Long-Term Outcomes of Stereotactic Radiosurgery for Vestibular Schwannoma Associated with Neurofibromatosis Type 2 in Comparison to Sporadic Schwannoma


 ,
,
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics of the Entire Cohort
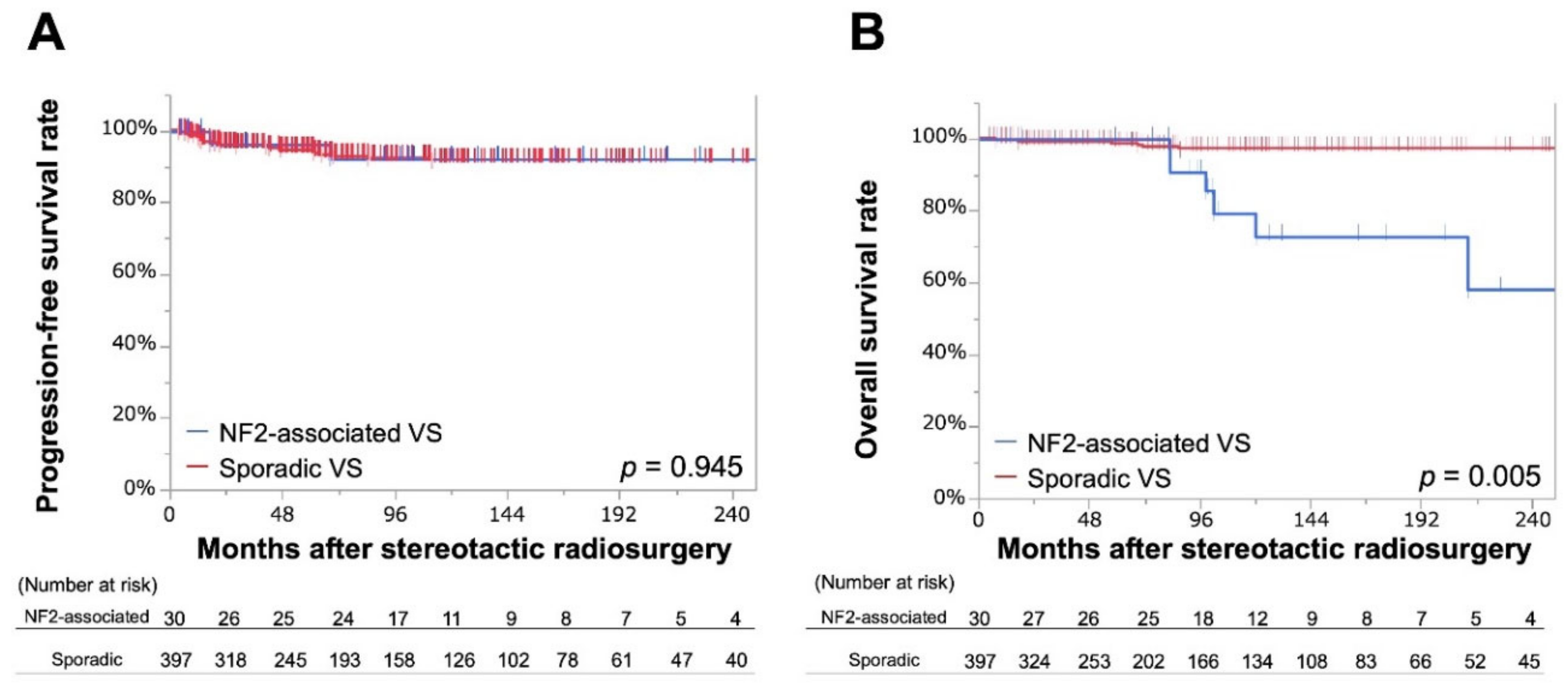
2.2. Endpoints for the Entire Cohort
2.3. Propensity Score Matching and Patient Background in the Matched Cohort
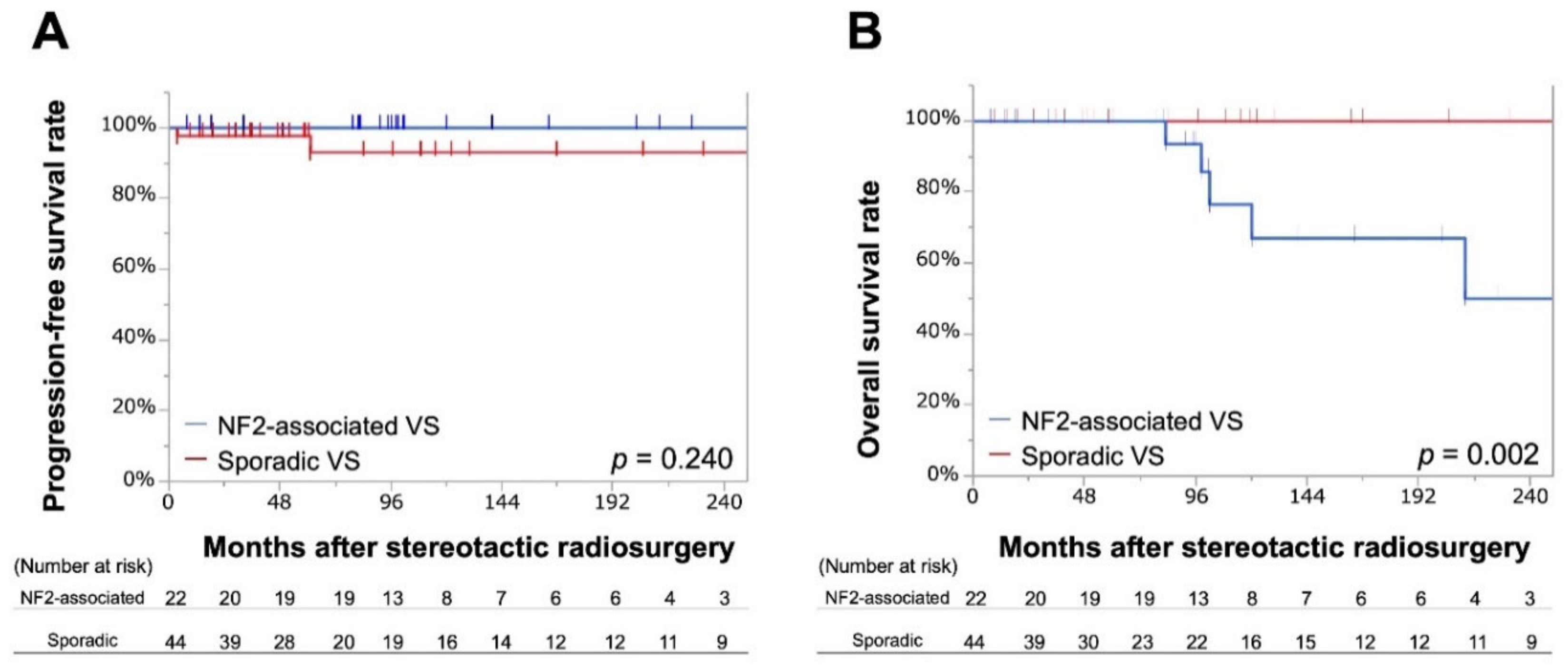
2.4. Endpoints in the Matched Cohort
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Radiosurgical Techniques and Post-SRS Management
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Evans, D.G.; Moran, A.; King, A.; Saeed, S.; Gurusinghe, N.; Ramsden, R. Incidence of vestibular schwannoma and neurofibromatosis 2 in the north west of england over a 10-year period: Higher incidence than previously thought. Otol. Neurotol. 2005, 26, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.G.; Howard, E.; Giblin, C.; Clancy, T.; Spencer, H.; Huson, S.M.; Lalloo, F. Birth incidence and prevalence of tumor-prone syndromes: Estimates from a uk family genetic register service. Am. J. Med. Genet. A 2010, 152, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Rouleau, G.A.; Merel, P.; Lutchman, M.; Sanson, M.; Zucman, J.; Marineau, C.; Hoang-Xuan, K.; Demczuk, S.; Desmaze, C.; Plougastel, B.; et al. Alteration in a new gene encoding a putative membrane-organizing protein causes neuro-fibromatosis type 2. Nature 1993, 363, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Trofatter, J.A.; MacCollin, M.M.; Rutter, J.L.; Murrell, J.R.; Duyao, M.P.; Parry, D.M.; Eldridge, R.; Kley, N.; Menon, A.G.; Pulaski, K.; et al. A novel moesin-, ezrin-, radixin-like gene is a candidate for the neurofibromatosis 2 tumor suppressor. Cell 1993, 72, 791–800. [Google Scholar] [CrossRef]
- Blakeley, J.O.; Plotkin, S.R. Therapeutic advances for the tumors associated with neurofibromatosis type 1, type 2, and schwannomatosis. Neuro Oncol. 2016, 18, 624–638. [Google Scholar] [CrossRef] [PubMed]
- Ferner, R.E. Neurofibromatosis 1 and neurofibromatosis 2: A twenty first century perspective. Lancet. Neurol. 2007, 6, 340–351. [Google Scholar] [CrossRef]
- Coy, S.; Rashid, R.; Stemmer-Rachamimov, A.; Santagata, S. An update on the cns manifestations of neurofibromatosis type 2. Acta Neuropathol. 2019, 1–23. [Google Scholar] [CrossRef]
- Choi, J.W.; Lee, J.Y.; Phi, J.H.; Wang, K.C.; Chung, H.T.; Paek, S.H.; Kim, D.G.; Park, S.H.; Kim, S.K. Clinical course of vestibular schwannoma in pediatric neurofibromatosis type 2. J. Neurosurg. Pediatr. 2014, 13, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.G.; Kalamarides, M.; Hunter-Schaedle, K.; Blakeley, J.; Allen, J.; Babovic-Vuskanovic, D.; Belzberg, A.; Bollag, G.; Chen, R.; DiTomaso, E.; et al. Consensus recommendations to accelerate clinical trials for neurofibromatosis type 2. Clin. Cancer Res. 2009, 15, 5032–5039. [Google Scholar] [CrossRef] [PubMed]
- Bourn, D.; Carter, S.A.; Evans, D.G.; Goodship, J.; Coakham, H.; Strachan, T. A mutation in the neurofibromatosis type 2 tumor-suppressor gene, giving rise to widely different clinical phenotypes in two unrelated individuals. Am. J. Hum. Genet. 1994, 55, 69–73. [Google Scholar]
- Kondziolka, D.; Lunsford, L.D.; McLaughlin, M.R.; Flickinger, J.C. Long-term outcomes after radiosurgery for acoustic neuromas. N. Engl. J. Med. 1998, 339, 1426–1433. [Google Scholar] [CrossRef] [PubMed]
- Iwai, Y.; Yamanaka, K.; Shiotani, M.; Uyama, T. Radiosurgery for acoustic neuromas: Results of low-dose treatment. Neurosurgery 2003, 53, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Lunsford, L.D.; Niranjan, A.; Flickinger, J.C.; Maitz, A.; Kondziolka, D. Radiosurgery of vestibular schwannomas: Summary of experience in 829 cases. J. Neurosurg. 2005, 102, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Kida, Y.; Kato, T.; Iizuka, H.; Kuramitsu, S.; Yamamoto, T. Long-term safety and efficacy of stereotactic radiosurgery for vestibular schwannomas: Evaluation of 440 patients more than 10 years after treatment with gamma knife surgery. J. Neurosurg. 2013, 118, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Klijn, S.; Verheul, J.B.; Beute, G.N.; Leenstra, S.; Mulder, J.J.; Kunst, H.P.; Hanssens, P.E. Gamma knife radiosurgery for vestibular schwannomas: Evaluation of tumor control and its predictors in a large patient cohort in the netherlands. J. Neurosurg. 2016, 124, 1619–1626. [Google Scholar] [CrossRef]
- Hasegawa, T.; Kato, T.; Yamamoto, T.; Naito, T.; Kato, N.; Torii, J.; Ishii, K. Long-term hearing outcomes after gamma knife surgery in patients with vestibular schwannoma with hearing preservation: Evaluation in 92 patients with serial audiograms. J. Neurooncol. 2018, 138, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Mallory, G.W.; Pollock, B.E.; Foote, R.L.; Carlson, M.L.; Driscoll, C.L.; Link, M.J. Stereotactic radiosurgery for neurofibromatosis 2-associated vestibular schwannomas: Toward dose optimization for tumor control and functional outcomes. Neurosurgery 2014, 74, 292–301. [Google Scholar] [CrossRef]
- Massager, N.; Delbrouck, C.; Masudi, J.; De Smedt, F.; Devriendt, D. Hearing preservation and tumour control after radiosurgery for nf2-related vestibular schwannomas. B-ENT 2013, 9, 29–36. [Google Scholar]
- Mathieu, D.; Kondziolka, D.; Flickinger, J.C.; Niranjan, A.; Williamson, R.; Martin, J.J.; Lunsford, L.D. Stereotactic radiosurgery for vestibular schwannomas in patients with neurofibromatosis type 2: An analysis of tumor control, complications, and hearing preservation rates. Neurosurgery 2007, 60, 460–470. [Google Scholar] [CrossRef]
- Phi, J.H.; Kim, D.G.; Chung, H.T.; Lee, J.; Paek, S.H.; Jung, H.W. Radiosurgical treatment of vestibular schwannomas in patients with neurofibromatosis type 2: Tumor control and hearing preservation. Cancer 2009, 115, 390–398. [Google Scholar] [CrossRef]
- Rowe, J.; Radatz, M.; Kemeny, A. Radiosurgery for type ii neurofibromatosis. Prog. Neurol. Surg. 2008, 21, 176–182. [Google Scholar] [PubMed]
- Rowe, J.G.; Radatz, M.W.; Walton, L.; Soanes, T.; Rodgers, J.; Kemeny, A.A. Clinical experience with gamma knife stereotactic radiosurgery in the management of vestibular schwannomas secondary to type 2 neurofibromatosis. J. Neurol. Neurosurg. Psychiatry 2003, 74, 1288–1293. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Liu, A. Long-term follow-up studies of gamma knife surgery for patients with neurofibromatosis type 2. J. Neurosurg. 2014, 121, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Kruyt, I.J.; Verheul, J.B.; Hanssens, P.E.J.; Kunst, H.P.M. Gamma knife radiosurgery for treatment of growing vestibular schwannomas in patients with neurofibromatosis type 2: A matched cohort study with sporadic vestibular schwannomas. J. Neurosurg. 2018, 128, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Subach, B.R.; Kondziolka, D.; Lunsford, L.D.; Bissonette, D.J.; Flickinger, J.C.; Maitz, A.H. Stereotactic radiosurgery in the management of acoustic neuromas associated with neurofibromatosis type 2. J. Neurosurg. 1999, 90, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Kida, Y.; Kobayashi, T.; Tanaka, T.; Mori, Y. Radiosurgery for bilateral neurinomas associated with neurofibromatosis type 2. Surg. Neurol. 2000, 53, 383–389; discussion 389–390. [Google Scholar] [CrossRef]
- Roche, P.H.; Regis, J.; Pellet, W.; Thomassin, J.M.; Gregoire, R.; Dufour, H.; Peragut, J.C. Neurofibromatosis type 2. Preliminary results of gamma knife radiosurgery of vestibular schwannomas. Neurochirurgie 2000, 46, 339–353. [Google Scholar]
- Shin, M.; Ueki, K.; Kurita, H.; Kirino, T. Malignant transformation of a vestibular schwannoma after gamma knife radiosurgery. Lancet 2002, 360, 309–310. [Google Scholar] [CrossRef]
- Sharma, M.S.; Singh, R.; Kale, S.S.; Agrawal, D.; Sharma, B.S.; Mahapatra, A.K. Tumor control and hearing preservation after gamma knife radiosurgery for vestibular schwannomas in neurofibromatosis type 2. J. Neurooncol. 2010, 98, 265–270. [Google Scholar] [CrossRef]
- Boari, N.; Bailo, M.; Gagliardi, F.; Franzin, A.; Gemma, M.; del Vecchio, A.; Bolognesi, A.; Picozzi, P.; Mortini, P. Gamma knife radiosurgery for vestibular schwannoma: Clinical results at long-term follow-up in a series of 379 patients. J. Neurosurg. 2014, 121, 123–142. [Google Scholar] [CrossRef]
- Bowden, G.; Cavaleri, J.; Monaco, E., III; Niranjan, A.; Flickinger, J.; Lunsford, L.D. Cystic vestibular schwannomas respond best to radiosurgery. Neurosurgery 2017, 81, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Petit, J.H.; Hudes, R.S.; Chen, T.T.; Eisenberg, H.M.; Simard, J.M.; Chin, L.S. Reduced-dose radiosurgery for vestibular schwannomas. Neurosurgery 2001, 49, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Inoue, H.K. Low-dose radiosurgery for large vestibular schwannomas: Long-term results of functional preservation. J. Neurosurg. 2005, 102, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Ruttledge, M.H.; Andermann, A.A.; Phelan, C.M.; Claudio, J.O.; Han, F.Y.; Chretien, N.; Rangaratnam, S.; MacCollin, M.; Short, P.; Parry, D.; et al. Type of mutation in the neurofibromatosis type 2 gene (nf2) frequently determines severity of disease. Am. J. Hum. Genet. 1996, 59, 331–342. [Google Scholar] [PubMed]
- Kluwe, L.; MacCollin, M.; Tatagiba, M.; Thomas, S.; Hazim, W.; Haase, W.; Mautner, V.F. Phenotypic variability associated with 14 splice-site mutations in the nf2 gene. Am. J. Med. Genet. 1998, 77, 228–233. [Google Scholar] [CrossRef]
- Ragge, N.K. Clinical and genetic patterns of neurofibromatosis 1 and 2. Br. J. Ophthalmol. 1993, 77, 662–672. [Google Scholar] [CrossRef]
- Brackmann, D.E.; Fayad, J.N.; Slattery, W.H., 3rd; Friedman, R.A.; Day, J.D.; Hitselberger, W.E.; Owens, R.M. Early proactive management of vestibular schwannomas in neurofibromatosis type 2. Neurosurgery 2001, 49, 274–283. [Google Scholar]
- Slattery, W.H., 3rd; Fisher, L.M.; Hitselberger, W.; Friedman, R.A.; Brackmann, D.E. Hearing preservation surgery for neurofibromatosis type 2-related vestibular schwannoma in pediatric patients. J. Neurosurg. 2007, 106, 255–260. [Google Scholar] [CrossRef]
- Gugel, I.; Grimm, F.; Teuber, C.; Kluwe, L.; Mautner, V.F.; Tatagiba, M.; Schuhmann, M.U. Management of nf2-associated vestibular schwannomas in children and young adults: Influence of surgery and clinical factors on tumor volume and growth rate. J. Neurosurg. Pediatr. 2019, 1, 1–9. [Google Scholar]
- Caye-Thomasen, P.; Baandrup, L.; Jacobsen, G.K.; Thomsen, J.; Stangerup, S.E. Immunohistochemical demonstration of vascular endothelial growth factor in vestibular schwannomas correlates to tumor growth rate. Laryngoscope 2003, 113, 2129–2134. [Google Scholar] [CrossRef]
- Plotkin, S.R.; Stemmer-Rachamimov, A.O.; Barker, F.G., 2nd; Halpin, C.; Padera, T.P.; Tyrrell, A.; Sorensen, A.G.; Jain, R.K.; di Tomaso, E. Hearing improvement after bevacizumab in patients with neurofibromatosis type 2. N. Engl. J. Med. 2009, 361, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Mautner, V.F.; Nguyen, R.; Knecht, R.; Bokemeyer, C. Radiographic regression of vestibular schwannomas induced by bevacizumab treatment: Sustain under continuous drug application and rebound after drug discontinuation. Ann. Oncol. 2010, 21, 2294–2295. [Google Scholar] [CrossRef] [PubMed]
- Mautner, V.F.; Nguyen, R.; Kutta, H.; Fuensterer, C.; Bokemeyer, C.; Hagel, C.; Friedrich, R.E.; Panse, J. Bevacizumab induces regression of vestibular schwannomas in patients with neurofibromatosis type 2. Neuro. Oncol. 2010, 12, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, S.R.; Merker, V.L.; Halpin, C.; Jennings, D.; McKenna, M.J.; Harris, G.J.; Barker, F.G., 2nd. Bevacizumab for progressive vestibular schwannoma in neurofibromatosis type 2: A retrospective review of 31 patients. Otol. Neurotol. 2012, 33, 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Demetriades, A.K.; Saunders, N.; Rose, P.; Fisher, C.; Rowe, J.; Tranter, R.; Hardwidge, C. Malignant transformation of acoustic neuroma/vestibular schwannoma 10 years after gamma knife stereotactic radiosurgery. Skull Base 2010, 20, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Yanamadala, V.; Williamson, R.W.; Fusco, D.J.; Eschbacher, J.; Weisskopf, P.; Porter, R.W. Malignant transformation of a vestibular schwannoma after gamma knife radiosurgery. World Neurosurg. 2013, 79, 593.e1–593.e8. [Google Scholar] [CrossRef] [PubMed]
- Mindermann, T.; Schlegel, I. How to distinguish tumor growth from transient expansion of vestibular schwannomas following gamma knife radiosurgery. Acta Neurochir. 2014, 156, 1121–1123. [Google Scholar] [CrossRef]
- Nagano, O.; Higuchi, Y.; Serizawa, T.; Ono, J.; Matsuda, S.; Yamakami, I.; Saeki, N. Transient expansion of vestibular schwannoma following stereotactic radiosurgery. J. Neurosurg. 2008, 109, 811–816. [Google Scholar] [CrossRef]
- Yomo, S.; Arkha, Y.; Delsanti, C.; Roche, P.H.; Thomassin, J.M.; Regis, J. Repeat gamma knife surgery for regrowth of vestibular schwannomas. Neurosurgery 2009, 64, 48–55. [Google Scholar] [CrossRef]
- Kim, Y.H.; Kim, D.G.; Han, J.H.; Chung, H.T.; Kim, I.K.; Song, S.W.; Park, J.H.; Kim, J.W.; Park, C.K.; Kim, C.Y.; et al. Hearing outcomes after stereotactic radiosurgery for unilateral intracanalicular vestibular schwannomas: Implication of transient volume expansion. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 61–67. [Google Scholar] [CrossRef]
- Sun, S.; Liu, A. Long-term follow-up studies of gamma knife surgery with a low margin dose for vestibular schwannoma. J. Neurosurg. 2012, 117, 57–62. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | NF2-Associated VSs | Sporadic VSs | p Value |
|---|---|---|---|
| Number of patients (tumors), n | 25 (30) | 397 (397) | / |
| Age at SRS, year, mean ± SD | 38 ± 18 | 56 ± 13 | <0.001 * |
| Observation period, months, mean ± SD | 121 ± 82 | 103 ± 91 | 0.300 |
| Target volume, cm3, mean ± SD | 4.4 ± 4.1 | 2.0 ± 2.0 | <0.001 * |
| Prescription dose, Gy, mean ± SD | 13 ± 0.4 | 13 ± 0.1 | 0.883 |
| Central dose, Gy, mean ± SD | 27 ± 0.7 | 27 ± 0.2 | 0.760 |
| Male sex, n (%) | 6 (20.0) | 196 (49) | 0.002 * |
| Prior surgical intervention, n (%) | 19 (63) | 88 (22) | <0.001 * |
| Variables | Bivariate | Multivariate | ||
|---|---|---|---|---|
| p Value | HR (95%CI) | p Value | HR (95%CI) | |
| Presence of NF2 (vs. absence) | 0.945 | 0.95 (0.15–3.21) | 0.424 | 0.56 (0.09–2.09) |
| Age at SRS >55 years (vs. ≤55 years) | 0.270 | 0.65 (0.29–1.40) | 0.440 | 0.72 (0.31–1.65) |
| Volume >2.0 cm3 (vs. ≤2.0 cm3) | 0.449 | 1.35 (0.61–2.93) | 0.503 | 1.32 (0.58–2.91) |
| Prescription dose >13 Gy (vs. ≤13 Gy) | 0.999 | 1.00 (0.44–2.18) | 0.805 | 0.90 (0.39–2.01) |
| Central dose >26 Gy (vs. ≤26 Gy) | 0.640 | 0.83 (0.38–1.80) | / | / |
| Male sex (vs. female sex) | 0.072 | 0.48 (0.20–1.07) | / | / |
| Prior surgery (vs. absence of prior surgery) | 0.035 * | 2.39 (1.07–5.17) | 0.051 | 2.31 (1.00–5.18) |
| Variables | NF2-associated VSs | Sporadic VSs | p Value |
|---|---|---|---|
| All complications | 4 (13.3) | 35 (8.9) | 0.69 |
| -Trigeminal neuralgia | 1 (3.3) | 11 (2.8) | 0.86 |
| -Facial paresis | 2 (6.7) | 18 (4.5) | 0.59 |
| -Hydrocephalus | 2 (6.7) | 15 (3.8) | 0.44 |
| -CTCAE gr. 3–4 | 2 (6.7) | 23 (5.8) | 0.84 |
| Variables | Bivariate | Multivariate | ||
|---|---|---|---|---|
| p Value | OR (95%CI) | p Value | OR (95%CI) | |
| Presence of NF2 (vs. absence) | 0.937 | 1.06 (0.24–4.72) | 0.832 | 0.84 (0.17–4.20) |
| Age at SRS >55 years (vs. ≤55 years) | 0.712 | 0.86 (0.40–1.88) | 0.432 | 1.41 (0.60–3.32) |
| Volume >2.0 cm3 (vs. ≤2.0 cm3) | 0.425 | 1.38 (0.63–3.02) | 0.496 | 1.34 (0.57–3.15) |
| Prescription dose >13 Gy (vs. ≤13 Gy) | <0.001 * | 7.61 (3.00–19.32) | <0.001 * | 8.30 (3.19–21.62) |
| Central dose >26 Gy (vs. ≤26 Gy) | 0.034 * | 2.44 (1.07–5.57) | / | / |
| Male sex (vs. female sex) | 0.063 | 0.45 (0.19–1.05) | / | / |
| Prior surgery (vs. absence of prior surgery) | 0.891 | 1.06 (0.44–2.60) | 0.915 | 1.05 (0.40–2.76) |
| Variables | NF2-Associated VS (n = 22) | Sporadic VS (n = 44) | p Value | %Bias |
|---|---|---|---|---|
| Volume, cm3, mean ± SD | 3.2 ± 0.4 | 3.1 ± 0.3 | 0.827 | 3.4 |
| Age at SRS, year, mean ± SD | 45 ± 15 | 46 ± 16 | 0.937 | −2.1 |
| Male sex, n (%) | 6 (27) | 12 (27) | 1.000 | 0.0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shinya, Y.; Hasegawa, H.; Shin, M.; Sugiyama, T.; Kawashima, M.; Takahashi, W.; Iwasaki, S.; Kashio, A.; Nakatomi, H.; Saito, N. Long-Term Outcomes of Stereotactic Radiosurgery for Vestibular Schwannoma Associated with Neurofibromatosis Type 2 in Comparison to Sporadic Schwannoma. Cancers 2019, 11, 1498. https://doi.org/10.3390/cancers11101498
Shinya Y, Hasegawa H, Shin M, Sugiyama T, Kawashima M, Takahashi W, Iwasaki S, Kashio A, Nakatomi H, Saito N. Long-Term Outcomes of Stereotactic Radiosurgery for Vestibular Schwannoma Associated with Neurofibromatosis Type 2 in Comparison to Sporadic Schwannoma. Cancers. 2019; 11(10):1498. https://doi.org/10.3390/cancers11101498
Chicago/Turabian StyleShinya, Yuki, Hirotaka Hasegawa, Masahiro Shin, Takehiro Sugiyama, Mariko Kawashima, Wataru Takahashi, Shinichi Iwasaki, Akinori Kashio, Hirofumi Nakatomi, and Nobuhito Saito. 2019. "Long-Term Outcomes of Stereotactic Radiosurgery for Vestibular Schwannoma Associated with Neurofibromatosis Type 2 in Comparison to Sporadic Schwannoma" Cancers 11, no. 10: 1498. https://doi.org/10.3390/cancers11101498