A Novel Comprehensive Clinical Stratification Model to Refine Prognosis of Glioblastoma Patients Undergoing Surgical Resection

 , ,
, ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
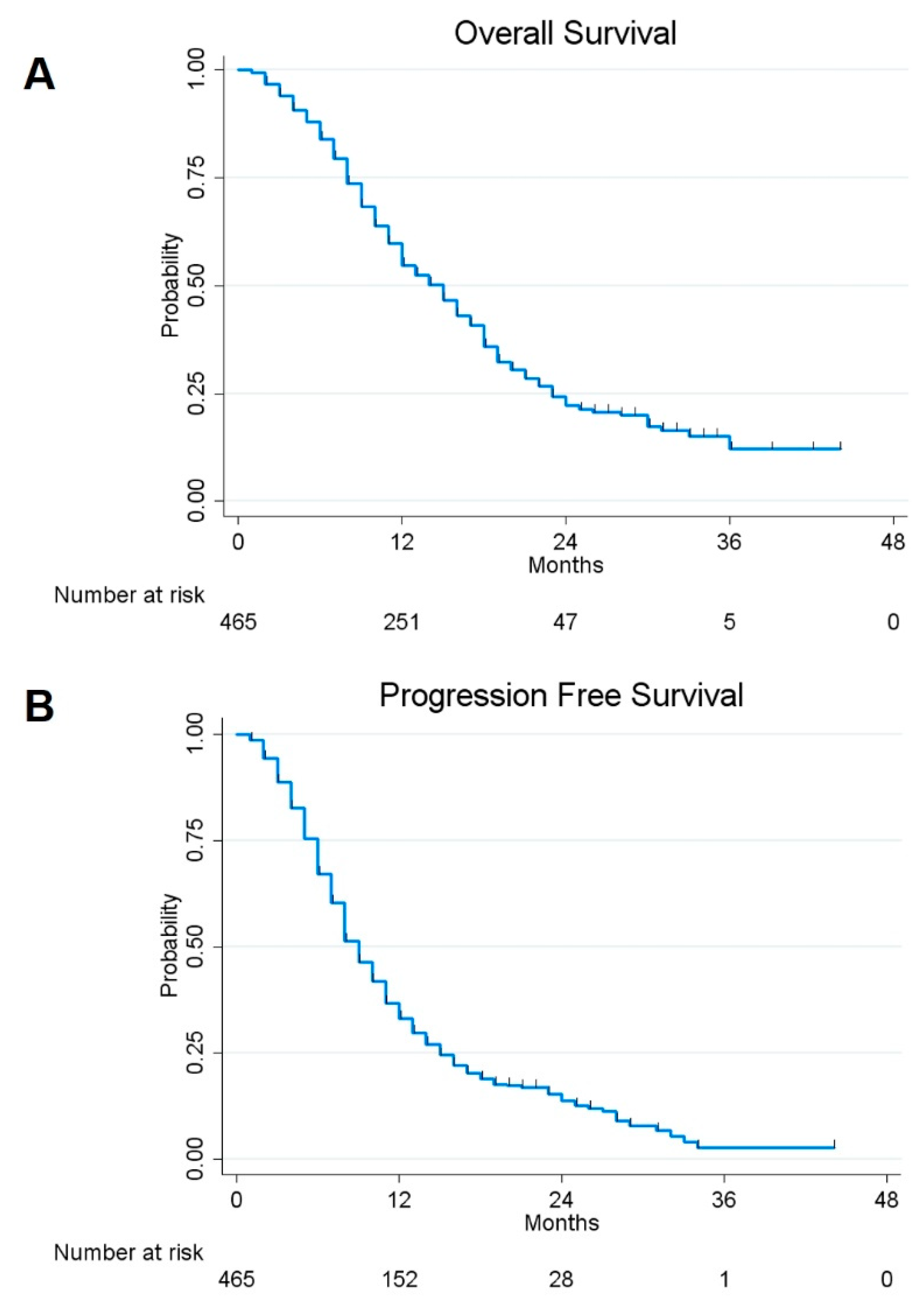
2.1. Survival Analysis and Risk Factors
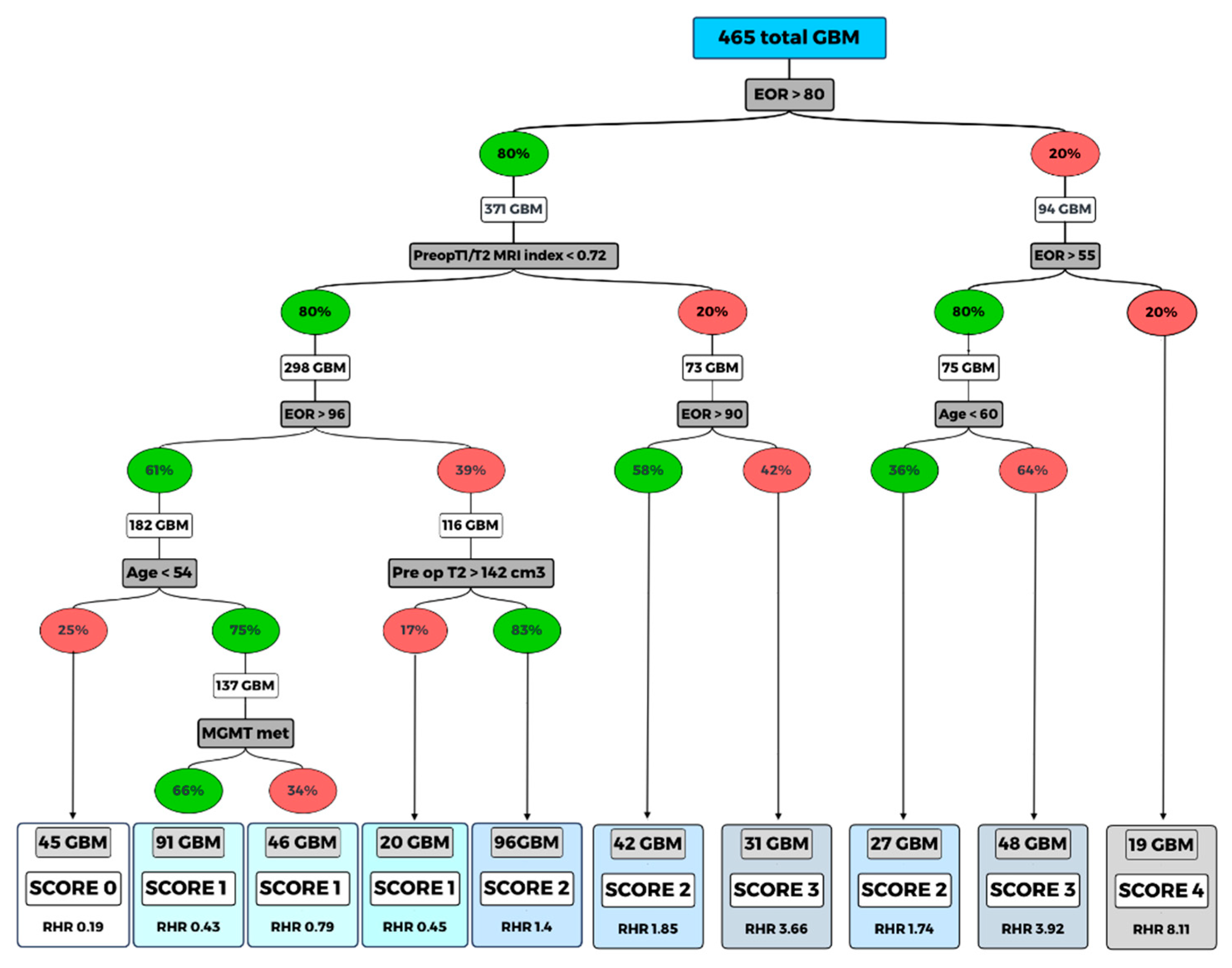
2.2. Classification and Regression Tree (CART) Model
2.3. Treatment at Tumor Progression
3. Discussion
4. Materials and Methods
4.1. Volumetric Analysis
4.2. Post-Operative Treatment
4.3. Statistical Analysis
4.4. Classification and Regression Tree (CART) Method
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Value (N and %, Mean ± Standard Deviation (SD) or Median and Range) |
|---|---|
| No. of patients | 465 |
| Age (years) | 63 (20–85) |
| Sex | |
| Female | 176 (37.85%) |
| Male | 289 (62.15%) |
| Side | |
| Left | 228 (49.03%) |
| Right | 237 (50.97%) |
| Tumor Site | |
| Precentral | 182 (39.14%) |
| Postcentral | 128 (27.53%) |
| Temporal + Insular | 155 (33.33%) |
| Intra-operative protocol | |
| CEUS + / 5-ALA + | 43 (9.25%) |
| CEUS - / 5-ALA + | 35 (7.53%) |
| CEUS + / 5-ALA - | 34 (7.31%) |
| CEUS - / 5-ALA - | 353 (75.91%) |
| Radiological Features | |
| Ependymal involvement (yes vs. no) | 143 vs. 322 (30.75% vs 69.25%) |
| Corpus Callosum involvement (yes vs. no) | 155 vs. 310 (33.33% vs 66.67%) |
| Necrotic-cystic component (yes vs. no) | 319 vs. 146 (68.60% vs 31.40%) |
| Midline shift (yes vs no) | 222 vs. 243 (47.74% vs 52.26%) |
| Preoperative Tumoral Volume computed on postcontrast T1-weighted images, cm3 | 31 (0.682–136) |
| Preoperative Tumoral Volume computed on T2-weighted images, cm3 | 65 (3–497) |
| Preoperative ΔT1/T2 MRI Index | 48.55 (1.13–100) |
| Residual tumor, cm3 | 0.959 (0–37.506) |
| EOR (continuous variable) | 95 (38–100) |
| EOR (categorical variable) | |
| EOR = 100% | 184 (39.57%) |
| 99% ≤ EOR ≤ 90% | 133 (28.6%) |
| 89% ≤ EOR ≤ 80% | 76 (16.34%) |
| EOR ≤ 79% | 72 (15.48%) |
| Biological Features | |
| MGMT methylation (yes vs no) | 290 vs. 175 (62.37% vs. 37.63%) |
| IDH 1/2 mutation (yes vs no) | 38 vs. 427 (8.17% vs. 91.83%) |
| Ki-67 | 25 (2-95) |
| Two-gene model | |
| MGMT met and IDH 1/2 mut | 27 (5.81%) |
| MGMT met and IDH 1/2 wt | 263 (56.56%) |
| MGMT unmet and IDH 1/2 mut | 10 (2.15%) |
| MGMT unmet and IDH 1/2 wt | 165 (35.48%) |
| Postoperative Protocol | |
| Stupp protocol | 345 (74.2%) |
| Stupp protocol + CWs | 60 (12.9 %) |
| Stupp interrupted for side effects | 60 (12.9 %) |
| Value (N and %, Mean ± SD or Median and Range) | |
|---|---|
| Clinical presentation | |
| No deficits | 41 (8.82%) |
| Not-specific symptoms (headache, nausea, vomiting, disorientation etc.) | 165 (35.48%) |
| Motor deficits | 89 (19.14%) |
| Sensory deficits | 16 (3.44%) |
| Visual/speech deficits | 66 (14.19%) |
| Seizures | 88 (18.92%) |
| Post-operative course | |
| No deficits | 263 (56.56%) |
| Not-specific symptoms (headache, nausea, vomiting, disorientation etc.) | 64 (13.76%) |
| Motor deficits | 80 (17.20%) |
| Sensory deficits | 3 (0.65%) |
| Visual/speech deficits | 52 (11.18%) |
| Seizures | 3 (0.65%) |
| 6-monts follow-up (in 394 pts alive) | |
| No deficits | 245 (62.18%) |
| Not-specific symptoms (headache, nausea, vomiting, disorientation etc.) | 94 (23.86%) |
| Motor deficits | 35 (8.88%) |
| Sensory deficits | 1 (0.25%) |
| Visual/speech deficits | 17 (4.31%) |
| Seizures | 2 (0.51%) |
| KPS | |
| Pre-operative | 90 (50–100) |
| Immediate post-operative | 90 (50–100) |
| 6-monts follow-up (in 394 pts alive) | 90 (50–100) |
| OS (alive vs dead) | 158 vs. 307 (33.98% vs. 66.02%) |
| OS at 1-year follow-up | 54.78% |
| OS at 2-year follow-up | 22.28% |
| PFS (no recurrence vs recurrence) | 96 vs. 369 (20.65% vs. 79.35%) |
| PFS at 1 year follow-up | 33.05% |
| PFS at 2 year follow-up | 13.82% |
References
- Guden, M.; Ayata, H.B.; Ceylan, C.; Kilic, A.; Engin, K. Prognostic factors effective on survival of patients with glioblastoma: Anadolu Medical Center experience. Indian J. Cancer 2016, 53, 382–386. [Google Scholar]
- Nam, J.Y.; De Groot, J.F. Treatment of Glioblastoma. J. Oncol. Pr. 2017, 13, 629–638. [Google Scholar] [CrossRef] [PubMed]
- Ohgaki, H. Epidemiology of Brain Tumors. Methods Mol. Biol. 2009, 472, 323–342. [Google Scholar] [PubMed]
- Weller, M.; Bent, M.V.D.; Hopkins, K.; Tonn, J.C.; Stupp, R.; Falini, A.; Cohen-Jonathan-Moyal, E.; Frappaz, D.; Henriksson, R.; Balaña, C.; et al. EANO guideline for the diagnosis and treatment of anaplastic gliomas and glioblastoma. Lancet Oncol. 2014, 15, 395–403. [Google Scholar] [CrossRef] [Green Version]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Brada, M.; Bent, M.J.V.D.; Tonn, J.-C.; Pentheroudakis, G. High-grade glioma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Hegi, M.E.; Gorlia, T.; Erridge, S.C.; Perry, J.; Hong, Y.-K.; Aldape, K.D.; Lhermitte, B.; Pietsch, T.; Grujicic, D.; et al. Cilengitide combined with standard treatment for patients with newly diagnosed glioblastoma with methylated MGMT promoter (CENTRIC EORTC 26071-22072 study): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2014, 15, 1100–1108. [Google Scholar] [CrossRef] [Green Version]
- Sanai, N.; Berger, M. Extent of resection influences outcomes for patients with gliomas. Rev. Neurol. 2011, 167, 648–654. [Google Scholar] [CrossRef]
- Lacroix, M.; Abi-Said, D.; Fourney, D.R.; Gokaslan, Z.L.; Shi, W.; Demonte, F.; Lang, F.F.; McCutcheon, I.E.; Hassenbusch, S.J.; Holland, E.; et al. A multivariate analysis of 416 patients with glioblastoma multiforme: Prognosis, extent of resection, and survival. J. Neurosurg. 2001, 95, 190–198. [Google Scholar] [CrossRef] [Green Version]
- McGirt, M.J.; Than, K.D.; Weingart, J.D.; Chaichana, K.L.; Attenello, F.J.; Olivi, A.; Laterra, J.; Kleinberg, L.R.; Grossman, S.A.; Brem, H.; et al. Gliadel (BCNU) wafer plus concomitant temozolomide therapy after primary resection of glioblastoma multiforme. J. Neurosurg. 2009, 110, 583–588. [Google Scholar] [CrossRef]
- Chaudhry, N.S.; Shah, A.H.; Ferraro, N.; Snelling, B.M.; Bregy, A.; Madhavan, K.; Komotar, R.J. Predictors of long-term survival in patients with glioblastoma multiforme: Advancements from the last quarter century. Cancer Invest. 2013, 31, 287–308. [Google Scholar] [CrossRef]
- Wijnenga, M.M.J.; French, P.J.; Dubbink, H.J.; Dinjens, W.N.M.; Atmodimedjo, P.N.; Kros, J.M.; Smits, M.; Gahrmann, R.; Rutten, G.J.; Verheul, J.B.; et al. The impact of surgery in molecularly defined low-grade glioma: An integrated clinical, radiological, and molecular analysis. Neuro Oncol. 2018, 20, 103–112. [Google Scholar] [CrossRef] [Green Version]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, J.P.; Aboagye, E.O.; Adams, J.E.; Aerts, H.J.; Barrington, S.F.; Beer, A.J.; Boellaard, R.; Bohndiek, S.E.; Brady, M.; Brown, G.; et al. Imaging biomarker roadmap for cancer studies. Nat. Rev. Clin. Oncol. 2017, 14, 169–186. [Google Scholar] [CrossRef] [PubMed]
- Gittleman, H.; Lim, D.; Kattan, M.W.; Chakravarti, A.; Gilbert, M.R.; Lassman, A.B.; Lo, S.S.; Machtay, M.; Sloan, A.E.; Sulman, E.P.; et al. An independently validated nomogram for individualized estimation of survival among patients with newly diagnosed glioblastoma: NRG Oncology RTOG 0525 and 0825. Neuro-Oncology 2016, 19, 669–677. [Google Scholar]
- Brown, T.J.; Brennan, M.C.; Li, M.; Church, E.W.; Brandmeir, N.J.; Rakszawski, K.L.; Patel, A.S.; Rizk, E.B.; Suki, D.; Sawaya, R.; et al. Association of the Extent of Resection With Survival in Glioblastoma: A Systematic Review and Meta-analysis. JAMA Oncol. 2016, 2, 1460–1469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahman, M.; Abbatematteo, J.; De Leo, E.K.; Kubilis, P.S.; Vaziri, S.; Bova, F.; Sayour, E.; Mitchell, D.; Quinones-Hinojosa, A. The effects of new or worsened postoperative neurological deficits on survival of patients with glioblastoma. J. Neurosurg. 2017, 127, 123–131. [Google Scholar] [CrossRef]
- Chaichana, K.L.; Cabrera-Aldana, E.E.; Jusue-Torres, I.; Wijesekera, O.; Olivi, A.; Rahman, M.; Quiñones-Hinojosa, A. When Gross Total Resection of a Glioblastoma Is Possible, How Much Resection Should Be Achieved? World Neurosurg. 2014, 82, 257–265. [Google Scholar] [CrossRef]
- Awad, A.-W.; Karsy, M.; Sanai, N.; Spetzler, R.; Zhang, Y.; Xu, Y.; Mahan, M.A. Impact of removed tumor volume and location on patient outcome in glioblastoma. J. Neuro-Oncol. 2017, 135, 161–171. [Google Scholar] [CrossRef]
- Ng, K.; Kim, R.; Kesari, S.; Carter, B.; Chen, C.C. Genomic profiling of glioblastoma: Convergence of fundamental biologic tenets and novel insights. J. Neurooncol. 2012, 107, 1–12. [Google Scholar] [CrossRef]
- Weller, M.; Felsberg, J.; Hartmann, C.; Berger, H.; Steinbach, J.P.; Schramm, J.; Westphal, M.; Schackert, G.; Simon, M.; Tonn, J.C.; et al. Molecular Predictors of Progression-Free and Overall Survival in Patients With Newly Diagnosed Glioblastoma: A Prospective Translational Study of the German Glioma Network. J. Clin. Oncol. 2009, 27, 5743–5750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gessler, F.; Bernstock, J.D.; Braczynski, A.; Lescher, S.; Baumgarten, P.; Harter, P.N.; Mittelbronn, M.; Wu, T.; Seifert, V.; Senft, C. Surgery for Glioblastoma in Light of Molecular Markers: Impact of Resection and MGMT Promoter Methylation in Newly Diagnosed IDH-1 Wild-Type Glioblastomas. Neurosurgery 2019, 84, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Mampre, D.; Ehresman, J.; Pinilla-Monsalve, G.; Osorio, M.A.G.; Olivi, A.; Quinones-Hinojosa, A.; Chaichana, K.L. Extending the resection beyond the contrast-enhancement for glioblastoma: Feasibility, efficacy, and outcomes. Br. J. Neurosurg. 2018, 32, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Grabowski, M.M.; Recinos, P.F.; Nowacki, A.S.; Schroeder, J.L.; Angelov, L.; Barnett, G.H.; Vogelbaum, M.A. Residual tumor volume versus extent of resection: Predictors of survival after surgery for glioblastoma. J. Neurosurg. 2014, 121, 1115–1123. [Google Scholar] [CrossRef] [PubMed]
- Chaichana, K.L.; Jusue-Torres, I.; Navarro-Ramirez, R.; Raza, S.M.; Pascual-Gallego, M.; Ibrahim, A.; Hernandez-Hermann, M.; Gomez, L.; Ye, X.; Weingart, J.D.; et al. Establishing percent resection and residual volume thresholds affecting survival and recurrence for patients with newly diagnosed intracranial glioblastoma. Neuro-Oncology 2014, 16, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Coburger, J.; Hagel, V.; Wirtz, C.R.; König, R. Surgery for Glioblastoma: Impact of the Combined Use of 5-Aminolevulinic Acid and Intraoperative MRI on Extent of Resection and Survival. PLoS ONE 2015, 10, e0131872. [Google Scholar] [CrossRef] [Green Version]
- Cordova, J.S.; Gurbani, S.S.; Holder, C.A.; Olson, J.J.; Schreibmann, E.; Shi, R.; Guo, Y.; Shu, H.-K.G.; Shim, H.; Hadjipanayis, C.G. Semi-Automated Volumetric and Morphological Assessment of Glioblastoma Resection with Fluorescence-Guided Surgery. Mol. Imaging Boil. 2016, 18, 454–462. [Google Scholar] [CrossRef] [Green Version]
- Suchorska, B.; Weller, M.; Tabatabai, G.; Senft, C.; Hau, P.; Sabel, M.C.; Herrlinger, U.; Ketter, R.; Schlegel, U.; Marosi, C.; et al. Complete resection of contrast-enhancing tumor volume is associated with improved survival in recurrent glioblastoma—Results from the DIRECTOR trial. Neuro-Oncology 2016, 18, 549–556. [Google Scholar] [CrossRef]
- Grossman, R.; Shimony, N.; Shir, D.; Gonen, T.; Sitt, R.; Kimchi, T.J.; Harosh, C.B.; Ram, Z. Dynamics of FLAIR Volume Changes in Glioblastoma and Prediction of Survival. Ann. Surg. Oncol. 2017, 24, 794–800. [Google Scholar] [CrossRef]
- Fukui, A.; Muragaki, Y.; Saito, T.; Maruyama, T.; Nitta, M.; Ikuta, S.; Kawamata, T. Volumetric Analysis Using Low-Field Intraoperative Magnetic Resonance Imaging for 168 Newly Diagnosed Supratentorial Glioblastomas: Effects of Extent of Resection and Residual Tumor Volume on Survival and Recurrence. World Neurosurg. 2017, 98, 73–80. [Google Scholar] [CrossRef]
- Eseonu, C.I.; Refaey, K.; Garcia, O.; Raghuraman, G.; Quinones-Hinojosa, A. Volumetric Analysis of Extent of Resection, Survival, and Surgical Outcomes for Insular Gliomas. World Neurosurg. 2017, 103, 265–274. [Google Scholar] [CrossRef]
- Henker, C.; Kriesen, T.; Glass, Ä.; Schneider, B.; Piek, J. Volumetric quantification of glioblastoma: Experiences with different measurement techniques and impact on survival. J. Neuro-Oncol. 2017, 135, 391–402. [Google Scholar] [CrossRef]
- Coburger, J.; Segovia, J.; Ganslandt, O.; Ringel, F.; Wirtz, C.R.; Renovanz, M. Counseling Patients with a Glioblastoma Amenable Only for Subtotal Resection: Results of a Multicenter Retrospective Assessment of Survival and Neurologic Outcome. World Neurosurg. 2018, 114, 1180–1185. [Google Scholar] [CrossRef]
- Zacharaki, E.; Morita, N.; Bhatt, P.; O’Rourke, D.; Melhem, E.R.; Davatzikos, C. Survival analysis of patients with high-grade gliomas based on data mining of imaging variables. Am. J. Neuroradiol. 2012, 33, 1065–1071. [Google Scholar] [CrossRef] [PubMed]
- Ganggayah, M.D.; Taib, N.A.; Har, Y.C.; Lio, P.; Dhillon, S.K. Predicting factors for survival of breast cancer patients using machine learning techniques. BMC Med. Inform. Decis. Mak. 2019, 19, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sudhamathy, G.; Thilagu, M.; Padmavathi, G. Comparative analysis of R package classifiers using breast cancer dataset. Int. J. Eng. Technol. 2016, 8, 2127–2136. [Google Scholar]
- Chen, W.; Xie, X.; Wang, J.; Pradhan, B.; Hong, H.; Bui, D.T.; Duan, Z.; Ma, J. A comparative study of logistic model tree, random forest, and classification and regression tree models for spatial prediction of landslide susceptibility. CATENA 2017, 151, 147–160. [Google Scholar] [CrossRef] [Green Version]
- Muchlinski, D.; Siroky, D.; He, J.; Kocher, M. Comparing Random Forest with Logistic Regression for Predicting Class-Imbalanced Civil War Onset Data. Polit. Anal. 2016, 24, 87–103. [Google Scholar] [CrossRef]
- Ahmadipour, Y.; Jabbarli, R.; Gembruch, O.; Pierscianek, D.; Darkwah Oppong, M.; Dammann, P.; Wrede, K.; Özkan, N.; Müller, O.; Sure, U.; et al. Impact of Multifocality and Molecular Markers on Survival of Glioblastoma. World Neurosurg. 2019, 122, 461–466. [Google Scholar] [CrossRef]
- Molenaar, R.J.; Verbaan, D.; Lamba, S.; Zanon, C.; Jeuken, J.W.; Boots-Sprenger, S.H.; Wesseling, P.; Hulsebos, T.J.; Troost, D.; Van Tilborg, A.A.; et al. The combination of IDH1 mutations and MGMT methylation status predicts survival in glioblastoma better than either IDH1 or MGMT alone. Neuro-Oncology 2014, 16, 1263–1273. [Google Scholar] [CrossRef]
- Wee, C.W.; Kim, E.; Kim, I.H.; Kim, I.A.; Kim, N.; Suh, C.O. Novel Recursive Partitioning Analysis Classification for Newly Diagnosed Glioblastoma: A Multi-institutional Study Highlighting the MGMT Promoter Methylation and IDH1 Gene Mutation Status. Radiother. Oncol. 2017, 123, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Minniti, G.; Lombardi, G.; Paolini, S. Glioblastoma in Elderly Patients: Current Management and Future Perspectives. Cancers 2019, 11, 336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunha, M.L.V.D.; Esmeraldo, A.C.S.; Henriques, L.A.W.; Santos, M.A.M.D.J.; Medeiros, R.T.R.; Botelho, R.V. Elderly patients with glioblastoma: The impact of surgical resection extent on survival. Rev. Assoc. Med. Bras. 2019, 65, 937–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, S.; Meyer, F.B.; Buckner, J.C.; Uhm, J.H.; Yan, E.S.; Parney, I.F. Presentation, management, and outcome of newly diagnosed glioblastoma in elderly patients. J. Neurosurg. 2012, 118, 786–798. [Google Scholar] [CrossRef]
- Ius, T.; Pignotti, F.; Della Pepa, G.M.; Bagatto, D.; Isola, M.; Battistella, C.; Gaudino, S.; Pegolo, E.; Chiesa, S.; Arcicasa, M.; et al. Glioblastoma: From volumetric analysis to molecular predictors. J. Neurosurg. Sci. 2020, in press. [Google Scholar]
- Gorlia, T.; Stupp, R.; Brandes, A.A.; Rampling, R.R.; Fumoleau, P.; Dittrich, C.; Campone, M.M.; Twelves, C.C.; Raymond, E.; Hegi, M.E.; et al. New prognostic factors and calculators for outcome prediction in patients with recurrent glioblastoma: A pooled analysis of EORTC Brain Tumour Group phase I and II clinical trials. Eur. J. Cancer 2012, 48, 1176–1184. [Google Scholar] [CrossRef]
- Roy, S.; Lahiri, D.; Maji, T.; Biswas, J. Recurrent Glioblastoma: Where we stand. South Asian J. Cancer 2015, 4, 163–173. [Google Scholar] [CrossRef]
- Zhao, Y.-H.; Wang, Z.-F.; Pan, Z.-Y.; Péus, D.; Delgado-Fernandez, J.; Pallud, J.; Li, Z.-Q. A Meta-Analysis of Survival Outcomes Following Reoperation in Recurrent Glioblastoma: Time to Consider the Timing of Reoperation. Front. Neurol. 2019, 10, 286. [Google Scholar] [CrossRef] [Green Version]
- Chaul-Barbosa, C.; Marques, D.F. How We Treat Recurrent Glioblastoma Today and Current Evidence. Curr. Oncol. Rep. 2019, 21, 94. [Google Scholar] [CrossRef]
- Azoulay, M.; Santos, F.; Shenouda, G.; Petrecca, K.; Oweida, A.; Guiot, M.C.; Owen, S.; Panet-Raymond, V.; Souhami, L.; Abdulkarim, B.S. Benefit of re-operation and salvage therapies for recurrent glioblastoma multiforme: Results from a single institution. J. Neuro-Oncol. 2017, 97, 377–426. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, M.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preusser, M.; Berghoff, A.S.; Manzl, C.; Filipits, M.; Weinhäusel, A.; Pulverer, W.; Dieckmann, K.; Widhalm, G.; Wöhrer, A.; Knosp, E.; et al. Clinical Neuropathology practice news 1-2014: Pyrosequencing meets clinical and analytical performance criteria for routine testing of MGMT promoter methylation status in glioblastoma. Clin. Neuropathol. 2014, 33, 6–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ius, T.; Angelini, E.; De Schotten, M.T.; Mandonnet, E.; Duffau, H. Evidence for potentials and limitations of brain plasticity using an atlas of functional resectability of WHO grade II gliomas: Towards a “minimal common brain”. Neuroimage 2011, 56, 992–1000. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.S.; Chang, E.F.; Lamborn, K.R.; Chang, S.M.; Prados, M.D.; Cha, S.; Tihan, T.; Vandenberg, S.; McDermott, M.W.; Berger, M.S. Role of Extent of Resection in the Long-Term Outcome of Low-Grade Hemispheric Gliomas. J. Clin. Oncol. 2008, 26, 1338–1345. [Google Scholar] [CrossRef] [PubMed]
- Breiman, L.; Friedman, J.H.; Olshen, R.A.; Stone, C.J. Classification Regression Trees; Wadsworth International Group: Belmont, CA, USA, 1984. [Google Scholar]
- Yohannes, Y.; Hoddinott, J. Classification and Regression Tree: An Introduction; International Food Policy Research Institute: Washington, DC, USA, 1999. [Google Scholar]
- Schmid, M.; Wright, M.N.; Ziegler, A. On the use of Harrell’s C for clinical risk prediction via random survival forests. Expert Syst. Appl. 2016, 63, 450–459. [Google Scholar] [CrossRef] [Green Version]




| Variable | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value | |
| Age (yrs) | 1.029 | 1.018–1.040 | 0.000 | 1.028 | 1.017–1.039 | 0.000 |
| Sex | ||||||
| Male | 1 | |||||
| Female | 0.900 | 0.713–1.137 | 0.377 | |||
| Side | ||||||
| Left | 1 | |||||
| Right | 1.124 | 0.898–1.406 | 0.308 | |||
| Tumor Site | ||||||
| Precentral | 1 | |||||
| Retrocentral | 1.092 | 0.825–1.446 | 0.539 | 0.954 | 0.718–1.267 | 0.745 |
| Temporal + Insular | 1.250 | 0.961–1.626 | 0.097 | 1.286 | 0.986–1.677 | 0.063 |
| Radiological Features | ||||||
| Ependymal involvement (yes vs no) | 1.135 | 0.890–1.448 | 0.309 | |||
| Corpus Callosum involvement (yes vs no) | 1.012 | 0.799–1.281 | 0.922 | |||
| Necrotic-cystic component (yes vs no) | 0.923 | 0.725–1.176 | 0.517 | |||
| Midline shift (yes vs no) | 0.970 | 0.775–1.214 | 0.789 | |||
| Preoperative Tumoral Volume computed on postcontrast T1-weighted images, cm3 | 1.001 | 0.996–1.006 | 0.652 | |||
| Preoperative Tumoral Volume computed on T2-weighted images, cm3 | 0.993 | 0.991–0.995 | 0.000 | 0.997 | 0.995–1.000 | 0.058 |
| Preoperative ΔT1/T2 MRI Index | 1.022 | 1.017–1.026 | 0.000 | 1.016 | 1.009–1.022 | 0.000 |
| Residual tumor, cm3 | 1.085 | 1.067–1.103 | 0.000 | 0.962 | 0.925–1.000 | 0.053 |
| EOR (continuous variable) | 0.946 | 0.938–0.954 | 0.000 | 0.937 | 0.923–0.950 | 0.000 |
| EOR (categorical variable) | ||||||
| EOR = 100% | 1 | |||||
| 99% ≤ EOR ≤ 90% | 1.755 | 1.314–2.343 | 0.000 | |||
| 89% ≤ EOR ≤ 80% | 2.477 | 1.757–3.492 | 0.000 | |||
| EOR ≤ 79% | 6.300 | 4.537–8.748 | 0.000 | |||
| Biological Features | ||||||
| MGMT promoter methylation (yes vs no) | 0.605 | 0.482–0.760 | 0.000 | 0.606 | 0.480–0.765 | 0.000 |
| IDH 1/2 mutation (yes vs no) | 0.638 | 0.423–0.964 | 0.033 | 0.925 | 0.605–1.416 | 0.721 |
| Ki67 | 1.001 | 0.995–1.007 | 0.725 | |||
| Variable | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value | |
| Age (yrs) | 1.017 | 1.008–1.027 | 0.000 | 1.015 | 1.006–1.024 | 0.002 |
| Sex | ||||||
| Male | 1 | |||||
| Female | 0.851 | 0.687–1.054 | 0.140 | |||
| Side | ||||||
| Left | 1 | |||||
| Right | 1.091 | 0.889–1.339 | 0.404 | |||
| Tumor Site | ||||||
| Precentral | 1 | |||||
| Retrocentral | 1.045 | 0.811–1.347 | 0.733 | |||
| Temporal + Insular | 1.031 | 0.810–1.312 | 0.806 | |||
| Radiological Features | ||||||
| Ependymal involvement (yes vs no) | 1.114 | 0.893–1.390 | 0.338 | |||
| Corpus Callosum involvement (yes vs no) | 0.917 | 0.737–1.142 | 0.439 | |||
| Necrotic-cystic component (yes vs no) | 0.974 | 0.781–1.215 | 0.816 | |||
| Midline shift (yes vs no) | 0.979 | 0.797–1.202 | 0.838 | |||
| Preoperative Tumoral Volume computed on postcontrast T1-weighted images, cm3 | 1.003 | 0.999–1.008 | 0.170 | |||
| Preoperative Tumoral Volume computed on T2-weighted images, cm3 | 0.996 | 0.994–0.998 | 0.000 | 0.999 | 0.996–1.001 | 0.311 |
| Preoperative ΔT1/T2 MRI Index | 1.016 | 1.012–1.020 | 0.000 | 1.011 | 1.005–1.016 | 0.000 |
| Residual tumor, cm3 | 1.083 | 1.067–1.100 | 0.000 | 0.977 | 0.943–1.013 | 0.208 |
| EOR (continuous variable) | 0.949 | 0.942–0.957 | 0.000 | 0.948 | 0.935–0.961 | 0.000 |
| EOR (categorical variable) | ||||||
| EOR = 100% | 1 | |||||
| 99% ≤ EOR ≤ 90% | 1.622 | 1.254-2.098 | 0.000 | |||
| 89% ≤ EOR ≤ 80% | 2.425 | 1.783-3.298 | 0.000 | |||
| EOR ≤ 79% | 5.245 | 3.854-7.138 | 0.000 | |||
| Biological Features | ||||||
| MGMT promoter methylation (yes vs no) | 0.639 | 0.518-0.787 | 0.000 | 0.673 | 0.544-0.833 | 0.000 |
| IDH 1/2 mutation (yes vs no) | 0.706 | 0.488-1.023 | 0.066 | 0.894 | 0.612-1.305 | 0.561 |
| Ki67 | 1.000 | 0.995-1.006 | 0.873 | |||
| Score | Variables | OS% (95% CI) | HR (95%CI) | p-Value |
|---|---|---|---|---|
| 0 | Preoperative ΔT1/T2 MRI Index < 0.72; EOR > 96%; Age < 53 | 92.24 (77.82–97.43) | 1 | - |
| 1 | Preoperative ΔT1/T2 MRI Index < 0.72; EOR > 96%; Age > 53 | 84.36 (77.39–89.33) | 2.6 (1.4–5.0) | 0.003 |
| Preoperative ΔT1/T2 MRI Index < 0.72; EOR: 81%–95%; Preop T2-w vol > 147 cm3 | ||||
| 2 | Preoperative ΔT1/T2 MRI Index < 0.72; EOR: 81%–95%; Preop T2-w vol < 147cm3 | 43.85 (35.94–51.48) | 9.6 (5.1–18.3) | 0.000 |
| Preoperative ΔT1/T2 MRI Index > 0.72; EOR >91% | ||||
| EOR: 56%–80%; Age < 59 | ||||
| 3 | Preoperative ΔT1/T2 MRI Index > 0.72; EOR 81%–90% | 11.58 (5.69–19.76) | 28.1 (14.4–54.7) | 0.000 |
| EOR: 56%–80%; age > 60 | ||||
| 4 | EOR < 55% | 5.26 (0.36–21.43) | 85.4 (38.5–189.3) | 0.000 |
| GAPS Score | 1-Year Estimated PFS |
|---|---|
| Score 0 | 65.60% |
| Score 1 | 55.54% |
| Score 2 | 13.09% |
| Score 3–4 | 3.93% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ius, T.; Pignotti, F.; Della Pepa, G.M.; La Rocca, G.; Somma, T.; Isola, M.; Battistella, C.; Gaudino, S.; Polano, M.; Dal Bo, M.; et al. A Novel Comprehensive Clinical Stratification Model to Refine Prognosis of Glioblastoma Patients Undergoing Surgical Resection. Cancers 2020, 12, 386. https://doi.org/10.3390/cancers12020386
Ius T, Pignotti F, Della Pepa GM, La Rocca G, Somma T, Isola M, Battistella C, Gaudino S, Polano M, Dal Bo M, et al. A Novel Comprehensive Clinical Stratification Model to Refine Prognosis of Glioblastoma Patients Undergoing Surgical Resection. Cancers. 2020; 12(2):386. https://doi.org/10.3390/cancers12020386
Chicago/Turabian StyleIus, Tamara, Fabrizio Pignotti, Giuseppe Maria Della Pepa, Giuseppe La Rocca, Teresa Somma, Miriam Isola, Claudio Battistella, Simona Gaudino, Maurizio Polano, Michele Dal Bo, and et al. 2020. "A Novel Comprehensive Clinical Stratification Model to Refine Prognosis of Glioblastoma Patients Undergoing Surgical Resection" Cancers 12, no. 2: 386. https://doi.org/10.3390/cancers12020386