Relationship between Caregivers’ Smoking at Home and Urinary Levels of Cotinine in Children

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval of the Study Protocol
2.2. Study Population and Procedures
2.3. Measurements
2.3.1. ETS Exposure by Determination of Urinary Levels of Cotinine
2.3.2. Self-Reporting of ETS Exposure of Children by Caregivers
2.3.3. Smoking Restrictions in the Home
2.3.4. Self-Reporting of Smoking Status by Caregivers
2.4. Statistical Analyses
3. Results
3.1. Characteristics of Caregivers and Children

{kind=link}
| Characteristic | N | Value |
|---|---|---|
| Sex (%) | ||
| male | 510 | 93.92 |
| female | 33 | 6.08 |
| Caregivers | 543 | |
| Mother | 33 | 6.1 |
| Father | 477 | 87.8 |
| Others (e.g., sibling, grandparent) | 33 | 6.1 |
| Age (years) | 543 | 35.3 ± 6.6 |
| Ethnicity (%) | ||
| Han | 541 | 99.63 |
| other | 2 | 0.37 |
| Marital status (married vs. other) (%) | 541 | 99.63 |
| Income (<RMB 5999) | 345 | 63.5 |
| Home size (m2; mean ± SD) | 543 | 111.4 ± 51.9 |
| Number of cohabiting smokers (%) | ||
| 0 | 118 | 21.73 |
| 1 | 310 | 57.09 |
| >1 | 115 | 21.73 |
| Daily consumption of cigarettes (%) | ||
| Light (1–10) | 162 | 38.12 |
| Moderate (11–20) | 179 | 42.12 |
| Heavy (>20) | 84 | 19.76 |
| Number of cigarettes smoked in one day by caregiver a | ||
| Overall | 425 | 13.00 (6.00–18.00) |
| At home | 425 | 6.00 (3.00–8.00) |
| Domestic smoking rules of caregiver (%) | ||
| Total restriction | 0 | 0.00 |
| Partial restriction | 11 | 2.03 |
| No restriction | 532 | 97.97 |
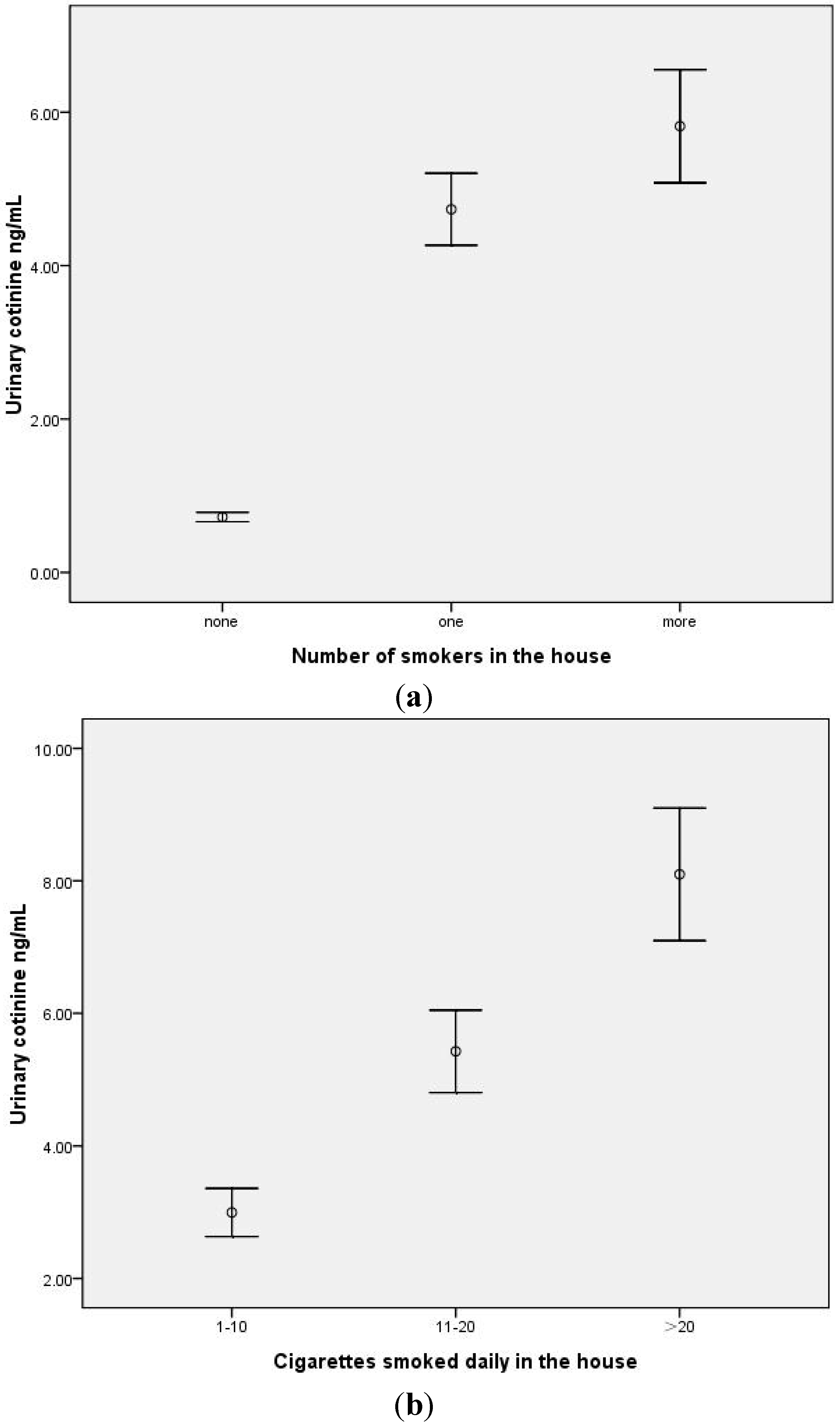
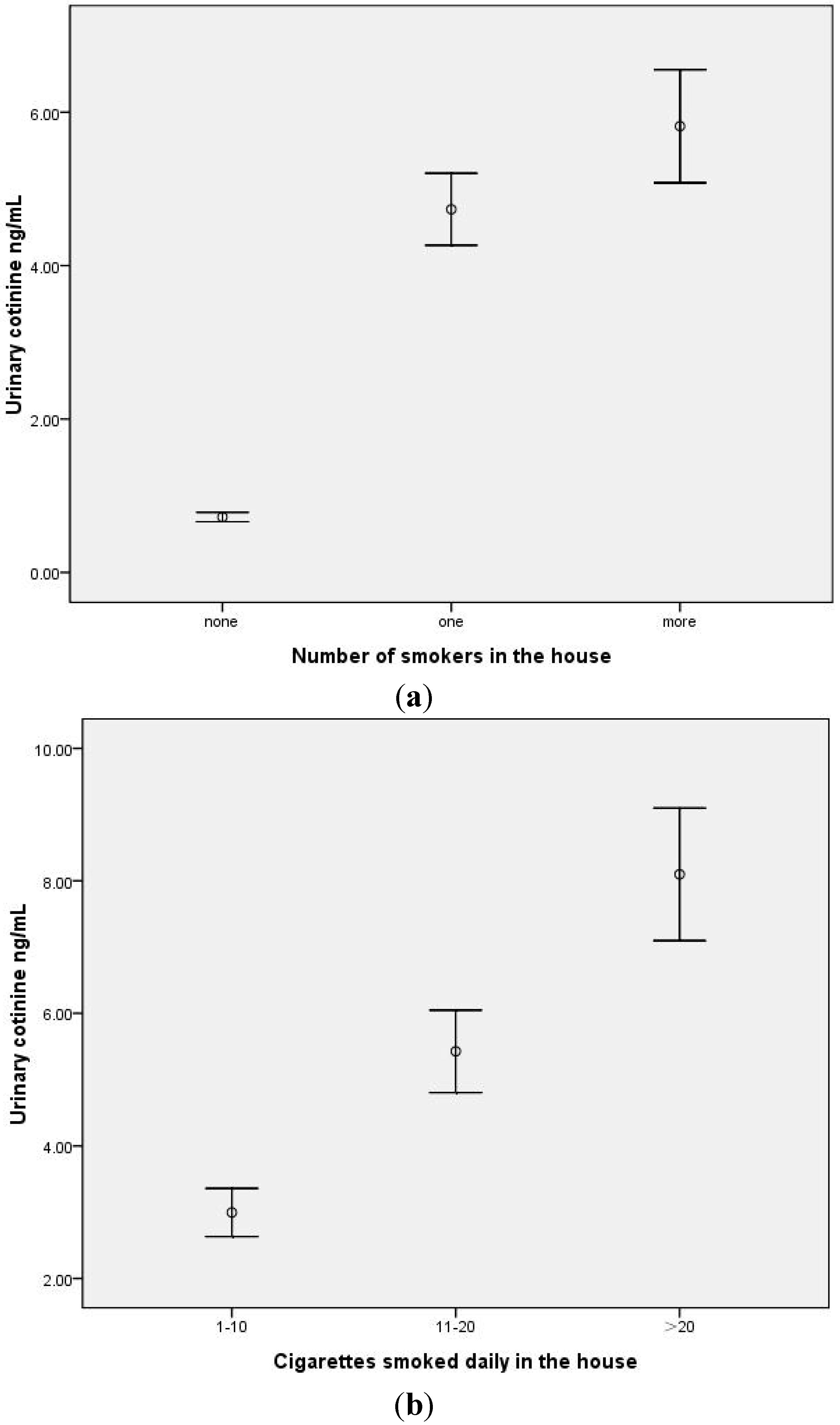
3.2. Children Exposed to ETS by Caregivers and Urinary Levels of Cotinine
| Variable | N | Arithmetic Mean (ng/mL) | 95% Confidence Interval | Median (ng/mL) | Interquartile Range | p | r * |
|---|---|---|---|---|---|---|---|
| No. of caregiving smokers | 543 | 0.665 ** | |||||
| 0 | 118 | 0.72 | 0.66–0.78 | 0.72 | 0.47, 0.91 | <0.001 | |
| 1 | 310 | 4.73 | 4.27–5.20 | 2.97 | 2.12, 5.43 | ||
| >1 | 115 | 5.82 | 5.09–6.55 | 4.46 | 3.10, 7.31 | ||
| Smoking restriction | 425 | ||||||
| Partial smoking restriction | 11 | 4.25 | 1.92–6.58 | 2.55 | 2.21, 4.31 | 0.520 | |
| No smoking restriction | 414 | 5.05 | 4.65–5.45 | 3.43 | 2.29, 5.96 | ||
| Daily cigarette consumption of caregiver | 425 | 0.573 ** | |||||
| light (1–10) | 162 | 3.00 | 2.64–3.35 | 2.29 | 1.90, 2.71 | <0.001 | |
| moderate (11–20) | 179 | 5.43 | 4.81–6.04 | 4.15 | 3.01, 5.85 | ||
| heavy (>20) | 84 | 8.10 | 7.10–9.09 | 7.73 | 4.15, 10.67 |
| Independent Variable | Beta (Unstandardized Coefficient) | Std Error * | Beta (Standardized Coefficient) | R2 | t | p |
|---|---|---|---|---|---|---|
| MODEL a | 0.650 | |||||
| Children not living with smoker (reference group ) | 1 | |||||
| Children living with one smoker | 1.256 | 0.134 | 0.650 | 9.403 | 0.000 | |
| Children living with more than one smoker | 1.481 | 0.139 | 0.633 | 10.640 | 0.000 | |
| Daily cigarette consumption (>20) | 0.647 | 0.070 | 0.245 | 9.302 | 0.000 | |
| Smoker smokes at home every day | 0.330 | 0.125 | 0.151 | 2.650 | 0.008 |
4. Discussion
4.1. A High Proportion of Preschool Children Are Exposed to ETS at Home
4.2. Smoking Restrictions in Families Were Low
4.3. Strengths and Limitations
5. Conclusions
Funding Sources
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Protano, C.; Vitali, M. The new danger of thirdhand smoke: Why passive smoking does not stop at secondhand smoke. Environ. Health Perspect. 2011, 119. [Google Scholar] [CrossRef] [PubMed]
- Yi, O.; Kwon, H.J.; Kim, H.; Ha, M.; Hong, S.-J.; Hong, Y.-C.; Leem, J.-H.; Sakong, J.; Lee, C.G.; Kim, S.-Y.; et al. Effect of environmental tobacco smoke on atopic dermatitis among children in Korea. Environ. Res. 2012, 113, 40–45. [Google Scholar] [CrossRef]
- Burton, A. Does the smoke ever really clear? Thirdhand smoke exposure raises new concerns. Environ. Health Perspect. 2011, 119, 70–74. [Google Scholar] [CrossRef]
- Matt, G.E.; Quintana, P.J.E.; Destaillats, H.; Gundel, L.A.; Sleiman, M.; Singer, B.C.; Jacob, P., III; Benowitz, N.; Winickoff, J.P.; Rehan, V.; et al. Thirdhand tobacco smoke: Emerging evidence and arguments for a multidisciplinary research agenda. Environ. Health Perspect. 2011, 119, 1218–1226. [Google Scholar] [CrossRef]
- Schick, S.F.; Farraro, K.F.; Perrino, C.; Sleiman, M.; van de Vossenberg, G.; Trinh, M.P.; Hammond, S.K.; Jenkins, B.M.; Balmes, J. Thirdhand cigarette smoke in an experimental chamber: Evidence of surface deposition of nicotine, nitrosamines and polycyclic aromatic hydrocarbons and de novo formation of NNK. Tob. Control 2014, 23, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Oberg, M.; Jaakkola, M.S.; Woodward, A.; Peruga, A.; Pruss-Ustun, A. Worldwide burden of disease from exposure to second-hand smoke: A retrospective analysis of data from 192 countries. Lancet. 2011, 377, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Tanski, S.E.; Wilson, K.M. Children and secondhand smoke: Clear evidence for action. Pediatrics 2012, 129, 170–171. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.L.; Hashim, A.; McKeever, T.; Cook, D.G.; Britton, J.; Leonardi-Bee, J. Parental and household smoking and the increased risk of bronchitis , bronchiolitis and other lower respiratory infections in infancy: Systematic review and meta-analysis. Respir. Res. 2011, 12. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.R.; Farber, H.J.; Knowles, S.B.; Lavori, P.W. A randomized trial of parental behavioral counseling and cotinine feedback for lowering environmental tobacco smoke exposure in children with asthma: results of the LET’S Manage Asthma trial. Chest 2011, 139, 581–590. [Google Scholar] [CrossRef] [PubMed]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Tobacco smoke and involuntary smoking. IARC Monogr. Eval. Carcinog. Risks Hum. 2004, 83, 1–1438. [Google Scholar]
- Csakanyi, Z.; Czinner, A.; Spangler, J.; Rogers, T.; Katona, G. Relationship of environmental tobacco smoke to otitis media (OM) in children. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 989–993. [Google Scholar] [CrossRef] [PubMed]
- Yao, T.; Sung, H.Y.; Mao, Z.; Hu, T.W.; Max, W. Secondhand smoke exposure at home in rural China. Cancer Causes Control 2012, 23, 109–115. [Google Scholar] [CrossRef]
- Zhu, C. Implementation Rules on Regulations on Public Places Sanitation Administration. Available online: http://www.tobaccocontrollaws.org/files/live/China/China%20-%20MOH%20Order%20No.%2080.pdf (accessed on 10 March 2011).
- Protano, C.; Andreoli, R.; Manini, P.; Guidotti, M.; Vitali, M. A tobacco-related carcinogen: Assessing the impact of smoking behaviours of cohabitants on benzene exposure in children. Tob. Control 2012, 21, 325–329. [Google Scholar] [CrossRef] [PubMed]
- McNabola, A.; Gill, L.W. The control of environmental tobacco smoke: A policy review. Int. J. Environ. Res. Public Health. 2009, 6, 741–758. [Google Scholar] [CrossRef] [PubMed]
- Office of the Leading Small Group for Implementation of the Framework Convention on Tobacco Control. 2007 China Tobacco Control Report. Create a Smoke-Free Environment, Enjoy a Healthy Life; Ministry of Health: Beijing, China, 2007. [Google Scholar]
- Ashley, M.J.; Ferrence, R. Reducing children’s exposure to environmental tobacco smoke in homes: Issues and strategies. Tob. Control. 1998, 7, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Eakin, M.N.; Rand, C.S.; Borrelli, B.; Bilderback, A.; Hovell, M.; Riekert, K.A. Effectiveness of motivational interviewing to reduce head start children’s secondhand smoke exposure. A randomized clinical trial. Am. J. Respir. Crit. Care Med. 2014, 189, 1530–1537. [Google Scholar] [CrossRef]
- Mantziou, V.; Vardavas, C.I.; Kletsiou, E.; Priftis, K.N. Predictors of childhood exposure to parental secondhand smoke in the house and family car. Int J. Environ. Res. Public Health. 2009, 6, 433–444. [Google Scholar] [CrossRef]
- Patja, K.; Hakala, S.; Prattala, R.; Ojala, K.; Boldo, E.; Oberg, M. Adult smoking as a proxy for environmental tobacco smoke exposure among children—Comparing the impact of the level of information in Estonia, Finland and Latvia. Prev. Med. 2009, 49, 240–244. [Google Scholar] [CrossRef]
- Avila-Tang, E.; Al-Delaimy, W.K.; Ashley, D.L.; Benowitz, N.; Bernert, J.T.; Kim, S.; Samet, J.M.; Hecht, S.S. Assessing secondhand smoke using biological markers. Tob. Control. 2013, 22, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Rangiah, K.; Hwang, W.T.; Mesaros, C.; Vachani, A.; Blair, I.A. Nicotine exposure and metabolizer phenotypes from analysis of urinary nicotine and its 15 metabolites by LC-MS. Bioanalysis 2011, 3, 745–761. [Google Scholar] [CrossRef]
- Wilson, K.M.; Klein, J.D.; Blumkin, A.K.; Gottlieb, M.; Winickoff, J.P. Tobacco-smoke exposure in children who live in multiunit housing. Pediatrics 2011, 127, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Winickoff, J.P.; Nabi-Burza, E.; Chang, Y.; Finch, S.; Regan, S.; Wasserman, R.; Ossip, D.; Woo, H.; Klein, J.; Dempsey, J.; et al. Implementation of a parental tobacco control intervention in pediatric practice. Pediatrics 2013, 132, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.L.; Yen, Y.Y.; Lin, P.L.; Chiu, C.H.; Hsu, C.C.; Chen, T.; Hu, C.Y.; Lin, Y.Y.; Lee, C.H.; Chen, F.L.; et al. Household secondhand smoke exposure of elementary schoolchildren in Southern Taiwan and factors associated with their confidence in avoiding exposure: A cross-sectional study. BMC Public Health 2012, 12. [Google Scholar] [CrossRef]
- Bleakley, A.; Hennessy, M.; Mallya, G.; Romer, D. Home smoking policies in urban households with children and smokers. Prev. Med. 2014, 62, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, P.C.; Currie, D.B.; Currie, C.E.; Haw, S.J. Changes in child exposure to environmental tobacco smoke (CHETS) study after implementation of smoke-free legislation in Scotland: National cross sectional survey. BMJ. 2007, 335. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, D.A.; Meyers, M.J.; Oh, S.S.; Nguyen, E.A.; Fuentes-Afflick, E.; Wu, A.H.; Jacob, P.; Benowitz, N.L. Determination of tobacco smoke exposure by plasma cotinine levels in infants and children attending urban public hospital clinics. Arch. Pediatr. Adolesc. Med. 2012, 166, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Tung, K.Y.; Wu, K.Y.; Tsai, C.H.; Su, M.W.; Chen, C.H.; Lin, M.H.; Chen, Y.C.; Wu, W.C.; Lee, Y.L. Association of time-location patterns with urinary cotinine among asthmatic children under household environmental tobacco smoke exposure. Environ. Res. 2013, 124, 7–12. [Google Scholar] [CrossRef]
- Mak, Y.W.; Loke, A.Y.; Abdullah, A.S.; Lam, T.H. Household smoking practices of parents with young children, and predictors of poor household smoking practices. Public Health 2008, 122, 1199–1209. [Google Scholar] [CrossRef] [PubMed]
- Jatlow, P.; McKee, S.; O’Malley, S.S. Correction of urine cotinine concentrations for creatinine excretion: Is it useful? Clin. Chem. 2003, 49, 1932–1934. [Google Scholar] [CrossRef]
- Matt, G.E.; Wahlgren, D.R.; Hovell, M.F.; Zakarian, J.M.; Bernert, J.T.; Meltzer, S.B.; Pirkle, J.L.; Caudill, S. Measuring environmental tobacco smoke exposure in infants and young children through urine cotinine and memory-based parental reports: Empirical findings and discussion. Tob. Control 1999, 8, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L. Cotinine as a biomarker of environmental tobacco smoke exposure. Epidemiol. Rev. 1996, 18, 188–204. [Google Scholar] [CrossRef] [PubMed]
- Abidin, E.Z.; Semple, S.; Omar, A.; Rahman, H.A.; Turner, S.W.; Ayres, J.G. A survey of schoolchildren’s exposure to secondhand smoke in Malaysia. BMC Public Health 2011, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ossip, D.J.; Chang, Y.C.; Nabi-Burza, E.; Drehmer, J.; Finch, S.; Hipple, B.; Rigotti, N.A.; Klein, J.D.; Winickoff, J.P. Strict smoke-free home policies among smoking parents in pediatric settings. Acad. Pediatr. 2013, 13, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Baxi, R.; Sharma, M.; Roseby, R.; Polnay, A.; Priest, N.; Waters, E.; Spencer, N.; Webster, P. Family and carer smoking control programmes for reducing children’s exposure to environmental tobacco smoke. Cochrane Database Syst. Rev. 2014, 3. [Google Scholar] [CrossRef]
- Protano, C.; Andreoli, R.; Manini, P.; Vitali, M. How home-smoking habits affect children: A cross-sectional study using urinary cotinine measurement in Italy. Int. J. Public Health 2012, 57, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Gu, D.; Wu, X.; Reynolds, K.; Duan, X.; Xin, X.; Reynolds, R.F.; Whelton, P.K.; He, J.; InterASIA Collaborative Group. Cigarette smoking and exposure to environmental tobacco smoke in China: The international collaborative study of cardiovascular disease in Asia. Am. J. Public Health 2004, 94, 1972–1976. [Google Scholar]
- Abdullah, A.S.; Hua, F.; Xia, X.; Hurlburt, S.; Ng, P.; MacLeod, W.; Siegel, M.; Griffiths, S.; Zhang, Z. Second-hand smoke exposure and household smoking bans in Chinese families: A qualitative study. Health Soc. Care Community 2011, 20, 1–9. [Google Scholar] [PubMed]
- Wilson, I.; Semple, S.; Mills, L.M.; Ritchie, D.; Shaw, A.; O’Donnell, R.; Bonella, P.; Turner, S.; Amos, A. REFRESH—Reducing families’ exposure to secondhand smoke in the home: A feasibility study. Tob. Control 2013, 22. [Google Scholar] [CrossRef]
- Protano, C.; Guidotti, M.; Manini, P.; Petyx, M.; La Torre, G.; Vitali, M. Benzene exposure in childhood: Role of living environments and assessment of available tools. Environ. Int. 2010, 36, 779–787. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Yang, M.; Tian, L.; Huang, Z.; Chen, F.; Hu, J.; Wang, F.; Chen, G.; Xiao, S. Relationship between Caregivers’ Smoking at Home and Urinary Levels of Cotinine in Children. Int. J. Environ. Res. Public Health 2014, 11, 12499-12513. https://doi.org/10.3390/ijerph111212499
Wang Y, Yang M, Tian L, Huang Z, Chen F, Hu J, Wang F, Chen G, Xiao S. Relationship between Caregivers’ Smoking at Home and Urinary Levels of Cotinine in Children. International Journal of Environmental Research and Public Health. 2014; 11(12):12499-12513. https://doi.org/10.3390/ijerph111212499
Chicago/Turabian StyleWang, Yun, Mei Yang, Lang Tian, Zhiqiang Huang, Faming Chen, Jingsong Hu, Fuzhi Wang, Gui Chen, and Shuiyuan Xiao. 2014. "Relationship between Caregivers’ Smoking at Home and Urinary Levels of Cotinine in Children" International Journal of Environmental Research and Public Health 11, no. 12: 12499-12513. https://doi.org/10.3390/ijerph111212499