Household Air Pollution, Levels of Micronutrients and Heavy Metals in Cord and Maternal Blood, and Pregnancy Outcomes

 and
and
Abstract
:1. Introduction
2. Materials and Methods
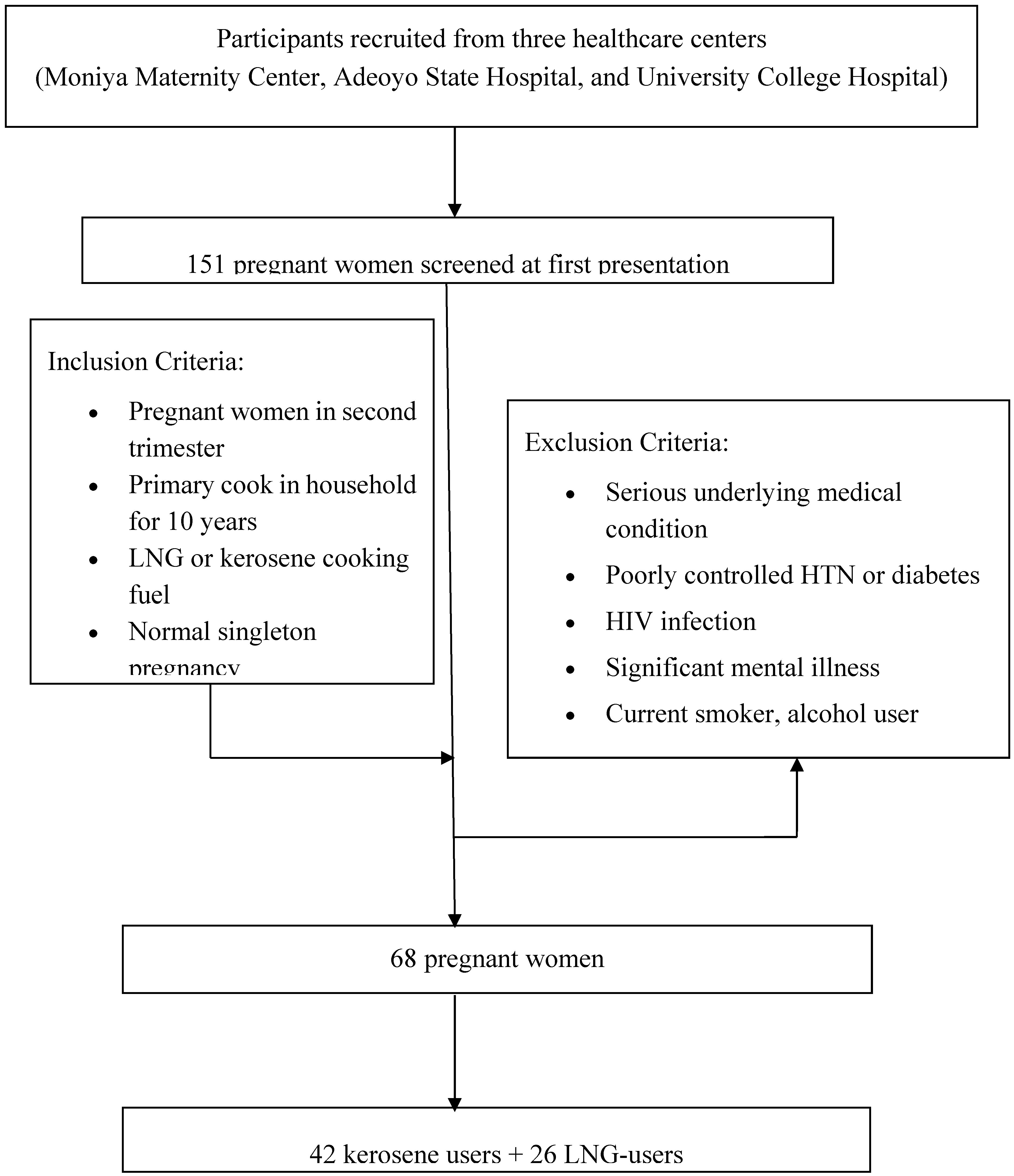
2.1. Study Design, Study Site, and Recruitment of Subjects
2.2. Blood Sample Collection and Analysis
2.3. Data Analysis
3. Results
3.1. Socio-Demographic Characteristics
3.2. Pregnancy Outcomes
3.3. Levels of Micronutrients and Heavy Metals
3.4. Correlation between Maternal and Fetal Micronutrients Levels
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Lam, N.L.; Smith, K.R.; Gauthier, A.; Bates, M.N. Kerosene: A review of household uses and their hazards in low- and middle-income countries. J. Toxicol. Environ. Health 2012, 15, 396–432. [Google Scholar] [CrossRef] [PubMed]
- Mills, N.L.; Tornqvist, H.; Robinson, S.D.; Gonzalez, M.; Darnley, K.; MacNee, W.; Boon, N.A.; Donaldson, K.; Blomberg, A.; Sandstrom, T.; et al. Diesel exhaust inhalation causes vascular dysfunction and impaired endogenous fibrinolysis. Circulation 2005, 112, 3930–3936. [Google Scholar] [CrossRef]
- Ibitoye, F.I. The millennium development goals and household energy requirements in Nigeria. SpringerPlus 2013, 2, 529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akpoveta, O.V. OSA: Determination of Heavy Metal Contents in Refined Petroleum Products. IOSR J. Appl. Chem. 2014, 7, 1–2. [Google Scholar]
- Nagar, J.K.R.; Shrivastava, J.P. Association of heavy metals composition of particulate matter with environmental tobacco smoke and cooking fuels in indoor air of Delhi. Int. J. Sci. Nat. 2014, 5, 547–552. [Google Scholar]
- Kim, O.; le Nghiem, H.; Phyu, Y.L. Emission of polycyclic aromatic hydrocarbons, toxicity, and mutagenicity from domestic cooking using sawdust briquettes, wood, and kerosene. Environ. Sci. Technol. 2002, 36, 833–839. [Google Scholar] [PubMed]
- Raiyani, C.V.; Jani, J.P.; Desai, N.M.; Shah, S.H.; Shah, P.G.; Kashyap, S.K. Assessment of indoor exposure to polycyclic aromatic hydrocarbons for urban poor using various types of cooking fuels. Bull. Environ. Contam. Toxicol. 1993, 50, 757–763. [Google Scholar] [CrossRef]
- Kandpal, J.B.M.R.; Kandpal, T.C. Indoor air pollution from domestic cookstoves using coal, kerosene and LPG. Energy Convers. Manag. 1995, 36, 1067–1072. [Google Scholar] [CrossRef]
- Olopade, C.O.; Frank, E.; Bartlett, E.; Alexander, D.; Dutta, A.; Ibigbami, T.; Adu, D.; Olamijulo, J.; Arinola, G.; Karrison, T.; et al. Effect of a clean stove intervention on inflammatory biomarkers in pregnant women in Ibadan, Nigeria: A randomized controlled study. Environ. Int. 2017, 98, 181–190. [Google Scholar] [CrossRef]
- Nadeau, K.; McDonald-Hyman, C.; Noth, E.M.; Pratt, B.; Hammond, S.K.; Balmes, J.; Tager, I. Ambient air pollution impairs regulatory T-cell function in asthma. J. Allergy Clin. Immunol. 2010, 126, 845–852. [Google Scholar] [CrossRef]
- Ukaejiofo, E.O. Biochemical and haematological assessment of workers exposed to some petroleum products in Enugu Urban, Enugu State, Nigeria. Niger. J. Med. 2006, 15, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Neeti, K.P.T. Effects of Heavy Metal Poisoning during Pregnancy. Int. Res. J. Environ. Sci. 2013, 2, 88–92. [Google Scholar]
- Oluwole, O.; Arinola, G.O.; Ana, G.R.; Wiskel, T.; Huo, D.; Olopade, O.I.; Olopade, C.O. Relationship between household air pollution from biomass smoke exposure, and pulmonary dysfunction, oxidant-antioxidant imbalance and systemic inflammation in rural women and children in Nigeria. Glob. J. Health Sci. 2013, 5, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Squadrito, G.L.; Cueto, R.; Dellinger, B.; Pryor, W.A. Quinoid redox cycling as a mechanism for sustained free radical generation by inhaled airborne particulate matter. Free Radic. Biol. Med. 2001, 31, 1132–1138. [Google Scholar] [CrossRef]
- Ohyama, M.; Otake, T.; Adachi, S.; Kobayashi, T.; Morinaga, K. A comparison of the production of reactive oxygen species by suspended particulate matter and diesel exhaust particles with macrophages. Inhal. Toxicol. 2007, 9, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Edem, V.F.; Ige, O.; Arinola, O.G. Plasma vitamins and essential trace elements in newly diagnosed pulmonary tuberculosis patients and at different durations of anti-tuberculosis chemotherapy. Egypt. J. Chest Dis. Tubercul. 2015, 64, 675–679. [Google Scholar] [CrossRef]
- Arinola, G.O.; Morenikeji, O.A.; Akinwande, K.S.; Alade, A.O.; Olateru-Olagbegi, O.; Alabi, P.E.; Rahamon, S.K. Serum Levels of Cytokines and IgE in Helminth-Infected Nigerian Pregnant Women and Children. Ann. Glob. Health 2015, 81, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, A.R.; Gold, E.B.; Yang, X.; Lee, K.; Brown, K.H.; Bhutta, Z.A. Prenatal exposure to wood fuel smoke and low birth weight. Environ. Health Perspect. 2008, 116, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Abusalah, A.; Gavana, M.; Haidich, A.B.; Smyrnakis, E.; Papadakis, N.; Papanikolaou, A.; Benos, A. Low birth weight and prenatal exposure to indoor pollution from tobacco smoke and wood fuel smoke: A matched case-control study in Gaza Strip. Matern. Child Health J. 2012, 16, 1718–1727. [Google Scholar] [CrossRef] [PubMed]
- Amegah, A.K.; Quansah, R.; Jaakkola, J.J.K. Household Air Pollution from Solid Fuel Use and Risk of Adverse Pregnancy Outcomes: A Systematic Review and Meta-Analysis of the Empirical Evidence. PLoS ONE 2014, 9, e13920. [Google Scholar] [CrossRef]
- Rehfuess, E.; WHO. Fuel for Life: Household Energy and Health; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Lakshmi, P.V.; Virdi, N.K.; Sharma, A.; Tripathy, J.P.; Smith, K.R.; Bates, M.N.; Kumar, R. Household air pollution and stillbirths in India: Analysis of the DLHS-II National Survey. Environ. Res. 2013, 121, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Epstein, M.B.; Bates, M.N.; Arora, N.K.; Balakrishnan, K.; Jack, D.W.; Smith, K.R. Household fuels, low birth weight, and neonatal death in India: The separate impacts of biomass, kerosene, and coal. Int. J. Hyg. Environ. Health 2013, 216, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Alexander, D.; Northcross, A.; Wilson, N.; Dutta, A.; Pandya, R.; Ibigbami, T.; Adu, D.; Olamijulo, J.; Morhason-Bello, O.; Karrison, T.; et al. Randomized Controlled Ethanol Cookstove Intervention and Blood Pressure in Pregnant Nigerian Women. Am. J. Respir. Crit. Care Med. 2017, 195, 1629–1639. [Google Scholar] [CrossRef] [PubMed]
- Alexander, D.A.; Northcross, A.; Karrison, T.; Morhasson-Bello, O.; Wilson, N.; Atalabi, O.M.; Dutta, A.; Adu, D.; Ibigbami, T.; Olamijulo, J.; et al. Pregnancy outcomes and ethanol cook stove intervention: A randomized-controlled trial in Ibadan, Nigeria. Environ. Int. 2017, 111, 152–163. [Google Scholar] [CrossRef] [PubMed]
- Fenech, M. The role of folic acid and Vitamin B12 in genomic stability of human cells. Mutat. Res. 2001, 475, 57–67. [Google Scholar] [CrossRef]
- Perng, W.; Villamor, E.; Shroff, M.R.; Nettleton, J.A.; Pilsner, J.R.; Liu, Y.; Diez-Roux, A.V. Dietary intake, plasma homocysteine, and repetitive element DNA methylation in the Multi-Ethnic Study of Atherosclerosis (MESA). Nutr. Metab. Cardiovasc. Dis. 2014, 24, 614–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EL-Safty, I.A.; Gadallah, M.; Shafik, A.; Shouman, A.E. Effect of mercury vapour exposure on urinary excretion of calcium, zinc and copper: Relationship to alterations in functional and structural integrity of the kidney. Toxicol. Ind. Health 2002, 18, 377–388. [Google Scholar] [CrossRef]
- Xu, L.; Deng, H.; Xia, J.; Li, H.; Zhou, J.; Wang, D.; Pan, Q.; Long, Z. Identification of mutation in a candidate gene for hereditary multiple exostoses type II. Chin. Med. J. 1999, 112, 72–75. [Google Scholar]
- Crider, K.S.; Yang, T.P.; Berry, R.J.; Bailey, L.B. Folate and DNA methylation: A review of molecular mechanisms and the evidence for folate’s role. Adv. Nutr. 2012, 3, 21–38. [Google Scholar] [CrossRef]
- Baker, P.N.; Wheeler, S.J.; Sanders, T.A.; Thomas, J.E.; Hutchinson, C.J.; Clarke, K.; Berry, J.L.; Jones, R.L.; Seed, P.T.; Poston, L. A prospective study of micronutrient status in adolescent pregnancy. Am. J. Clin. Nutr. 2009, 89, 1114–1124. [Google Scholar] [CrossRef] [Green Version]
- Hininger, I.; Chollat-Namy, A.; Sauvaigo, S.; Osman, M.; Faure, H.; Cadet, J.; Favier, A.; Roussel, A.M. Assessment of DNA damage by comet assay on frozen total blood: Method and evaluation in smokers and non-smokers. Mutat. Res. 2004, 558, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Sengupta, B.; Paladhi, P.K.R. Single megadose vitamin A supplementation of Indian mothers and morbidity in breastfed young infants. Postgrad. Med. J. 2003, 79, 397–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christian, P.; Khatry, S.K.; Katz, J.; Pradhan, E.K.; LeClerq, S.C.; Shrestha, S.R.; Adhikari, R.K.; Sommer, A.; West, K.P., Jr. Effects of alternative maternal micronutrient supplements on low birth weight in rural Nepal: Double blind randomised community trial. BMJ 2003, 326, 571. [Google Scholar] [CrossRef] [PubMed]
- Dejmek, J.; Solansk, Y.I.; Podrazilova, K.; Sram, R.J. The exposure of nonsmoking and smoking mothers to environmental tobacco smoke during different gestational phases and fetal growth. Environ. Health Perspect. 2002, 110, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Kancherla, V.; Oakley, G.P., Jr.; Brent, R.L. Urgent global opportunities to prevent birth defects. Semin. Fetal Neonatal Med. 2014, 19, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roohani, N.; Hurrell, R.; Kelishadi, R.; Schulin, R. Zinc and its importance for human health: An integrative review. J. Res. Med. Sci. 2013, 18, 144–157. [Google Scholar] [PubMed]
- Liu, L.; Wylie, R.C.; Andrews, L.G.; Tollefsbol, T.O. Aging, cancer and nutrition: The DNA methylation connection. Mech. Ageing Dev. 2003, 124, 989–998. [Google Scholar] [CrossRef]
- Smulders, Y.M.; Smith, D.E.; Kok, R.M.; Teerlink, T.; Swinkels, D.W.; Stehouwer, C.D.; Jakobs, C. Cellular folate vitamer distribution during and after correction of vitamin B12 deficiency: A case for the methylfolate trap. Br. J. Haematol. 2006, 132, 623–629. [Google Scholar] [CrossRef]
- Toole, J.F.; Malinow, M.R.; Chambless, L.E.; Spence, J.D.; Pettigrew, L.C.; Howard, V.J.; Sides, E.G.; Wang, C.H.; Stampfer, M. Lowering homocysteine in patients with ischemic stroke to prevent recurrent stroke, myocardial infarction, and death: The Vitamin Intervention for Stroke Prevention (VISP) randomized controlled trial. JAMA 2004, 291, 565–575. [Google Scholar] [CrossRef]
- Nelen, W.L.; Blom, H.J.; Steegers, E.A.; den Heijer, M.; Thomas, C.M.; Eskes, T.K. Homocysteine and folate levels as risk factors for recurrent early pregnancy loss. Obstet. Gynecol. 2000, 95, 519–524. [Google Scholar]
- Van der Put, N.M.; van Straaten, H.W.; Trijbels, F.J.; Blom, H.J. Folate, homocysteine and neural tube defects: An overview. Exp. Biol. Med. 2001, 226, 243–270. [Google Scholar] [CrossRef]
- WHO. Indoor Air Pollution: National Burden of Disease Estimates; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Bates, M.N.; Chandyo, R.K.; Valentiner-Branth, P.; Pokhrel, A.K.; Mathisen, M.; Basnet, S.; Shrestha, P.S.; Strand, T.A.; Smith, K.R. Acute lower respiratory infection in childhood and household fuel use in Bhaktapur, Nepal. Environ. Health Perspect. 2013, 121, 637–642. [Google Scholar] [CrossRef] [PubMed]
- Moshammer, H.; Fletcher, T.; Heinrich, J.; Hoek, G.; Hruba, F.; Pattenden, S.; Rudnai, P.; Slachtova, H.; Speizer, F.E.; Zlotkowska, R.; et al. Gas cooking is associated with small reductions in lung function in children. Eur. Respir. J. 2010, 36, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Bates, M.N.; Pokhrel, A.K.; Chandyo, R.K.; Valentiner-Branth, P.; Mathisen, M.; Basnet, S.; Strand, T.A.; Burnett, R.T.; Smith, K.R. Kitchen PM2.5 concentrations and child acute lower respiratory infection in Bhaktapur, Nepal: The importance of fuel type. Environ. Res. 2018, 161, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Willers, S.M.; Brunekreef, B.; Oldenwening, M.; Smit, H.A.; Kerkhof, M.; De Vries, H.; Gerritsen, J.; De Jongste, J.C. Gas cooking, kitchen ventilation, and asthma, allergic symptoms and sensitization in young children—The PIAMA study. Allergy 2006, 61, 563–568. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Guidelines for Indoor Air Quality Guidelines: Household Fuel Combustion; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Oluwole, O.; Ana, G.R.; Arinola, G.O.; Wiskel, T.; Falusi, A.G.; Huo, D.; Olopade, O.I.; Olopade, C.O. Effect of stove intervention on household air pollution and the respiratory health of women and children in rural Nigeria. Air Qual. Atmos. Health 2013, 6, 553–561. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Kerosene Users (N = 42) | LNG Users (N = 26) | p-Value |
|---|---|---|---|
| Age, years (mean (SD)) | 29.48 (4.54) | 28.42 (5.33) | 0.391 |
| Parity (mean (SD)) | 3.24 (1.74) | 2.50 (2.14) | 0.123 |
| Multivitamins use during pregnancy (%) | 4.8 | 3.8 | 0.862 |
| Daily vegetable consumption during pregnancy (%) | 66.7 | 61.5 | 0.674 |
| Passive cigarette smokers (%) | 4.8 | 19.2 | 0.056 |
| Family income per year | |||
| Low (<N250,000) (%) | 78.6 | 30.8 | <0.001 * |
| Medium (≥N250,000 and <N500,000) (%) | 14.3 | 3.8 | - |
| High (≥N500,000) (%) | 7.1 | 65.4 | - |
| Education above high school (%) | 14.3 | 46.2 | 0.001 * |
| Number of children | |||
| 1–2 (%) | 11.9 | 52.0 | <0.001 * |
| 3–4 (%) | 45.2 | 40.0 | - |
| >4 (%) | 42.9 | 8.0 | - |
| Married (%) | 61.9 | 65.4 | 0.768 |
| Modern homes (%) | 52.1 | 45.9 | 0.153 |
| Pregnancy Outcomes | Kerosene Users (N = 42) | LNG Users (N = 26) | p-Value |
|---|---|---|---|
| Gestational Age, weeks (mean (SD)) | 35.46 (3.05) | 34.98 (3.12) | 0.532 |
| Birth weight, kg (mean (SD)) | 3.02 (0.43) | 3.43 (0.32) | <0.001 |
| Head circumference, cm (mean (SD)) | 35.14 (3.20) | 35.54 (3.89) | 0.655 |
| Chest circumference, cm (mean (SD)) | 35.26 (3.58) | 34.46 (3.14) | 0.354 |
| CTH length, cm (mean (SD)) | 46.43 (3.89) | 45.23 (4.02) | 0.232 |
| Placenta weight, kg (mean (SD)) | 0.82 (0.09) | 0.77 (0.13) | 0.082 |
| Heavy Metals and Micronutrients | Kerosene Users (N = 42) | LNG Users (N = 26) | p-Value |
|---|---|---|---|
| Maternal blood | |||
| Zinc (Zn) | 95.43 (16.06) | 77.14 (16.26) | <0.001 * |
| Lead (Pb) | 5.23 (0.94) | 4.23 (0.99) | <0.001 * |
| Mercury (Hg) | 9.88 (1.62) | 7.98 (0.93) | <0.001 * |
| Iodine (I) | 57.50 (12.02) | 48.85 (5.70) | <0.001 * |
| B6 | 8.71 (1.45) | 6.74 (0.93) | <0.001 * |
| B12 | 436.41 (86.64) | 461.74 (90.65) | 0.254 |
| Folic acid | 6.68 (1.70) | 7.59 (1.54) | 0.026 * |
| Homocysteine | 7.72 (1.17) | 6.68 (1.70) | 0.111 |
| Fetal cord blood | |||
| Zinc (Zn) | 92.78 (19.14) | 124.28 (24.90) | <0.001 * |
| Lead (Pb) | 4.45 (1.95) | 5.77 (2.25) | 0.017 |
| Mercury (Hg) | 8.32 (3.50) | 10.72 (4.00) | 0.015 |
| Iodine (I) | 49.62 (20.80) | 65.60 (19.27) | 0.002 * |
| B6 | 7.31 (2.13) | 11.23 (3.04) | <0.001 * |
| B12 | 249.95 (82.54) | 346.26 (49.90) | <0.001 * |
| Folic acid | 7.72 (2.04) | 10.93 (1.57) | <0.001 * |
| Homocysteine | 7.75 (1.36) | 10.42 (1.36) | <0.001 * |
| Heavy Metals and Micronutrients | Overall (N = 67) | Kerosene Users (N = 42) | LNG Users (N = 26) |
|---|---|---|---|
| β (SE) | β (SE) | β (SE) | |
| Zinc (Zn) | −0.002 (0.003) | 0.004 (0.004) | 0.003 (0.004) |
| Lead (Pb) | −0.159 (0.047) * | −0.030 (0.072) * | −0.185 (0.055) |
| Mercury (Hg) | −0.098 (0.030) * | −0.034 (0.042) | −0.102 (0.068) |
| Iodine (I) | −0.014 (0.005) * | −0.007 (0.006) | −0.017 (0.011) |
| B6 | −0.064 (0.033) | 0.016 (0.047) | 0.033 (0.071) |
| B12 | 0.001 (0.001) | 0.001 (0.001) | 0.000 (0.001) |
| Folic acid | 0.012 (0.032) | −0.015 (0.040) | −0.035 (0.042) |
| Homocysteine | −0.014 (0.029) | 0.009 (0.032) | −0.003 (0.056) |
| Mother/Fetal Cord | Zinc | Iodine | B6 | B12 | Folic Acid | Homocysteine |
|---|---|---|---|---|---|---|
| Zinc | −0.48 ** | −0.37 ** | −0.48 ** | −0.35 ** | −0.52 ** | −0.51 ** |
| Iodine | - | 0.02 | −0.32 ** | −0.29 ** | −0.24 ** | −0.25 * |
| B6 | - | - | −0.56 ** | −0.30 * | −0.37 | −0.56 ** |
| B12 | - | - | - | 0.21 | 0.16 | 0.04 |
| Folic acid | - | - | - | - | 0.15 | 0.14 |
| Homocysteine | - | - | - | - | - | −0.09 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arinola, G.O.; Dutta, A.; Oluwole, O.; Olopade, C.O. Household Air Pollution, Levels of Micronutrients and Heavy Metals in Cord and Maternal Blood, and Pregnancy Outcomes. Int. J. Environ. Res. Public Health 2018, 15, 2891. https://doi.org/10.3390/ijerph15122891
Arinola GO, Dutta A, Oluwole O, Olopade CO. Household Air Pollution, Levels of Micronutrients and Heavy Metals in Cord and Maternal Blood, and Pregnancy Outcomes. International Journal of Environmental Research and Public Health. 2018; 15(12):2891. https://doi.org/10.3390/ijerph15122891
Chicago/Turabian StyleArinola, Ganiyu Olatunbosun, Anindita Dutta, Oluwafemi Oluwole, and Christopher O. Olopade. 2018. "Household Air Pollution, Levels of Micronutrients and Heavy Metals in Cord and Maternal Blood, and Pregnancy Outcomes" International Journal of Environmental Research and Public Health 15, no. 12: 2891. https://doi.org/10.3390/ijerph15122891