
The Effects of Forest Therapy on Coping with Chronic Widespread Pain: Physiological and Psychological Differences between Participants in a Forest Therapy Program and a Control Group

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Design
2.2. Experimental Treatment
2.3. Physiological Indices
2.4. Psychological Indices
2.5. Procedure
2.6. Statistical Analyses
3. Results
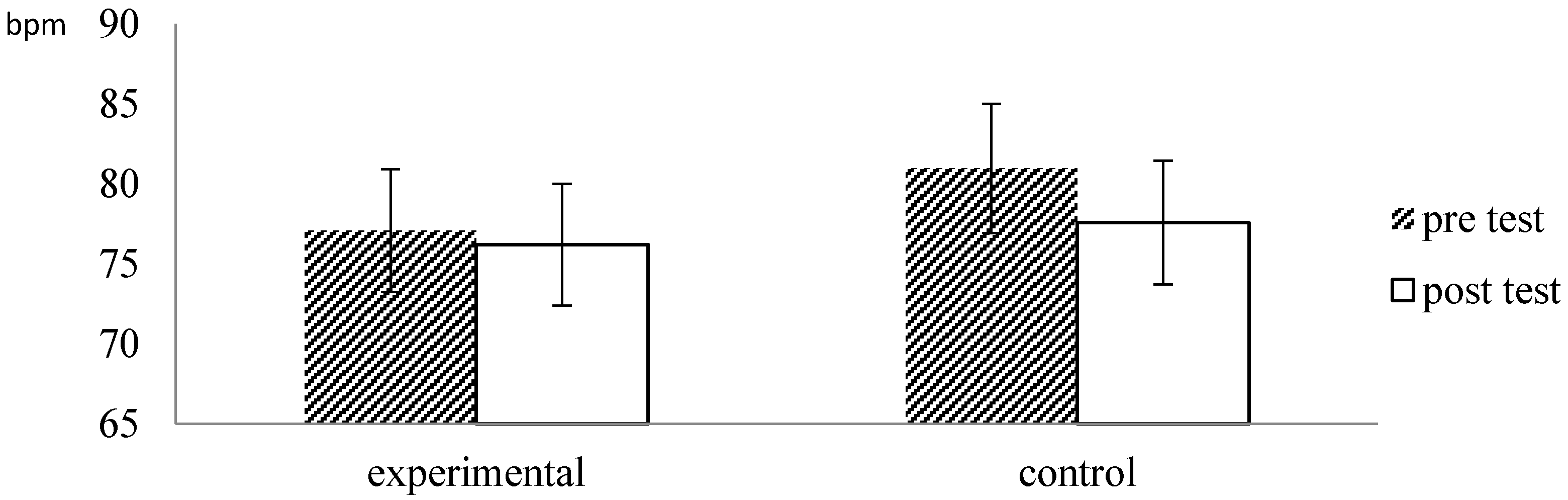
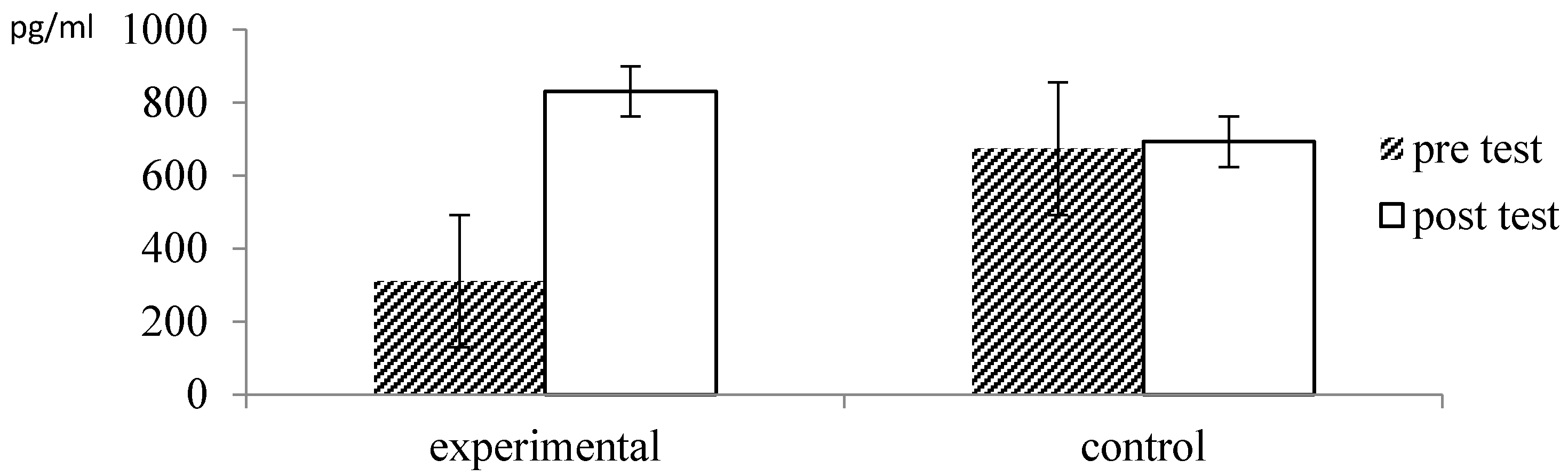
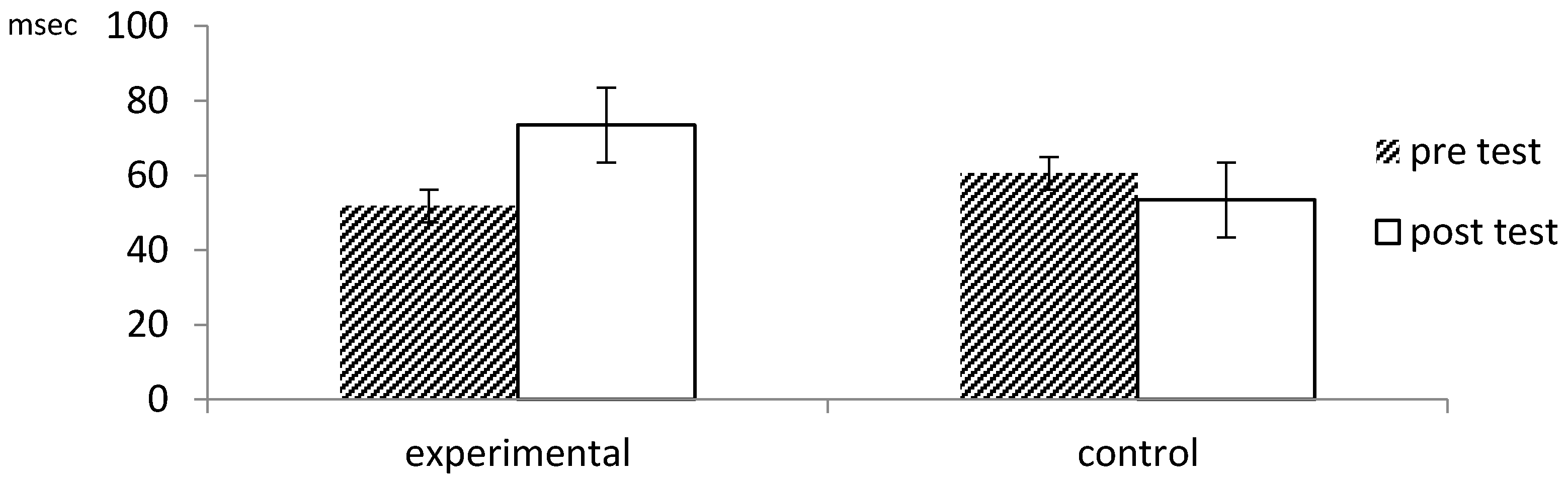
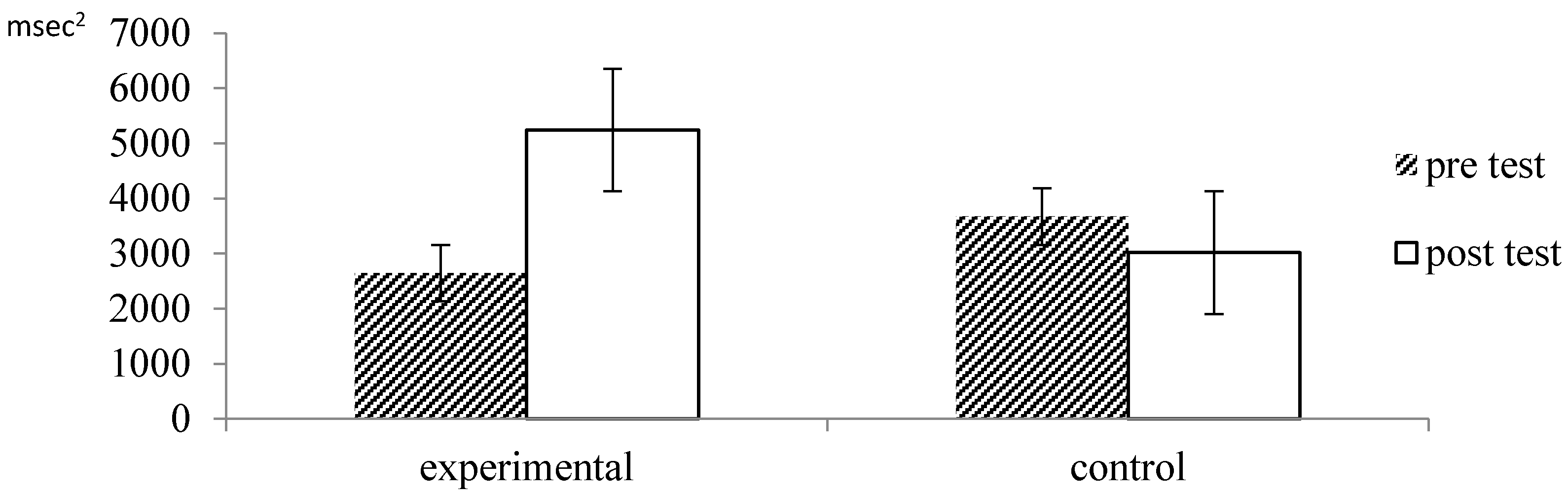
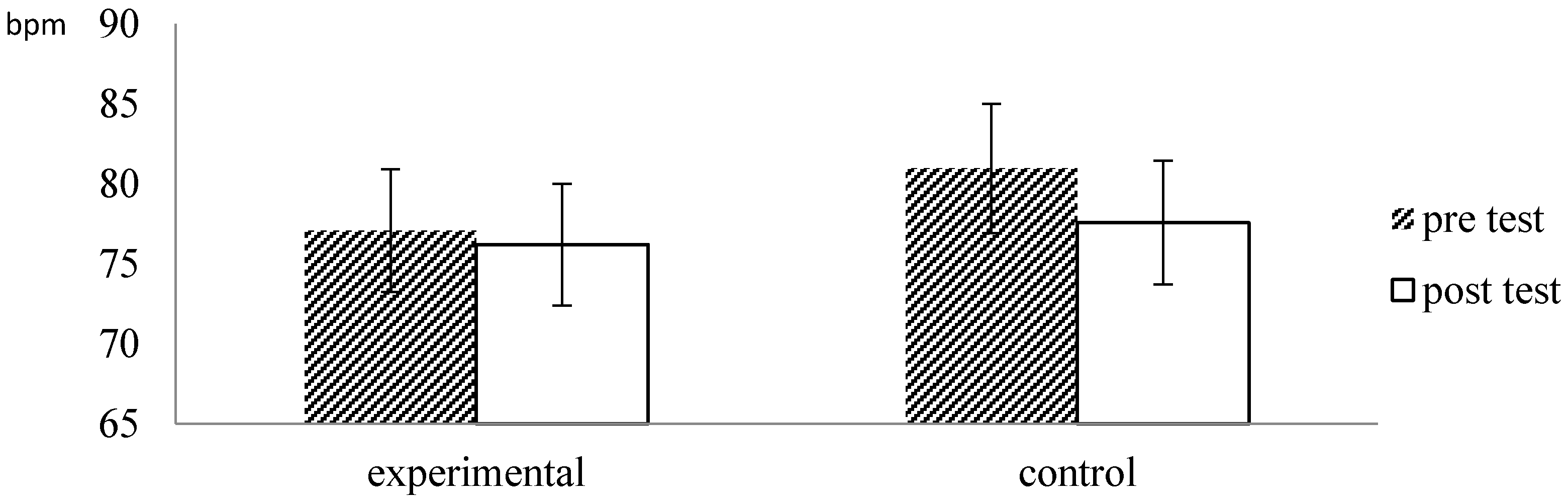
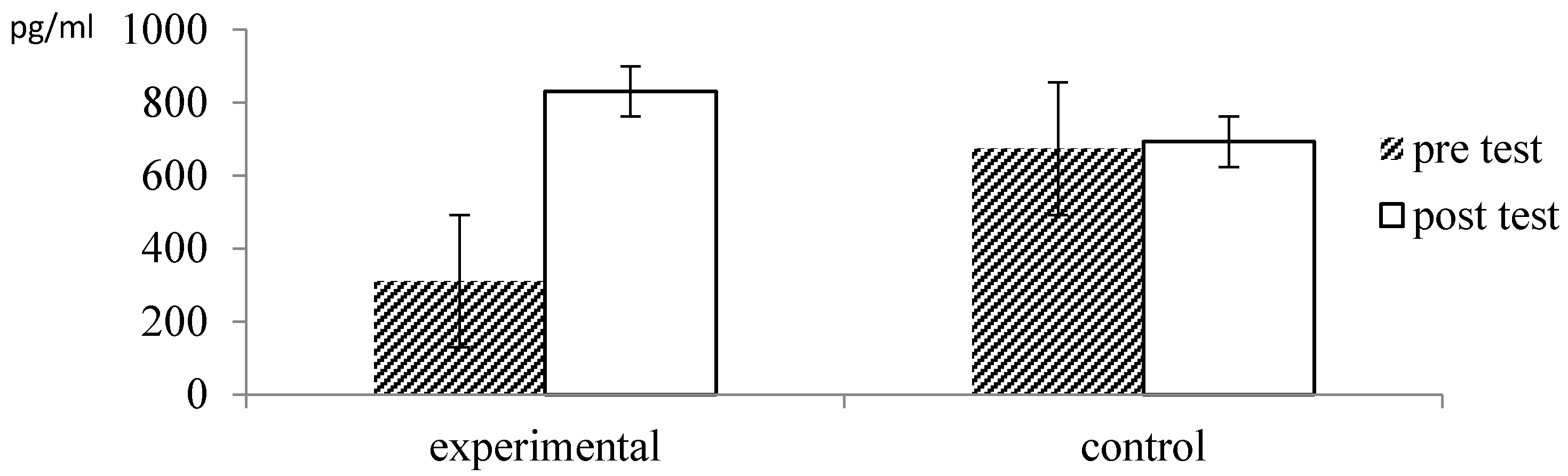
3.1. Physiological Measures
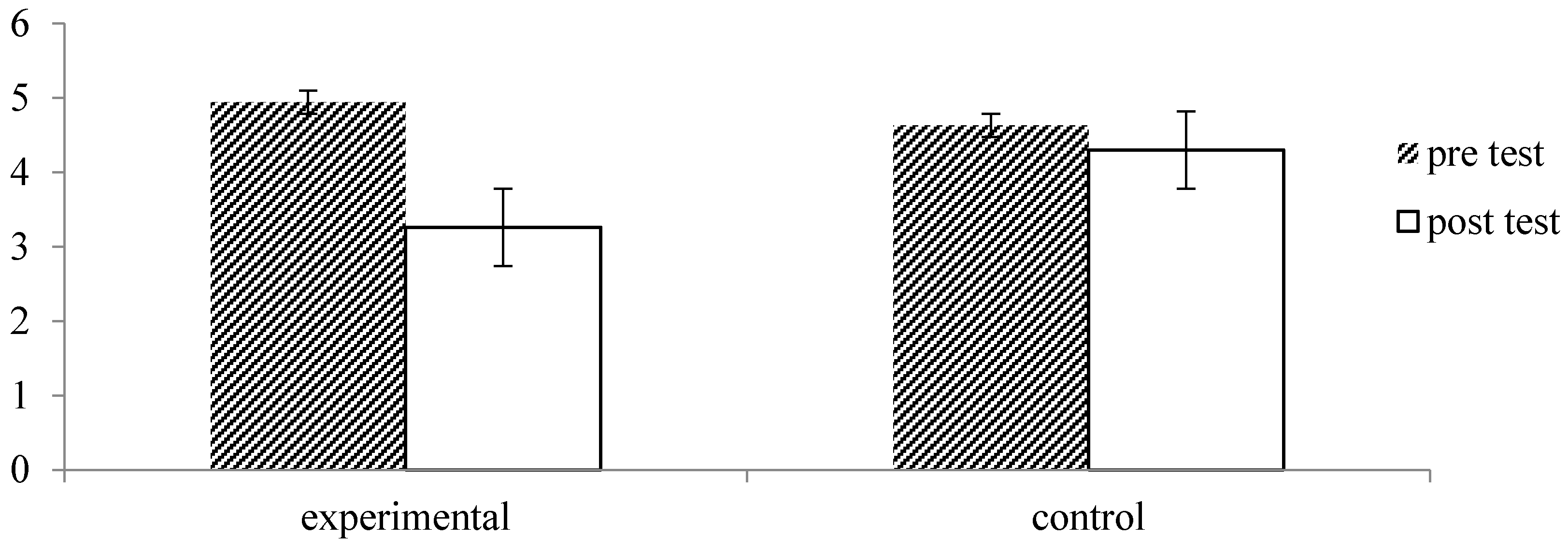
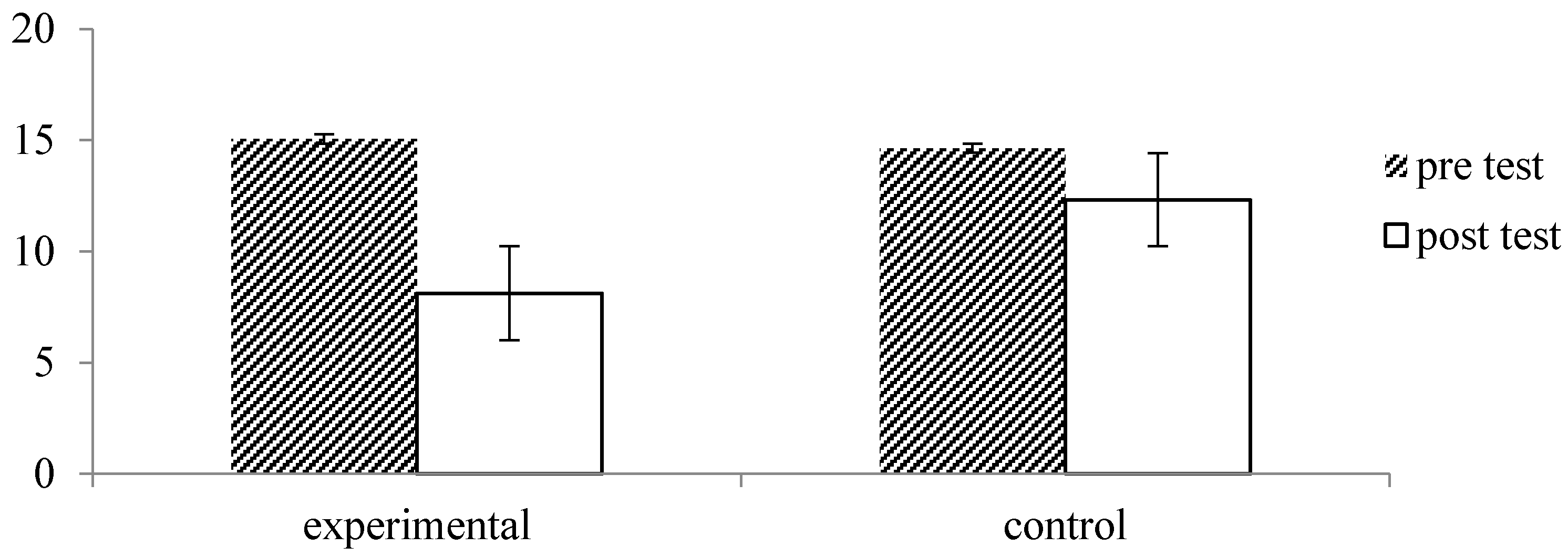
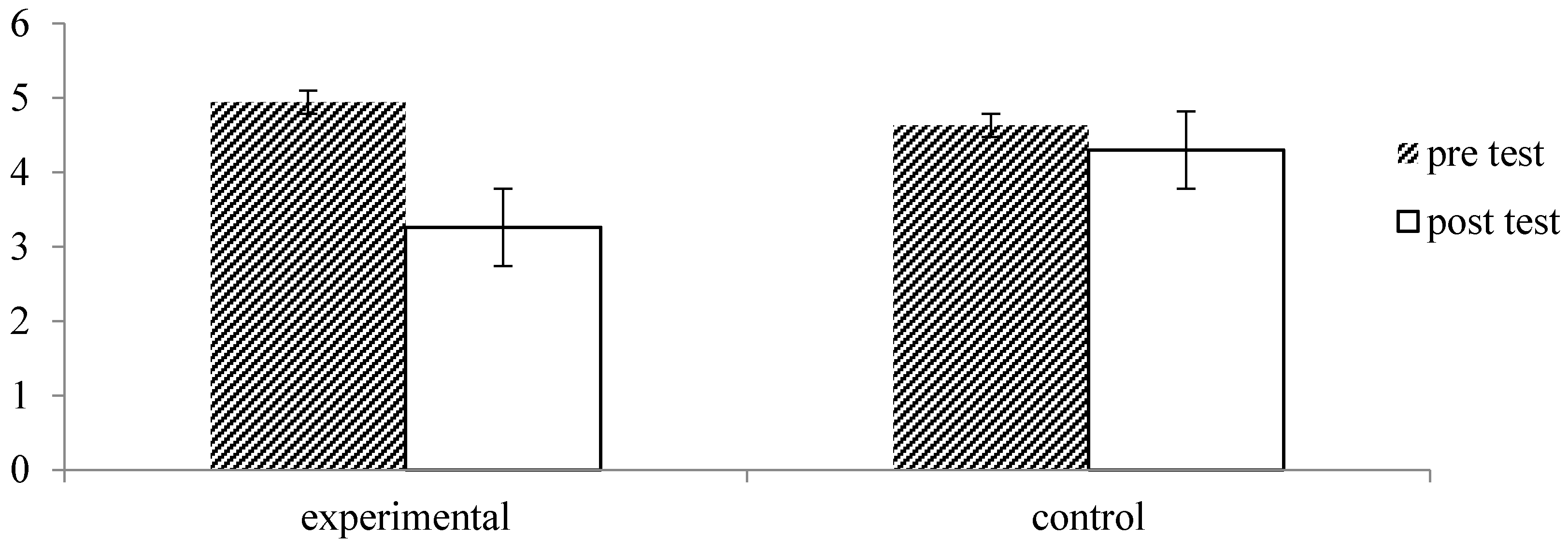
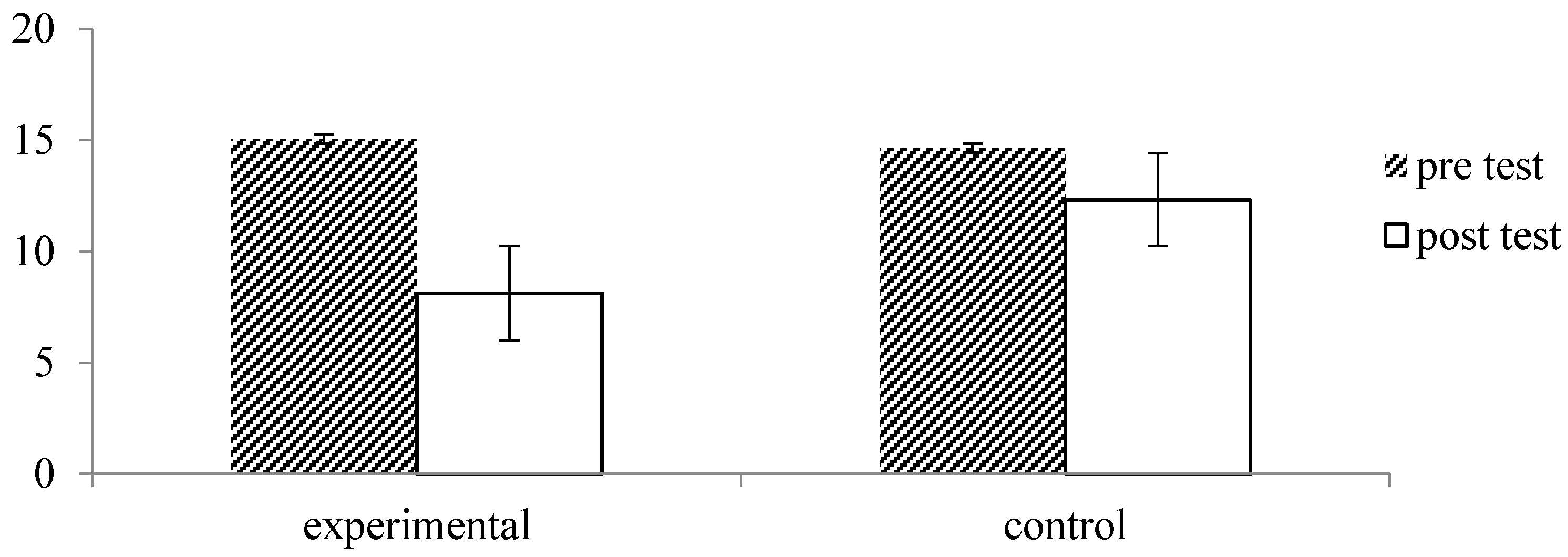
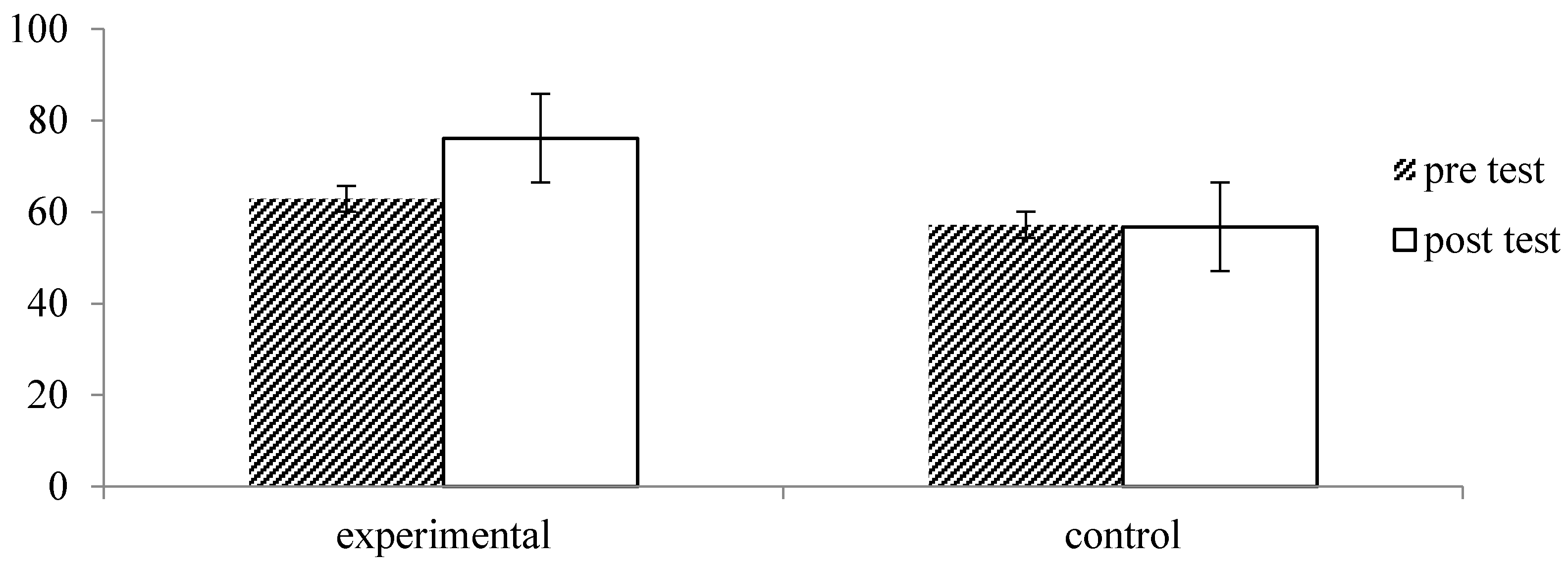
3.2. Psychological Measures
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American college of rheumatology 1990 criteria for the classification of fibromyalgia. Arthr. Rheum 1990, 33, 160–172. [Google Scholar] [CrossRef]
- De Rooij, A.; van der Leeden, M.; Roorda, L.D.; Steultjens, M.P.M.; Dekker, J. Predictors of outcome of multidisciplinary treatment in chronic widespread pain: An observational study. BMC Musculoskelet. Disord. 2013, 14. [Google Scholar] [CrossRef]
- Davies, K.A.; Macfarlane, G.J.; Nicholl, B.I.; Dickens, C.; Morriss, R.; Ray, D.; McBeth, J. Restorative sleep predicts the resolution of chronic widespread pain: Results from the EPIFUND study. Rheumatology 2008, 47, 1809–1813. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Kim, C.H.; Shin, H.C.; Sung, E.J. Clinical characteristics of patients with medically unexplained chronic widespread pain: A primary care center study. Korean J. Fam Med. 2011, 32, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Sarno, J.E. The mindbody prescription. In Grand Central Publishing; Shin, S.C., Ed.; Springer: Seoul, Korea, 2006; pp. 1–50. [Google Scholar]
- Glajchen, M. Chronic pain: Treatment barriers and strategies for clinical practice. Med. Pract. 2001, 15, 211–218. [Google Scholar]
- Schaefer, C.; Mann, R.; Masters, E.T.; Cappelleri, J.C.; Daniel, S.R.; Zlateva, G.; McElroy, H.J.; Chandran, A.B.; Adams, E.H.; Assaf, A.R.; et al. The comparative burden of chronic widespread pain and fibromyalgia in the United States. In Pain Practice; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar]
- Hunfeld, J.A.M.; Perquin, C.W.; Duivenvoorden, H.J.; Hazebroek-Kampschreur, A.A.J.M.; Passchier, J.; van Suijlekom-Smit, L.W.A.; van der Wouden, J.C. Chronic pain and its impact quality of life in adolescents and their families. J. Pediatr. Psychol. 2001, 26, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Korea Institute for Health and Social Affairs. A Report on the Health Related Quality of Life in Korea; Korea Institute for Health and Social Affairs: Seoul, Korea, 2011. [Google Scholar]
- Smith, B.H.; Elliott, A.M.; Chambers, W.A.; Smith, W.C.; Hannaford, P.C.; Penny, K. The impact of chronic pain in the community. Fam. Pract. 2001, 18, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Kim, H.J.; Kim, J.K. Prevalence of chronic widespread pain and fibromyalgia syndrome: A Korean hospital-based study. Rheumatol. Int. 2012, 32, 3435–3442. [Google Scholar] [CrossRef] [PubMed]
- Korea Institute for Health and Social Affairs. In-Depth Analyses of the Third National Health and Nutrition Examination Survey: The Health Interview and Health Behavior Survey Part; Institute for Health and Social Affairs: Seoul, Korea, 2007. [Google Scholar]
- Lee, J.; Ellis, B.; Price, C.; Baranowski, A.P. Chronic widespread pain, including fibromyalgia: A pathway for care developed by the British Pain Society. Br. J. Anaesthesia. 2013, 10. [Google Scholar] [CrossRef] [PubMed]
- Thieme, K.; Flor, H.; Turk, D.C. Psychological pain treatment in fibromyalgia syndrome: Efficacy of operant behavioural and cognitive behavioural treatments. Arthritis Res. Ther. 2006, 8. [Google Scholar] [CrossRef]
- De Rooij, A.; de Boer, M.R.; van der Leeden, M.; Roorda, L.D.; Steultjens, M.P.M.; Dekker, J. Cognitive mechanism of change in multidisciplinary treatment of patients with chronic widespread pain: A prospective cohort study. J. Rehabil. Med. 2013, 46. [Google Scholar] [CrossRef] [PubMed]
- Ariene, L.; Lynn, F.M.; Jane, R. Teaching Strategies for Health Education and Health Promotion: Working with Patients, Families, and Communities; Jones and Bartlett Publishers: Burlington, MA, USA, 2009; p. 279. [Google Scholar]
- Lee, J.; Ellis, B.; Price, A.; Baranowski, A.P. Chronic widespread pain, including fibromyalgia. Br. J. Anaesth. 2014, 112, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Hansen, G.R.; Streltzer, J. The psychology of pain. Emerg. Med. Clin. N Am. 2005, 23, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, K.; Miyazaki, Y.; Hirano, H. Forest therapy. In Korea Forest Therapy Forum; Lee, S.H., Ed.; Springer: Seoul, Korea, 2006; pp. 1–50. [Google Scholar]
- Li, Q.; Kawada, T. Effect of forest therapy on the human psycho-neuro-endocrino-immune network. Nihon Eiseigaku. Zasshi. 2011, 66, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Jung, W.H.; Woo, J.M.; Ryu, J.S.; Han, J.W. The relationship between using forest environment and stress of workers in medical and counseling industries. Korean Inst. Foresty Rec. Welf. 2014, 18, 1–10. [Google Scholar]
- Gathright, J.; Yamada, Y.; Morita, M. Tree-assisted therapy: Therapeutic and societal benefits from purpose-specific technical recreational tree-climbing programs. Arboricult. Urban. Forestry 2008, 34, 222–229. [Google Scholar]
- Sung, J.D.; Woo, J.M.; Kim, W.; Lim, S.K.; Chung, E.J. The effect of cognitive behavior therapy-based “forest Therapy” program on blood pressure, salivary cortisol level, and quality of life in elderly hypertensive patients. Clin. Exp. Hypertens. 2012, 34, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ochiai, H.; Ikei, H.; Song, C.R.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; et al. Physiological and psychological effects of forest therapy on middle-aged males with high-normal blood pressure. Int. J. Environ. Res. Public Health 2015, 12, 2532–2542. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Lim, S.K.; Chung, E.J.; Woo, J.M. The effect of cognitive behavior therapy based psychotherapy applied in a forest environment on physiological changes and remission of major depressive disorder. Psychiatry Investig. 2009, 6, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Friedman, B.H.; Thayer, J.F. Anxiety and autonomic flexibility: A cardiovascular approach. Biol. Psychol. 1998, 49, 303–23. [Google Scholar] [PubMed]
- Kim, W.; Woo, J.M.; Chae, J.H. Heart rate variability in psychiatry. J. Korean Neuropsychiatr. Assoc. 2005, 44, 176–184. [Google Scholar]
- Kim, G.M.; Woo, J.M. Determinants for heart rate variability in a normal Korean population. J. Korean Med. Sci. 2011, 26, 1293–1298. [Google Scholar] [CrossRef] [PubMed]
- Levy, S.; Herberman, R.; Lippman, M.; d’Angelo, T. Correlation of stress factors with sustained depression of natural killer cell activity and predicted prognosis in patients with breast cancer. J. Clin. Oncol. 1987, 5, 348–353. [Google Scholar] [PubMed]
- Koo, K.C.; Shim, D.H.; Yang, C.M.; Lee, S.B.; Kim, S.M.; Shin, T.Y.; Kim, K.H.; Yoon, H.G.; Rha, K.H.; Lee, J.M.; et al. Reduction of the CD16–CD56(bright)NK cell subset precedes NK cell dysfunction in prostate cancer. PLoS ONE 2013, 8, e78049. [Google Scholar] [CrossRef] [PubMed]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for pain (VAS Pain), Numeric Rating Scale for pain (NRS pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63, 240–252. [Google Scholar]
- Williams, A.C.; Richardson, P.H. What does the BDI measure in chronic pain. Pain 1993, 55, 259–266. [Google Scholar] [CrossRef]
- Lee, Y.H.; Song, J.Y. A Study of the reliability and the validity of the BDI, SDS, and MMPI-D Scale. Korean J. Clin. Psychol. 1991, 10, 98–113. [Google Scholar]
- Obradovic, M.; Lai, A.; Liedqens, H. Validity and responsiveness of EuroQol-5 dimension (EQ-5D) versus Short Form-6 dimension (SF-6D) questionnaire in chronic pain. Health Qual. Life Outcomes. 2013, 11. [Google Scholar] [CrossRef] [PubMed]
- Shin, W.S.; Shin, C.S.; Yeoun, P.S. The influence of forest therapy camp on depression in alcoholics. Environ. Health Prev. Med. 2012, 17, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.D.; Woo, J.M.; Kim, W.; Lim, S.K.; Chung, A.S. Relationship between blood pressure variability and the quality of life. Yonsei. Med. J. 2014, 55, 374–378. [Google Scholar] [CrossRef] [PubMed]
- Jung, W.H.; Woo, J.M.; Ryu, J.S. Effect of a forest therapy program and the forest environment on female worker’s stress. Urban. Foresty. Urban. Green. 2015, 14, 274–281. [Google Scholar] [CrossRef]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: New York, NY, USA, 1989. [Google Scholar]
- Joung, D.W.; Kim, G.W.; Choi, Y.H.; Lim, H.J.; Park, S.J.; Woo, J.M.; Park, B.J. The prefrontal cortex activity and psychological effects of viewing forest landscapes in autumn season. Int. J. Environ. Res. Public Health 2015, 12, 7235–7243. [Google Scholar] [CrossRef] [PubMed]
- Song, C.R.; Ikei, H.; Kobayashi, M.; Miura, T.; Taue, M.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; Miyazaki, Y. Effect of forest walking on autonomic nervous system activity in middle-aged hypertensive individuals: A pilot study. Int. J. Environ. Res. Public Health 2015, 12, 2687–2699. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.; Gmeiner, S.; Schultz, C.; Lower, M.; Kuhn, K.; Naranjo, J.R.; Brenneisen, C.; Hinterberger, T. Mindfulness-based Stress Reduction (MBSR) as treatment for chronic back pain—An observational study with assessment of thalamocortical dysrhythmis. Forsch. Komplement. 2015, 22, 298–303. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Mean (Standard Deviation) | p | ||
|---|---|---|---|---|
| Experimental Group | Control Group | |||
| Total sample number | 33 | 28 | ||
| Sex | Male | 16 | 10 | 0.315 |
| Female | 17 | 18 | ||
| Age (years) | 41.6 (6.5) | 37.5 (8.4) | 0.035 * | |
| Height (cm) | 166.8 (8.2) | 165.4 (8.0) | 0.507 | |
| Weight (kg) | 66.7 (14.6) | 63.21 (13.5) | 0.341 | |
| Smoking | Yes/No | 10/23 | 5/23 | 0.232 |
| Drinking | Yes/No | 21/10 | 20/8 | 0.759 |
| Working Type | Day work | 27 | 25 | 0.443 |
| Two shifts | 3 | 3 | ||
| other | 3 | 0 | ||
| Working hours | 8.3 (0.7) | 8.6 (1.0) | 0.167 | |
| Economic status | Fair | 21 | 19 | 0.730 |
| poor | 12 | 9 | ||
| Sleep duration (hours per day) | 5.9 (1.1) | 6.5 (0.9) | 0.038 * | |
| Duration of suffering pain (month) | 3 months or less | 3 | 7 | 0.504 |
| 3–6 months | 4 | 3 | ||
| 6–12 months | 9 | 5 | ||
| 12–24 months | 4 | 2 | ||
| 24 months or more | 13 | 11 | ||
| Time | Program | Location |
|---|---|---|
| Day 1 | ||
| 09:00–11:00 | Orientation and Pre-test | Seoul Paik Hospital (Indoors) |
| 11:00–13:00 | Going to forest | |
| 13:00–14:00 | Lunch | Saneum Natural Recreation Forest (Outdoors) |
| 14:00–16:00 | Walk in the forest and forest activities | |
| 16:00–17:30 | Free time | |
| 17:30–19:00 | Dinner | |
| 19:00–20:00 | Music therapy | Saneum Natural Recreation Forest Auditorium (Indoors) |
| 20:00–21:00 | Psychoeducation: Coping with pain and stress | |
| Day 2 | Saneum Natural Recreation Forest (Outdoors) | |
| 08:30–09:30 | Breakfast | |
| 09:30–11:00 | Stimulation bodily exercise | |
| 11:00–11:30 | Mindfulness-based meditation | |
| 11:30–12:30 | Herbal tea time | |
| 12:30–13:30 | Lunch | |
| 13:30–15:00 | Post-test | Saneum Natural Recreation Forest Auditorium (Indoors) |
| Variable | Sub-Factor | Group | Mean (Standard Deviation) | |||
|---|---|---|---|---|---|---|
| Pre Test | Post Test | t | p | |||
| ECG | SDNN | Experimental (n = 32) | 51.86 (19.55) | 73.50 (29.17) | −4.959 | 0.000 *** |
| Control (n = 26) | 60.60 (21.37) | 53.43 (19.90) | 2.643 | 0.014 * | ||
| TP | Experimental (n = 32) | 2645.43 (1898.77) | 5244.58 (4185.12) | −3.977 | 0.000 *** | |
| Control (n = 26) | 80.98 (8.06) | 77.59 (7.55) | 2.467 | 0.021 * | ||
| HR | Experimental (n = 32) | 77.09 (6.30) | 76.21 (6.23) | 1.102 | 0.279 | |
| Control (n = 26) | 80.98 (8.06) | 77.59 (7.55) | 2.467 | 0.021 * | ||
| NK cell | Experimental (n = 33) | 604.20 (754.92) | 1131.56 (990.29) | −5.391 | 0.000 *** | |
| Control (n = 28) | 1067.16 (908.15) | 1194.80 (996.99) | −1.715 | 0.098 | ||
| Variable | Group | Mean (Standard Deviation) | |||
|---|---|---|---|---|---|
| Pre Test | Post Test | t | p | ||
| VAS Pain | Experimental (n = 33) | 4.94 (1.62) | 3.26 (1.69) | 6.681 | 0.000 *** |
| Control (n = 28) | 4.63 (1.92) | 4.30 (2.10) | 1.185 | 0.246 | |
| BDI | Experimental (n = 33) | 15.06 9.43) | 8.12 (7.05) | 6.869 | 0.000 *** |
| Control (n = 28) | 14.64 (9.67) | 12.32 (9.99) | 2.601 | 0.015 * | |
| EQ-VAS | Experimental (n = 33) | 62.88 (16.78) | 76.09 (16.34) | −7.798 | 0.000 *** |
| Control (n = 28) | 57.21 (23.14) | 56.75 (24.35) | 0.148 | 0.884 | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, J.-W.; Choi, H.; Jeon, Y.-H.; Yoon, C.-H.; Woo, J.-M.; Kim, W. The Effects of Forest Therapy on Coping with Chronic Widespread Pain: Physiological and Psychological Differences between Participants in a Forest Therapy Program and a Control Group. Int. J. Environ. Res. Public Health 2016, 13, 255. https://doi.org/10.3390/ijerph13030255
Han J-W, Choi H, Jeon Y-H, Yoon C-H, Woo J-M, Kim W. The Effects of Forest Therapy on Coping with Chronic Widespread Pain: Physiological and Psychological Differences between Participants in a Forest Therapy Program and a Control Group. International Journal of Environmental Research and Public Health. 2016; 13(3):255. https://doi.org/10.3390/ijerph13030255
Chicago/Turabian StyleHan, Jin-Woo, Han Choi, Yo-Han Jeon, Chong-Hyeon Yoon, Jong-Min Woo, and Won Kim. 2016. "The Effects of Forest Therapy on Coping with Chronic Widespread Pain: Physiological and Psychological Differences between Participants in a Forest Therapy Program and a Control Group" International Journal of Environmental Research and Public Health 13, no. 3: 255. https://doi.org/10.3390/ijerph13030255