Characteristics and Trends of Pneumoconiosis in the Jiangsu Province, China, 2006–2017

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sources of Data
2.2. Definition
2.3. Statistical Analysis
3. Results
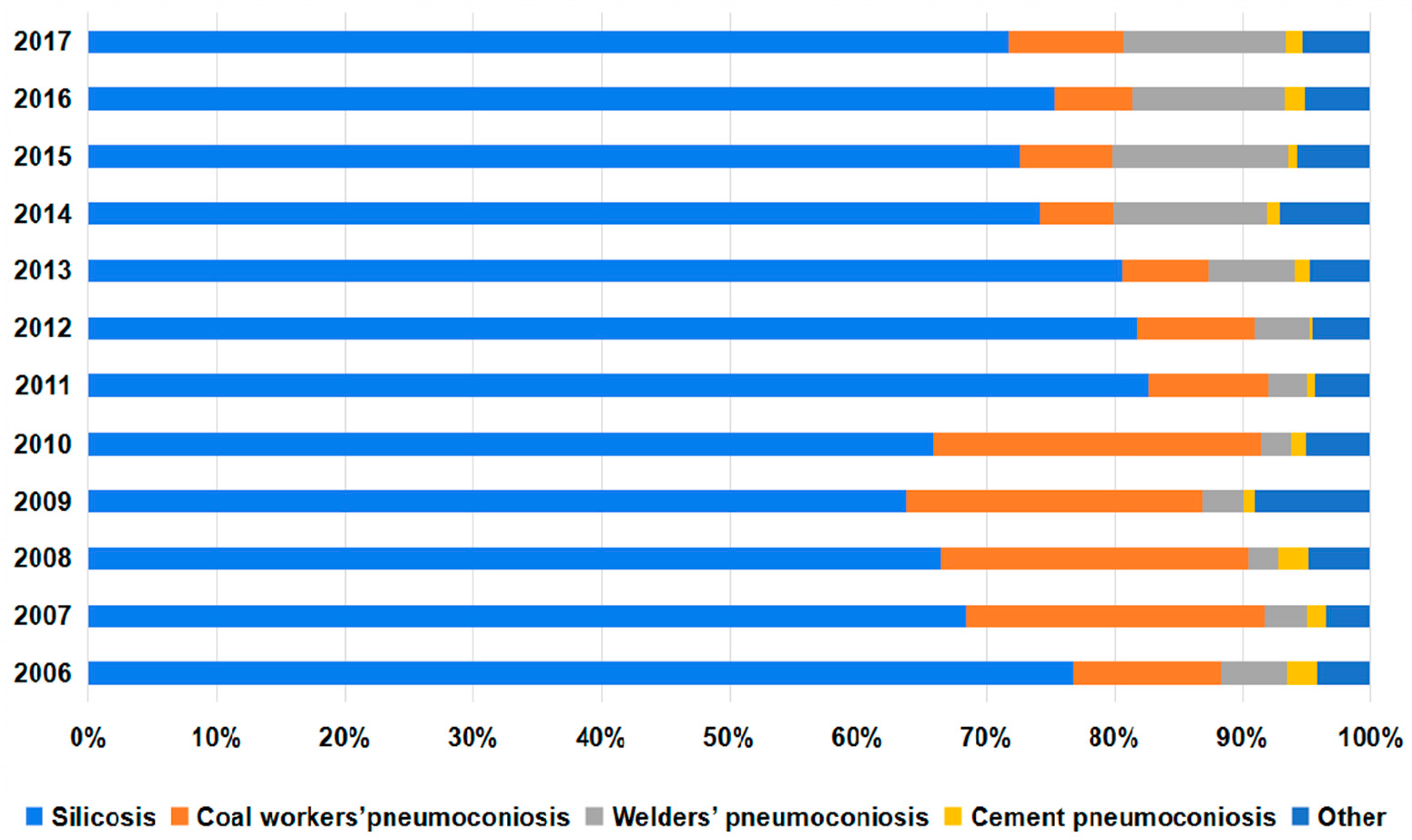
3.1. Changes in the Number of Pneumoconiosis Cases Reported from 2006 to 2017
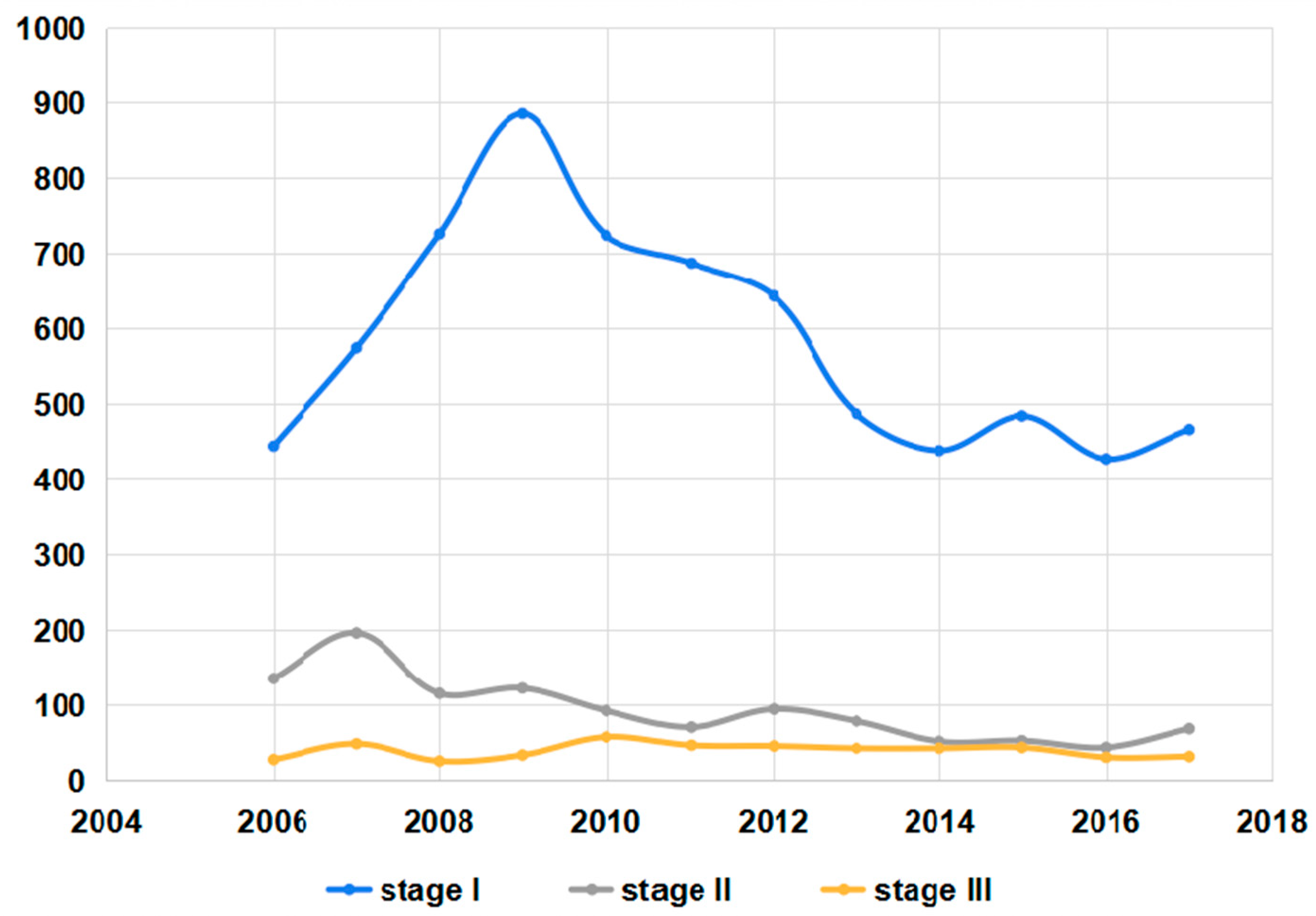
3.2. Changes in the Stages of Pneumoconiosis Cases Reported from 2006 to 2017
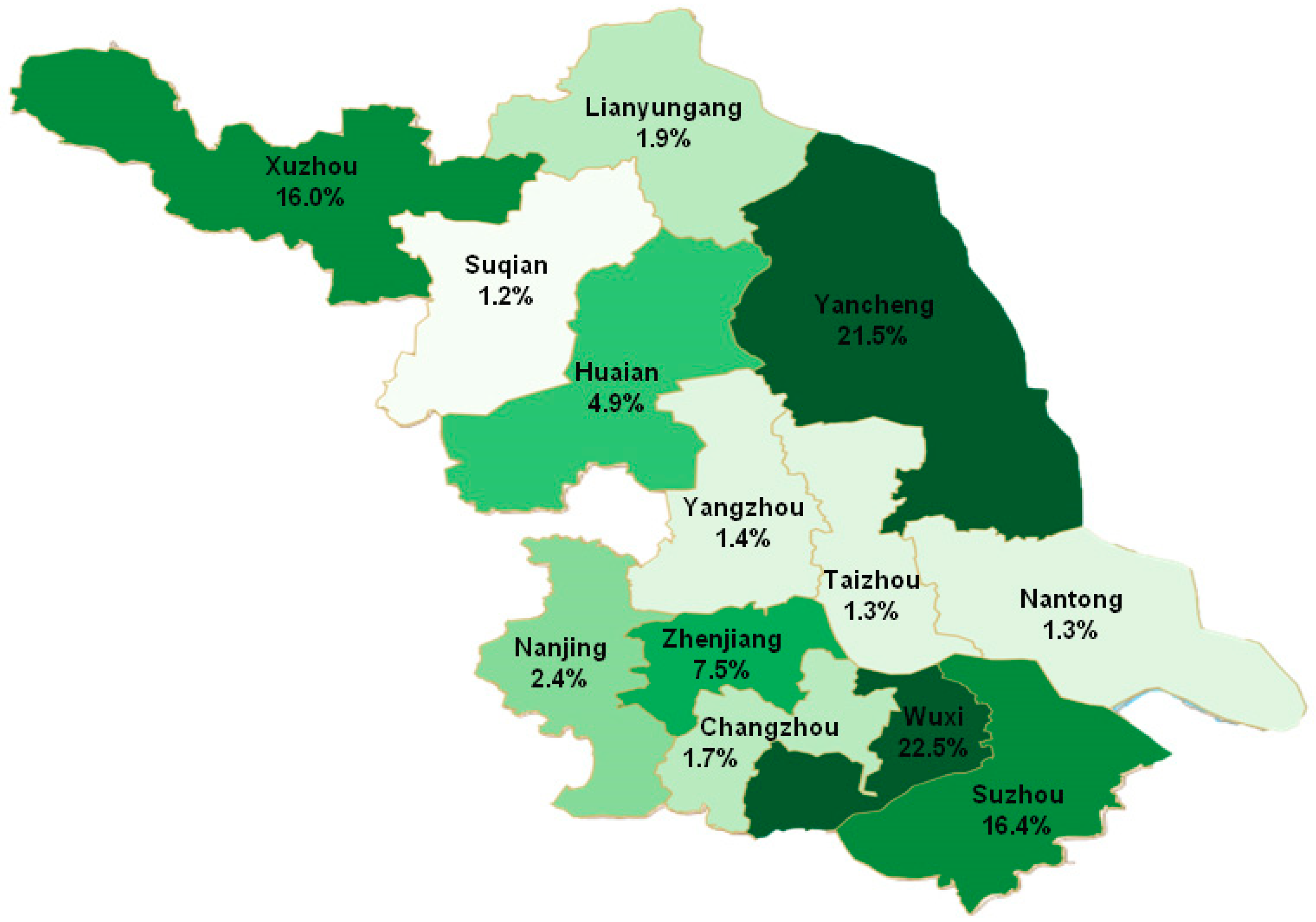
3.3. Regional Distribution of Pneumoconiosis Cases Reported from 2006 to 2017
3.4. Enterprise Ownership Type and Scale Distribution of Pneumoconiosis Cases Reported from 2006 to 2017
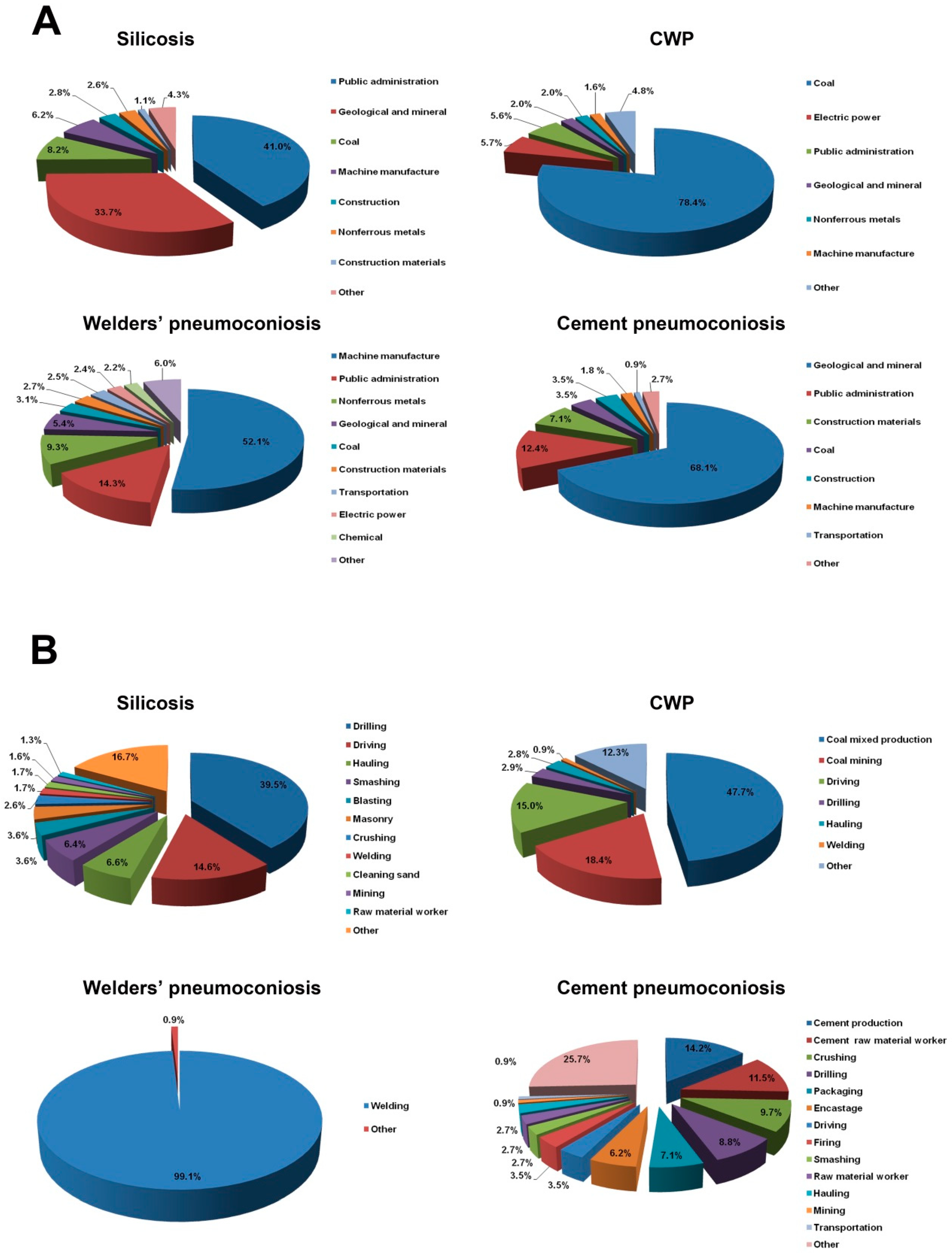
3.5. Industry and Occupation Distribution of Pneumoconiosis Cases Reported from 2006 to 2017
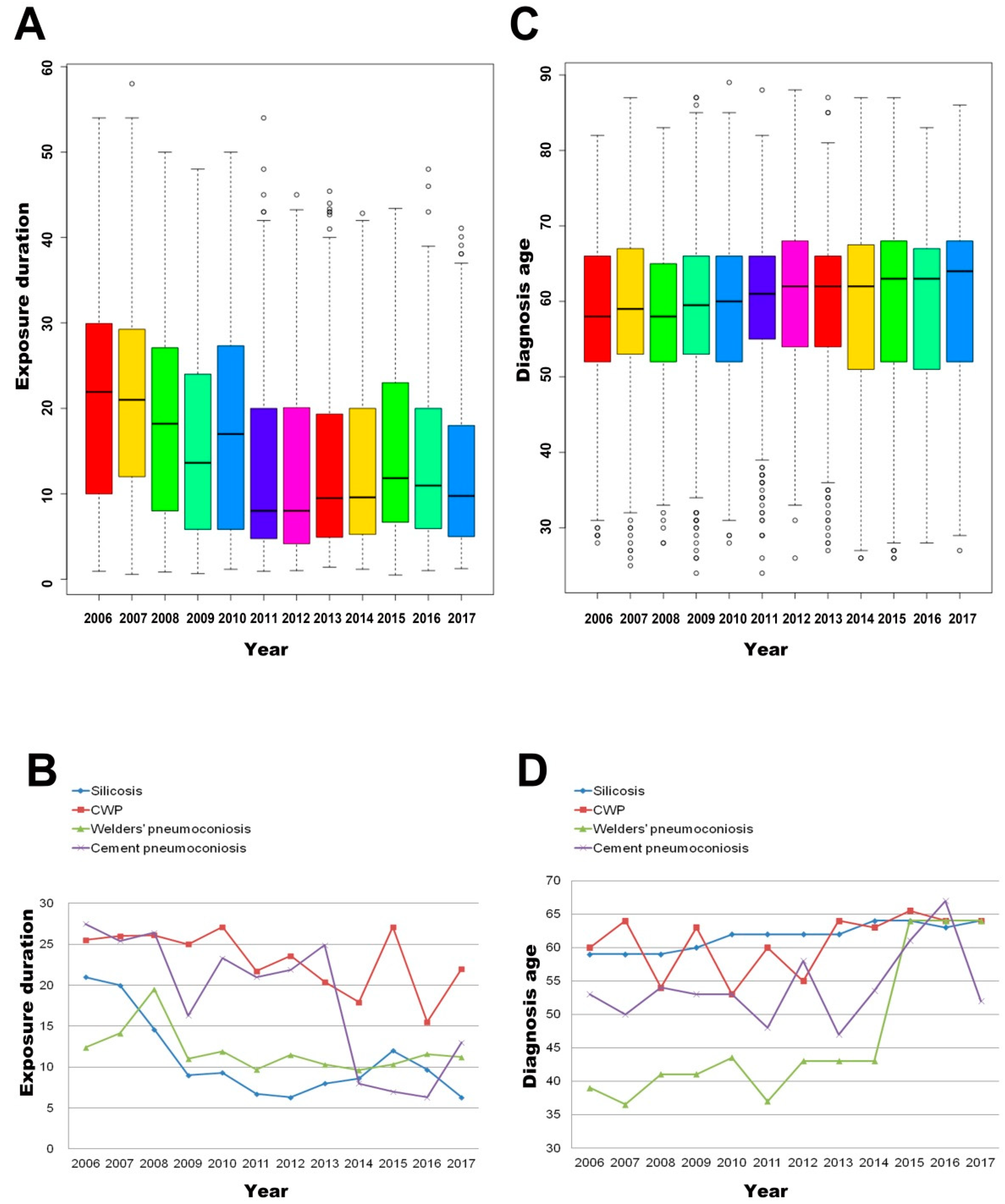
3.6. The Overall Annual Trend of the Average Exposure Duration and Diagnosis Age of Pneumoconiosis Cases from 2006 to 2017
4. Discussion
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Fourth International Pneumoconiosis Conference. Report of the Working Party on the Definition of Pneumoconiosis; International Labour Organization: Geneva, Switzerland, 1971. [Google Scholar]
- Pascolo, L.; Borelli, V.; Canzonieri, V.; Gianoncelli, A.; Birarda, G.; Bedolla, D.E.; Salomé, M.; Vaccari, L.; Calligaro, C.; Cotte, M.; et al. Differential protein folding and chemical changes in lung tissues exposed to asbestos or particulates. Sci. Rep. 2015, 5, 12129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Laney, A.S.; Weissman, D.N. The classic pneumoconioses: New epidemiological and laboratory observations. Clin. Chest Med. 2012, 33, 745–758. [Google Scholar] [CrossRef] [PubMed]
- Choi, B.S.; Park, S.Y.; Lee, J.O. Current status of pneumoconiosis patients in Korea. J. Korean Med. Sci. 2010, 25, S13–S19. [Google Scholar] [CrossRef] [PubMed]
- Nelson, G. Occupational respiratory diseases in the South African mining industry. Glob. Health Action 2013, 6, 19520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Global Occupational Health Network Newsletter: Elimination of Silicosis. Available online: http://www.who.int/occupational_health/publications/newsletter/gohnet12e.pdf (accessed on 18 June 2018).
- McNamee, R.; Carder, M.; Chen, Y.; Agius, R. Measurement of trends in incidence of work-related skin and respiratory diseases, UK 1996–2005. Occup. Environ. Med. 2008, 65, 808–814. [Google Scholar] [CrossRef] [PubMed]
- Scarselli, A.; Binazzi, A.; Marinaccio, A. Occupational exposure to crystalline silica: Estimating the number of workers potentially at high risk in Italy. Am. J. Ind. Med. 2008, 51, 941–949. [Google Scholar] [CrossRef]
- Antao, V.C.; Pinheiro, G.A.; Kavakama, J.; Terra-Filho, M. High prevalence of silicosis among stone carvers in Brazil. Am. J. Ind. Med. 2004, 45, 194–201. [Google Scholar] [CrossRef]
- Jp, N.A.; Imanaka, M.; Suganuma, N. Japanese Workplace Health Management in Pneumoconiosis Prevention. J. Occup. Health 2017, 59, 91–103. [Google Scholar] [CrossRef]
- WHO. Hazard Prevention and Control in the Work Environment: Airborne Dust. Available online: http://www.who.int/occupational_health/publications/airdust/en/ (accessed on 8 August 2018).
- Zhang, M.; Wang, D.; Zheng, Y.D.; Du, X.Y.; Chen, S.Y. Analyses on the characteristics and the trends of pneumoconiosis notified between 1997 and 2009, in China. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi 2013, 31, 321–334. [Google Scholar]
- Ding, B.M.; Zhou, P.; Xie, L.Z. Characteristics of occurrence of pneumoconiosis in Jiangsu Province between 2006 and 2007. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi 2009, 27, 36–37. [Google Scholar] [PubMed]
- Wang, D.; Zhang, M. Statistics on notification of pneumoconiosis in China in 2010. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi 2012, 30, 801–810. [Google Scholar] [PubMed]
- Graber, J.M.; Cohen, R.A.; Basanets, A.; Stayner, L.T.; Kundiev, Y.; Conroy, L.; Mukhin, V.V.; Lysenko, O.; Zvinchuk, A.; Hryhorczuk, D.O. Results from a Ukrainian-US collaborative study: Prevalence and predictors of respiratory symptoms among Ukrainian coal miners. Am. J. Ind. Med. 2012, 55, 1099–1109. [Google Scholar] [CrossRef] [PubMed]
- Mo, J.; Wang, L.; Au, W.; Su, M. Prevalence of coal workers’ pneumoconiosis in China: A systematic analysis of 2001-2011 studies. Int. J. Hyg. Environ. Health 2014, 217, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, S.; Levenstein, C.; Nelson, D.I.; Rosenberg, B.J. The cost effectiveness of occupational health interventions: Prevention of silicosis. Am. J. Ind. Med. 2005, 48, 503–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, Y.X.; Wong, O.; Fu, H.; Hu, T.X.; Xue, S.Z. The economic burden of pneumoconiosis in China. Occup. Environ. Med. 2003, 60, 383–384. [Google Scholar] [CrossRef] [Green Version]
- Han, L. Trend of Dust Pollution, Prevalence Characteristics and Prediction of Coal Workers’ Pneumoconiosis in a Mine in Eastern China. Ph.D. Thesis, Nanjing Medical University, Nanjing, China, 2015. [Google Scholar]
- Wang, B.H.; Cong, S.; Bao, H.L.; Feng, Y.J.; Fan, J.; Wang, N.; Fang, L.W.; Wang, L.H. Analysis on occupational exposure to dust and harmful gas and corresponding protection in adults aged 40 years and older in China, 2014. Zhonghua Liu Xing Bing Xue Za Zhi 2018, 39, 563–568. [Google Scholar]
- Xia, Y.; Liu, J.; Shi, T.; Xiang, H.; Bi, Y. Prevalence of pneumoconiosis in Hubei, China from 2008 to 2013. Int. J. Environ. Res. Public Health 2014, 11, 8612–8621. [Google Scholar] [CrossRef]
- Song, Z.F.; Qian, H.Y.; Wang, S.S.; Jia, X.M.; Ye, Y.; Ni, C.H. Analysis on the incidence of coal workers’ pneumoconiosis from 2003 to 2008 in a coal mining group. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi 2011, 29, 56–58. [Google Scholar]
- Zhang, M.; Zheng, Y.D.; Du, X.Y.; Lu, Y.; Li, W.J.; Qi, C.; Wu, Z.L. Silicosis in automobile foundry workers: A 29-year cohort study. Biomed. Environ. Sci. 2010, 23, 121–129. [Google Scholar] [CrossRef]
- Xiao, G.B.; Morinaga, K.; Wang, R.Y.; Xu, L.R.; Ma, Z.H.; Zhang, X.; Kishimoto, T.; Kohyama, N. Lung disorders of workers exposed to rush smear dust in China. Ind. Health 2006, 44, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Page, S.J. Comparison of coal mine dust size distributions and calibration standards for crystalline silica analysis. AIHA J. 2003, 64, 30–39. [Google Scholar] [CrossRef]
- Filios, M.S.; Mazurek, J.M.; Schleiff, P.L.; Reilly, M.J.; Rosenman, K.D.; Lumia, M.E.; Worthington, K. Summary of Notifiable Noninfectious Conditions and Disease Outbreaks: Surveillance for Silicosis—Michigan and New Jersey, 2003–2010. MMWR Morb. Mortal. Wkly. Rep. 2015, 62, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Zhang, M.; Zheng, Y.D. Study of estimation method for incidence of new cases of coal workers’ pneumoconiosis in China. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi 2013, 31, 24–29. [Google Scholar] [PubMed]
- Fernandez Alvarez, R.; Martinez Gonzalez, C.; Quero Martinez, A.; Blanco Perez, J.J.; Carazo Fernandez, L.; Prieto Fernandez, A. Guidelines for the diagnosis and monitoring of silicosis. Arch. Bronconeumol. 2015, 51, 86–93. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Silicosis | Coal Workers’ Pneumoconiosis | Welders’ Pneumoconiosis | Cement Pneumoconiosis | Other | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % |
| 1461 | 21.7 | 198 | 14.6 | 214 | 38.8 | 7 | 6.2 | 196 | 40.2 | 2076 | 22.5 |
| 1783 | 26.5 | 93 | 6.8 | 51 | 9.3 | 21 | 18.6 | 42 | 8.6 | 1990 | 21.5 |
| 1402 | 20.8 | 13 | 1.0 | 35 | 6.4 | 6 | 5.3 | 56 | 11.5 | 1512 | 16.4 |
| 604 | 9.0 | 814 | 59.9 | 39 | 7.1 | 8 | 7.1 | 17 | 3.5 | 1482 | 16.0 |
| 446 | 6.6 | 104 | 7.7 | 48 | 8.7 | 54 | 47.8 | 41 | 8.4 | 693 | 7.5 |
| 343 | 5.1 | 44 | 3.2 | 29 | 5.3 | 10 | 8.8 | 31 | 6.4 | 457 | 4.9 |
| 145 | 2.2 | 28 | 2.1 | 24 | 4.4 | 4 | 3.5 | 17 | 3.5 | 218 | 2.4 |
| 142 | 2.1 | 9 | 0.7 | 5 | 0.9 | 1 | 0.9 | 15 | 3.1 | 172 | 1.9 |
| 128 | 1.9 | 9 | 0.7 | 15 | 2.7 | 0 | 0.0 | 9 | 1.8 | 161 | 1.7 |
| 41 | 0.6 | 28 | 2.1 | 44 | 8.0 | 1 | 0.9 | 16 | 3.3 | 130 | 1.4 |
| 76 | 1.1 | 5 | 0.4 | 19 | 3.4 | 0 | 0.0 | 24 | 4.9 | 124 | 1.3 |
| 65 | 1.0 | 9 | 0.7 | 25 | 4.5 | 1 | 0.9 | 21 | 4.3 | 121 | 1.3 |
| 96 | 1.4 | 5 | 0.4 | 3 | 0.5 | 0 | 0.0 | 3 | 0.6 | 107 | 1.2 |
| Enterprise Ownership | Silicosis | Coal Workers’ Pneumoconiosis | Welders’ Pneumoconiosis | Cement Pneumoconiosis | Other | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | |
| State-owned | 3757 | 55.8 | 1260 | 92.7 | 170 | 30.9 | 34 | 30.1 | 175 | 35.9 | 5396 | 58.4 |
| Collective | 2037 | 30.3 | 34 | 2.5 | 36 | 6.5 | 7 | 6.2 | 86 | 17.6 | 2200 | 23.8 |
| Private | 841 | 12.5 | 40 | 2.9 | 310 | 56.3 | 29 | 25.7 | 193 | 39.5 | 1413 | 15.3 |
| Foreign | 48 | 0.7 | 21 | 1.5 | 30 | 5.4 | 36 | 31.9 | 25 | 5.1 | 160 | 1.7 |
| Hong Kong, Macao and Taiwan | 19 | 0.3 | 0 | 0.0 | 3 | 0.5 | 2 | 1.8 | 2 | 0.4 | 26 | 0.3 |
| Other types | 30 | 0.4 | 4 | 0.3 | 2 | 0.4 | 5 | 4.4 | 7 | 1.4 | 48 | 0.5 |
| Enterprise Size | Silicosis | Coal Workers’ Pneumoconiosis | Welders’ Pneumoconiosis | Cement Pneumoconiosis | Other | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | |
| Large | 749 | 11.1 | 896 | 65.9 | 64 | 11.6 | 7 | 6.2 | 43 | 8.8 | 1759 | 19.0 |
| Medium | 490 | 7.3 | 261 | 19.2 | 141 | 25.6 | 60 | 53.1 | 79 | 16.2 | 1031 | 11.2 |
| Small | 3577 | 53.1 | 98 | 7.2 | 269 | 48.8 | 23 | 20.4 | 197 | 40.4 | 4164 | 45.1 |
| Micro | 367 | 5.5 | 18 | 1.3 | 35 | 6.4 | 9 | 8.0 | 24 | 4.9 | 453 | 4.9 |
| Unknown | 1549 | 23.0 | 86 | 6.3 | 42 | 7.6 | 14 | 12.4 | 145 | 29.7 | 1836 | 19.9 |
| Year | n | Mean (SD) | Range | Median | Quantile |
|---|---|---|---|---|---|
| 2006 | 685 | 20.7 (11.6) | 0.9–54.0 | 21.9 | (10.0, 29.9) |
| 2007 | 904 | 20.9 (11.0) | 0.6–58.0 | 21.0 | (12.0, 29.3) |
| 2008 | 802 | 18.3 (10.8) | 0.8–50.0 | 18.2 | (8.0, 27.1) |
| 2009 | 842 | 15.3 (10.3) | 0.7–48.0 | 13.6 | (5.8, 24.0) |
| 2010 | 1201 | 17.1 (11.1) | 1.2–50.0 | 17.0 | (5.8, 27.3) |
| 2011 | 841 | 12.8 (10.2) | 0.9–54.0 | 8.0 | (4.8, 20.0) |
| 2012 | 874 | 12.7 (10.4) | 1.0–45.0 | 8.0 | (4.2, 20.1) |
| 2013 | 670 | 12.9 (9.8) | 1.4–45.4 | 9.5 | (4.9, 19.3) |
| 2014 | 603 | 13.3 (9.7) | 1.2–42.8 | 9.6 | (5.3, 20.0) |
| 2015 | 665 | 15.1 (10.0) | 0.5–43.4 | 11.8 | (6.7, 23.0) |
| 2016 | 500 | 13.5 (9.6) | 1.0–48.0 | 11.0 | (5.9, 20.0) |
| 2017 | 656 | 12.4 (9.1) | 1.3–41.1 | 9.8 | (5.0, 18.0) |
| Total | 9243 | 15.7 (10.8) | 0.5–58.0 | 13.2 | (0.5, 58.0) |
| Year | n | Mean (SD) | Range | Median | Quantile |
|---|---|---|---|---|---|
| 2006 | 685 | 58.2 (10.7) | 28–82 | 58 | (52, 66) |
| 2007 | 904 | 59.0 (10.7) | 25–87 | 59 | (53, 67) |
| 2008 | 802 | 57.7 (10.1) | 28-83 | 58 | (52, 65) |
| 2009 | 842 | 59.0 (10.5) | 24–87 | 60 | (53, 66) |
| 2010 | 1201 | 58.8 (10.3) | 28–89 | 60 | (52, 66) |
| 2011 | 841 | 60.1 (9.9) | 24–88 | 61 | (55, 66) |
| 2012 | 874 | 60.7 (10.4) | 26–88 | 62 | (54, 68) |
| 2013 | 670 | 59.9 (10.5) | 27-87 | 62 | (54, 66) |
| 2014 | 603 | 59.5 (11.6) | 26–87 | 62 | (51, 67.5) |
| 2015 | 665 | 60.4 (11.7) | 26–87 | 63 | (52, 68) |
| 2016 | 500 | 60.4 (10.9) | 28–83 | 63 | (51, 67) |
| 2017 | 656 | 60.7 (11.0) | 27–86 | 64 | (52, 68) |
| Total | 9243 | 59.4 (10.7) | 24–89 | 61 | (53, 67) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, L.; Yao, W.; Bian, Z.; Zhao, Y.; Zhang, H.; Ding, B.; Shen, H.; Li, P.; Zhu, B.; Ni, C. Characteristics and Trends of Pneumoconiosis in the Jiangsu Province, China, 2006–2017. Int. J. Environ. Res. Public Health 2019, 16, 437. https://doi.org/10.3390/ijerph16030437
Han L, Yao W, Bian Z, Zhao Y, Zhang H, Ding B, Shen H, Li P, Zhu B, Ni C. Characteristics and Trends of Pneumoconiosis in the Jiangsu Province, China, 2006–2017. International Journal of Environmental Research and Public Health. 2019; 16(3):437. https://doi.org/10.3390/ijerph16030437
Chicago/Turabian StyleHan, Lei, Wenxi Yao, Zilong Bian, Yuan Zhao, Hengdong Zhang, Bangmei Ding, Han Shen, Ping Li, Baoli Zhu, and Chunhui Ni. 2019. "Characteristics and Trends of Pneumoconiosis in the Jiangsu Province, China, 2006–2017" International Journal of Environmental Research and Public Health 16, no. 3: 437. https://doi.org/10.3390/ijerph16030437