Liquid Biopsy in Lung Cancer Screening: The Contribution of Metabolomics. Results of A Pilot Study

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Sample Analysis
2.3. Data Analysis
3. Results
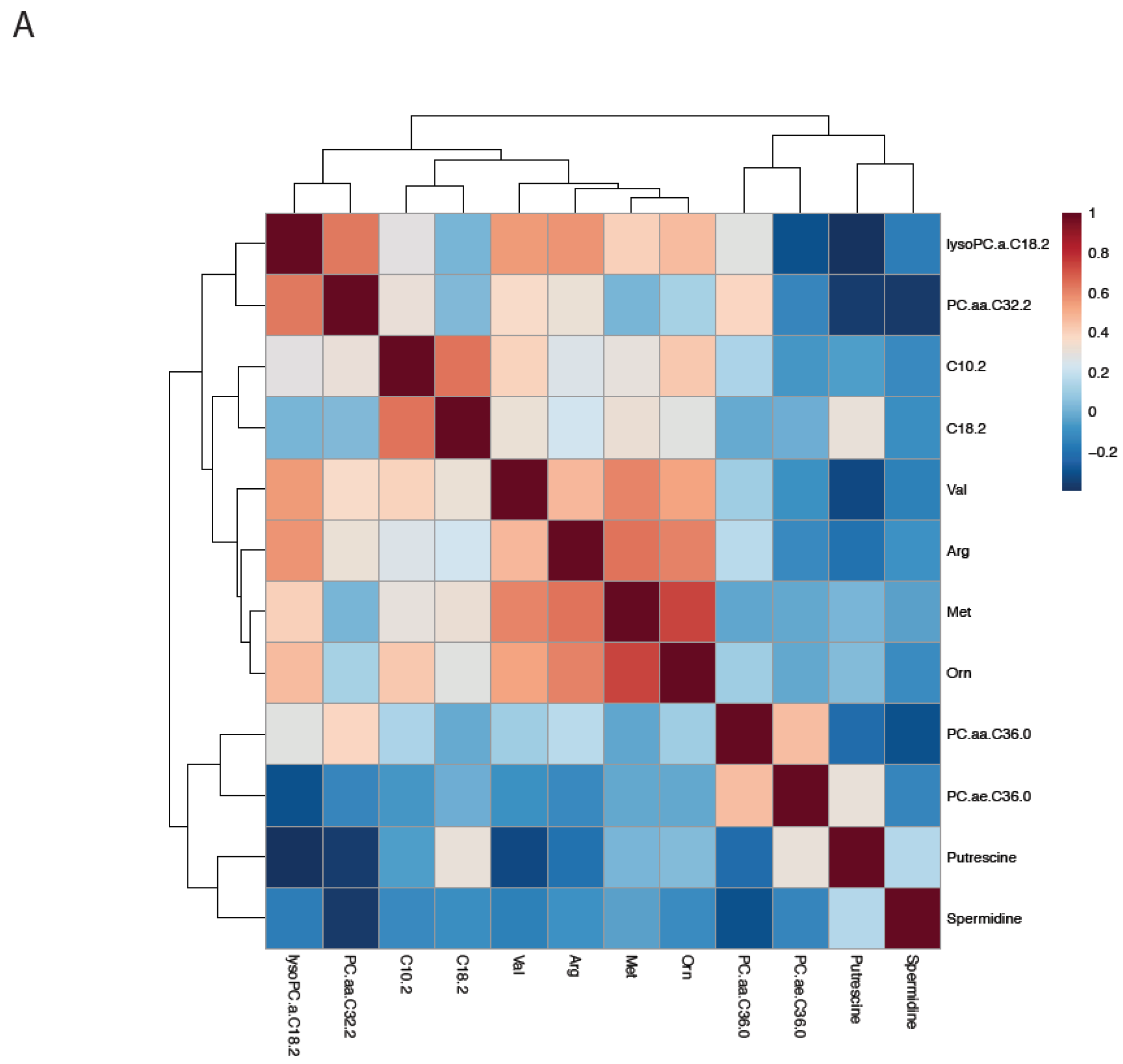
3.1. Cluster Analysis and Correlation Matrix
3.2. Univariate Results
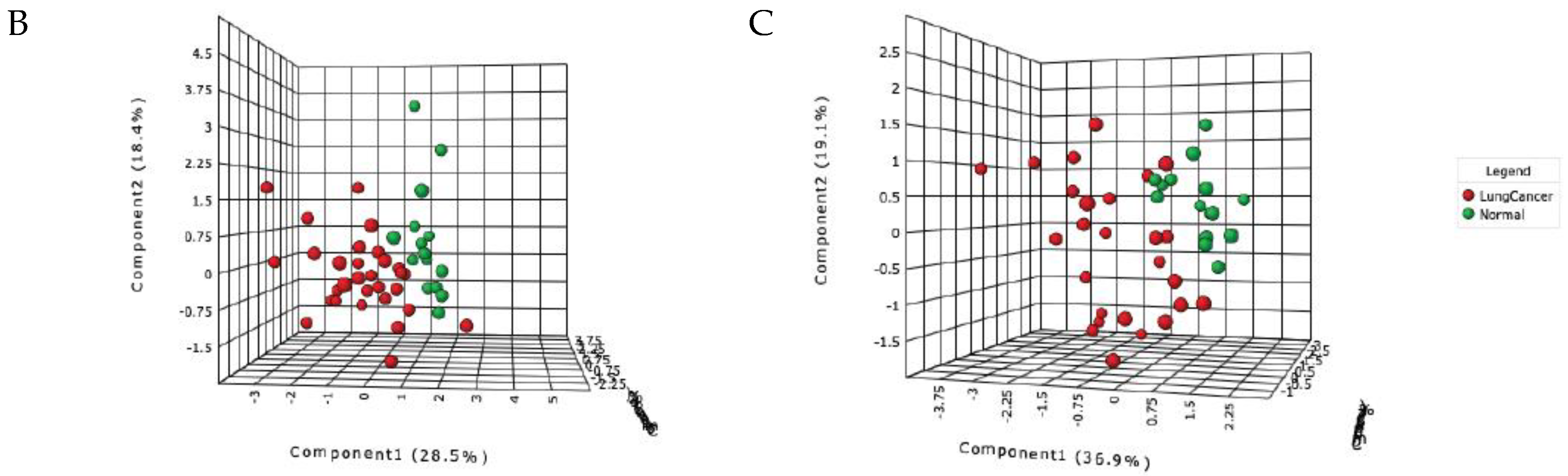
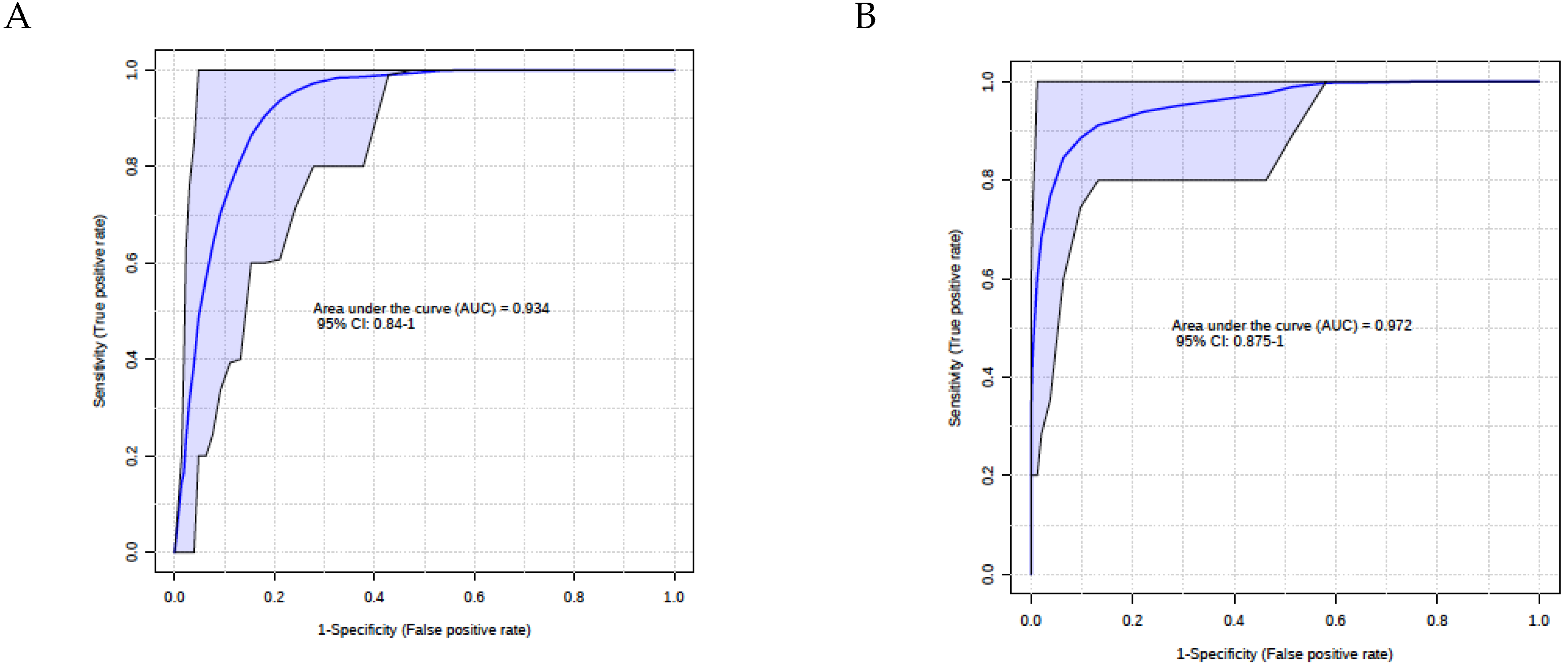
3.3. Multivariate Results
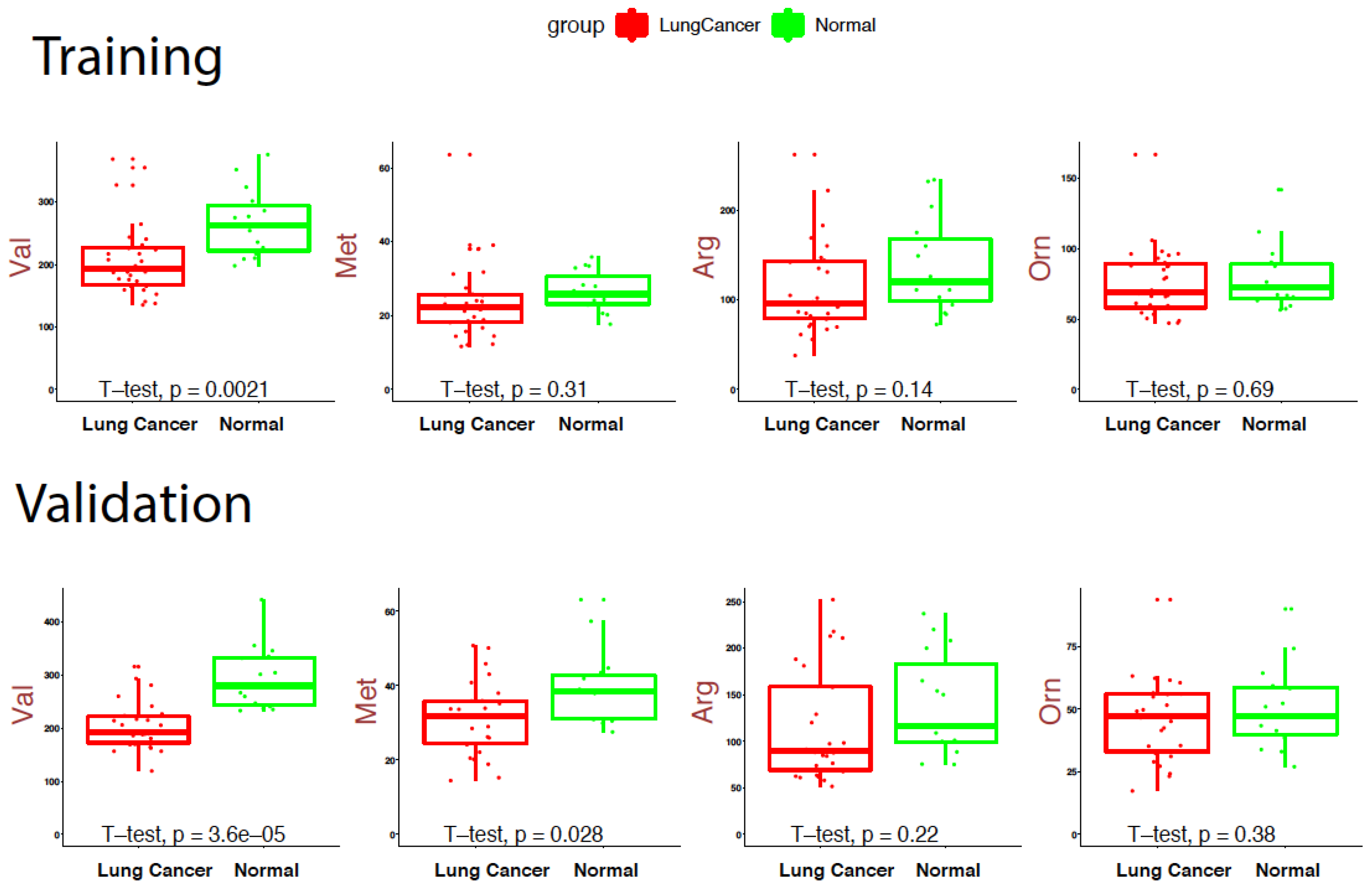
3.4. Box Plots
4. Discussion
5. Conclusions
- There is an urgent need to identify reliable, sensitive and economical diagnostic test for lung cancer, which is typically detected late and non-symptomatic where treatment options are limited and tend to be aggressive.
- Metabolomics is moving to clinical bedside with increased number of approved tests now being offered for diagnosis, prognosis and surveillance.
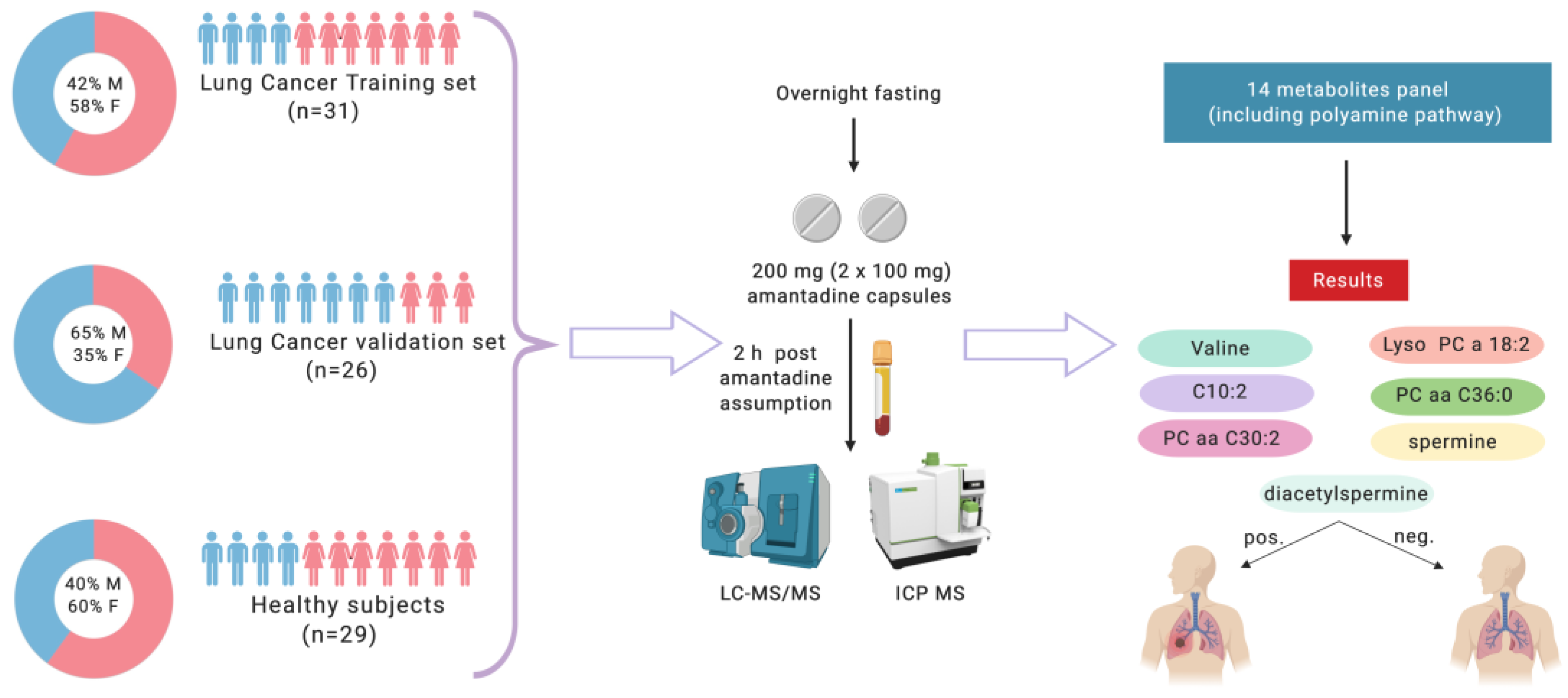
- We report in this paper a robust panel of 14 metabolites associated in the SSAT-1/polyamine pathway along with other endogenous metabolites comprised of amino acids, biogenic amines, acylcarnitines and glycerophospholipids amines that correctly discriminated between lung cancer patients from healthy controls using an established and customized assay.
- Detection and measurement of these specific metabolites can be employed to distinguish between healthy participants and patients with a diagnosis of lung cancer using existing LCMS equipment and infrastructure.
- This test can complement the SSAT1 Amantadine assay to further increase tissue specificity.
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- PDQ Adult Treatment Editorial Board. Non-small cell lung cancer treatment (PDQ®): Health professional version. In PDQ Cancer Information Summaries; National Cancer Institute (US), Bethesda: Rockville, MD, USA, 2002. Available online: http://www.ncbi.nlm.nih.gov/books/NBK65865/ (accessed on 27 July 2019).
- Jemal, A.; Ward, E.M.; Johnson, C.J.; Cronin, K.A.; Ma, J.; Ryerson, A.B.; Mariotto, A.; Lake, A.J.; Wilson, R.; Sherman, R.L.; et al. Annual Report to the Nation on the Status of Cancer, 1975–2014, Featuring Survival. J. Natl. Cancer Inst. 2017, 109, 8. [Google Scholar] [CrossRef]
- Corrales, L.; Nogueira, A.; Passiglia, F.; Listi, A.; Caglevic, C.; Giallombardo, M.; Raez, L.; Santos, E.; Rolfo, C. Second-Line Treatment of Non-Small Cell Lung Cancer: Clinical, Pathological, and Molecular Aspects of Nintedanib. Front. Med. 2017, 4, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horeweg, N.; Scholten, E.T.; de Jong, P.A.; van der Aalst, C.M.; Weenink, C.; Lammers, J.W.; Nackaerts, K.; Vliegenthart, R.; ten Haaf, K.; Yousaf-Khan, U.A.; et al. Detection of lung cancer through low-dose CT screening (NELSON): A prespecified analysis of screening test performance and interval cancers. Lancet Oncol. 2014, 15, 1342–1350. [Google Scholar] [CrossRef]
- Gartman, E.J.; Jankowich, M.D.; Baptiste, J.; Nici, L. Providence VA lung cancer screening program: Performance: Comparison of Local False Positive and Invasive Procedure Rates to Published Trial Data, A98. Clinical Strategies to Improve Lung Cancer Early Detection: Who is at Risk Here. In American Journal of Respiratory and Critical Care Medicine, Proceedings of the American Thoracic Society International Conference Abstracts, San-Diego, CA, USA, 18–23 May 2018; American Thoracic Society: New York, NY, USA; Volume 197, p. A2477.
- Seijo, L.M.; Peled, N.; Ajona, D.; Boeri, M.; Field, J.K.; Sozzi, G.; Pio, R.; Zulueta, J.J.; Spira, A.; Massion, P.P.; et al. Biomarkers in Lung Cancer Screening: Achievements, Promises, and Challenges. J. Thorac. Oncol. 2019, 14, 343–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamdani, H.; Ahmed, S.; Armstrong, S.; Mok, T.; Jalal, S.I. Blood-based tumor biomarkers in lung cancer for detection and treatment. Transl. Lung Cancer Res. 2017, 6, 648–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leygo, C.; Williams, M.; Jin, H.C.; Chan, M.W.Y.; Chu, W.K.; Grusch, M.; Cheng, Y.Y. DNA Methylation as a Noninvasive Epigenetic Biomarker for the Detection of Cancer. Dise. Markers 2017, 2017, 3726595. [Google Scholar] [CrossRef] [PubMed]
- Wishart, S.D.; Mandal, R.; Stanislaus, A.; Ramirez-Gaona, M. Cancer Metabolomics and the Human Metabolome Database. Metabolites 2016, 6, 10. [Google Scholar] [CrossRef] [PubMed]
- Jordan, K.W.; Adkins, C.B.; Su, L.; Halpern, E.F.; Mark, E.J.; Christiani, D.C.; Cheng, L.L. Comparison of squamous cell carcinoma and adenocarcinoma of the lung by metabolomic analysis of tissue–serum pairs. Lung Cancer 2010, 68, 44–50. [Google Scholar] [CrossRef]
- Hori, S.; Nishiumi, S.; Kobayashi, K.; Shinohara, M.; Hatakeyama, Y.; Kotani, Y.; Hatano, N.; Maniwa, Y.; Nishio, W.; Bamba, T.; et al. A metabolomic approach to lung cancer. Lung Cancer 2011, 74, 284–292. [Google Scholar] [CrossRef]
- Mathé, E.A.; Patterson, A.D.; Haznadar, M.; Manna, S.K.; Krausz, K.W.; Bowman, E.D.; Shields, P.G.; Idle, J.R.; Smith, P.B.; Anami, K.; et al. Noninvasive Urinary Metabolomic Profiling Identifies Diagnostic and Prognostic Markers in Lung Cancer. Cancer Res. 2014, 74, 3259. [Google Scholar] [CrossRef]
- Miyamoto, S.; Taylor, L.S.; Barupal, K.D.; Taguchi, A.; Wohlgemuth, G.; Wikoff, R.W.; Yoneda, Y.K.; Gandara, R.D.; Hanash, M.S.; Kim, K.; et al. Systemic Metabolomic Changes in Blood Samples of Lung Cancer Patients Identified by Gas Chromatography Time-of-Flight Mass Spectrometry. Metabolites 2015, 5, 192–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yokota, H.; Guo, J.; Matoba, M.; Higashi, K.; Tonami, H.; Nagao, Y. Lactate, choline, and creatine levels measured by vitro 1H-MRS as prognostic parameters in patients with non-small-cell lung cancer. J. Magn. Reson. Imaging 2007, 25, 992–999. [Google Scholar] [CrossRef] [PubMed]
- Blackburn, E.H. Cancer Interception. Cancer Prev. Res. (Phila) 2011, 4, 787. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Li, Z.; Lazar, L.; Fang, Z.; Tang, C.; Zhao, J. Metabolomics workflow for lung cancer: Discovery of biomarkers. Clin. Chim. Acta 2019, 495, 436–445. [Google Scholar] [CrossRef] [PubMed]
- Maes, E.; Mertens, I.; Valkenborg, D.; Pauwels, P.; Rolfo, C.; Baggerman, G. Proteomics in cancer research: Are we ready for clinical practice? Crit. Rev. Oncol. Hematol. 2015, 96, 437–448. [Google Scholar] [CrossRef] [PubMed]
- Pegg, A.E. Functions of Polyamines in Mammals. J. Biol. Chem. 2016, 291, 14904–14912. [Google Scholar] [CrossRef] [Green Version]
- Babbar, N.; Hacker, A.; Huang, Y.; Casero, R.A. Tumor Necrosis Factor α Induces Spermidine/Spermine N1-Acetyltransferase through Nuclear Factor κBin Non-small Cell Lung Cancer Cells. J. Biol. Chem. 2006, 281, 24182–24192. [Google Scholar] [CrossRef]
- Gabrielson, E.; Tully, E.; Hacker, A. Induction of spermidine/spermine N1-acetyltransferase in breast cancer tissues treated with the polyamine analogue N1, N11-diethylnorspermine. Cancer Chemother Pharmacol. 2004, 54, 122–126. [Google Scholar] [CrossRef]
- Huang, W.; Eickhoff, J.C.; Mehraein-Ghomi, F.; Church, D.R.; Wilding, G.; Basu, H.S. Expression of spermidine/spermine N1-acetyl transferase (SSAT) in human prostate tissues is related to prostate cancer progression and metastasis. Prostate 2015, 75, 1150–1159. [Google Scholar] [CrossRef]
- Pegg, A.E. Spermidine/spermine-N1-acetyltransferase: A key metabolic regulator. Am. J. Phy. Endocrinol. Metab. 2008, 294, E995–E1010. [Google Scholar] [CrossRef]
- Kingsnorth, A.N.; Wallace, H.M. Elevation of monoacetylated polyamines in human breast cancers. Eu. J. Cancer Clin. Oncol. 1985, 21, 1057–1062. [Google Scholar] [CrossRef]
- Pine, M.; Huben, R.; Pegg, A. Production of N1-acetyl spermidine by renal cell tumors. J. Urol. 1989, 141, 651–655. [Google Scholar] [CrossRef]
- Sessa, A.; Perin, A. Increased synthesis of N1-acetylspermidine in hepatic preneoplastic nodules and hepatomas. Cancer Lett. 1991, 56, 159–163. [Google Scholar] [CrossRef]
- YeA, C.; Bulovskaya, L.N.; Pavlova, M.V.; Krupkin, R.G. Activity of N-acetyltransferase in patients with malignant lymphomas. Neoplasma 1978, 25, 471–475. [Google Scholar]
- Bredel, M.; Bredel, C.; Juric, D.; Harsh, G.R.; Vogel, H.; Recht, L.D.; Sikic, B.I. Functional network analysis reveals extended gliomagenesis pathway maps and three novel MYC-interacting genes in human gliomas. Cancer Res. 2005, 65, 8679–8689. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kotliarova, S.; Kotliarov, Y.; Li, A.; Su, Q.; Donin, N.M.; Pastorino, S.; Purow, B.W.; Christopher, N.; Zhang, W.; et al. Tumor stem cells derived from glioblastomas cultured in bFGF and EGF more closely mirror the phenotype and genotype of primary tumors than do serum-cultured cell lines. Cancer Cell 2006, 9, 391–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, L.; Hui, A.M.; Su, Q.; Vortmeyer, A.; Kotliarov, Y.; Pastorino, S.; Passaniti, A.; Menon, J.; Walling, J.; Bailey, R.; et al. Neuronal and glioma-derived stem cell factor induces angiogenesis within the brain. Cancer Cell 2006, 9, 287–300. [Google Scholar] [CrossRef] [Green Version]
- Bras, A.P.; Hoff, H.R.; Aoki, F.Y.; Sitar, D.S. Amantadine acetylation may be effected by acetyltransferases other than NAT1 or NAT2. Can. J. Physiol. Pharmacol. 1998, 76, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Maksymiuk, A.W.; Sitar, D.S.; Ahmed, R.; Cheng, B.; Bach, H.; Bagchi, R.A.; Aroutiounova, N.; Tappia, P.S.; Ramjiawan, B. Spermidine/spermine N1-acetyltransferase-1 as a diagnostic biomarker in human cancer. Future Sci. OA 2018, 4, FSO345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maksymiuk, A.W.; Tappia, P.S.; Sitar, D.S.; Akhtar, P.S.; Khatun, N.; Parveen, R.; Ahmed, R.; Ahmed, R.B.; Cheng, B.; Huang, G.; et al. Use of amantadine as substrate for SSAT-1 activity as a reliable clinical diagnostic assay for breast and lung cancer. Future Sci. OA 2019, 5, FSO365. [Google Scholar] [CrossRef] [Green Version]
- Mankiewicz, R. The Story of Mathematics, Paperback ed.; Princeton University Press: Princeton, NJ, USA, 2004; p. 158. ISBN 978-0691120461. [Google Scholar]
- Yoav, B.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar]
- Hanley, J.A. Receiver operating characteristic (ROC) methodology: The state of the art. Crit. Rev. Diagn. Imaging 1989, 29, 307–335. [Google Scholar] [PubMed]
- Li, Y.; Song, X.; Zhao, X.; Zou, L.; Xu, G. Serum metabolic profiling study of lung cancer using ultra high performance liquid chromatography/quadrupole time-of-flight mass spectrometry. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2014, 966, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Fan, T.W.M.; Lane, A.N.; Higashi, R.M.; Farag, M.A.; Gao, H.; Bousamra, M.; Miller, D.M. Altered regulation of metabolic pathways in human lung cancer discerned by (13) C stable isotope-resolved metabolomics (SIRM). Mol. Cancer 2009, 8, 41. [Google Scholar] [CrossRef] [PubMed]
- Kami, K.; Fujimori, T.; Sato, H.; Sato, M.; Yamamoto, H.; Ohashi, Y.; Sugiyama, N.; Ishihama, Y.; Onozuka, H.; Ochiai, A.; et al. Metabolomic profiling of lung and prostate tumor tissues by capillary electrophoresis time-of-flight mass spectrometry. Metabolomics 2013, 9, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, A.; Kami, K.; Sugimoto, M.; Sugawara, M.; Toki, N.; Onozuka, H.; Kinoshita, T.; Saito, N.; Ochiai, A.; Tomita, M.; et al. Quantitative metabolome profiling of colon and stomach cancer microenvironment by capillary electrophoresis time-of-flight mass spectrometry. Cancer Res. 2009, 69, 4918–4925. [Google Scholar] [CrossRef] [PubMed]
- Wikoff, W.R.; Hanash, S.; DeFelice, B.; Miyamoto, S.; Barnett, M.; Zhao, Y.; Goodman, G.; Feng, Z.; Gandara, D.; Fiehn, O.; et al. Diacetylspermine Is a Novel Prediagnostic Serum Biomarker for Non-Small-Cell Lung Cancer and Has Additive Performance With Pro-Surfactant Protein B. J. Clin. Oncol. 2015, 33, 3880–3886. [Google Scholar] [CrossRef] [PubMed]
- Bras, A.P.; Janne, J.; Porter, C.W.; Sitar, D.S. Spermidine/spermine n(1)-acetyltransferase catalyzes amantadine acetylation. Drug Metab. Dispos. 2001, 29, 676–680. [Google Scholar] [PubMed]
- Battaglia, V.; DeStefano Shields, C.; Murray-Stewart, T.; Casero, R.A.J. Polyamine catabolism in carcinogenesis: Potential targets for chemotherapy and chemoprevention. Amino Acids 2014, 46, 511–519. [Google Scholar] [CrossRef]
- Takenoshita, S.; Matsuzaki, S.; Nakano, G.; Kimura, H.; Hoshi, H.; Shoda, H.; Nakamura, T. Selective elevation of the N1-acetylspermidine level in human colorectal adenocarcinomas. Cancer Res. 1984, 44, 845–847. [Google Scholar]
- Available online: https://undark.org/article/bangladesh-arsenic-poisoning-drinking-water/ (accessed on 27 July 2019).
- Soza-Ried, C.; Bustamante, E.; Caglevic, C.; Rolfo, C.; Sirera, R.; Marsiglia, H. Oncogenic role of arsenic exposure in lung cancer: A forgotten risk factor. Crit. Rev. Oncol. Hematol. 2019, 139, 128–133. [Google Scholar] [CrossRef] [PubMed]





© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singhal, S.; Rolfo, C.; Maksymiuk, A.W.; Tappia, P.S.; Sitar, D.S.; Russo, A.; Akhtar, P.S.; Khatun, N.; Rahnuma, P.; Rashiduzzaman, A.; et al. Liquid Biopsy in Lung Cancer Screening: The Contribution of Metabolomics. Results of A Pilot Study. Cancers 2019, 11, 1069. https://doi.org/10.3390/cancers11081069
Singhal S, Rolfo C, Maksymiuk AW, Tappia PS, Sitar DS, Russo A, Akhtar PS, Khatun N, Rahnuma P, Rashiduzzaman A, et al. Liquid Biopsy in Lung Cancer Screening: The Contribution of Metabolomics. Results of A Pilot Study. Cancers. 2019; 11(8):1069. https://doi.org/10.3390/cancers11081069
Chicago/Turabian StyleSinghal, Sandeep, Christian Rolfo, Andrew W. Maksymiuk, Paramjit S. Tappia, Daniel S. Sitar, Alessandro Russo, Parveen S. Akhtar, Nazrina Khatun, Parveen Rahnuma, Ahmed Rashiduzzaman, and et al. 2019. "Liquid Biopsy in Lung Cancer Screening: The Contribution of Metabolomics. Results of A Pilot Study" Cancers 11, no. 8: 1069. https://doi.org/10.3390/cancers11081069