1. Introduction
Delirium is defined as a disturbance of consciousness, presenting with a sudden onset, characterized by a fluctuating course of attention and accompanied by a change in cognition or perception [
1]. It is an acute neuropsychiatric syndrome that impairs the ability of the patient to receive information, process it and store for further recall, that requires monitoring and treatment [
2]. Reported to be a relatively common complication among patients undergoing cardiac surgery, it is associated with increased mortality, longer intensive care unit (ICU) and hospital stay, loss of independence, and an increased risk of developing postoperative cognitive dysfunction [
3,
4,
5,
6,
7]. A new classification of delirium phenotypes is based on clinical risk factors and includes sedative-associated, sepsis-associated, hypoxic and metabolic delirium [
8]. This emphasizes that delirium is a cumulative effect of multiple interconnecting insults, that include neuroinflammation and oxidative stress [
9,
10]. Most likely, the cascade of events starts with generalized inflammation leading to endothelial dysfunction that increases the permeability of the blood-brain barrier and the development of inflammatory changes of the nervous tissue, damage to neurons and exaggerated response of microglial cells [
10].
The diagnosis of delirium is based upon clinical observation therefore it should involve validated bedside psychometric diagnostic tools for accuracy—either CAM-ICU (Cognitive Assessment Method for ICU) or ICDSC (Intensive Care Delirium Screening Checklist) [
2]. Despite active monitoring there are a number of patients that remain undiagnosed, with either hypoactive or subsyndromal delirium [
11,
12]. Research involving biomarkers did not indicate any single particular one for delirium screening, rather an identification of a panel of biomarkers that may lead to an accurate and timely diagnosis and improvement in prediction and recognition of delirium [
13,
14,
15]. Therefore, the researchers keep searching for an accurate ideal biomarker for delirium, that would have a high predictive value, be readily available, reliable and cheap.
The differential white blood cell (WBC) count is one of the tests routinely performed in the majority of hospitalized patients at no additional cost. The number of information provided by it, both in health and in disease, is larger that is commonly thought and cannot be overestimated. Transient elevations of the serum white blood cell count and decreases of platelet count are regarded as normal physiological responses to inflammation. Both, the neutrophil-to-lymphocyte ratio (NLR), and the platelet-to-lymphocyte ratio (PLR), as well as platelet-to-WBC ratio are easily available markers of generalized inflammation reported in different research settings [
16,
17]. An increase in the NLR level has been identified as an outcome measure in cerebrovascular and cardiovascular diseases [
18,
19], neuropsychiatric disorders (i.e., stroke, Alzheimer’s disease or schizophrenia) [
16,
20,
21], autoimmune diseases (i.e., systemic lupus erythematosus, ulcerative colitis) [
22,
23] and various malignant tumors [
24,
25]. A pilot study performed by Egberts et al. reported an association between increased NLR and delirium in elderly patients admitted to a geriatric unit [
17].
Some studies have shown that in certain medical conditions a better predictor of inflammation is the platelet-to-lymphocyte ratio—this was found in chronic renal failure, autoimmune diseases, and cardiovascular diseases [
26,
27]. Serum inflammatory markers based on the differential WBC count, NLR and PLR, have been found to be better predicting factors for mortality and outcome in various medical conditions, as well as predictors of cardiovascular risk as compared with traditional infection markers, including C-reactive protein (CRP) or the total leucocyte count [
28,
29].
To date, a possible association between the panel of white-cell derived biomarkers and postoperative delirium has not been investigated. Therefore, the authors aimed at evaluating which of the markers of inflammation derived from the white cell count, namely NLR, PLR and platelet-to-WBC count ratio (PWR), as well as CRP could serve best for their prognostic value before and after the operation in prediction of delirium after cardiac surgery. Moreover, the aim of this study was to create a model that, using objective clinical and laboratory data, would be useful in assessing the risk of delirium after CABG (coronary artery bypass grafting).
2. Methods
2.1. Study Design and Patient Selection
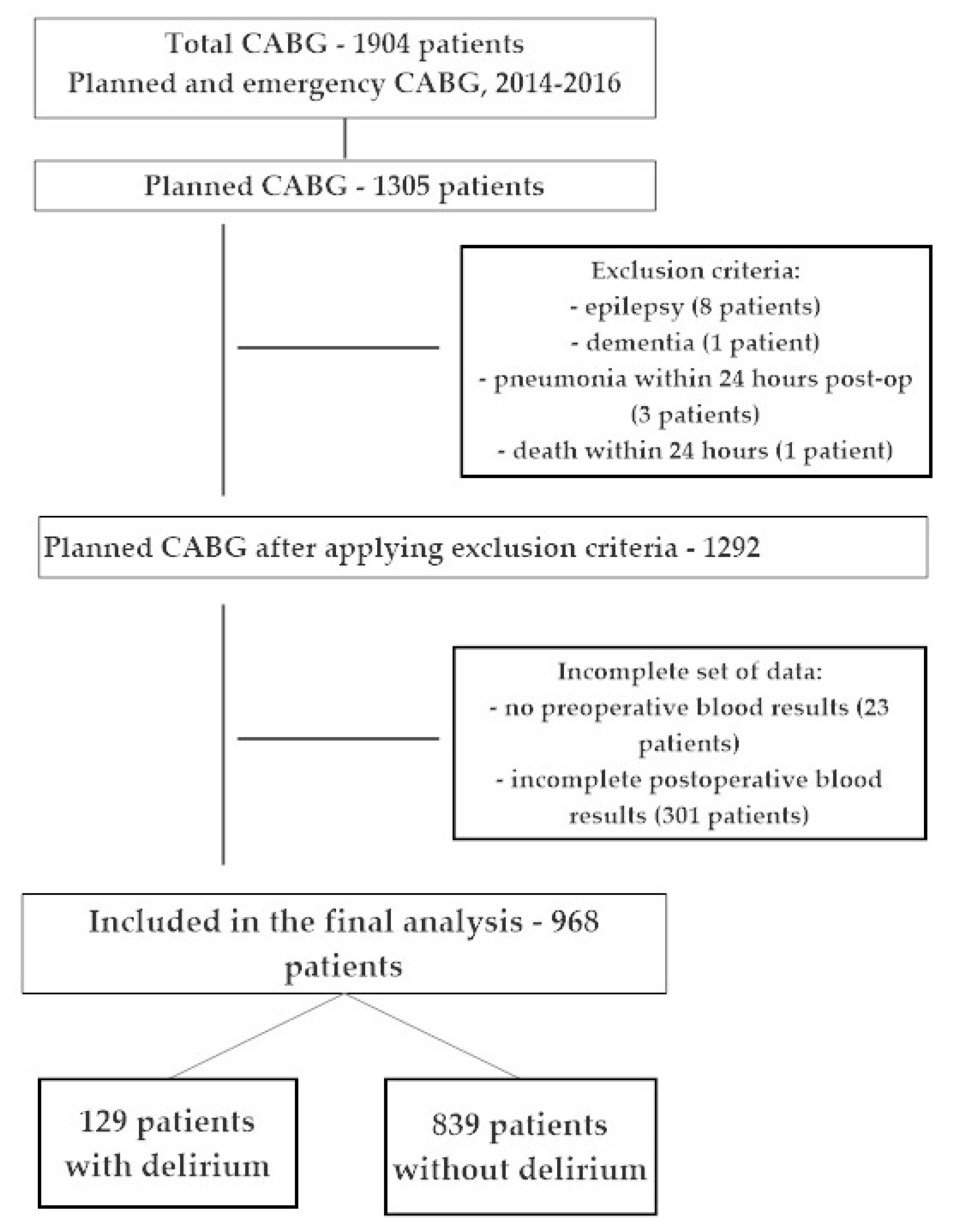
A retrospective cohort analysis was performed including data collected from all patients undergoing cardiac surgery in a cardiac surgery department at the university hospital between 1 January 2014 and 31 December 2016. From the total group of patients undergoing the coronary artery bypass grafting procedure (CABG) at our institution, we included data regarding only patients undergoing planned, isolated CABG. We excluded patients with known pre-operative delirium or cognitive disorder (MMSE below 24 points, known dementia or mild cognitive impairment, MCI), neuropsychiatric disorder (i.e., cognitive impairment, depression, schizophrenia, epilepsy), with known pre-operative infection or who developed a significant postoperative infection (pulmonary, urinary, sepsis) within the first 48 h after CABG. Patients who died either during or within first 24 h after the operation were excluded from further analysis. Only patients with a full set of blood results were included in the analysis. We divided the patients into two groups based on the presence (Delirium +) or absence (Delirium −) of delirium in the postoperative period.
Figure 1 shows that from a total group of 1904 patients undergoing general anesthesia for coronary artery bypass surgery (CABG) between 2014 and 2016, 1305 patients underwent a planned, isolated CABG procedures, which created a very homogeneous group of patients. The study excluded patients with epilepsy (8), with dementia (1), patients who died during the first 24 h after surgery (1), patients with pneumonia within 24 h after surgery (3) and 23 patients who did not have pre-operative laboratory tests. After applying the exclusion criteria, the final analysis included 968 patients with complete perioperative data.
2.2. Data Collection
We reviewed the medical records for demographic data and comorbidities, followed by the preoperative anesthetic visit with a detailed questionnaire. Concomitant diseases included: cardiovascular—atrial fibrillation, congestive heart failure (only NYHA classes III and IV were recorded), hypertension, myocardial infarction, internal carotid artery stenosis and extracardiac arteriopathy; metabolic—thyroid disorders, dyslipidemia, impaired glucose tolerance, diabetes; pulmonary—chronic obstructive pulmonary disease; renal—acute kidney injury and chronic renal insufficiency; neurological—stroke, transient ischemic attack (TIA). Data regarding smoking prior to the operation was also recorded. We used EuroScore Logistics 2 scale to calculate the perioperative risk for each patient.
We collected data regarding the postoperative outcome, which included the following information: intubation time, hospital length of stay, ICU length of stay, 30-day and 1-year mortality, as well as postoperative complications (cardiac and pulmonary, neurological, renal, infectious) using chart review. All laboratory testing was performed as part of routine preoperative and postoperative care. All biomarkers were collected in the morning, by the clinical staff, transported to the central laboratory immediately after collection and processed in the clinical lab.
Both pre-operative evaluation in the cardiac surgery outpatient clinic and premedication anesthetic assessment was performed to ensure patient safety. Intraoperative surgical and anesthetic approach followed a well-established local protocol. All patients were anesthetized with intravenous induction of general anaesthesia using fentanyl and etomidate, followed by pancuronium for muscle relaxation to facilitate tracheal intubation. For maintenance of general anesthesia an inhalational agent (sevoflurane) was used along with additional doses of fentanyl for pain control and pancuronium for muscle relaxation. Heparin was administered intravenously before initiation of the cardio-pulmonary bypass (CPB) and was guided by ACT (activated clotting time). Data regarding the procedure included the following information: operating time, cardiopulmonary bypass time, cross-clamping time and the volume of postoperative drainage.
After the operation and after weaning the patient from CPB, protamine sulphate was used to reverse the action of heparin guided by ACT. After the operation patients were transferred to cardiac ICU and remained intubated and mechanically ventilated as long as they required postoperative monitoring and treatment. Postoperative pain was controlled with intravenous morphine infusion and non-opioid analgesic administration (paracetamol or metamizole). Postoperatively patients were sedated with either propofol or dexmedetomidine, pain control was provided by multimodal analgesia (continuous intravenous morphine and non-opioid analgesic medications). After meeting extubation protocol criteria patients were extubated and transferred to the cardiac surgery ward.
2.3. Ethical Consideration
According to the Declaration of Helsinki this study has been submitted to the bioethical committee and received a waiver due to the retrospective character (Bioethical Committee of Pomeranian Medical University in Szczecin, Poland, decision no. KB-0012/257/06/18, 28.06.2018). Prior to the operation each patient signed a written informed consent for both surgery and anesthesia with a consent for research data collection. All analyzed data was anonymous to ensure confidentiality.
2.4. White Cell Biomarkers and CRP Analysis
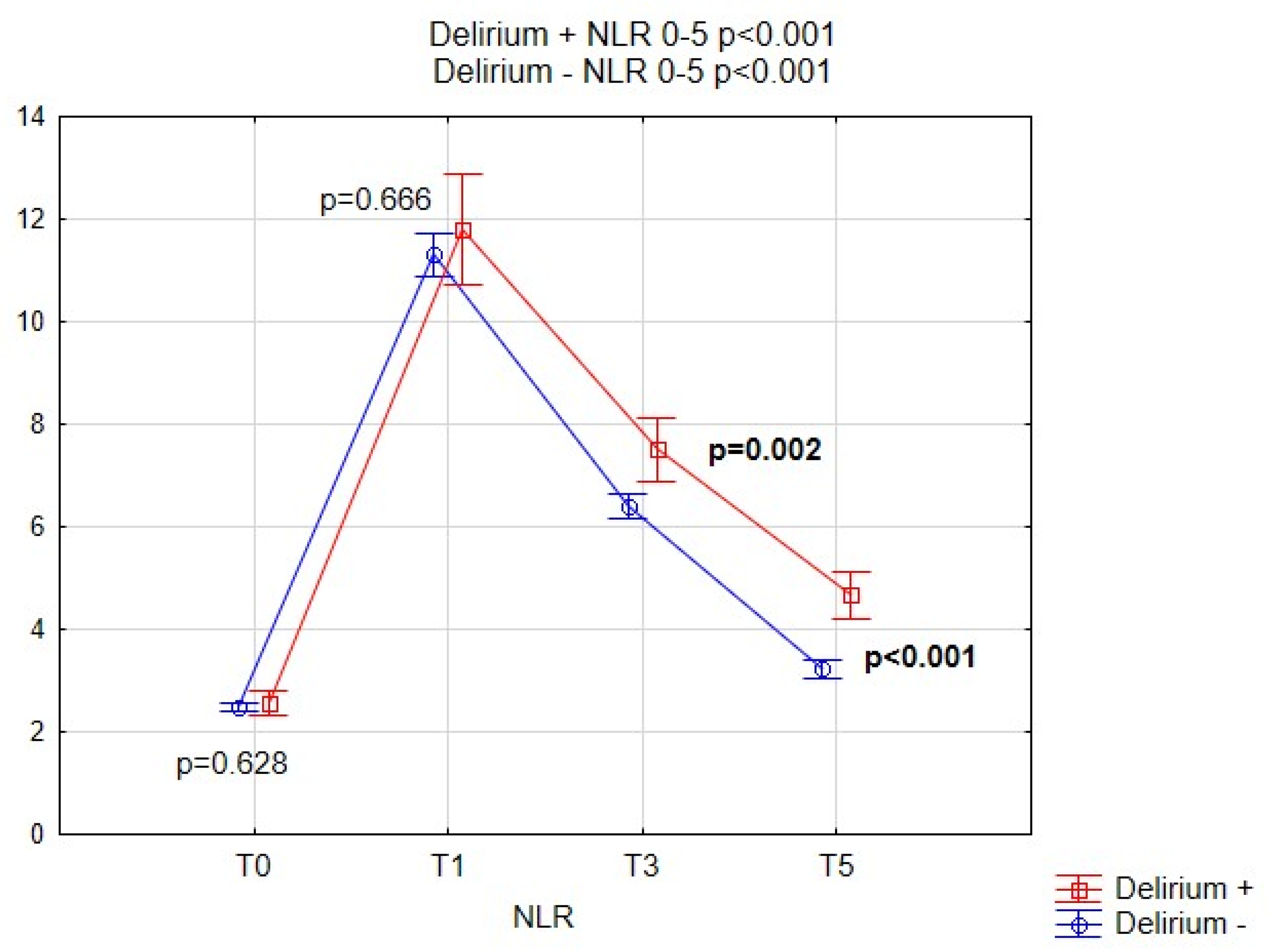
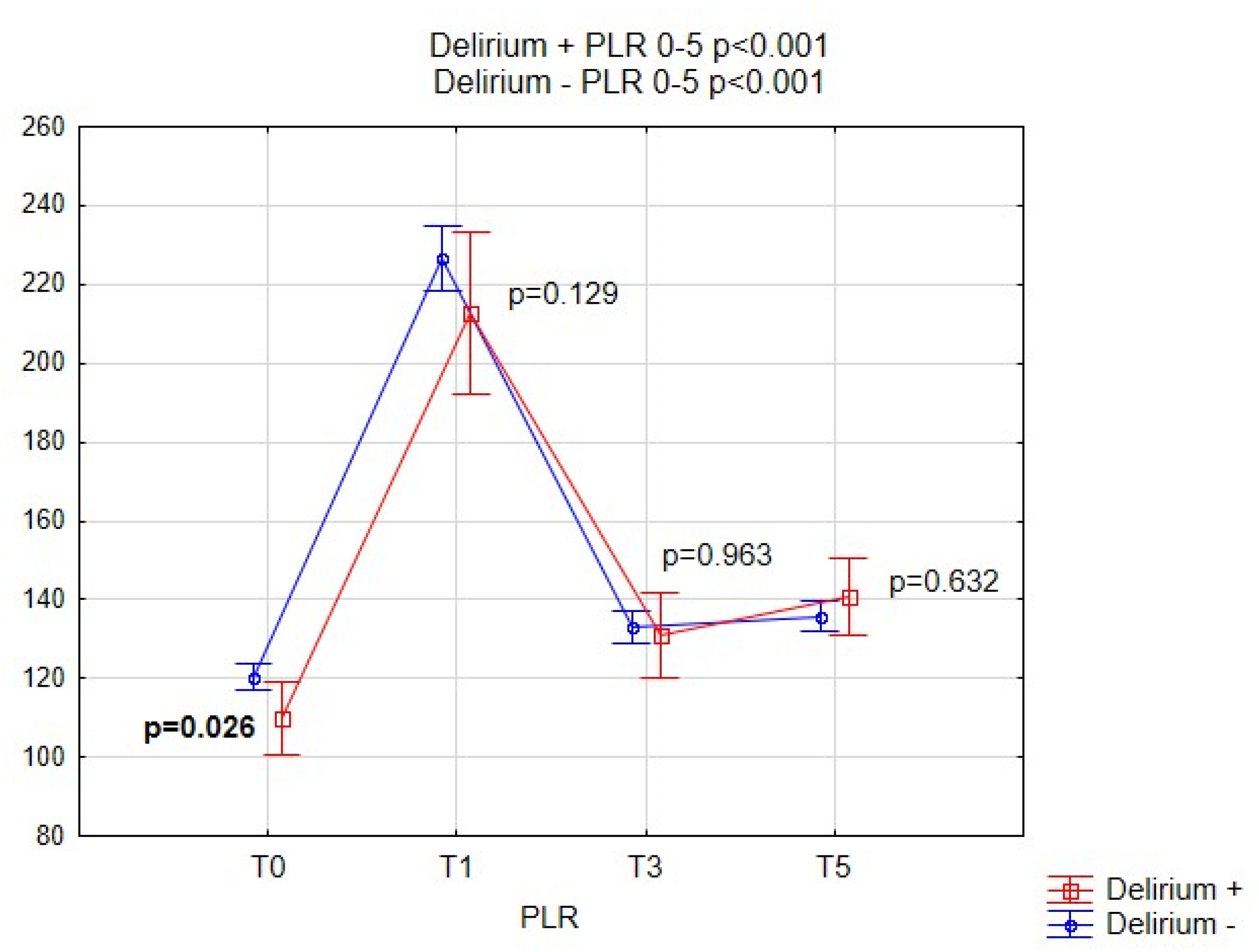
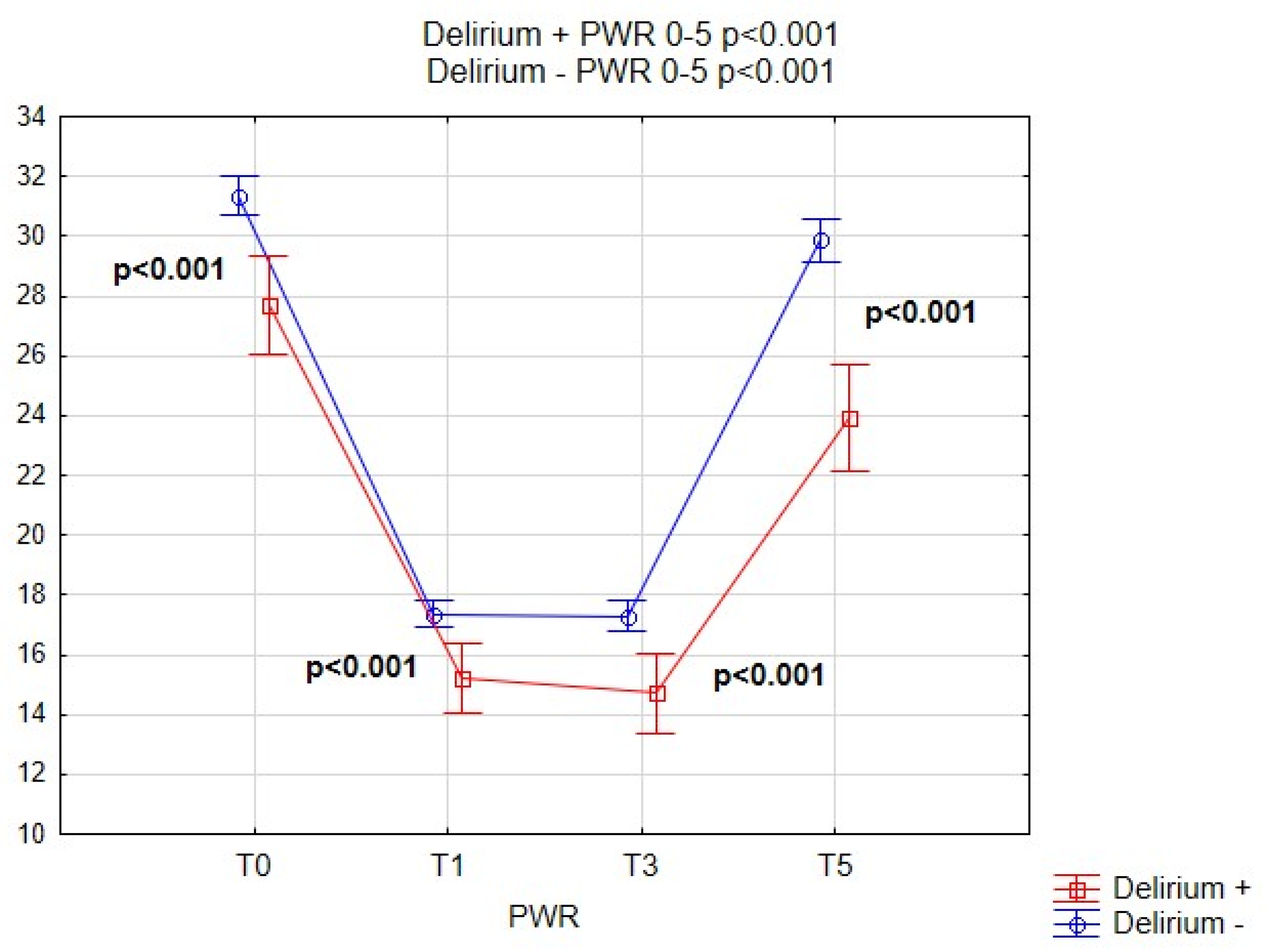
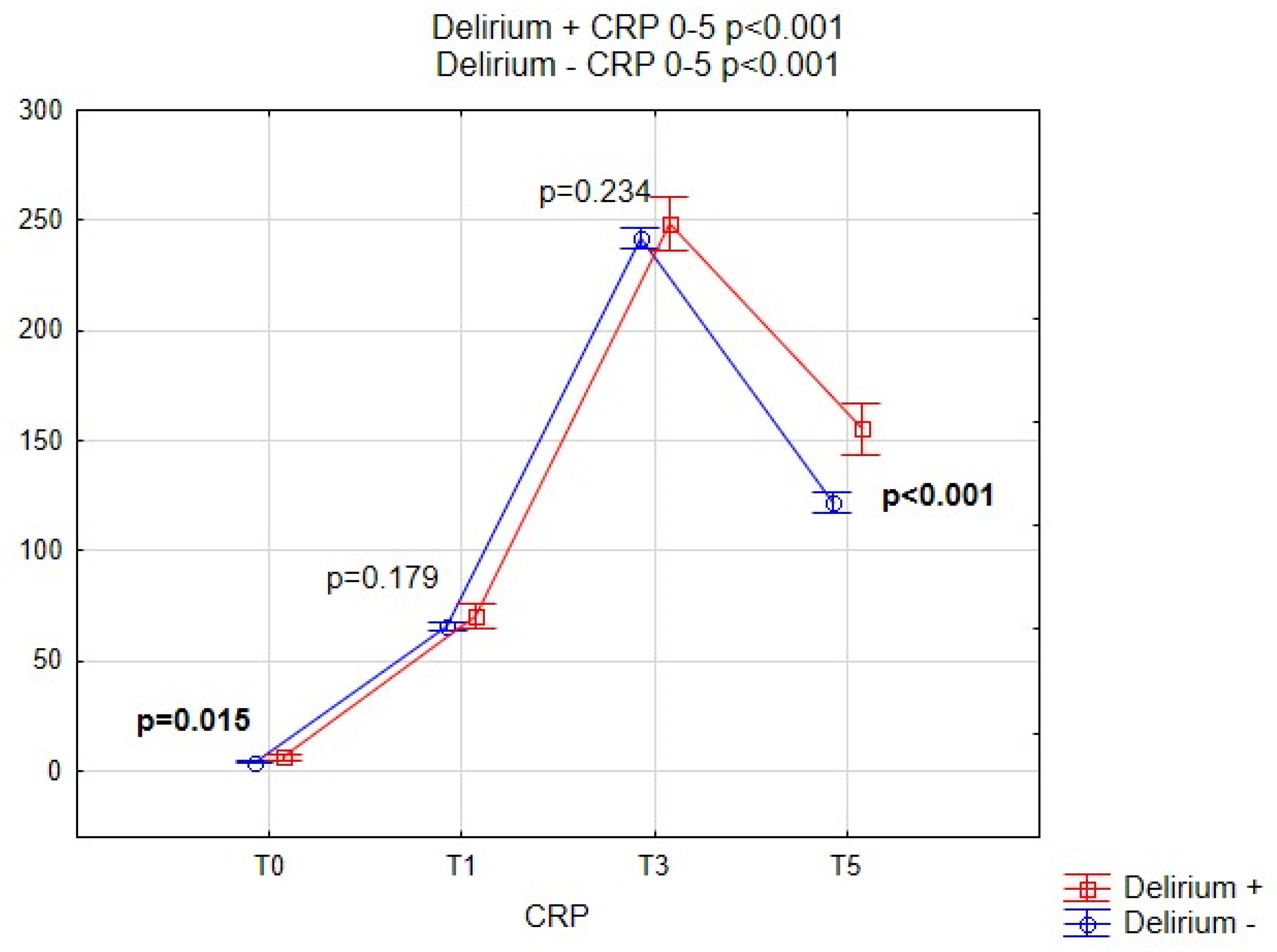
The WBC counts and CRP level were evaluated as part of routine perioperative testing. The blood was collected preoperatively (time T0, i.e., blood collected at admission, 24 h prior to surgery) and postoperatively (time T1, T3, T5 at day 1, 3, 5) after CABG. Blood morphology with full leukocyte differentiation was determined using the Sysmex XN-2000 analyzer the FSC, SSC DIFF, impedance, and spectrophotometric methods with sodium lauryl sulfate were used to determine hemoglobin. The C-reactive protein level was determined by the immunoturbidimetric method using a Roche Cobas 8000 analyzer. We calculated the neutrophil-to-lymphocyte ratio by dividing the absolute neutrophil count by the absolute lymphocyte count. The platelet-to-lymphocyte ratio was calculated by dividing the absolute platelet count over the absolute lymphocyte count. We calculated platelet-to-WBC ratio by dividing by the absolute platelet count over the WBC.
2.5. Delirium Assesment
We used the Polish version of the CAM-ICU test to screen all patients for delirium in the cardiac -ICU and in the post-operative ward [
6]. CAM-ICU was performed twice a day (morning and evening) during the first 6 days of the postoperative course. The team of nurses, anesthesiologists, intensivists and cardiac surgeons were involved in this process. The final delirium diagnosis was made by consultant neurologist using the standard criteria of Diagnostic Statistical Manual of Mental Disorders, fifth edition [
1]. The initial delirium screening was done in sedated patients in the cardiac-ICU by a nurse and a doctor (either of the above). Subsequent observations were carried out in all patients after they have been extubated (usually within 12 h after CABG).
2.6. Statistical Analysis
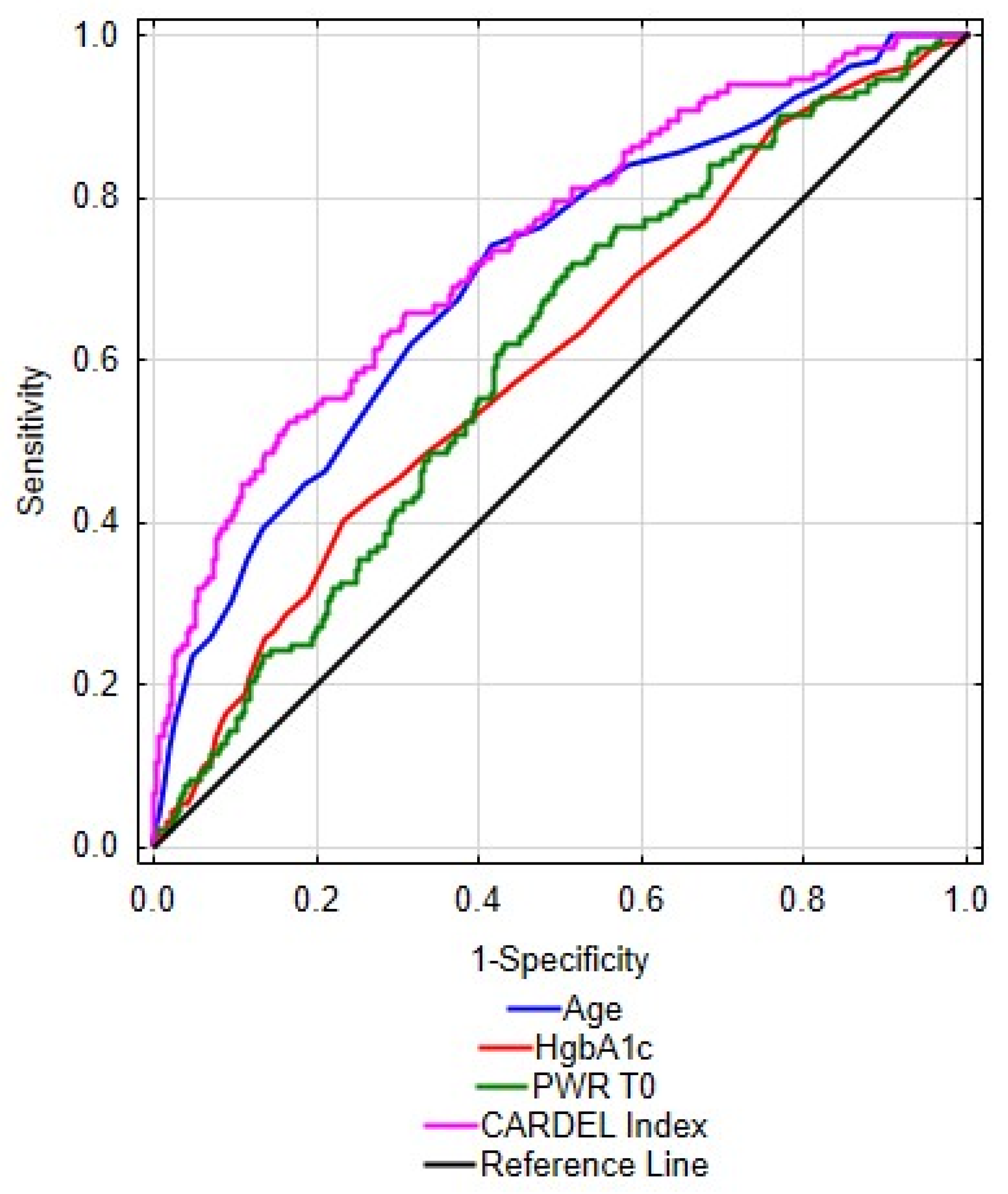
In order to characterize the population of this study we used descriptive statistics. We used proportions to present categorical variables and Chi-square test for comparison between the groups. Continuous variables were presented as means with standard deviation. We used Mann–Whitney U-test to compare baseline characteristics between patients with and without delirium. Spearman’s correlation coefficient was used to analyze the correlations between quantitative variables. In the next step, we used multivariate logistic regression analysis to find parameters most strongly and independently related to the occurrence of delirium. The multivariate models were constructed by forward selection of independent variables with two different Wald p-values required for inclusion. The “exploratory” model used classical p < 0.05 threshold, while the “reliable” model used p < 0.001 threshold. The lower threshold was applied as a correction for multiple comparisons, to prevent inclusion of variables only randomly associated with delirium into the reliable predictive model (nearly 50 independent pre-operative variables were analyzed as potential predictors of delirium, so the Bonferroni-corrected p is 0.05/50 = 0.001). Based on the reliable multivariate model parameters and depending on the contribution of each analyzed variable a formula for optimal prediction of delirium was calculated and presented as CARDEL Index (CARdiac DELirium Index). We also performed a receiver operating characteristic (ROC) analysis to determine the diagnostic value of the CARDEL index and its components for predicting the delirium. The cut-off points, which maximized Youden index (sensitivity + specificity − 1) were presented. Statistical significance was determined as p value below 0.05. The data was analyzed using Statistica 13 software with Medical Bundle 4.0.
4. Discussion
In this analysis of a large database including a homogenous group of patients undergoing CABG, we identified the platelet-to-WBC ratio (PWR) as a novel and independent predictor of postoperative delirium in patients undergoing planned cardiac surgery. A lower Platelet/WBC ratio was independently associated with a higher risk of postoperative delirium in patients undergoing CABG. To our knowledge, this is the first study to identify the Platelet-to-WBC ratio as a predictor of postoperative delirium after cardiac surgery. The mechanistic relationship between the PWR and delirium remains to be elucidated. The pre-operative level of white blood cells, along with the platelet level and their derived ratios may be used as surrogates for the baseline health status of patients in the pre-operative period. Those levels and ratios differ in patients who develop post-operative delirium due to neuroinflammation or immune system imbalance.
Not enough is known regarding the pathogenesis of delirium [
30]. Further identification of biomarkers may be helpful in broader understanding of pathogenic mechanisms, prognosis and diagnosis of delirium. The delirium markers identified so far point to inflammation and oxidative stress as the underlying mechanisms of delirium pathogenesis [
9,
10,
31]. The identification of known markers is expensive and time consuming, therefore it serves research purposes rather than being used in everyday clinical practice. An ideal biomarker should be cheap, repeatable, easily available, highly sensitive and very specific. The hematology parameters – differential white cell count seem to meet most of the above-mentioned criteria for an ideal diagnostic or prognostic marker. Numerous studies have shown the relationship between elevated NLR and cerebrovascular diseases [
21], schizophrenia [
16], Alzheimer’s disease, disease severity and poor prognosis in cardiovascular diseases [
19] or cancer [
24,
25].
The response of the immune system induced by surgical stress leads to an increase in the neutrophil count accompanied by the concomittant decrease in the lymphocyte count, along with a decrease in platelet count [
32,
33]. It has been shown that the composition of peripheral blood cells has been associated with the risk of post-operative complications in patients undergoing high-risk vascular procedures [
34]. When considering delirium, a certain degree of neuroinflammation may be seen as elevation in the level of neutrophils and the neutrophil-to-lymphocyte ratio [
35]. Moreover, a study performed by Egberts et al. pointed to the potential relationship between impaired NLR and delirium in the elderly population [
17]. The NLR level has been proposed as a novel biomarker in various inflammatory or metabolic diseases (i.e., SLE, ulcerative colitis, inflammatory arthritis, diabetes mellitus, coronary artery disease), but its value has not been proven in patients with delirium in our study [
36].
Some studies indicate a superior role of PLR over NLR [
37], very numerous studies dispute the role of the commonest derived parameter—the platelet-to-white blood cell ratio—calculated from blood morphology, without the need to perform the differential white cells analysis, which makes it very inexpensive and easy to obtain. Our study has shown that that lower pre-operative mean PLR values and lower PWR values were found in patients with postoperative delirium. The association was strongest for PWR and remained significant at T1 (
p < 0.001), T3 (
p < 0.001) and T5 (
p < 0.001). PWR has recently been shown to be an independent prognostic predictor for outcomes in some diseases. According to Chen et al. the platelet-to-WBC ratio on admission to the hospital may be useful at predicting the 90-day outcome in patients with ischemic stroke who received intravenous thrombolysis [
38]. It was also useful in predicting post-operative infectious complications after radical nephrectomy in patients with renal cancer [
39].
The mechanisms of neuroinflammation in patients undergoing cardio-pulmonary bypass have been described previously and the role of neutrophils in this process must be acknowledged to better understand the mechanisms leading to changes in serum NLR and PWR. We hypothesize that changes in the white blood cells differential count, as well as the CRP concentration may show that post-cardiac surgery delirium is associated with inadequate immune system response. Growing evidence suggests that neutrophils and lymphocytes are major effectors of acute inflammation, including neuroinflammation in delirium among elderly patients and post-stroke delirium [
17,
40]. The non-specific immune system activation, depicted by an increase in the neutrophil count and a decrease in the lymphocyte count, may be the first line response during generalized stress, leading to an imbalance between neutrophils and lymphocytes in the peripheral circulation [
41,
42]. The degree of neutrophil count elevation and the subsequent NLR rise may depict the degree of neuroinflammation. This observation may be the basis of delirium prediction by systemic inflammatory indicators [
35]. Lymphopenia has been described as a known predictor of mortality in critically ill patients and may be regarded as a bedside marker of immunosuppression [
33,
35]. Inoue et al. have undertaken a study to determine whether lymphopenia was associated with ICU delirium. These researchers reported that patients with decreased lymphocyte levels showed a trend towards a higher chance of ICU delirium (
p = 0.07) [
30]. An imbalance of derived inflammatory white blood cell factors (NLR, PWR) may reflect subclinical inflammation [
33].
One of the aims of the study performed by us was to create a model that, using objective pre-operative clinical and laboratory data, would be useful in assessing the risk of delirium after CABG. The index being a function of age, HbA1c and PWR was analyzed as a CARDEL index to check its diagnostic efficiency. In addition, it was checked whether correlations exist between the above three variables. Variables included in the model are completely uncorrelated and therefore completely independent of each other, therefore the index CARDEL can be treated as an indicator for delirium prediction. The analysis showed that the CARDEL index is better in predicting the development of delirium after CABG than any of these factors alone. An important virtue of this model is the use of information regarding the components of the immune system and preoperative laboratory values, because it has been suggested that the pathophysiology of delirium is multifactorial. The CARDEL index is simple to count, easy to analyze and, above all, cheap, because it was calculated using routine, easily accessible and objective pre-operative parameters. However, it must be underlined that this is a preliminary analysis of the CARDEL index and further research must follow to confirm these results. We plan to perform an independent prospective observational study in a different patient population to further investigate the results obtained in this study.
No other research reported a predictive model based on routine pre-operative values for predicting the occurrence of delirium after cardiac surgery. A systematic analysis of the studies involving predictive models for delirium in the elderly population in the hospital was carried out by Lindroth et al. [
43] Their analysis covered information retrieved from accessible databases (CINAHL, Cochrane, Embase PubMed, PsychINFO, SocinFO, Web of Science) from 1 January 1990 until 31 December 2016 and included studies involving patients over 60 years old, hospitalized, in which the authors developed and approved a prognostic prediction model for delirium. A priori analyzes excluded patients with delirium associated with alcohol and analyzes involving less than 50 people. After a complete review of 192 studies, 27 studies were included in the final analysis. Twenty-three forecasting models of delirium were identified. The assessment of delirium was usually unsystematic, which resulted in a varied incidence of delirium in the populations studied. Fourteen models have been externally validated with ROC AUC between 0.52 and 0.94. The authors identified design constraints, data collection methods and model metrics reporting statistics, and concluded in their summary that delirium prediction models, exhibit variable and inadequate prediction capabilities [
43]. Lindroth et al. emphasized the need to develop robust models for predicting delirium in hospitalized patients to create predictive systems for specific populations [
43]. A recent prospective observational study called DELIAS Study was performed by Kotfis et al. in patients with acute ischemic stroke, with an aim to assess whether the ratio of neutrophil-to-lymphocyte count can be used as a potential prognostic marker for delirium in patients with ischemic stroke [
40]. As a result of various combinations of laboratory inflammatory markers and clinical parameters, the authors proposed the DELIAS index based on logistic regression, with the area under the ROC curve of 0.801 and
p < 0.001). The authors concluded that NLR can be considered as a potential predictor of delirium after acute ischemic stroke, and the DELIAS index, easily calculated on the basis of combined laboratory and clinical parameters, shows the highest predictive value for delirium in the analyzed group of patients presenting with acute ischemic stroke [
40].
This study exhibits certain limitations. First of all, this study is a single-center analysis and further studies are necessary to confirm our results in a different population of patients. Second, this was a retrospective analysis, therefore the data available may be limited and may not include all information. Third, the observational design of the study may limit the ability to identify all causal associations. Fourth, certain co-morbidities might influence the mean levels of white cell subtypes although patients with chronic inflammation and inflammatory diseases were excluded from the analysis. Fifth, delirium assessment was completed by routine clinical staff and it is well documented that clinical staff routinely miss delirium, especially hypoactive delirium.
A definite strength of this analysis is a very large number of patients included. This provides reliable data about easy to obtain and calculate biomarkers. The value of white cell count markers cannot be overestimated in patients undergoing surgery, as this laboratory workup is available from almost every hospitalized patient. Another important factor is the availability of serial measurements of NLR, PLR and PWR based on white cell count as this is easily obtainable at pre-defined time-points before and after the surgery.

 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}