Reply to Comment—Osteonecrosis of the Jaw in Myeloma Patients Receiving Denosumab or Zoledronic Acid. Comment on Pivotal Trial by Raje et al. Published in Lancet Oncology


{kind=link}
1. There Was Higher Rate of Osteonecrosis of the Jaw (ONJ) Reported in the Multiple Myeloma Study Compared with Other Pivotal Trials (Despite Similar Drug Exposure)
2. How Many Patients Received Dental Procedures Overall, That Is, the Global Treated Population, and Their Reasons?
3. ONJ Cases May Have Been Overlooked Due to a Change in ONJ Criteria during the Trial; How Did This Change in Criteria Influence the Results?
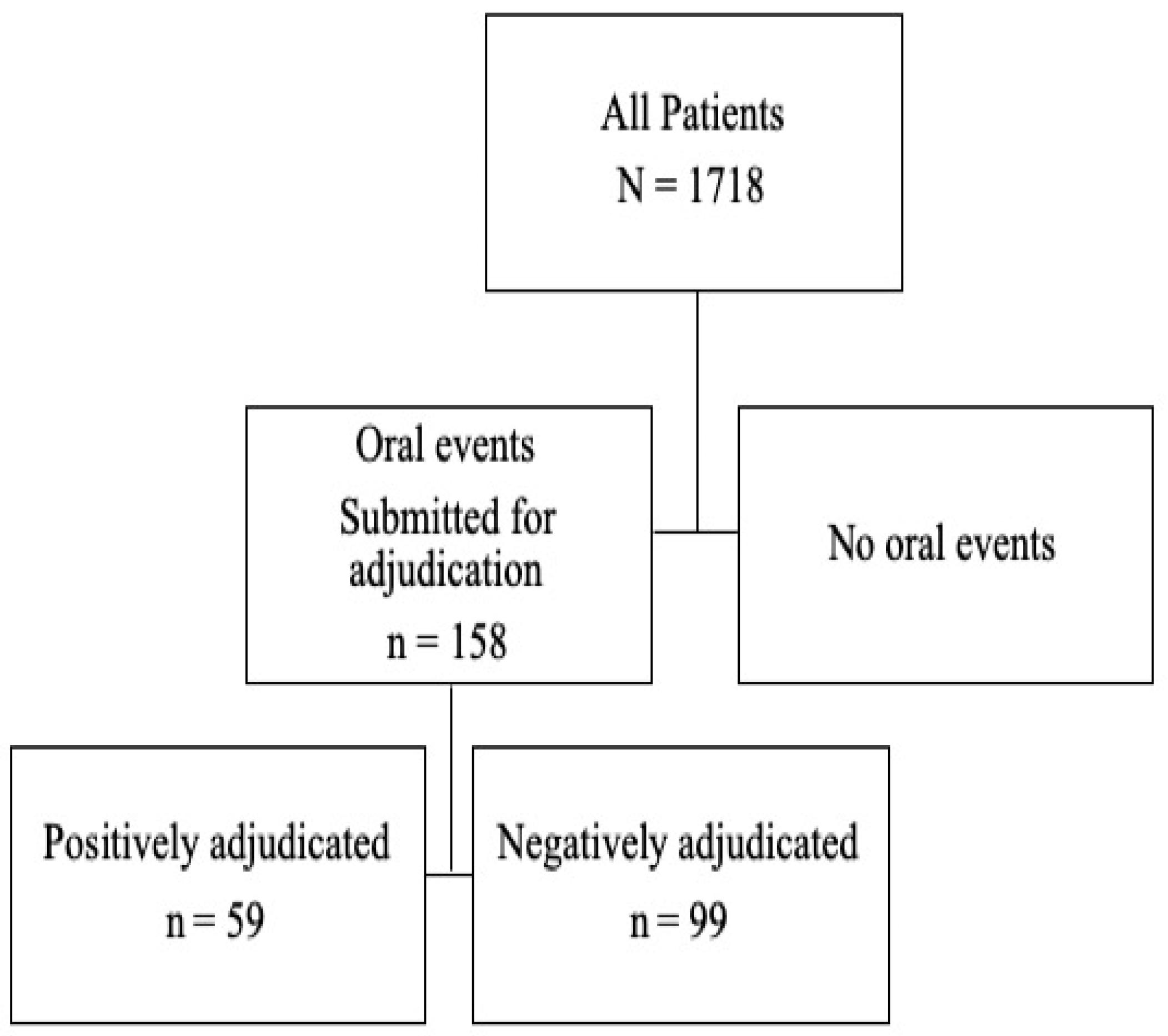
4. What Are the Numbers of “Potential” ONJ Cases Registered by Investigators, and Defined by the Presence of Clinical Signs and Symptoms Suggestive of ONJ, in Both Treatment Arms? Are These Rates Comparable to those from Another Solid Tumor Study (Saad et al., 2012) That Reported That Only One-Third of Potential ONJ Cases Were Adjudicated?
5. Long-Term ONJ Estimates from the Multiple Myeloma Trial Are Awaited with Interest
6. Reports on the Cost-Effectiveness of Denosumab Versus Zoledronic Acid in Myeloma Patients Are Needed
7. Summary
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fusco, V.; Campisi, G.; de Boissieu, P.; Monaco, F.; Baraldi, A.; Numico, G.; Bedogni, A. Osteonecrosis of the Jaw in Myeloma Patients Receiving Denosumab or Zoledronic Acid. A Commentary of the Pivotal Trial by Raje et al. Published on Lancet Oncology. Dent. J. 2018, 6, 42. [Google Scholar] [CrossRef] [PubMed]
- Raje, N.; Terpos, E.; Willenbacher, W.; Shimizu, K.; Garcia-Sanz, R.; Durie, B.; Legiec, W.; Krejci, M.; Laribi, K.; Zhu, L.; et al. Denosumab versus zoledronic acid in bone disease treatment of newly diagnosed multiple myeloma: An international, double-blind, double-dummy, randomised, controlled, phase 3 study. Lancet Oncol. 2018, 19, 370–381. [Google Scholar] [CrossRef]
- Henry, D.H.; Costa, L.; Goldwasser, F.; Hirsh, V.; Hungria, V.; Prausova, J.; Scagliotti, G.V.; Sleeboom, H.; Spencer, A.; Vadhan-Raj, S.; et al. Randomized, double-blind study of denosumab versus zoledronic acid in the treatment of bone metastases in patients with advanced cancer (excluding breast and prostate cancer) or multiple myeloma. J. Clin. Oncol. 2011, 29, 1125–1132. [Google Scholar] [CrossRef]
- Fizazi, K.; Carducci, M.; Smith, M.; Damiao, R.; Brown, J.; Karsh, L.; Milecki, P.; Shore, N.; Rader, M.; Wang, H.; et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: A randomised, double-blind study. Lancet 2011, 377, 813–822. [Google Scholar] [CrossRef]
- Stopeck, A.T.; Lipton, A.; Body, J.J.; Steger, G.G.; Tonkin, K.; de Boer, R.H.; Lichinitser, M.; Fujiwara, Y.; Yardley, D.A.; Viniegra, M.; et al. Denosumab compared with zoledronic acid for the treatment of bone metastases in patients with advanced breast cancer: A randomized, double-blind study. J. Clin. Oncol. 2010, 28, 5132–5139. [Google Scholar] [CrossRef] [PubMed]
- Saad, F.; Brown, J.E.; Van Poznak, C.; Ibrahim, T.; Stemmer, S.M.; Stopeck, A.T.; Diel, I.J.; Takahashi, S.; Shore, N.; Henry, D.H.; et al. Incidence, risk factors, and outcomes of osteonecrosis of the jaw: Integrated analysis from three blinded active-controlled phase III trials in cancer patients with bone metastases. Ann. Oncol. 2012, 23, 1341–1347. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.B.; Hellstein, J.W.; Kalmar, J.R. Narrative [corrected] review: Bisphosphonates and osteonecrosis of the jaws. Ann. Intern. Med. 2006, 144, 753–761. [Google Scholar] [CrossRef]
- King, A.E.; Umland, E.M. Osteonecrosis of the jaw in patients receiving intravenous or oral bisphosphonates. Pharmacotherapy 2008, 28, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Then, C.; Horauf, N.; Otto, S.; Pautke, C.; von Tresckow, E.; Rohnisch, T.; Baumann, P.; Schmidmaier, R.; Bumeder, I.; Oduncu, F.S. Incidence and risk factors of bisphosphonate-related osteonecrosis of the jaw in multiple myeloma patients having undergone autologous stem cell transplantation. Onkologie 2012, 35, 658–664. [Google Scholar] [CrossRef]
- Jackson, G.H.; Morgan, G.J.; Davies, F.E.; Wu, P.; Gregory, W.M.; Bell, S.E.; Szubert, A.J.; Navarro Coy, N.; Drayson, M.T.; Owen, R.G.; et al. Osteonecrosis of the jaw and renal safety in patients with newly diagnosed multiple myeloma: Medical Research Council Myeloma IX Study results. Br. J. Haematol. 2014, 166, 109–117. [Google Scholar] [CrossRef] [Green Version]
- Jadu, F.; Lee, L.; Pharoah, M.; Reece, D.; Wang, L. A retrospective study assessing the incidence, risk factors and comorbidities of pamidronate-related necrosis of the jaws in multiple myeloma patients. Ann. Oncol. 2007, 18, 2015–2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melea, P.I.; Melakopoulos, I.; Kastritis, E.; Tesseromatis, C.; Margaritis, V.; Dimopoulos, M.A.; Terpos, E. Conservative treatment of bisphosphonate-related osteonecrosis of the jaw in multiple myeloma patients. Int. J. Dent. 2014, 2014, 427273. [Google Scholar] [CrossRef]
- Bamias, A.; Kastritis, E.; Bamia, C.; Moulopoulos, L.A.; Melakopoulos, I.; Bozas, G.; Koutsoukou, V.; Gika, D.; Anagnostopoulos, A.; Papadimitriou, C.; et al. Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: Incidence and risk factors. J. Clin. Oncol. 2005, 23, 8580–8587. [Google Scholar] [CrossRef]
- Vahtsevanos, K.; Kyrgidis, A.; Verrou, E.; Katodritou, E.; Triaridis, S.; Andreadis, C.G.; Boukovinas, I.; Koloutsos, G.E.; Teleioudis, Z.; Kitikidou, K.; et al. Longitudinal cohort study of risk factors in cancer patients of bisphosphonate-related osteonecrosis of the jaw. J. Clin. Oncol. 2009, 27, 5356–5362. [Google Scholar] [CrossRef] [PubMed]
- Kos, M. Incidence and risk predictors for osteonecrosis of the jaw in cancer patients treated with intravenous bisphosphonates. Arch. Med. Sci. 2015, 11, 319–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarnbring, F.; Kashani, A.; Bjork, A.; Hoffman, T.; Krawiec, K.; Ljungman, P.; Lund, B. Role of intravenous dosage regimens of bisphosphonates in relation to other aetiological factors in the development of osteonecrosis of the jaws in patients with myeloma. Br. J. Oral Maxillofac. Surg. 2015, 53, 1007–1011. [Google Scholar] [CrossRef]
- Tsao, C.; Darby, I.; Ebeling, P.R.; Walsh, K.; O’Brien-Simpson, N.; Reynolds, E.; Borromeo, G. Oral health risk factors for bisphosphonate-associated jaw osteonecrosis. J. Oral Maxillofac. Surg. 2013, 71, 1360–1366. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F.; American Association of Oral and Maxillofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw—2014 update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef] [PubMed]
- Thumbigere-Math, V.; Tu, L.; Huckabay, S.; Dudek, A.Z.; Lunos, S.; Basi, D.L.; Hughes, P.J.; Leach, J.W.; Swenson, K.K.; Gopalakrishnan, R. A retrospective study evaluating frequency and risk factors of osteonecrosis of the jaw in 576 cancer patients receiving intravenous bisphosphonates. Am. J. Clin. Oncol. 2012, 35, 386–392. [Google Scholar] [CrossRef]
- XGEVA® (Denosumab) Prescribing Information; Amgen Inc.: Thousand Oaks, CA, USA, 2018.
- Amgen Inc. Data on file. Unpublished work.
- European Medicines Agency. XGEVA® Summary of product characteristics. In Denosumab; Amgen, Inc.: Breda, The Netherlands, 2015. [Google Scholar]
- Mucke, T.; Deppe, H.; Hein, J.; Wolff, K.D.; Mitchell, D.A.; Kesting, M.R.; Retz, M.; Gschwend, J.E.; Thalgott, M. Prevention of bisphosphonate-related osteonecrosis of the jaws in patients with prostate cancer treated with zoledronic acid—A prospective study over 6 years. J. Craniomaxillofac. Surg. 2016, 44, 1689–1693. [Google Scholar] [CrossRef] [PubMed]
- Raje, N.; Roodman, G.D.; Willenbacher, W.; Shimizu, K.; Garcia-Sanz, R.; Terpos, E.; Kennedy, L.; Sabatelli, L.; Intorcia, M.; Hechmati, G. A cost-effectiveness analysis of denosumab for the prevention of skeletal-related events in patients with multiple myeloma in the United States of America. J. Med. Econ. 2018, 21, 525–536. [Google Scholar] [CrossRef] [PubMed]

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raje, N.; Terpos, E.; Jandial, D.D. Reply to Comment—Osteonecrosis of the Jaw in Myeloma Patients Receiving Denosumab or Zoledronic Acid. Comment on Pivotal Trial by Raje et al. Published in Lancet Oncology. Dent. J. 2019, 7, 54. https://doi.org/10.3390/dj7020054
Raje N, Terpos E, Jandial DD. Reply to Comment—Osteonecrosis of the Jaw in Myeloma Patients Receiving Denosumab or Zoledronic Acid. Comment on Pivotal Trial by Raje et al. Published in Lancet Oncology. Dentistry Journal. 2019; 7(2):54. https://doi.org/10.3390/dj7020054
Chicago/Turabian StyleRaje, Noopur, Evangelos Terpos, and Danielle D. Jandial. 2019. "Reply to Comment—Osteonecrosis of the Jaw in Myeloma Patients Receiving Denosumab or Zoledronic Acid. Comment on Pivotal Trial by Raje et al. Published in Lancet Oncology" Dentistry Journal 7, no. 2: 54. https://doi.org/10.3390/dj7020054