A Targeted and Tailored eHealth Weight Loss Program for Young Women: The Be Positive Be Healthe Randomized Controlled Trial

 ,
,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Recruitment
2.3. Intervention: Be Positive Be Healthe
2.4. Wait List Control Group
2.5. Data Collection
2.6. Outcomes
Efficacy
2.7. Acceptability
2.7.1. Sample Size
2.7.2. Randomization
2.7.3. Statistical Analysis
3. Results
3.1. Recruitment
3.2. Participants at Baseline
3.3. Program Efficacy
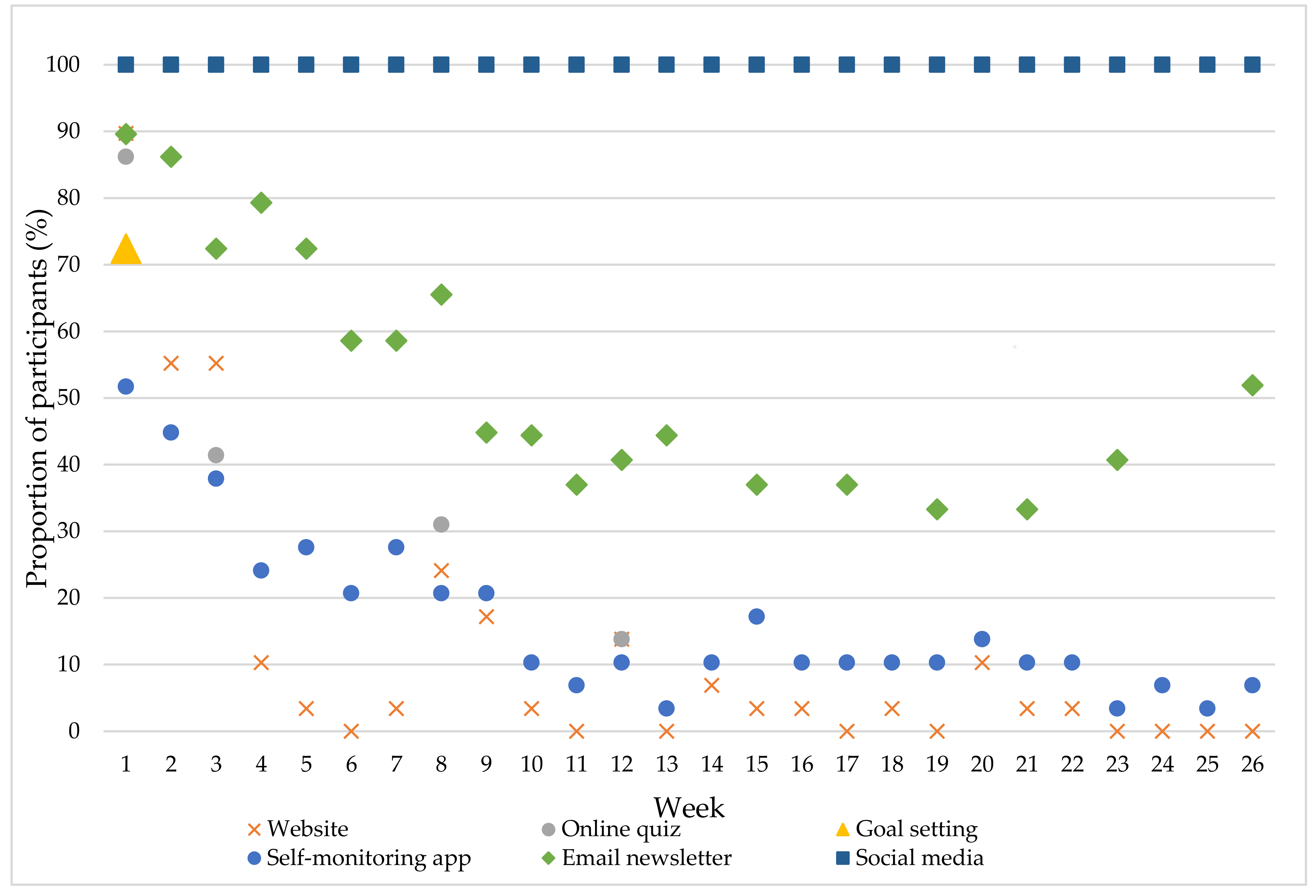
3.4. Program Acceptability
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Gordon-Larsen, P.; The, N.S.; Adair, L.S. Longitudinal trends in obesity in the united states from adolescence to the third decade of life. Obesity 2010, 18, 1801–1804. [Google Scholar] [CrossRef] [PubMed]
- Norman, J.E.; Bild, D.; Lewis, C.E.; Liu, K.; West, D.S. The impact of weight change on cardiovascular disease risk factors in young black and white adults: The cardia study. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Gomersall, S.R.; Dobson, A.J.; Brown, W.J. Weight gain, overweight, and obesity: Determinants and health outcomes from the australian longitudinal study on women’s health. Curr. Obes. Rep. 2014, 3, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Normal Weight, Overweight and Obesity among Adults Aged 20 and over, by Selected Characteristics: United States, Selected Years 1988–1994 through 2011–2014. Available online: http://www.cdc.gov/nchs/data/hus/2015/058.pdf (accessed on 20 October 2016).
- Grech, A.; Allman-Farinelli, M. Prevalence and period trends of overweight and obesity in Australian young adults. Eur. J. Clin. Nutr. 2016, 70, 1083–1085. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Overweight and Obesity in Australia: A Birth Cohort Analysis; Australian Institute of Health and Welfare: Canberra, Australia, 2017.
- Kulie, T.; Slattengren, A.; Redmer, J.; Counts, H.; Eglash, A.; Schrager, S. Obesity and women’s health: An evidence-based review. J. Am. Board Fam. Med. 2011, 24, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Ryan, D. Obesity in women: A life cycle of medical risk. Int. J. Obes. 2007, 31, S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Carslake, D.; Jeffreys, M.; Davey Smith, G. Being overweight in early adulthood is associated with increased mortality in middle age. Sci. Rep. 2016, 6, 36046. [Google Scholar] [CrossRef] [PubMed]
- Stang, J.; Huffman, L.G. Position of the academy of nutrition and dietetics: Obesity, reproduction, and pregnancy&outcomes. J. Acad. Nutr. Diet. 2016, 116, 677–691. [Google Scholar] [PubMed]
- Hutchesson, M.J.; Hulst, J.; Collins, C.E. Weight management interventions targeting young women: A systematic review. J. Acad. Nutr. Diet. 2013, 113, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Poobalan, A.S.; Aucott, L.S.; Precious, E.; Crombie, I.K.; Smith, W.C. Weight loss interventions in young people (18 to 25 year olds): A systematic review. Obes. Rev. 2010, 11, 580–592. [Google Scholar] [CrossRef] [PubMed]
- Gokee-LaRose, J.; Gorin, A.A.; Raynor, H.A.; Laska, M.N.; Jeffery, R.W.; Levy, R.L.; Wing, R.R. Are standard behavioral weight loss programs effective for young adults? Int. J. Obes. 2009, 33, 1374–1380. [Google Scholar] [CrossRef] [PubMed]
- Leonard, A.; Hutchesson, M.; Patterson, A.; Chalmers, K.; Collins, C. Recruitment and retention of young women into nutrition research studies: Practical considerations. Trials 2014, 15, 23–23. [Google Scholar] [CrossRef] [PubMed]
- Kreuter, M.W.; Skinner, C.S. Tailoring: What’s in a name? Health Educ. Res. 2000, 15, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Eyles, H.C.; Mhurchu, C.N. Does tailoring make a difference? A systematic review of the long-term effectiveness of tailored nutrition education for adults. Nutr. Rev. 2009, 67, 464–480. [Google Scholar] [CrossRef] [PubMed]
- Broekhuizen, K.; Kroeze, W.; Van Poppel, M.N.M.; Oenema, A.; Brug, J. A systematic review of randomized controlled trials on the effectiveness of computer-tailored physical activity and dietary behavior promotion programs: An update. Ann. Behav. Med. 2012, 44, 259–286. [Google Scholar] [CrossRef] [PubMed]
- Loria, C.M.; Signore, C.; Arteaga, S.S. The need for targeted weight-control approaches in young women and men. Am. J. Prev. Med. 2010, 38, 233–235. [Google Scholar] [CrossRef] [PubMed]
- Holley, T.J.; Collins, C.E.; Morgan, P.J.; Callister, R.; Hutchesson, M.J. Weight expectations, motivations for weight change and perceived factors influencing weight management in young australian women: A cross-sectional study. Public Health Nutr. 2016, 19, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Hutchesson, M.J.; Morgan, P.J.; Callister, R.; Pranata, I.; Skinner, G.; Collins, C.E. Be positive be healthe: Development and implementation of a targeted e-health weight loss program for young women. Telemed. J. e-Health 2016, 22, 519–528. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic. Report of a Who Consultation; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Panz, V.R.; Raal, F.J.; Paiker, J.; Immelman, R.; Miles, H. Performance of the cardiochek pa and cholestech ldx point-of-care analysers compared to clinical diagnostic laboratory methods for the measurement of lipids. Cardiovasc. J. S. Afr. 2005, 16, 112–117. [Google Scholar] [PubMed]
- Ferreira, C.E.; Franca, C.N.; Correr, C.J.; Zucker, M.L.; Andriolo, A.; Scartezini, M. Clinical correlation between a point-of-care testing system and laboratory automation for lipid profile. Clin. Chim. Acta 2015, 446, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Godin, G.; Shephard, R. Godin leisure-time exercise questionnaire. Med. Sci. Sports Exerc. 1997, 29, 36–38. [Google Scholar]
- Marshall, A.L.; Miller, Y.D.; Burton, N.W.; Brown, W.J. Measuring total and domain-specific sitting: A study of reliability and validity. Med. Sci. Sports Exerc. 2010, 42, 1094–1102. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.E.; Boggess, M.M.; Watson, J.F.; Guest, M.; Duncanson, K.; Pezdirc, K.; Rollo, M.; Hutchesson, M.J.; Burrows, T.L. Reproducibility and comparative validity of a food frequency questionnaire for australian adults. Clin. Nutr. 2014, 33, 906–914. [Google Scholar] [CrossRef] [PubMed]
- Endicott, J.; Nee, J.; Harrison, W.; Blumenthal, R. Quality of life enjoyment and satisfaction questionnaire: A new measure. Psychopharmacol. Bull. 1993, 29, 321–326. [Google Scholar] [PubMed]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Lytle, L.A.; Svetkey, L.P.; Patrick, K.; Belle, S.H.; Fernandez, I.D.; Jakicic, J.M.; Johnson, K.C.; Olson, C.M.; Tate, D.F.; Wing, R.; et al. The early trials: A consortium of studies targeting weight control in young adults. Transl. Behav. Med. 2014, 4, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Svetkey, L.P.; Batch, B.C.; Lin, P.H.; Intille, S.S.; Corsino, L.; Tyson, C.C.; Bosworth, H.B.; Grambow, S.C.; Voils, C.; Loria, C.; et al. Cell phone intervention for you (city): A randomized, controlled trial of behavioral weight loss intervention for young adults using mobile technology. Obesity 2015, 23, 2133–2141. [Google Scholar] [CrossRef] [PubMed]
- Godino, J.G.; Merchant, G.; Norman, G.J.; Donohue, M.C.; Marshall, S.J.; Fowler, J.H.; Calfas, K.J.; Huang, J.S.; Rock, C.L.; Griswold, W.G.; et al. Using social and mobile tools for weight loss in overweight and obese young adults (project smart): A 2-year, parallel-group, randomised, controlled trial. Lancet Diabetes Endocrinol. 2016, 4, 747–755. [Google Scholar] [CrossRef]
- Jakicic, J.M.; King, W.C.; Marcus, M.D.; Davis, K.K.; Helsel, D.; Rickman, A.D.; Gibbs, B.B.; Rogers, R.J.; Wahed, A.; Belle, S.H. Short-term weight loss with diet and physical activity in young adults: The idea study. Obesity 2015, 23, 2385–2397. [Google Scholar] [CrossRef] [PubMed]
- Jakicic, J.M.; Davis, K.K.; Rogers, R.J.; King, W.C.; Marcus, M.D.; Helsel, D.; Rickman, A.D.; Wahed, A.S.; Belle, S.H. Effect of wearable technology combined with a lifestyle intervention on long-term weight loss: The idea randomized clinical trial. JAMA 2016, 316, 1161–1171. [Google Scholar] [CrossRef] [PubMed]
- Moe, S.G.; Lytle, L.A.; Nanney, M.S.; Linde, J.A.; Laska, M.N. Recruiting and retaining young adults in a weight gain prevention trial: Lessons learned from the choices study. Clin. Trials 2016, 13, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, N.D.; Sauder, K.A.; Fabbri, S. Reach and effectiveness of the national diabetes prevention program for young women. Am. J. Prev. Med. 2017, 53, 714–718. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (tidier) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tate, D.F.; LaRose, J.G.; Griffin, L.P.; Erickson, K.E.; Robichaud, E.F.; Perdue, L.; Espeland, M.A.; Wing, R.R. Recruitment of young adults into a randomized controlled trial of weight gain prevention: Message development, methods, and cost. Trials 2014, 15, 326. [Google Scholar] [CrossRef] [PubMed]
- Lam, E.; Partridge, S.R.; Allman-Farinelli, M. Strategies for successful recruitment of young adults to healthy lifestyle programmes for the prevention of weight gain: A systematic review. Obes. Rev. 2016, 17, 178–200. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. National Health Survey: First Results, 2014-15. Available online: http://www.abs.gov.au/ausstats/[email protected]/Lookup/by%20Subject/4364.0.55.001~2014-15~Main%20Features~Exercise~29 (accessed on 25 January 2018).
- Pew Research Center. Social Media Usage: 2005–2015. Available online: http://www.pewinternet.org/2015/10/08/social-networking-usage-2005-2015/ (accessed on 10 December 2017).
- Pew Research Center. Social Media Update 2016. Available online: http://www.pewinternet.org/2016/11/11/social-media-update-2016/ (accessed on 10 December 2017).
- Hutchesson, M.J.; Rollo, M.E.; Krukowski, R.; Ells, L.; Harvey, J.; Morgan, P.J.; Callister, R.; Plotnikoff, R.; Collins, C.E. Ehealth interventions for the prevention and treatment of overweight and obesity in adults: A systematic review with meta-analysis. Obes. Rev. 2015, 16, 376–392. [Google Scholar] [CrossRef] [PubMed]
- Wolin, K.Y.; Steinberg, D.M.; Lane, I.B.; Askew, S.; Greaney, M.L.; Colditz, G.A.; Bennett, G.G. Engagement with ehealth self-monitoring in a primary care-based weight management intervention. PLoS ONE 2015, 10, e0140455. [Google Scholar] [CrossRef] [PubMed]
- Burke, L.E.; Wang, J.; Sevick, M.A. Self-monitoring in weight loss: A systematic review of the literature. J. Am. Diet. Assoc. 2011, 111, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Gokee-LaRose, J.; Tate, D.F.; Lanoye, A.; Fava, J.L.; Jelalian, E.; Blumenthal, M.; Caccavale, L.J.; Wing, R.R. Adapting evidence-based behavioral weight loss programs for emerging adults: A pilot randomized controlled trial. J. Health Psychol. 2017. [Google Scholar] [CrossRef]
- Glasgow, R.E. Ehealth evaluation and dissemination research. Am. J. Prev. Med. 2007, 32, S119–S126. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Technology | Description 1 |
|---|---|
| Be Positive Be Healthe Website Participants had password-protected log-ins | Resources provide advice on weight loss, general healthy eating and physical activity, and the 10 Steps to Success. These website resources remained static over the 6 months. |
| An online quiz with individualized email feedback in Week 1 to assess current weight, motivations, weight loss readiness, and behaviours of the 10 Steps to Success. Participants received automated personalized email feedback from their accredited practising dietitian (APD) focusing on: setting a realistic weight loss goal, their energy requirements for weight loss, and their current eating behaviours and physical activity levels compared to the 10 Steps to Success. | |
| Weight and behaviour change goals for each 10 Steps to Success were recorded in Week 1 following receipt of email feedback. | |
| Follow-up online quizzes (Weeks 3, 8, 12, 20) monitored progress towards goal achievement and APD provides automated personalized email feedback including virtual rewards (i.e., diamonds). | |
| Self-monitoring app Easy Diet Diary (Xyris Software Australia) Downloaded by participants and accessible via iPhone, iPad or iPod touch (Apple Inc., Cupertino, California, USA). | Used to record weight, energy intake and energy expenditure goals, and to self-monitor weight, food intake and physical activity. Provided automated feedback on nutrient content of food items and energy expended from exercises, as well as cumulative daily totals compared to goals. Participants were recommended to record weight one/week and food intake and physical activity at least four days/week. |
| Email newsletters, Hypertext Markup Language (HTML) newsletters sent to participants elected email address (Campaign Monitor) Text messages (SMS) Sent to participants elected mobile number (Twilio) | Email newsletters and text messages: provided practical tips to achieve and maintain 10 Steps to Success; reminded participants to complete other program tasks (e.g., quiz, self-monitoring, and goal setting); and promoted self-reward for achievement of goals and self-instruction. During Weeks 1–12 eNewsletters were sent once/week and text messages two/week; from Week 13–26 eNewsletters were sent fortnightly and text messages one/week. |
| Social Media Participants joined a private Facebook group and followed a private Instagram account using their personal account Content posted using Hootsuite | Provided dynamic content about 10 Steps to Success; created a social network for women to interact with each other (social support) and their APD. Three posts/week made by the APD (one educational, one weekly challenge, one practical tip for overcoming barriers) plus one reminder post on weeks other tasks were to be completed (e.g., online quizzes). Both accounts moderated by the APD and questions answered. |
| Variable | Intervention (n = 29) | Control (n = 28) | All (n = 57) |
|---|---|---|---|
| n (%) | n (%) | n (%) | |
| Age (years) (mean ± SD) | 26.3 ± 4.3 | 27.9 ± 5.0 | 27.1 ± 4.7 |
| Country of birth | |||
| Australia | 28 (96.6) | 24 (85.7) | 52 (91.2) |
| Other | 1 (3.5) | 4 (14.3) | 5 (8.8) |
| Marital status | |||
| Never married | 15 (51.7) | 13 (46.4) | 28 (49.1) |
| Married/de facto | 13 (44.8) | 14 (50.0) | 27 (47.4) |
| Separated/divorced | 1 (3.5) | 1 (3.6) | 2 (3.5) |
| Currently studying | |||
| Full-time student | 9 (31.0) | 8 (28.6) | 17 (29.8) |
| Part-time student | 6 (20.7) | 6 (21.4) | 12 (21.1) |
| Not a student | 14 (48.3) | 14 (50.0) | 28 (49.1) |
| Highest education level completed | |||
| Higher university (e.g., Masters, PhD) | 3 (10.3) | 1 (3.6) | 4 (7.0) |
| University degree | 13 (44.8) | 7 (25.0) | 20 (25.1) |
| Certificate/diploma | 6 (20.7) | 9 (32.1) | 15 (26.3) |
| Trade/apprenticeship | 1 (3.5) | 1 (3.6) | 1 (3.5) |
| Currently studying for first degree | 6 (20.7) | 9 (32.1) | 15 (26.3) |
| None | 0 (0.0) | 1 (3.6) | 1 (1.8) |
| Individual income | |||
| Lower ($0–$299/week) | 9 (31.0) | 4 (14.3) | 13 (22.8) |
| Middle ($300–$999/week) | 9 (31.0) | 16 (57.1) | 25 (43.9) |
| Higher ($1000 or more/week | 11 (37.9) | 8 (28.6) | 19 (33.3) |
| Weight (kg) | 79.8 (10.0) | 79.2 (10.3) | 79.5 (10.1) |
| Body mass index (kg/m2) | 29.3 (2.5) | 29.4 (2.5) | 29.4 (2.5) |
| Body fat (kg) | 30.2 (7.5) | 30.1 (6.6) | 30.2 (7.0) |
| Body fat (%) | 37.5 (6.1) | 37.9 (5.4) | 37.7 (5.7) |
| Waist circumference (cm) | 88.8 (9.0) | 88.2 (8.0) | 88.5 (8.5) |
| Blood pressure | |||
| Systolic (mmHg) | 111.9 (10.6) | 112.8 (6.2) | 112.3 (8.7) |
| Diastolic (mmHg) | 73.8 (8.0) | 75.4 (8.4) | 74.6 (8.2) |
| Blood lipids | |||
| Total cholesterol (mmol/L) 1 | 5.0 (1.0) | 5.0 (0.9) | 5.0 (0.9) |
| LDL-C (mmol/L) 2,3 | 2.8 (0.9) | 2.9 (0.6) | 2.8 (0.8) |
| HDL-C (mmol/L) 2,4 | 1.5 (0.4) | 1.5 (0.4) | 1.5 (0.4) |
| Triglycerides (mmol/L) 1 | 1.2 (0.3) | 1.2 (0.6) | 1.2 (0.4) |
| Physical activity | |||
| MVPA minutes/week 5,6 | 243 (268) | 167 (164) | 208 (227) |
| Sitting time (minutes/day) 7 | |||
| Weekday | 598 (266) | 605 (268) | 602 (264) |
| Weekend day | 508 (227) | 521 (218) | 515 (221) |
| Average of days | 567 (217) | 579 (227) | 573 (220) |
| Dietary intake | |||
| Energy intake (kJ/day) | 9106 (3483) | 7840 (3828) | 8484 (3680) |
| Alcohol (% energy/day) | 0.4 (0.6) | 0.5 (1.1) | 0.5 (0.9) |
| Alcohol (grams/day) | 1.5 (1.6) | 1.3 (1.8) | 1.4 (1.7) |
| Take-away (% energy/day) | 5.3 (3.3) | 5.7 (3.6) | 5.5 (3.4) |
| Fruit (% energy/day) | 4.9 (4.4) | 4.8 (3.0) | 4.9 (3.7) |
| Fruit (grams/day) | 133.2 (71.3) | 127.3 (98.2) | 130.3 (84.9) |
| Vegetables (% energy/day) | 9.6 (4.0) | 9.8 (4.9) | 9.7 (4.4) |
| Vegetables (grams/day) | 427.5 (185.6) | 322.0 (199.8) | 375.7 (198.3) |
| Core foods (% energy/day) | 53.6 (13.6) | 56.3 (10.4) | 54.9 (12.1) |
| Non-core foods (% energy/day) | 46.3 (13.6) | 43.7 (10.4) | 45.0 (12.1) |
| Quality of life | |||
| QLESQ 8 total score | 46.5 (8.9) | 47.1 (8.2) | 46.8 (8.5) |
| Satisfaction with life scale | 22.6 (6.2) | 20.5 (6.6) | 21.5 (6.5) |
| Outcome | Mean Change from Baseline to Six Months (95% CI) | Mean Difference between Groups (95% CI) | Group * Time p-Value | Effect Size | |||
|---|---|---|---|---|---|---|---|
| Control (n = 28) | p-Value | Intervention (n = 29) | p-Value | ||||
| Weight (kg) 1 | 0.01 (−1.69, 1.70) | 0.996 | −1.94 (−3.59, −0.29) | 0.022 | −1.94 (−4.31, 0.42) | 0.107 | −0.19 |
| Weight (kg) 2 | 0.55 (−1.28, 2.37) | 0.557 | −2.04 (−4.07, −0.01) | 0.049 | −2.59 (−5.32, 0.14) | 0.063 | −0.26 |
| Body mass index (BMI) (kg/m2) | −0.01 (−0.57, 0.55) | 0.970 | 0.69 (−1.24, −1.38) | 0.014 | −0.68 (−1.47, 1.09) | 0.091 | −0.27 |
| Body fat (kg) | 0.75 (−1.00, 2.49) | 0.403 | −2.36 (−4.27, −0.44) | 0.016 | −3.10 (−5.69, 0.52) | 0.019 | −0.44 |
| Body fat (%) | 0.27 (−1.29, 1.83) | 0.733 | −1.73 (−3.46, 0.003) | 0.050 | −2.00 (−4.33, 0.33) | 0.093 | −0.35 |
| Waist circumference (cm) | −3.5 (−5.1, −1.9) | <0.001 | −4.9 (−6.6, −3.1) | <0.001 | −1.4 (−3.8, 1.0) | 0.259 | −0.16 |
| Systolic blood pressure (mmHg) | −1.3 (−3.9, 1.3) | 0.323 | −4.2 (−7.1, −1.3) | 0.004 | −2.9 (−6.8, 1.0) | 0.144 | −0.33 |
| Diastolic blood pressure (mmHg) | −1.2 (−3.4, 1.0) | 0.297 | −3.0 (−5.5, −0.9) | 0.015 | −1.9 (−5.1, 1.4) | 0.267 | −0.23 |
| Total cholesterol | −0.10 (−0.46, 0.25) | 0.573 | −0.49 (−0.86,−0.12) | 0.009 | −0.39 (−0.90, 0.12) | 0.136 | −0.43 |
| LDL-C 3 | −0.19 (−0.61, 0.24) | 0.391 | −0.34 (−0.67, 0.003) | 0.071 | −0.15 (−0.69, 0.39) | 0.581 | −0.19 |
| HDL-C 4 | 0.10 (−0.03, 0.23) | 0.127 | −0.13 (−0.27, 0.002) | 0.054 | −0.23 (−0.42, −0.05) | 0.015 | −0.58 |
| Triglycerides | −0.18 (−0.40, 0.04) | 0.114 | −0.05 (−0.28, 0.18) | 0.674 | 0.13 (−0.19, 0.45) | 0.427 | 0.33 |
| MVPA minutes/week 5 | 38 (−9, 165) | 0.560 | −20 (−141, 102) | 0.749 | −58 (−233, 118) | 0.521 | −0.25 |
| MPA minutes/week | 67 (−20, 153) | 0.132 | 11 (−72, 94) | 0.789 | −55 (−175, 65) | 0.366 | −0.43 |
| VPA minutes/week | −31 (−93, 30) | 0.312 | −32 (−91, 28) | 0.302 | 0.0 (−86, 85) | 1.000 | 0.00 |
| Sitting time weekday (minutes/day) | −57 (−158, 44) | 0.270 | −35 (−136, 67) | 0.502 | 22 (−121, 165) | 0.764 | 0.08 |
| Sitting time weekend (minutes/day) | −44 (−152, 64) | 0.427 | −61 (−166, 45) | 0.258 | −17 (−168, 134) | 0.824 | −0.08 |
| Total sitting time (minutes/day) | −53 (−139, 34) | 0.235 | −44 (−132, 44) | 0.325 | 9 (−115, 132) | 0.892 | 0.04 |
| Energy intake (kJ/day) | −106 (−1348, 1136) | 0.867 | −910 (−2100, 280) | 0.134 | −804 (−2524, 916) | 0.359 | −0.22 |
| Fruit (% energy/day) | −0.73 (−2.16, 0.71) | 0.323 | 0.75 (−0.63, 2.24) | 0.388 | 1.47 (−0.52, 3.47) | 0.148 | 0.40 |
| Fruit (grams/day) | 8.83 (−21.00, 38.67) | 0.562 | 30.49 (1.94, 59.03) | 0.036 | 21.65 (−19.64, 62.95) | 0.304 | 0.26 |
| Vegetable (% energy/day) | −1.74 (−3.55, 0.07) | 0.059 | 2.97 (1.23, 4.71) | <0.001 | 4.71 (−2.20, 7.22) | <0.001 | 1.07 |
| Vegetable (grams/day) | 12.86 (−39.47, 65.18) | 0.630 | 54.47 (4.46, 104.48) | 0.033 | 41.61 (−30.77, 113.99) | 0.260 | 0.21 |
| Alcohol (% energy/day) | 0.03 (−0.28, 0.35) | 0.842 | −0.13 (−0.43, 0.17) | 0.384 | −0.17 (−0.60, 0.27) | 0.456 | −0.19 |
| Alcohol (grams/day) | 0.35 (−0.12, 0.81) | 0.144 | −0.34 (−0.78, 0.11) | 0.135 | −0.69 (−1.33, 0.04) | 0.037 | −0.41 |
| Takeaway (% energy/day) | 0.02 (−1.18, 1.23) | 0.970 | −1.32 (−2.48, −0.16) | 0.025 | −1.34 (−3.01, 0.33) | 0.116 | −0.39 |
| % energy from non-core foods | 0.89 (−4.67, 6.45) | 0.754 | −8.34 (−13.68, −3.00) | 0.002 | −9.23 (−16.94, 1.52) | 0.019 | −0.76 |
| % energy from core foods | −0.89 (−6.47, 4.69) | 0.754 | 8.50 (3.10, 13.82) | 0.002 | 9.35 (1.61, 17.09) | 0.018 | 0.77 |
| QLESQ total score 6 | 2.10 (−1.27, 5.50) | 0.222 | 3.27 (−0.39, 6.59) | 0.053 | 1.17 (−3.57, 5.90) | 0.630 | 0.14 |
| Satisfaction with life scale | 0.69 (−1.18, 2.57) | 0.469 | 0.35 (−1.44, 2.14) | 0.700 | −0.34 (−2.94, 2.26) | 0.797 | −0.05 |
| Acceptability Measures 1 | Website | Website Quizzes | Website: Goal Setting | Self-Monitoring App | eNewsletter | Text Messages | Social Media |
|---|---|---|---|---|---|---|---|
| Useful information about healthy eating | 3.6 ± 0.8 | 3.5 ± 1.0 | N/A 2 | 3.5 ± 0.9 | 3.6 ± 0.7 | 3.4 ± 1.0 | 3.8 ± 0.7 |
| Useful information about exercise | 3.4 ± 0.7 | 3.3 ± 1.1 | N/A 2 | 3.2 ± 1.0 | 3.4 ± 0.7 | 3.2 ± 1.1 | 3.8 ± 0.6 |
| Useful information about weight loss | 3.4 ± 0.9 | 3.5 ± 0.9 | N/A 2 | 2.9 ± 1.2 | 3.6 ± 0.7 | 3.4 ± 1.1 | 3.7 ± 0.7 |
| Helped me attain my goals | 3.0 ± 1.1 | 3.1 ± 1.0 | 3.3 ± 1.1 | 3.4 ± 0.9 | 3.1 ± 0.9 | 2.8 ± 0.7 | 3.0 ± 0.8 |
| Motivated me | 2.9 ± 1.0 | 3.2 ± 1.0 | 3.4 ± 1.0 | 3.6 ± 1.0 | 3.2 ± 0.8 | 2.9 ± 0.8 | 3.2 ± 1.0 |
| Made me feel accountable | 3.1 ± 0.9 | 3.4 ± 1.0 | 3.5 ± 1.0 | 3.8 ± 0.9 | 3.2 ± 0.8 | 3.0 ± 0.8 | 3.3 ± 1.0 |
| Was easy to access | 3.4 ± 0.9 | 3.8 ± 0.9 | 3.9 ± 0.8 | 3.8 ± 0.8 | 3.8 ± 0.8 | 3.6 ± 1.0 | 4.0 ± 0.7 |
| Visually appealing | 3.4 ± 0.8 | 3.6 ± 1.0 | N/A 2 | 4.0 ± 0.5 | 3.9 ± 0.8 | 3.0 ± 0.9 | 4.0 ± 0.7 |
| Component satisfaction | 3.0 ± 1.0 | 3.4 ± 0.9 | 3.8 ± 0.7 | 3.8 ± 0.8 | 3.7 ± 0.8 | 3.5 ± 0.8 | 3.7 ± 0.8 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hutchesson, M.J.; Callister, R.; Morgan, P.J.; Pranata, I.; Clarke, E.D.; Skinner, G.; Ashton, L.M.; Whatnall, M.C.; Jones, M.; Oldmeadow, C.; et al. A Targeted and Tailored eHealth Weight Loss Program for Young Women: The Be Positive Be Healthe Randomized Controlled Trial. Healthcare 2018, 6, 39. https://doi.org/10.3390/healthcare6020039
Hutchesson MJ, Callister R, Morgan PJ, Pranata I, Clarke ED, Skinner G, Ashton LM, Whatnall MC, Jones M, Oldmeadow C, et al. A Targeted and Tailored eHealth Weight Loss Program for Young Women: The Be Positive Be Healthe Randomized Controlled Trial. Healthcare. 2018; 6(2):39. https://doi.org/10.3390/healthcare6020039
Chicago/Turabian StyleHutchesson, Melinda J., Robin Callister, Philip J. Morgan, Ilung Pranata, Erin D. Clarke, Geoff Skinner, Lee M. Ashton, Megan C. Whatnall, Mark Jones, Christopher Oldmeadow, and et al. 2018. "A Targeted and Tailored eHealth Weight Loss Program for Young Women: The Be Positive Be Healthe Randomized Controlled Trial" Healthcare 6, no. 2: 39. https://doi.org/10.3390/healthcare6020039