mager, R.; Wirz-Justice, A.; Stefani, O. Evening exposure to a light-emitting diodes (LED)-backlit computer screen affects circadian physiology and cognitive performance. J. Appl. Physiol. 2011, 110, 1432–1438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aeschbach, D.; Matthews, J.R.; Postolache, T.T.; Jackson, M.A.; Giesen, H.A.; Wehr, T.A. Dynamics of the human EEG during prolonged wakefulness: Evidence for frequency-specific circadian and homeostatic influences. Neurosci. Lett. 1997, 239, 121–124. [Google Scholar] [CrossRef]
- Barbato, G.; Ficca, G.; Muscettola, G.; Fichele, M.; Beatrice, M.; Rinaldi, F. Diurnal variation in spontaneous eye-blink rate. Psychiatry Res. 2000, 6, 145–151. [Google Scholar] [CrossRef]
- Barbato, G.; De Padova, V.; Paolillo, A.R.; Arpaia, L.; Russo, E.; Ficca, G. Increased spontaneous eye blink rate following prolonged wakefulness. Physiol. Behav. 2007, 90, 151–154. [Google Scholar] [CrossRef]
- Podsakoff, M.P.; MacKenzie, S.; Jeong-Yeon, L.; Podsakoff, P.N. Common Method Biases in Behavioral Research: A Critical Review of the Literature and Recommended Remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]
- Halbesleben, J.R.B.; Wheeler, A.R.; Buckley, M.R. Clarifying the Relationship between Organizational Commitment and Job Performance—Applied Psychology Research Trends; Kiefer, K.H., Ed.; Nova Science: New York, NY, USA, 2008. [Google Scholar]
- Smith, A. Effects of caffeine on human behavior. Food Chem. Toxicol. 2002, 40, 1243–1250. [Google Scholar] [CrossRef]
- Adan, A.; Fabbri, M.; Natale, V.; Prat, G. Sleep Beliefs Scale (SBS) and circadian typology. J. Sleep Res. 2006, 15, 125–132. [Google Scholar] [CrossRef]


{kind=link}
| Variables | M | S.D. | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Workaholism | 3.19 | 0.36 | 0.77 | ||||||
| 2. Intensive smartphone use | 3 | 1.07 | 0.24 ** | 0.76 | |||||
| 3. Poor sleep quality | 2.43 | 0.77 | 0.23 ** | 0.18 ** | 0.77 | ||||
| 4. Daytime sleepiness | 2.61 | 0.83 | 0.29 ** | 0.19 ** | 0.65 ** | 0.77 | |||
| 5. Gender # | - | - | 0.05 | −0.05 | 0.07 | 0.12 ** | - | ||
| 6. Age | 44.01 | 12.56 | −0.09 | −0.20 * | 0.10 | −0.10 | 0.04 | - | |
| 7. Workload | 3.6 | 0.70 | 0.40 ** | 0.08 | 0.08 | −0.01 | 0.02 | −0.16 | 0.66 |
| 8. Job type | - | - | 0.03 | 0.14 * | −0.06 | 0.02 | −0.30 ** | −0.27 ** | 0.11 * |
| Models | B | LLCI | ULCI | R2 |
|---|---|---|---|---|
| Model 1 a: Mediation of smartphone use in the relationship between workaholism and poor sleep quality | ||||
| Outcome variable: Smartphone use | 0.09 * | |||
| Workaholism | 0.41 ** | 0.24 | 0.58 | |
| Covariate: Job type | 0.06 | −0.01 | 0.13 | |
| Covariate: Gender | −0.03 | −0.24 | 0.18 | |
| Covariate: Age | −0.01 | −0.02 | −0.01 | |
| Covariate: Workload | −0.06 | −0.22 | 0.09 | |
| Model 1 b: Mediation of smartphone use in the relationship between workaholism and poor sleep quality | ||||
| Outcome variable: Poor sleep quality | 0.10 ** | |||
| Workaholism | 0.30 ** | 0.18 | 0.43 | |
| Intensive smartphone use | 0.12 * | 0.05 | 0.18 | |
| Covariate: Job type | −0.02 | −0.70 | 0.03 | |
| Covariate: Gender | 0.25 * | 0.06 | 0.44 | |
| Covariate: Age | 0.01 | −0.002 | 0.01 | |
| Covariate: Workload | −0.001 | −0.14 | 0.14 | |
| Model 1 c: Mediation of smartphone use in the relationship between workaholism and daytime sleepiness | ||||
| Outcome variable: Daytime sleepiness | 0.47 ** | |||
| Workaholism | 0.41 | 0.27 | 0.54 | |
| Intensive smartphone use | 0.02 | −0.04 | 0.07 | |
| Poor sleep quality | 0.67 ** | 0.59 | 0.75 | |
| Covariate: Job type | 0.02 | −0.01 | 0.06 | |
| Covariate: Gender | 0.17 | 0.04 | 0.29 | |
| Covariate: Age | −0.01 | −0.01 | −0.01 | |
| Covariate: Workload | −0.01 | −0.09 | 0.09 | |
| Indirect effects | ||||
| Workaholism-intensive smartphone use-daytime sleepiness | −0.01 | −0.01 | 0.03 | |
| Workaholism-poor sleep quality-daytime sleepiness | 0.2 | 0.12 | 0.3 | |
| Workaholism-intensive smartphone use-poor sleep quality-daytime sleepiness | 0.03 | 0.01 | 0.06 | |
| Total effect | 0.4 | 0 | 0.27 |
| Models | B | LLCI | ULCI | R2 |
|---|---|---|---|---|
| Model 2 a: Mediation of smartphone use in the relationship between workaholism and daytime sleepiness | ||||
| Outcome variable: Smartphone use | 0.09 * | |||
| Workaholism | 0.41 ** | 0.24 | 0.58 | |
| Covariate: Job type | 0.06 | −0.01 | 0.14 | |
| Covariate: Gender | 0.03 | −0.25 | 0.18 | |
| Covariate: Age | −0.01 | −0.02 | 0.01 | |
| Covariate: Workload | −0.06 | −0.22 | 0.08 | |
| Model 2 b: Mediation of smartphone use in the relationship between workaholism and daytime sleepiness | ||||
| Outcome variable: Daytime sleepiness | 0.12 ** | |||
| Workaholism | 0.36 ** | 0.23 | 0.5 | |
| Intensive smartphone use | 0.10 * | 0.02 | 0.37 | |
| Covariate: Job type | 0.01 | −0.04 | 0.06 | |
| Covariate: Gender | 0.21 * | 0.04 | 0.37 | |
| Covariate: Age | −0.01 | −0.01 | 0.01 | |
| Covariate: Workload | −0.08 | −0.20 | 0.03 | |
| Model 2 c: Mediation of smartphone use in the relationship between workaholism and poor sleep quality | ||||
| Outcome variable: Poor sleep quality | 0.46 ** | |||
| Workaholism | 0.09 | −0.01 | 0.18 | |
| Intensive smartphone use | 0.06 | 0.01 | 0.11 | |
| Daytime sleepiness | 0.59 ** | 0.52 | 0.66 | |
| Covariate: Job type | −0.02 | −0.06 | 0.01 | |
| Covariate: Gender | −0.06 | −0.18 | 0.05 | |
| Covariate: Age | 0.01 | 0.01 | 0.01 | |
| Covariate: Workload | −0.06 | −0.14 | 0.02 | |
| Indirect effects | ||||
| Workaholism-intensive smartphone use-poor sleep quality | 0.01 | −0.01 | 0.05 | |
| Workaholism-daytime sleepiness-poor sleep quality | 0.22 | 0.13 | 0.31 | |
| Workaholism-intensive smartphone use-daytime sleepiness-poor sleep quality | 0.02 | 0.01 | 0.05 | |
| Total effect | 0.34 | 0.22 | 0.46 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spagnoli, P.; Balducci, C.; Fabbri, M.; Molinaro, D.; Barbato, G. Workaholism, Intensive Smartphone Use, and the Sleep-Wake Cycle: A Multiple Mediation Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3517. https://doi.org/10.3390/ijerph16193517
Spagnoli P, Balducci C, Fabbri M, Molinaro D, Barbato G. Workaholism, Intensive Smartphone Use, and the Sleep-Wake Cycle: A Multiple Mediation Analysis. International Journal of Environmental Research and Public Health. 2019; 16(19):3517. https://doi.org/10.3390/ijerph16193517
Chicago/Turabian StyleSpagnoli, Paola, Cristian Balducci, Marco Fabbri, Danila Molinaro, and Giuseppe Barbato. 2019. "Workaholism, Intensive Smartphone Use, and the Sleep-Wake Cycle: A Multiple Mediation Analysis" International Journal of Environmental Research and Public Health 16, no. 19: 3517. https://doi.org/10.3390/ijerph16193517