Biosocial Determinants of Persistent Schistosomiasis among Schoolchildren in Tanzania despite Repeated Treatment

Abstract
:1. Introduction
2. Materials and Methods
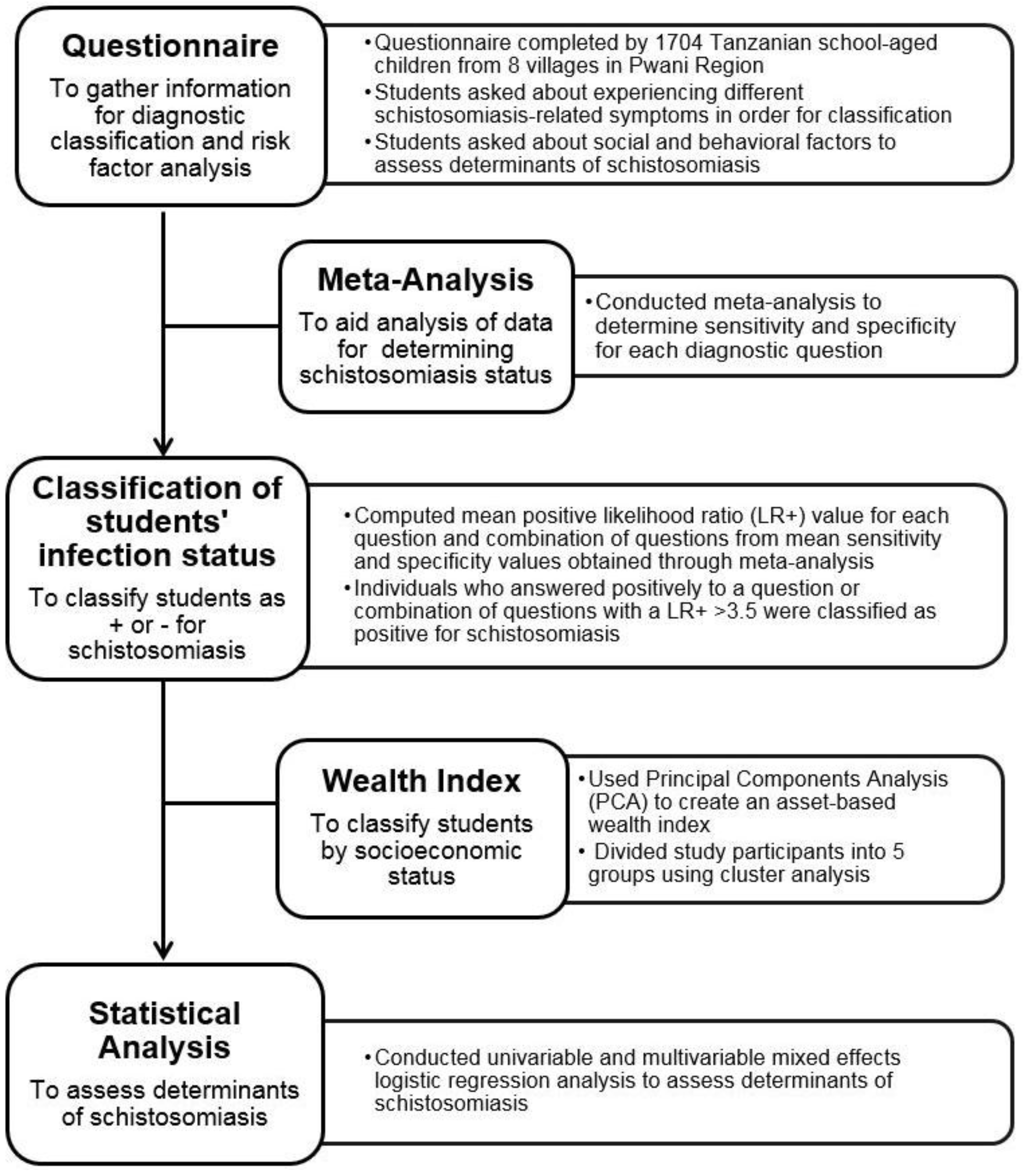
2.1. Overview of Study
2.2. Questionnaire
2.2.1. Study Area
2.2.2. Study Variables
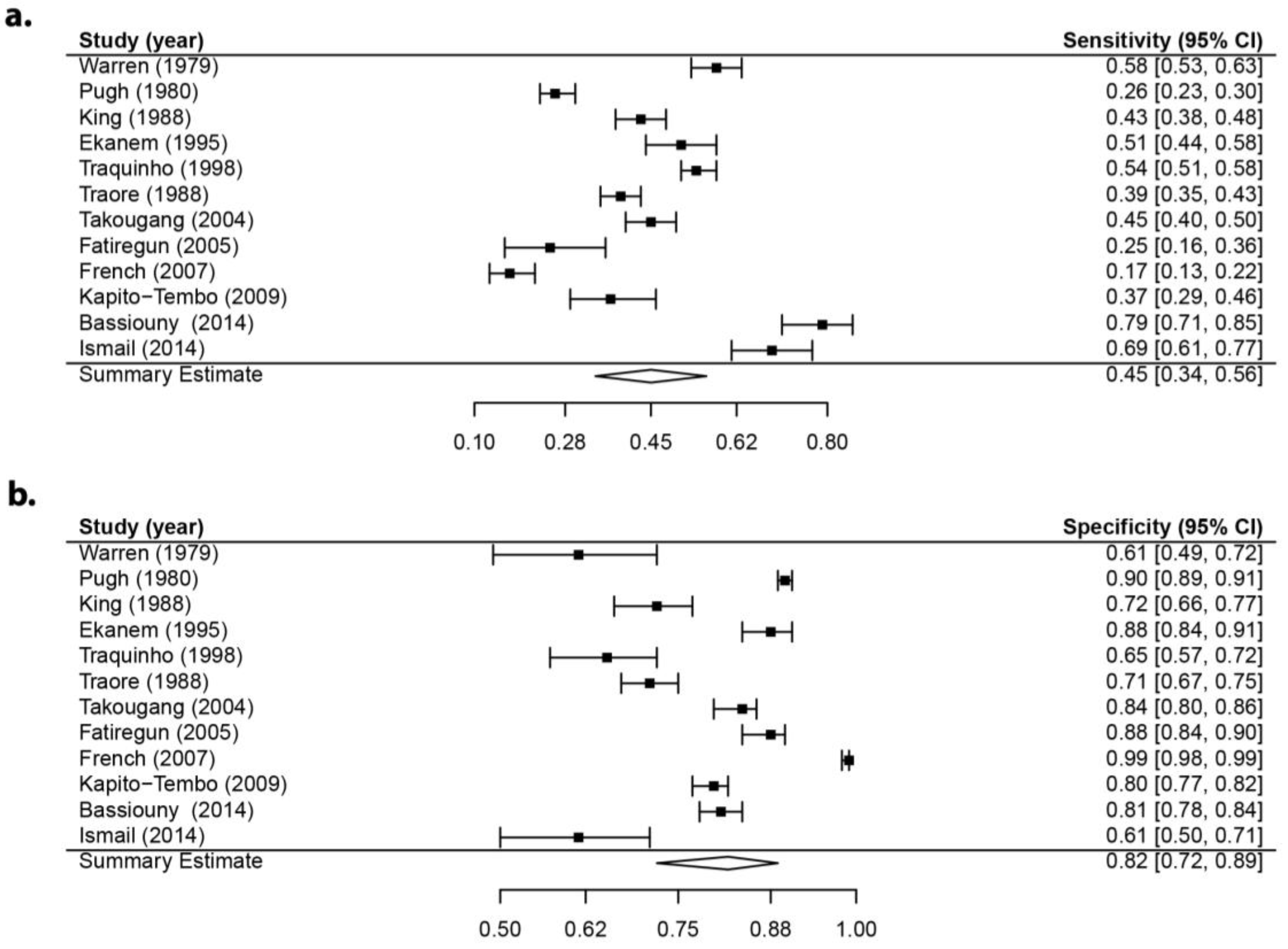
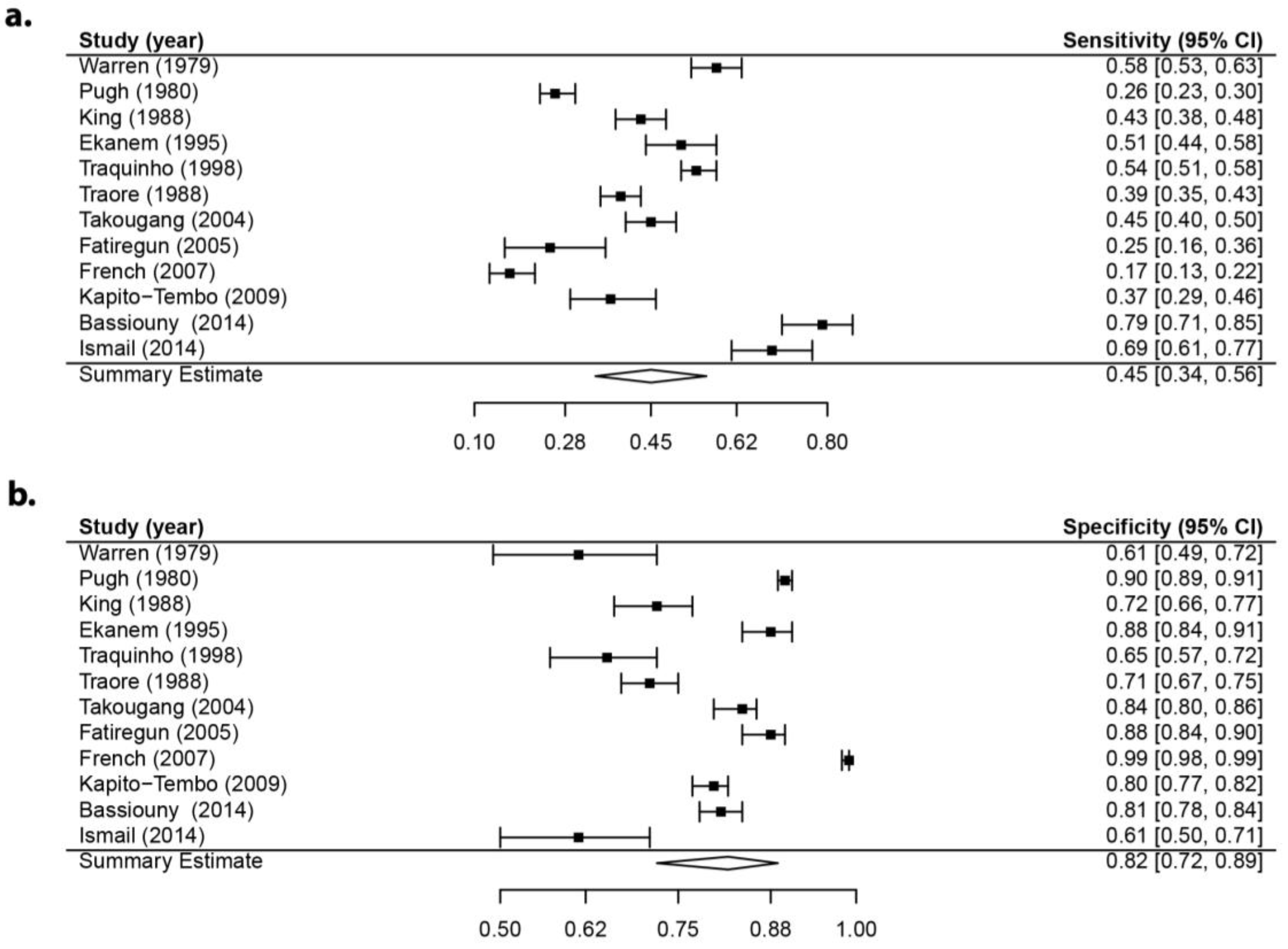
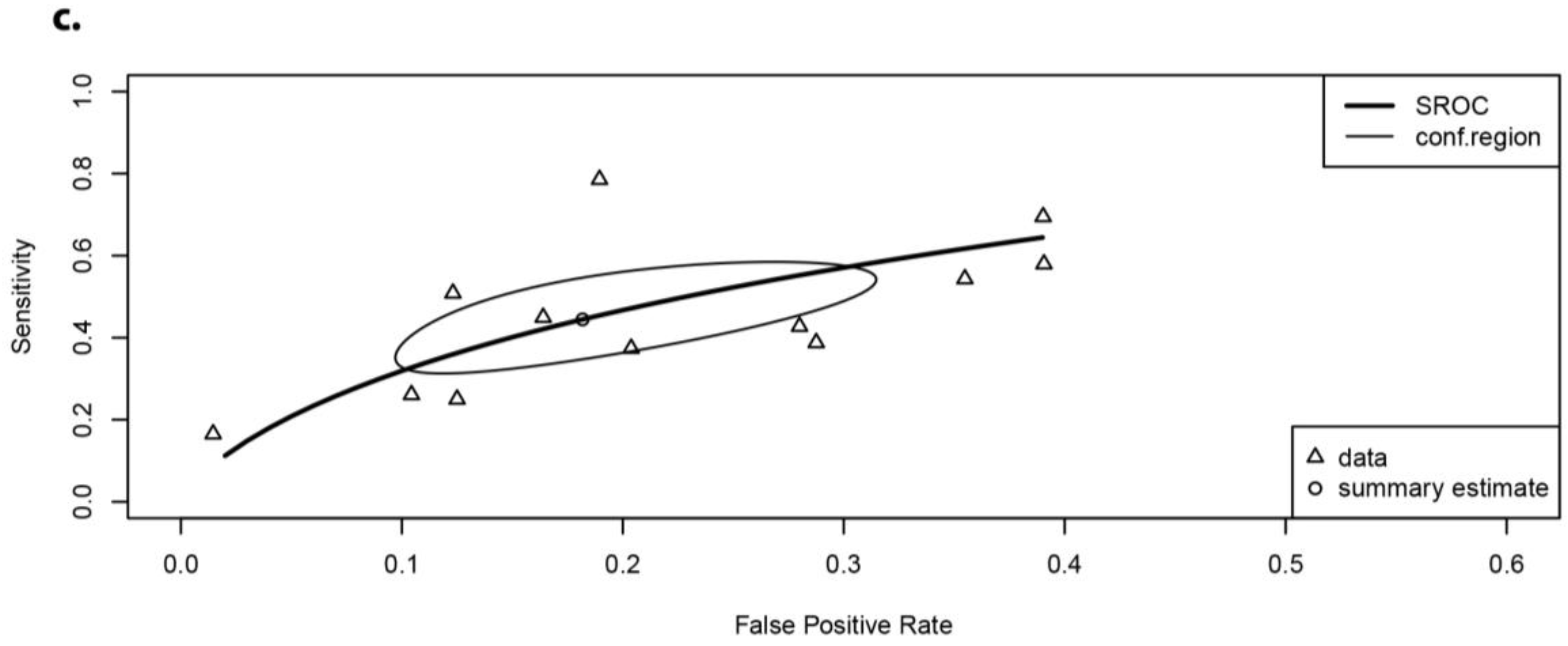
2.3. Meta-Analysis
2.3.1. Deriving Questions to Classify Infected Individuals
2.3.2. Meta-Analysis Procedure
2.3.3. Study Identification
2.3.4. Study Inclusion Criteria
2.3.5. Data Extraction
2.3.6. Quality Assessment
2.3.7. Analysis Procedure
2.4. Classifying Infection Status of Individuals
2.5. Wealth Index
2.6. Statistical Analysis
2.7. Ethical Approval
3. Results
3.1. Meta-Analysis
3.2. Wealth Index
3.3. Factors Associated with Self-Reported Schistosomiasis
3.3.1. General Characteristics of Study Population
3.3.2. Statistical Analyses
4. Discussion
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Colley, D.G.; Bustinduy, A.L.; Secor, W.E.; King, C.H. Human schistosomiasis. Lancet 2014, 383, 2253–2264. [Google Scholar] [CrossRef]
- Steinmann, P.; Keiser, J.; Bos, R.; Tanner, M.; Utzinger, J. Schistosomiasis and water resources development: Systematic review, meta-analysis, and estimates of people at risk. Lancet Infect. Dis. 2006, 6, 411–425. [Google Scholar] [CrossRef]
- Mazigo, H.D.; Nuwaha, F.; Kinung’hi, S.M.; Morona, D.; Pinot de Moira, A.; Wilson, S.; Heukelbach, J.; Dunne, D.W. Epidemiology and control of human schistosomiasis in Tanzania. Parasites Vectors 2012, 5, 274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health and Social Welfare (MoHSW). Tanzania Mainland Strategic Master Plan for the Neglected Tropical Diseases Control Program, 2012–2017; MoHSW: Dar es Salaam, Tanzania, 2012.
- King, C.H.; Keating, C.E.; Muruka, J.F.; Ouma, J.H.; Houser, H.; Siongok, T.K.A.; Mahmoud, A.A.F. Urinary tract morbidity in schistosomiasis haematobia: Associations with age and intensity of infection in an endemic area of Coast Province, Kenya. Am. J. Trop. Med. Hyg. 1988, 39, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Kabatereine, N.B.; Brooker, S.; Tukahebwa, E.M.; Kazibwe, F.; Onapa, A.W. Epidemiology and geography of Schistosoma mansoni in Uganda: Implications for planning control. Trop. Med. Int. Health 2004, 9, 372–380. [Google Scholar] [CrossRef] [PubMed]
- WHO. Schistosomiasis: Progress Report 2001–2011, Strategic Plan 2012–2020; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- WHO. Preventive Chemotherapy in Human Helminthiasis: Coordinated Use of Anthelminthic Drugs in Control Interventions: A Manual for Health Professionals and Programme Managers; WHO: Geneva, Switzerland, 2006; ISBN 978-92-4-154710-9. [Google Scholar]
- Cioli, D.; Pica-Mattoccia, L.; Basso, A.; Guidi, A. Schistosomiasis control: Praziquantel forever? Mol. Biochem. Parasitol. 2014, 195, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.J.; Savage, G.B.; Gray, D.J.; Atkinson, J.M.; Soares Magalhães, R.J.; Nery, S.V.; McCarthy, J.S.; Velleman, Y.; Wicken, J.H.; Traub, R.J.; et al. Water, sanitation, and hygiene (WASH): A critical component for sustainable soil-transmitted helminth and schistosomiasis control. PLoS Negl. Trop. Dis. 2014, 8, e2651. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.G.P.; Olveda, R.M.; Chy, D.; Olveda, D.U.; Li, Y.; Harn, D.A.; Gray, D.J.; McManus, D.P.; Tallo, V.; Chau, T.N.P.; et al. Can mass drug administration lead to the sustainable control of schistosomiasis? J. Infect. Dis. 2014, 211, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Inobaya, M.; Olveda, R.; Chau, T.; Olveda, D.; Ross, A.G.P. Prevention and control of schistosomiasis: A current perspective. Res. Rep. Trop. Med. 2014, 65–75. [Google Scholar] [CrossRef]
- Secor, W.E. Water-based interventions for schistosomiasis control. Pathog. Glob. Health 2014, 108, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Gray, D.J.; McManus, D.P.; Li, Y.; Williams, G.M.; Bergquist, R.; Ross, A.G. Schistosomiasis elimination: Lessons from the past guide the future. Lancet Infect. Dis. 2010, 10, 733–736. [Google Scholar] [CrossRef]
- Seto, E.Y.W.; Remais, J.V.; Carlton, E.J.; Wang, S.; Liang, S.; Brindley, P.J.; Qiu, D.; Spear, R.C.; de Wang, L.; Wang, T.P.; et al. Toward sustainable and comprehensive control of Schistosomiasis in China: Lessons from Sichuan. PLoS Negl. Trop. Dis. 2011, 5, 8–11. [Google Scholar] [CrossRef] [PubMed]
- N’Goran, E.K.; Utzinger, J.; N’Guessan, A.N.; Müller, I.; Zamblé, K.; Lohourignon, K.L.; Traoré, M.; Sosthène, B.A.; Lengeler, C.; Tanner, M. Reinfection with Schistosoma haematobium following school-based chemotherapy with praziquantel in four highly endemic villages in Côte d’Ivoire. Trop. Med. Int. Health 2001, 6, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Masaku, J.; Madigu, N.; Okoyo, C.; Njenga, S.M. Current status of Schistosoma mansoni and the factors associated with infection two years following mass drug administration programme among primary school children in Mwea irrigation scheme: A cross-sectional study. BMC Public Health 2015, 15, 739. [Google Scholar] [CrossRef] [PubMed]
- Kariuki, H.C.; Madsen, H.; Ouma, J.H.; Butterworth, A.E.; Dunne, D.W.; Booth, M.; Kimani, G.; Mwatha, J.K.; Muchiri, E.; Vennervald, B.J. Long term study on the effect of mollusciciding with niclosamide in stream habitats on the transmission of schistosomiasis mansoni after community-based chemotherapy in Makueni District, Kenya. Parasites Vectors 2013, 6, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimes, J.E.; Croll, D.; Harrison, W.E.; Utzinger, J.; Freeman, M.C.; Templeton, M.R. The roles of water, sanitation and hygiene in reducing schistosomiasis: A review. Parasites Vectors 2015, 8, 156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimes, J.E.T.; Croll, D.; Harrison, W.E.; Utzinger, J.; Freeman, M.C.; Templeton, M.R. The relationship between water, sanitation and schistosomiasis: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2014, 8, e3296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, M.C.; Ogden, S.; Jacobson, J.; Abbott, D.; Addiss, D.G.; Amnie, A.G.; Beckwith, C.; Cairncross, S.; Callejas, R.; Colford, J.M.; et al. Integration of water, sanitation, and hygiene for the prevention and control of neglected tropical diseases: A rationale for inter-sectoral collaboration. PLoS Negl. Trop. Dis. 2013, 7, e2439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bardosh, K. Global aspirations, local realities: The role of social science research in controlling neglected tropical diseases. Infect. Dis. Poverty 2014, 3, 35. [Google Scholar] [CrossRef] [PubMed]
- Allotey, P.; Reidpath, D.D.; Pokhrel, S. Social sciences research in neglected tropical diseases 1: The ongoing neglect in the neglected tropical diseases. Health Res. Policy Syst. 2010, 8, 32. [Google Scholar] [CrossRef] [PubMed]
- Gazzinelli, A.; Velasquez-Melendez, G.; Crawford, S.B.; LoVerde, P.T.; Correa-Oliveira, R.; Kloos, H. Socioeconomic determinants of schistosomiasis in a poor rural area in Brazil. Acta Trop. 2006, 99, 260–271. [Google Scholar] [CrossRef] [PubMed]
- Michael, E.; Madon, S. Socio-ecological dynamics and challenges to the governance of Neglected Tropical Disease control. Infect. Dis. Poverty 2017, 6, 35. [Google Scholar] [CrossRef] [PubMed]
- Klepac, P.; Metcalf, C.J.E.; McLean, A.R.; Hampson, K. Towards the endgame and beyond: Complexities and challenges for the elimination of infectious diseases. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2013, 368, 20120137. [Google Scholar] [CrossRef] [PubMed]
- Nzallah, A.W. Parasitological Survey of Schistosoma haematobium Infection among Schoolchildren in Mkuranga District, Tanzania. Ph.D. Thesis, Sokoine University of Agriculture, Morogoro, Tanzania, 2015. [Google Scholar]
- Red Urine Study Group. Identification of High-Risk Communities for Schistosomiasis in Africa: A Multicountry Study Prepared by the Red Urine Study Group; TDR/SER/PRS/15; Social and Economic Research Report Series; WHO: Geneva, Switzerland, 1995. [Google Scholar]
- Lengeler, C.; Utzinger, J.; Tanner, M. Questionnaires for rapid screening of schistosomiasis in sub-Saharan Africa. Bull. World Health Organ. 2002, 80, 235–242. [Google Scholar] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Gray, D.J.; Ross, A.G.; Li, Y.-S.; McManus, D.P. Diagnosis and management of schistosomiasis. BMJ 2011, 342, d2651. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Rutter, C.M.; Gatsonis, C.A. A hierarchical regression approach to meta-analysis of diagnostic test accuracy evaluations. Stat. Med. 2001, 20, 2865–2884. [Google Scholar] [CrossRef] [PubMed]
- Reitsma, J.B.; Glas, A.S.; Rutjes, A.W.S.; Scholten, R.J.P.M.; Bossuyt, P.M.; Zwinderman, A.H. Bivariate analysis of sensitivity and specificity produces informative summary measures in diagnostic reviews. J. Clin. Epidemiol. 2005, 58, 982–990. [Google Scholar] [CrossRef] [PubMed]
- Harbord, R.M.; Deeks, J.J.; Egger, M.; Whiting, P.; Sterne, J.A.C. A unification of models for meta-analysis of diagnostic accuracy studies. Biostatistics 2007, 8, 239–251. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Macaskill, P.; Irwig, L. The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J. Clin. Epidemiol. 2005, 58, 882–893. [Google Scholar] [CrossRef] [PubMed]
- Doebler, P. Mada: Meta-Analysis of Diagnostic Accuracy. R Package Version 0.5.7. 2015. Available online: https://CRAN.R-project.org/package=mada (accessed on 1 September 2017).
- Deeks, J.J.; Altman, D.G. Diagnostic tests 4: Likelihood ratios. BMJ 2004, 329, 168–169. [Google Scholar] [CrossRef] [PubMed]
- Attia, J. Moving beyond sensitivity and specificity: Using likelihood ratios to help interpret diagnostic tests. Aust. Prescr. 2003, 26, 111–113. [Google Scholar] [CrossRef]
- Jaeschke, R.; Guyatt, G.H.; Sackett, D.L. Users’ guides to the medical literature. III. How to use an article about a diagnostic test. B. What are the results and will they help me in caring for my patients? The Evidence-Based Medicine Working Group. JAMA 1994, 271, 703–707. [Google Scholar] [CrossRef] [PubMed]
- Filmer, D.; Pritchett, L. Estimating wealth effects without expenditure data—Or tears: An application to educational enrollments in states of India. Demography 2001, 38, 115–132. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, D.J. Measuring inequality with asset indicators. J. Popul. Econ. 2005, 18, 229–260. [Google Scholar] [CrossRef]
- Vyas, S.; Kumaranayake, L. Constructing socio-economic status indices: How to use principal components analysis. Health Policy Plan. 2006, 21, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Houweling, T.A.J.; Kunst, A.E.; Mackenbach, J.P. Measuring health inequality among children in developing countries: Does the choice of the indicator of economic status matter? Int. J. Equity Health 2003, 12, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charrad, M.; Ghazzali, N.; Boiteau, V.; Niknafs, A. NbClust: An R package for determining the relevant number of clusters in a data set. J. Stat. Soft 2014, 61, 1–36. [Google Scholar] [CrossRef]
- Groll, A. Glmmlasso: Variable Selection for Generalized Linear Mixed Models by L1-Penalized Estimation. R Package Version 1.5.1. 2017. Available online: https://CRAN.R-project.org/package=glmmLasso (accessed on 1 September 2017).
- Tibshirani, R. Regression shrinkage and selection via the lasso. J. R. Stat. Soc. Ser. B 1996, 58, 267–288. [Google Scholar]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting linear mixed-effects models using LME4. J. Stat. Softw. 2015, 67. [Google Scholar] [CrossRef]
- Warren, K.S.; Mahmoud, A.A.F.; Muruka, J.F.; Whittaker, L.R. Schistosomiasis haematobia in Coast Province Kenya: Relationship between egg output and morbidity. Am. J. Trop. Med. Hyg. 1979, 28, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Wahab, M.F.; Esmat, G.; Ramzy, I.; Fouad, R.; Abdel-Rahman, M.; Yosery, A.; Narooz, S.; Strickland, G.T. Schistosoma haematobium infection in Egyptian schoolchildren: Demonstration of both hepatic and urinary tract morbidity by ultrasonography. Trans. R. Soc. Trop. Med. Hyg. 1992, 86, 406–409. [Google Scholar] [CrossRef]
- Ekanem, E.E.; Ejezie, G.C.; Asindi, A.A.; Antia-Obong, O.E. Urinary symptoms and blood pressure of children with Schistosoma haematobium infection in south-eastern Nigeria. East Afr. Med. J. 1995, 72, 486–489. [Google Scholar] [PubMed]
- Mtasiwa, D.; Mayombana, C.; Kilima, P.; Tanner, M. Validation of reagent sticks in diagnosing urinary schistosomiasis in an urban setting. East Afr. Med. J. 1996, 73, 198–200. [Google Scholar] [PubMed]
- Onayade, A.; Abayomi, I.; Fabiyi, A. Urinary schistosomiasis: Options for control within endemic rural communities: A case study in south-west Nigeria. Public Health 1996, 110, 221–227. [Google Scholar] [CrossRef]
- Mafe, M.A. The diagnostic potential of three indirect tests for urinary schistosomiasis in Nigeria. Acta Trop. 1997, 68, 277–284. [Google Scholar] [CrossRef]
- Traore, M.; Traore, H.A.; Kardorff, R.; Diarra, A.; Landoure, A.; Vester, U.; Doehring, E.; Bradley, D.J. The public health significance of urinary schistosomiasis as a cause of morbidity in two districts in Mali. Am. J. Trop. Med. Hyg. 1998, 59, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Traquinho, G.A.; Quintó, L.; Nalá, R.M.; Gama Vaz, R.; Corachan, M. Schistosomiasis in northern Mozambique. Trans. R. Soc. Trop. Med. Hyg. 1998, 92, 279–281. [Google Scholar] [CrossRef]
- Guyatt, H.; Brooker, S.; Lwambo, N.J.S.; Siza, J.E.; Bundy, D.A.P. The performance of school-based questionnaires of reported blood in urine in diagnosing Schistosoma haematobium infection: Patterns by age and sex. Trop. Med. Int. Health 1999, 4, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Takougang, I.; Meli, J.; Fotso, S.; Angwafo, F.; Kamajeu, R.; Ndumbe, P.M. Hematuria and dysuria in the self-diagnosis of urinary schistosomiasis among school-children in Northern Cameroon. Afr. J. Health Sci. 2004, 11, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Bowie, C.; Purcell, B.; Shaba, B.; Makaula, P.; Perez, M. A national survey of the prevalence of schistosomiasis and soil transmitted helminths in Malaŵi. BMC Infect. Dis. 2004, 4, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fatiregun, A.; Osungbade, K.; Olumide, E. Diagnostic performance of screening methods for urinary schistosomiasis in a school-based control programme, in Ibadan, Nigeria. J. Community Med. Prim. Health Care 2005, 17, 24–27. [Google Scholar] [CrossRef]
- French, M.D.; Rollinson, D.; Basáñez, M.G.; Mgeni, A.F.; Khamis, I.S.; Stothard, J.R. School-based control of urinary schistosomiasis on Zanzibar, Tanzania: Monitoring micro-haematuria with reagent strips as a rapid urological assessment. J. Pediatr. Urol. 2007, 3, 364–368. [Google Scholar] [CrossRef] [PubMed]
- Kapito-Tembo, A.P.; Mwapasa, V.; Meshnick, S.R.; Samanyika, Y.; Banda, D.; Bowie, C.; Radke, S. Prevalence distribution and risk factors for Schistosoma hematobium infection among school children in Blantyre, Malawi. PLoS Negl. Trop. Dis. 2009, 3, e361. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, B.A. Two practical and cost effective methods for urinary schistosomiasis screening in Yemeni schoolchildren. Iran. J. Public Health 2009, 38, 78–83. [Google Scholar]
- Kihara, J.; Mwandawiro, C.; Waweru, B.; Gitonga, C.W.; Brooker, S. Preparing for national school-based deworming in Kenya: The validation and large-scale distribution of school questionnaires with urinary schistosomiasis. Trop. Med. Int. Health 2011, 16, 1326–1333. [Google Scholar] [CrossRef] [PubMed]
- Banwat, M.E.; Ogbonna, C.; Daboer, J.C.; Chingle, M.P.; Envuladu, E.A.; Audu, S.; Lar, L.A. Prevalence of urinary schistosomiasis in school-aged children in Langai, Plateau State: Pre- and post-intervention. Niger. J. Med. 2012, 21, 146–149. [Google Scholar] [PubMed]
- Abou-Zeid, A.H.; Abkar, T.A.; Mohamed, R.O. Schistosomiasis infection among primary school students in a war zone, Southern Kordofan State, Sudan: A cross-sectional study. BMC Public Health 2013, 13, 643. [Google Scholar] [CrossRef] [PubMed]
- Bassiouny, H.K.; Hasab, A.A.; El-Nimr, N.A.; Al-Shibani, L.A.; Al-Waleedi, A.A. Rapid diagnosis of schistosomiasis in Yemen using a simple questionnaire and urine reagent strips. East. Mediterr. Health J. 2014, 20, 242–249. [Google Scholar] [PubMed]
- Ismail, H.; Hong, S.-T.; Babiker, A.; Hassan, R.; Sulaiman, M.; Jeong, H.-G.; Kong, W.-H.; Lee, S.-H.; Cho, H.-I.; Nam, H.-S.; et al. Prevalence, risk factors, and clinical manifestations of schistosomiasis among school children in the White Nile River basin, Sudan. Parasites Vectors 2014, 7, 478. [Google Scholar] [CrossRef] [PubMed]
- Bogoch, I.I.; Andrews, J.R.; Dadzie Ephraim, R.K.; Utzinger, J. Simple questionnaire and urine reagent strips compared to microscopy for the diagnosis of Schistosoma haematobium in a community in northern Ghana. Trop. Med. Int. Health 2012, 17, 1217–1221. [Google Scholar] [CrossRef] [PubMed]
- Pugh, R.N.H.; Bell, D.R.; Gilles, H.M. Malumfashi endemic diseases research project, XV. The potential medical importance of bilharzia in Northern Nigeria: A suggested rapid, cheap and effective solution for control of Schistosoma haematobium infection. Ann. Trop. Med. Parasitol. 1980, 74, 597–613. [Google Scholar] [CrossRef] [PubMed]
- Gabr, N.S.; Hammad, T.A.; Orieby, A.; Shawky, E.; Khattab, M.A.; Strickland, G.T. The epidemiology of schistosomiasis in Egypt: Minya Governorate. Am. J. Trop. Med. Hyg. 2000, 62, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Wahab, M.F.; Esmat, G.; Ramzy, I.; Narooz, S.; Medhat, E.; Ibrahim, M.; El-Boraey, Y.; Strickland, G.T. The epidemiology of schistosomiasis in Egypt: Fayoum Governorate. Am. J. Trop. Med. Hyg. 2000, 62, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Hammam, H.M.; Allam, F.A.; Moftah, F.M.; Abdel-Aty, M.A.; Hany, A.H.; Abd-El-Motagaly, K.F.; Nafeh, M.A.; Khalifa, R.; Mikhail, N.N.; Talaat, M.; et al. The epidemiology of schistosomiasis in Egypt: Assiut governorate. Am. J. Trop. Med. Hyg. 2000, 62, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Hammam, H.M.; Zarzour, A.H.; Moftah, F.M.; Abdel-Aty, M.A.; Hany, A.H.; El-Kady, A.Y.; Nasr, A.M.; Abd-El-Samie, A.; Qayed, M.H.; Mikhail, N.N.; et al. The epidemiology of schistosomiasis in Egypt: Qena governorate. Am. J. Trop. Med. Hyg. 2000, 62, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Cook, J.A.; Baker, S.T.; Warren, K.S.; Jordan, P. A controlled study of morbidity of schistosomiasis mansoni in St. Lucian children, based on quantitative egg excretion. Am. J. Trop. Med. Hyg. 1974, 23, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Hiatt, R.A. Morbidity from Schistosoma mansoni infections: An epidemiologic study based on quantitative analysis of egg excretion in two highland Ethiopian villages. Am. J. Trop. Med. Hyg. 1976, 25, 808–817. [Google Scholar] [CrossRef] [PubMed]
- Hiatt, R.A.; Gebre-Medhin, M. Morbidity from Schistosoma mansoni infections: An epidemiologic study based on quantitative analysis of egg excretion in Ethiopian children. Am. J. Trop. Med. Hyg. 1977, 26, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Arap Siongok, T.K.; Mahmoud, A.A.; Ouma, J.H.; Warren, K.S.; Muller, A.S.; Handa, A.K.; Houser, H.B. Morbidity in schistosomiasis mansoni in relation to intensity of infection: Study of a community in Machakos, Kenya. Am. J. Trop. Med. Hyg. 1976, 25, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Cline, B.L.; Rymzo, W.T.; Hiatt, R.A.; Knight, W.B.; Berrios-Duran, L.A. Morbidity from Schistosoma mansoni in a Puerto Rican community: A population-based study. Am. J. Trop. Med. Hyg. 1977, 26, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Sukwa, T.Y.; Bulsara, M.K.; Wurapa, F.K. The relationship between morbidity and intensity of Schistosoma mansoni infection in a rural Zambian community. Int. J. Epidemiol. 1986, 15, 248–251. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, M.D.; de Barros, H.L.; Katz, N. A clinical epidemiologic study in a schistosomiasis mansoni endemic area (Tuparecê, Minas Gerais). Rev. Inst. Med. Trop. Sao Paulo 1985, 27, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Proietti, F.A.; Antunes, C.M. Sensitivity, specificity and positive predictive value of selected clinical signs and symptoms associated with schistosomiasis mansoni. Int. J. Epidemiol. 1989, 18, 680–683. [Google Scholar] [CrossRef] [PubMed]
- De Lima e Costa, M.F.; Rocha, R.S.; Colley, D.; Gazzinelli, G.; Katz, N. Validity of selected clinical signs and symptoms in diagnosis of Schistosoma mansoni infection. Rev. Inst. Med. Trop. Sao Paulo 1991, 33, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Utzinger, J.; N’Goran, E.K.; Esse Aya, C.M.; Acka Adjoua, C.; Lohourignon, K.L.; Tanner, M.; Lengeler, C. Schistosoma mansoni, intestinal parasites and perceived morbidity indicators in schoolchildren in a rural endemic area of western Côte d’ivoire. Trop. Med. Int. Health 1998, 3, 711–720. [Google Scholar] [CrossRef] [PubMed]
- Utzinger, J.; N’Goran, E.K.; Tanner, M.; Lengeler, C. Simple anamnestic questions and recalled water-contact patterns for self-diagnosis of Schistosoma mansoni infection among schoolchildren in western Côte d’Ivoire. Am. J. Trop. Med. Hyg. 2000, 62, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Handzel, T.; Karanja, D.M.; Addiss, D.G.; Hightower, A.W.; Rosen, D.H.; Colley, D.G.; Andove, J.; Slutsker, L.; Secor, W.E. Geographic distribution of schistosomiasis and soil-transmitted helminths in western Kenya: Implications for anthelminthic mass treatment. Am. J. Trop. Med. Hyg. 2003, 69, 318–323. [Google Scholar] [PubMed]
- Cançado, C.B.; Firmo, J.O.; Fernandes, S.C.; Rocha, R.S.; Lima e Costa, M.F. Effect of skin colour and selected physical characteristics on Schistosoma mansoni dependent morbidity. Rev. Inst. Med. Trop. Sao Paulo 1995, 37, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Gryseels, B. The morbidity of schistosomiasis mansoni in the Rusizi Plain (Burundi). Trans. R. Soc. Trop. Med. Hyg. 1988, 82, 582–587. [Google Scholar] [CrossRef]
- Omer, A.H.; Hamilton, P.J.; Marshall, T.F.; Draper, C.C. Infection with Schistosoma mansoni in the Gezire area of the Sudan. J. Trop. Med. Hyg. 1976, 79, 151–157. [Google Scholar] [PubMed]
- Barreto, M.L. Geographical and socioeconomic factors relating to the distribution of Schistosoma mansoni infection in an urban area of north-east Brazil. Bull. World Health Organ. 1991, 69, 93–102. [Google Scholar] [PubMed]
- Abdel-Wahab, M.F.; Esmat, G.; Medhat, E.; Narooz, S.; Ramzy, I.; El-Boraey, Y.; Strickland, G.T. The epidemiology of schistosomiasis in Egypt: Menofia Governorate. Am. J. Trop. Med. Hyg. 2000, 62, 28–34. [Google Scholar] [CrossRef] [PubMed]
- El-Hawey, A.M.; Amr, M.M.; Abdel-Rahman, A.H.; El-Ibiary, S.A.; Agina, A.M.; Abdel-Hafez, M.A.; Waheeb, A.A.; Hussein, M.H.; Strickland, G.T. The epidemiology of schistosomiasis in Egypt: Gharbia Governorate. Am. J. Trop. Med. Hyg. 2000, 62, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Barakat, R.; Farghaly, A.; El Masry, A.G.; El-Sayed, M.K.; Hussein, M.H. The epidemiology of schistosomiasis in Egypt: Patterns of Schistosoma mansoni infection and morbidity in Kafer El-Sheikh. Am. J. Trop. Med. Hyg. 2000, 62, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Habib, M.; Abdel Aziz, F.; Gamil, F.; Cline, B.L. The epidemiology of schistosomiasis in Egypt: Qalyubia Governorate. Am. J. Trop. Med. Hyg. 2000, 62, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Nooman, Z.M.; Hasan, A.H.; Waheeb, Y.; Mishriky, A.M.; Ragheb, M.; Abu-Saif, A.N.; Abaza, S.M.; Serwah, A.A.; El-Gohary, A.; Saad, A.; et al. The epidemiology of schistosomiasis in Egypt: Ismailia governorate. Am. J. Trop. Med. Hyg. 2000, 62, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Sukwa, T.Y.; Bulsara, M.K.; Wurapa, F.K. Evaluation of selected symptoms in the diagnosis of Schistosoma mansoni infection. Trop. Geographical Med. 1985, 37, 295–297. [Google Scholar]
- Krauth, S.J.; Musard, C.; Traoré, S.I.; Zinsstag, J.; Achi, L.Y.; N’Goran, E.K.; Utzinger, J. Access to, and use of, water by populations living in a schistosomiasis and fascioliasis co-endemic area of northern Côte d’Ivoire. Acta Trop. 2015, 149, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Kittur, N.; Castleman, J.D.; Campbell, C.H., Jr.; King, C.H.; Colley, D.G. Comparison of Schistosoma mansoni prevalence and intensity of infection, as determined by the circulating cathodic antigen urine assay or by the Kato-Katz fecal assay: A systematic review. Am. J. Trop. Med. Hyg. 2016, 94, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Enk, M.J.; Lima, A.C.L.; Barros, H.D.S.; Massara, C.L.; Coelho, P.M.Z.; Schall, V.T. Factors related to transmission of and infection with Schistosoma mansoni in a village in the south-eastern region of Brazil. Mem. Inst. Oswaldo Cruz 2010, 105, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Massara, C.L.; Peixoto, S.V.; Da Silva Barros, H.; Enk, M.J.; Dos Santos Carvalho, O.; Schall, V. Factors associated with schistosomiasis mansoni in a population from the municipality of Jaboticatubas, State of Minas Gerais, Brazil. Mem. Inst. Oswaldo Cruz 2004, 99, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Amuta, E.U.; Houmsou, R.S. Prevalence, intensity of infection and risk factors of urinary schistosomiasis in pre-school and school aged children in Guma Local Government Area, Nigeria. Asian Pac. J. Trop. Med. 2014, 7, 34–39. [Google Scholar] [CrossRef]
- Rudge, J.W.; Stothard, J.R.; Basáñez, M.G.; Mgeni, A.F.; Khamis, I.S.; Khamis, A.N.; Rollinson, D. Micro-epidemiology of urinary schistosomiasis in Zanzibar: Local risk factors associated with distribution of infections among schoolchildren and relevance for control. Acta Trop. 2008, 105, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Geleta, S.; Alemu, A.; Getie, S.; Mekonnen, Z.; Erko, B. Prevalence of urinary schistosomiasis and associated risk factors among Abobo Primary School children in Gambella Regional State, southwestern Ethiopia: A cross-sectional study. Parasites Vectors 2015, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Useh, M.F.; Ejezie, G.C. Modification of behaviour and attitude in the control of schistosomiasis. 1. Observations on water-contact patterns and perception of infection. Ann. Trop. Med. Parasitol. 1999, 93, 711–720. [Google Scholar] [CrossRef] [PubMed]
- Clements, A.C.A.; Barnett, A.G.; Nyandindi, U.; Lwambo, N.J.S.; Kihamia, C.M.; Blair, L. Age and gender effects in self-reported urinary schistosomiasis in Tanzania. Trop. Med. Int. Health 2008, 13, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Michelson, E.H. Adam’s rib awry? Women and schistosomiasis. Soc. Sci. Med. 1993, 37, 493–501. [Google Scholar] [CrossRef]
- Webster, M.; Libranda-Ramirez, B.D.; Aligui, G.D.; Olveda, R.M.; Ouma, J.H.; Kariuki, H.C.; Kimani, G.; Olds, G.R.; Fulford, A.J.; Butterworth, A.E.; et al. The influence of sex and age on antibody isotype responses to Schistosoma mansoni and Schistosoma japonicum in human populations in Kenya and the Philippines. Parasitology 1997, 114, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Remoue, F.; To Van, D.; Schacht, A.-M.; Picquet, M.; Garraud, O.; Vercruysse, J.; Ly, A.; Capron, A.; Riveau, G. Gender-dependent specific immune response during chronic human schistosomiasis haematobia. Clin. Exp. Immunol. 2001, 124, 62–68. [Google Scholar] [CrossRef] [PubMed]
- De Moira, A.P.; Fulford, A.J.C.; Kabatereine, N.B.; Ouma, J.H.; Booth, M.; Dunne, D.W. Analysis of complex patterns of human exposure and immunity to schistosomiasis mansoni: The influence of age, sex, ethnicity and IgE. PLoS Negl. Trop. Dis. 2010, 4, e820. [Google Scholar] [CrossRef] [Green Version]
- Krentel, A.; Fischer, P.U.; Weil, G.J. A review of factors that influence individual compliance with mass drug administration for elimination of lymphatic filariasis. PLoS Negl. Trop. Dis. 2013, 7. [Google Scholar] [CrossRef] [PubMed]
- Ximenes, R.; Southgate, B.; Smith, P.G.; Guimarães Neto, L. Socioeconomic determinants of schistosomiasis in an urban area in the northeast of Brazil. Rev. Panam. Salud Pública 2003, 14, 409–421. [Google Scholar] [CrossRef] [PubMed]
- Muhumuza, S.; Kitimbo, G.; Oryema-Lalobo, M.; Nuwaha, F. Association between socio economic status and schistosomiasis infection in Jinja District, Uganda. Trop. Med. Int. Health 2009, 14, 612–619. [Google Scholar] [CrossRef] [PubMed]
- King, C.H. Parasites and poverty: The case of schistosomiasis. Acta Trop. 2010, 113, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Chami, G.F.; Kontoleon, A.A.; Bulte, E.; Fenwick, A.; Kabatereine, N.B.; Tukahebwa, E.M.; Dunne, D.W. Profiling nonrecipients of mass drug administration for schistosomiasis and hookworm infections: A comprehensive analysis of praziquantel and albendazole coverage in community-directed treatment in Uganda. Clin. Infect. Dis. 2016, 62, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Walz, Y.; Wegmann, M.; Dech, S.; Raso, G.; Utzinger, J. Risk profiling of schistosomiasis using remote sensing: Approaches, challenges and outlook. Parasites Vectors 2015, 8, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clennon, J.A.; Mungai, P.L.; Muchiri, E.M.; King, C.H.; Kitron, U. Spatial and temporal variations in local transmission of Schistosoma haematobium in Msambweni, Kenya. Am. J. Trop. Med. Hyg. 2006, 75, 1034–1041. [Google Scholar] [PubMed]
- Gryseels, B.; Polman, K.; Clerinx, J.; Kestens, L. Human schistosomiasis. Lancet 2006, 368, 1106–1118. [Google Scholar] [CrossRef]
- Stratton, L.; O’Neill, M.S.; Kruk, M.E.; Bell, M.L. The persistent problem of malaria: Addressing the fundamental causes of a global killer. Soc. Sci. Med. 2008, 67, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Alsan, M.M.; Westerhaus, M.; Herce, M.; Nakashima, K.; Farmer, P.E. Poverty, global health, and infectious disease: Lessons from Haiti and Rwanda. Infect. Dis. Clin. N. Am. 2011, 25, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Bates, I.; Fenton, C.; Gruber, J.; Lalloo, D.; Lara, A.M.; Squire, S.B.; Theobald, S.; Thomson, R.; Tolhurst, R. Vulnerability to malaria, tuberculosis, and HIV/AIDS infection and disease. Part 1: Determinants operating at individual and household level. Lancet Infect. Dis. 2004, 4, 267–277. [Google Scholar] [CrossRef]
- Allotey, P.; Gyapong, M. The Gender Agenda in the Control of Tropical Diseases: A Review of Current Evidence; WHO: Geneva, Switzerland, 2005. [Google Scholar]
- Wilcox, B.A.; Colwell, R.R. Emerging and reemerging infectious diseases: Biocomplexity as an interdisciplinary paradigm. EcoHealth 2005, 2, 244–257. [Google Scholar] [CrossRef]
- Waltner-Toews, D. An ecosystem approach to health and its applications to tropical and emerging diseases. Cad. Saude Publica 2001, 17, 7–36. [Google Scholar] [CrossRef] [PubMed]
- Madon, S. Challenges of accountability in resource-poor contexts: Lessons about invited spaces from Karnataka’s Village Health Committees. Oxf. Dev. Stud. 2016. [Google Scholar] [CrossRef]
- Cornwall, A. Introduction: New democratic spaces? The politics and dynamics of institutionalised participation. IDS Bull. 2004, 35, 1–10. [Google Scholar] [CrossRef] [Green Version]
- WHO; UNICEF. Progress on Drinking Water, Sanitation and Hygiene: 2017 Update and SDG Baselines; WHO and UNICEF: Geneva, Switzerland, 2017. [Google Scholar]
- Worku, L.; Damte, D.; Endris, M.; Tesfa, H.; Aemero, M. Schistosoma mansoni infection and associated determinant factors among school children in Sanja Town, Northwest Ethiopia. J. Parasitol. Res. 2014, 2014, 792536. [Google Scholar] [CrossRef] [PubMed]
- Kloos, H.; Rodrigues, J.C.A.P.; Pereira, W.R.; Velásquez-Meléndez, G.; LoVerde, P.; Oliveira, R.C.; Gazzinelli, A. Combined methods for the study of water contact behavior in a rural schistosomiasis-endemic area in Brazil. Acta Trop. 2006, 97, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Nalugwa, A.; Olsen, A.; Tukahebwa, M.E.; Nuwaha, F. Intestinal schistosomiasis among preschool children along the shores of Lake Victoria in Uganda. Acta Trop. 2015, 142, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Kvalsvig, J.D.; Schutte, C.H. The role of human water contact patterns in the transmission of schistosomiasis in an informal settlement near a major industrial area. Ann. Trop. Med. Parasitol. 1986, 80, 13–26. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| S. haematobium Diagnostic Question(s) | Sensitivity 1 | Specificity 1 | LR+ 2 | Number (+) from Questionnaire Data |
|---|---|---|---|---|
| Blood in urine | 0.508 | 0.868 | 3.85 3 | 28 |
| Pain during urination | 0.445 | 0.818 | 2.45 | 142 |
| History of schistosomiasis infection | 0.365 | 0.807 | 1.89 | 156 |
| Blood in urine Pain during urination | 0.226 | 0.976 | 9.41 3 | 13 |
| Blood in urine History of schistosomiasis infection | 0.185 | 0.975 | 7.28 3 | 8 |
| Pain during urination History of schistosomiasis infection | 0.162 | 0.965 | 4.62 3 | 83 |
| Blood in urine Pain during urination History of schistosomiasis infection | 0.083 | 0.995 | 17.80 3 | 19 |
| S. mansoni Diagnostic Question(s) | Sensitivity 1 | Specificity 1 | LR+ 2 | Number (+) from Questionnaire Data |
|---|---|---|---|---|
| Blood in stool | 0.249 | 0.904 | 2.69 | 19 |
| Bloody diarrhea | 0.283 | 0.849 | 1.87 | 14 |
| Abdominal pain | 0.399 | 0.666 | 1.19 | 332 |
| History of schistosomiasis | 0.329 | 0.765 | 1.40 | 157 |
| Blood in stool Bloody diarrhea | 0.070 | 0.986 | 4.86 3 | 5 |
| Blood in stool Abdominal pain | 0.099 | 0.968 | 3.10 | 19 |
| Blood in stool History of schistosomiasis | 0.082 | 0.977 | 3.63 3 | 11 |
| Bloody diarrhea Abdominal pain | 0.113 | 0.950 | 2.24 | 20 |
| Bloody diarrhea History of schistosomiasis | 0.093 | 0.965 | 2.62 | 3 |
| Abdominal pain History of schistosomiasis | 0.131 | 0.922 | 1.67 | 70 |
| Blood in stool Bloody diarrhea History of schistosomiasis | 0.023 | 0.997 | 6.81 3 | 0 |
| Blood in stool Bloody diarrhea Abdominal pain | 0.028 | 0.995 | 5.81 3 | 6 |
| Blood in stool History of schistosomiasis Abdominal pain | 0.033 | 0.992 | 4.34 3 | 10 |
| Bloody diarrhea History of schistosomiasis Abdominal pain | 0.037 | 0.988 | 3.13 | 10 |
| Blood in stool Bloody diarrhea History of schistosomiasis Abdominal pain | 0.009 | 0.999 | 8.13 3 | 5 |
| Eigenvalue | Percentage of Variance | Cumulative Percentage of Variance | |
|---|---|---|---|
| Component 1 | 1.872 | 20.8 | 20.8 |
| Component 2 | 1.574 | 17.5 | 38.3 |
| Component 3 | 1.185 | 13.2 | 51.5 |
| Component 4 | 0.917 | 10.2 | 61.7 |
| Component 5 | 0.875 | 9.7 | 71.4 |
| Component 6 | 0.835 | 9.3 | 80.7 |
| Component 7 | 0.625 | 6.9 | 87.6 |
| Component 8 | 0.570 | 6.3 | 93.9 |
| Component 9 | 0.547 | 6.1 | 100.0 |
| Asset | Mean | Std Dev | Factor Score |
|---|---|---|---|
| House | 0.95 | 0.22 | 0.37 |
| Latrine | 0.96 | 0.19 | 0.36 |
| Land | 0.89 | 0.32 | 0.25 |
| Radio | 0.74 | 0.44 | 0.23 |
| TV | 0.16 | 0.37 | 0.02 |
| Motorcycle | 0.26 | 0.44 | 0.12 |
| Bicycle | 0.73 | 0.44 | 0.25 |
| Phone | 0.83 | 0.38 | 0.27 |
| Fridge | 0.10 | 0.30 | 0.02 |
| Characteristic | n (%) |
|---|---|
| Sex | |
| Male | 685 (40.2) |
| Female | 1019 (59.8) |
| Age | |
| <13 years old | 779 (45.7) |
| ≥13 years old | 925 (54.3) |
| District | |
| Rufiji | 894 (52.5) |
| Mkuranga | 810 (47.5) |
| Village | |
| Bungu | 268 (15.7) |
| izapala | 160 (9.4) |
| MgombaKaskazini | 241 (14.1) |
| Mgomba Kati | 248 (14.6) |
| Misasa | 197 (11.6) |
| Mkamba | 249 (14.6) |
| Njopeka | 204 (12.0) |
| Pagae | 137 (8.0) |
| Education of Parent | |
| No formal education | 350 (20.5) |
| Incomplete primary education | 947 (55.6) |
| Primary education | 280 (16.4) |
| Incomplete secondary school | 93 (5.5) |
| Secondary education | 34 (2.0) |
| Occupation of Parent | |
| Agriculture or livestock keeping | 1260 (73.9) |
| All other | 444 (26.1) |
| Wealth Index | |
| Cluster 1 (poorest) | 38 (2.2) |
| Cluster 2 | 73 (4.3) |
| Cluster 3 | 302 (17.7) |
| Cluster 4 | 487 (28.6) |
| Cluster 5 (least poor) | 804 (47.2) |
| Schistosomiasis Infection Status | |
| S. haematobium | 151 (8.9) |
| S. mansoni | 37 (2.2) |
| S. haematobium or S. mansoni | 168 (9.9) |
| Variable | COR 1 | 95% CI 2 | p-Value |
|---|---|---|---|
| Sex | |||
| Male | 2.49 | 1.79–3.47 | <0.001 * |
| Female | Ref | -- | -- |
| Age | |||
| <13 years old | 1.17 | 0.84–1.63 | 0.348 |
| ≥13 years old | Ref | -- | -- |
| Education of Parent | |||
| No formal education | 0.57 | 0.22–1.43 | 0.228 |
| Incomplete primary | 0.40 | 0.17–0.98 | 0.044 * |
| Primary education | 0.52 | 0.21–1.30 | 0.161 |
| Incomplete secondary | 0.95 | 0.34–2.61 | 0.916 |
| Secondary education | Ref | -- | -- |
| Occupation of Parent | |||
| Agriculture or livestock keeping | 1.01 | 0.68–1.45 | 0.964 |
| All other | Ref | -- | -- |
| Wealth Index | |||
| Cluster 1 (poorest) | Ref | -- | -- |
| Cluster 2 | 0.59 | 0.20–1.72 | 0.336 |
| Cluster 3 | 0.68 | 0.28–1.62 | 0.382 |
| Cluster 4 | 0.50 | 0.21–1.17 | 0.109 |
| Cluster 5 (least poor) | 0.47 | 0.20–1.09 | 0.077 |
| Latrine Use | |||
| Yes (home or neighbors) | Ref | -- | -- |
| No | 2.55 | 1.05–6.23 | 0.039 * |
| Main Source of Drinking Water | |||
| Safe (wells and rainwater) | Ref | -- | -- |
| Unsafe (river, dam, etc.) | 3.05 | 1.79–5.19 | <0.001* |
| Frequency of River Contact | |||
| 1+/day | 0.45 | 0.25–0.81 | 0.007* |
| 1–4 times/week | 0.65 | 0.36–1.17 | 0.149 |
| Never | Ref | -- | -- |
| Frequency of Lake Contact | |||
| 1+/day | 0.56 | 0.27–1.19 | 0.132 |
| 1–4 times/week | 1.01 | 0.53–1.91 | 0.982 |
| Never | Ref | -- | -- |
| Frequency of Dam Contact | |||
| 1+/day | 0.79 | 0.41–1.53 | 0.492 |
| 1–4 times/week | 1.01 | 0.54–1.88 | 0.973 |
| Never | Ref | -- | -- |
| Frequency of Spring Contact | |||
| 1+/day | 0.52 | 0.25–1.06 | 0.073 |
| 1–times/week | 0.75 | 0.39–1.41 | 0.367 |
| Never | Ref | -- | -- |
| Variable | Penalized 1 | Reduced 2 | ||||
|---|---|---|---|---|---|---|
| AOR 3 | 95% CI 4 | AOR 3 | 95% CI 4 | |||
| Sex | ||||||
| Male | 2.68 | 1.89–3.80 | <0.001 * | 2.69 | 1.90–3.80 | <0.001 * |
| Female | Ref | -- | -- | Ref | -- | -- |
| Age | 1 | -- | -- | -- | -- | -- |
| Occupation of Parent | 1 | -- | -- | -- | -- | -- |
| Latrine Use | ||||||
| Yes (home or neighbors) | Ref | -- | -- | Ref | -- | -- |
| No | 2.32 | 0.90–5.98 | 0.083 | 2.33 | 0.90–6.01 | 0.080 |
| Main Source of Drinking Water | ||||||
| Safe (wells and rainwater) | Ref | -- | -- | Ref | -- | -- |
| Unsafe (river, dam, etc.) | 3.55 | 2.02–6.26 | <0.001 * | 3.57 | 2.03–6.27 | <0.001 * |
| Wealth Index | ||||||
| Cluster 1 (poorest) | Ref | -- | -- | Ref | -- | -- |
| Cluster 2 | 0.55 | 0.26–1.17 | 0.118 | 0.54 | 0.18–1.63 | 0.275 |
| Cluster 3 | 0.64 | 0.42–0.98 | 0.040 * | 0.64 | 0.26–1.56 | 0.326 |
| Cluster 4 | 0.43 | 0.27–0.68 | <0.001 * | 0.43 | 0.18–1.04 | 0.060 |
| Cluster 5 (least poor) | 0.38 | 0.04–3.46 | 0.391 | 0.38 | 0.16–0.90 | 0.028 * |
| Frequency of Lake Contact | ||||||
| 1+/day | 1.65 | 0.37–7.38 | 0.513 | 1.66 | 0.59–4.67 | 0.341 |
| 1–4 times/week | 3.25 | 1.80–5.89 | <0.001 * | 3.25 | 1.25–8.47 | 0.016 * |
| Never | Ref | -- | -- | Ref | -- | -- |
| Frequency of River Contact | ||||||
| 1+/day | 0.26 | 0.08–0.85 | 0.025 * | 0.26 | 0.12–0.56 | <0.001 * |
| 1–4 times/week | 0.27 | 0.15–0.48 | <0.001 * | 0.26 | 0.12–0.60 | 0.001 * |
| Never | Ref | -- | -- | Ref | -- | -- |
| Frequency of Spring Contact | 1 | -- | -- | -- | -- | -- |
| Frequency of Dam Contact | 1 | -- | -- | -- | -- | -- |
| Education of Parent | ||||||
| No formal education | 0.65 | 0.34–1.22 | 0.176 | 0.64 | 0.24–1.71 | 0.375 |
| Incomplete primary | 0.46 | 0.32–0.64 | <0.001 * | 0.45 | 0.18–1.16 | 0.100 |
| Primary education | 0.56 | 0.08–4.09 | 0.564 | 0.55 | 0.21–1.47 | 0.236 |
| Incomplete secondary | 0.99 | 0.51–1.89 | 0.967 | 0.98 | 0.33–2.89 | 0.976 |
| Secondary education | Ref | -- | -- | Ref | -- | -- |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donohue, R.E.; Mashoto, K.O.; Mubyazi, G.M.; Madon, S.; Malecela, M.N.; Michael, E. Biosocial Determinants of Persistent Schistosomiasis among Schoolchildren in Tanzania despite Repeated Treatment. Trop. Med. Infect. Dis. 2017, 2, 61. https://doi.org/10.3390/tropicalmed2040061
Donohue RE, Mashoto KO, Mubyazi GM, Madon S, Malecela MN, Michael E. Biosocial Determinants of Persistent Schistosomiasis among Schoolchildren in Tanzania despite Repeated Treatment. Tropical Medicine and Infectious Disease. 2017; 2(4):61. https://doi.org/10.3390/tropicalmed2040061
Chicago/Turabian StyleDonohue, Rose E., Kijakazi O. Mashoto, Godfrey M. Mubyazi, Shirin Madon, Mwele N. Malecela, and Edwin Michael. 2017. "Biosocial Determinants of Persistent Schistosomiasis among Schoolchildren in Tanzania despite Repeated Treatment" Tropical Medicine and Infectious Disease 2, no. 4: 61. https://doi.org/10.3390/tropicalmed2040061