School-Based Intervention on Cardiorespiratory Fitness in Brazilian Students: A Nonrandomized Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
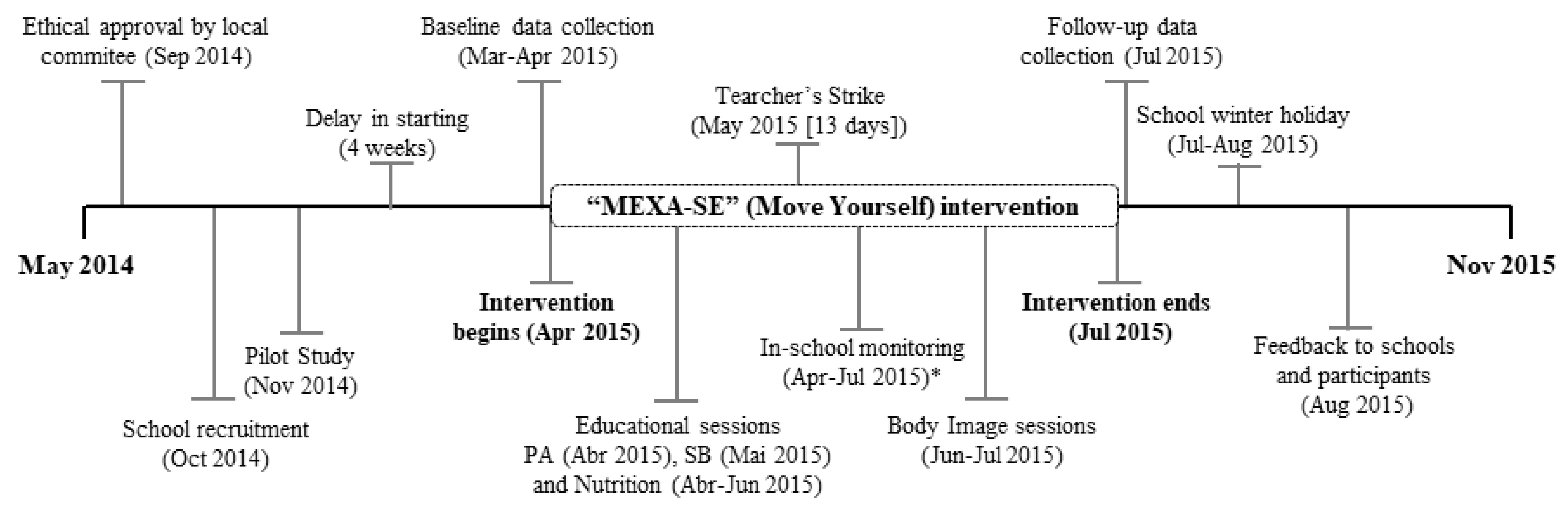
2.2. Intervention
2.2.1. Theoretical Aspects
2.2.2. Intervention Strategies
First Component: PE Classes
Second Component: Active Recess
Third Component: Educational Sessions
Fourth Component: Education Materials
Control Group
2.3. Variable Measures
2.4. Data Collection
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
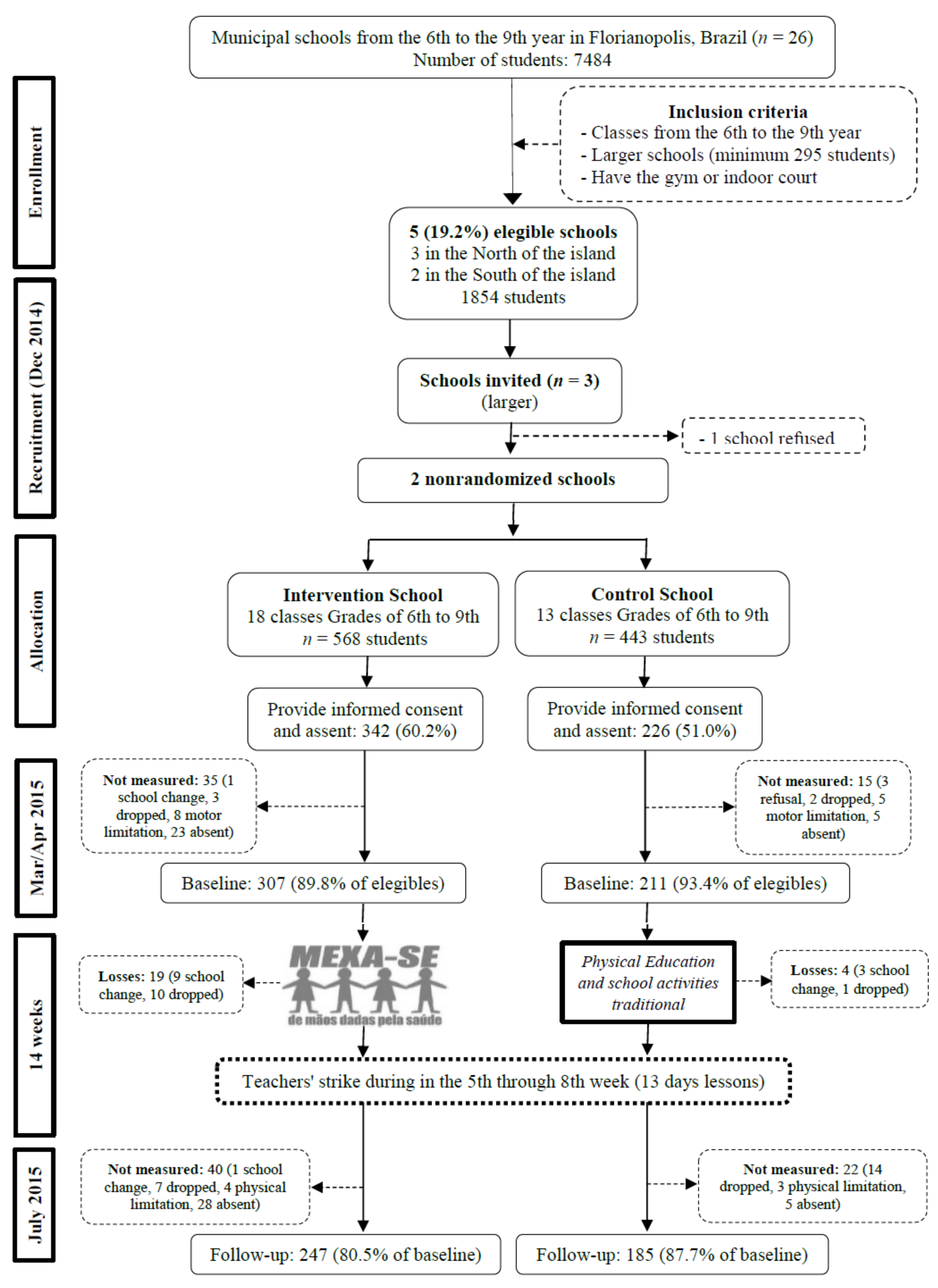
3.1. Participants
Deviations
3.2. Comparison of Baseline Characteristics
3.3. Efect of Intervention
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ruiz, J.R.; Castro-Pinero, J.; Espana-Romero, V.; Artero, E.G.; Ortega, F.B.; Cuenca, M.M.; Jimenez-Pavon, D.; Chillon, P.; Girela-Rejon, M.J.; Mora, J.; et al. Field-based fitness assessment in young people: The ALPHA health-related fitness test battery for children and adolescents. Br. J. Sports Med. 2011, 45, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Moreira, C.; Santos, R.; de Farias, J.; Vale, S.; Santos, P.; Soares-Miranda, L.; Marques, A.; Mota, J. Metabolic risk factors, physical activity and physical fitness in azorean adolescents: A cross-sectional study. BMC Public Health 2011, 11, 214. [Google Scholar] [CrossRef] [PubMed]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.-C.; Artero, E.G.; Sui, X.; Blair, S.N. Mortality trends in the general population: The importance of cardiorespiratory fitness. J. Psychopharmacol. 2010, 24, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Dobbins, M.; Husson, H.; DeCorby, K.; LaRocca, R.L. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst. Rev. 2013, 2, CD007651. [Google Scholar] [CrossRef]
- Minatto, G.; Barbosa Filho, V.C.; Berria, J.; Petroski, E.L. School-Based Interventions to Improve Cardiorespiratory Fitness in Adolescents: Systematic Review with Meta-analysis. Sports Med. 2016, 46, 1273–1292. [Google Scholar] [CrossRef] [PubMed]
- Burns, R.D.; Brusseau, T.A.; Fu, Y. Moderators of School-Based Physical Activity Interventions on Cardiorespiratory Endurance in Primary School-Aged Children: A Meta-Regression. Int. J. Environ. Res. Public Health 2018, 15, 1764. [Google Scholar] [CrossRef]
- Costigan, S.A.; Eather, N.; Plotnikoff, R.C.; Taaffe, D.R.; Lubans, D.R. High-intensity interval training for improving health-related fitness in adolescents: A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 1253–1261. [Google Scholar] [CrossRef]
- Brasil. Instituto Brasileiro de Geografia e Estatística (IBGE). Informação Demográfica e Socioeconômica Número 28. Indicadores Sociais Municipais. Uma Análise dos Resultados do Censo Demográfico 2010. Rio de Janeiro: IBGE. 2010. Available online: http://ibge.gov.br/home/estatistica/populacao/condicaodevida/pof/2008_2009 (accessed on 21 January 2016).
- Brasil. Presidente da República. Decreto Nº 6.286, de 5 de dezembro de 2007. Institui o Programa Saúde na Escola (PSE), e dá Outras Providências. Diário Oficial da União, P.E., Brasília, DF, 5 dez., Ed. Available online: http://www.planalto.gov.br/ccivil_03/_ato2007-2010/2007/decreto/d6286.htm (accessed on 29 June 2014).
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef]
- Bronfenbrenner, B. Ecological Models of Human Development; Elsevier: Oxford, UK, 1994. [Google Scholar]
- Seefeldt, V.; Malina, R.M.; Clark, M.A. Factors affecting levels of physical activity in adults. Sports Med. 2002, 32, 143–168. [Google Scholar] [CrossRef]
- Stotz, E.N. Enfoques sobre educação e saúde. In Participação Popular, Educação e Saúde: Teoria e Prática; Valla, V.V., Stotz, E.N., Eds.; Relume-Dumará: Rio de Janeiro, Brazil, 2003; pp. 11–22. [Google Scholar]
- United States Department of Health and Human Services (USDHHS). Physical Activity Evaluation Handbook; Departament of Health and Human Services, Ed.; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2002.
- Prefeitura Municipal de Florianopolis. Secretaria Minicipal de Educação. Departamento de Educação Fundamental. Proposta Curricular. Florianópolis, 2008. Available online: http://www.pmf.sc.gov.br/arquivos/arquivos/pdf/09_04_2018_14.01.14.62a2765c21e81be772971fd729542791.pdf (accessed on 12 June 2014).
- Brasil; Secretaria de Educação Fundamental. Parâmetros Curriculares Nacionais: Educação Física; MEC/SEF: Brasília, Brazil, 1998; p. 114. Available online: http://portal.mec.gov.br/seb/arquivos/pdf/livro07.pdf (accessed on 10 September 2013).
- Leger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Duarte, M.F.S.; Duarte, C.R. Validade do teste aeróbico de corrida de vai-e-vem de 20 metros. Rev. Bras. Cienc. Mov. 2001, 9, 7–14. [Google Scholar]
- Stewart-Brown, S. What Is the Evidence on School Health Promotion in Improving Health or Preventing Disease and, Specifically, What Is the Effectiveness of the Health Promoting Schools Approach? WHO Regional Office for Europe: Copenhagen. Available online: http://www.euro.who.int/document/e88185.pdf (accessed on 5 July 2006).
- Gore, C.; Norton, K.; Olds, T.; Whittingham, N.; Birchall, K.; Clough, M.; Dickerson, B.; Downie, L. Certificação em antropometria: Um modelo Australiano. In Antropométrica; Norton, K., Olds, T., Eds.; Artmed: Porto Alegre, Brazil, 2005; pp. 375–388. [Google Scholar]
- Farias Júnior, J.C.; Lopes, A.S.; Mota, J.; Santos, M.P.; Ribeiro, J.C.; Hallal, P.C. Validade e reprodutibilidade de um questionário para medida de atividade física em adolescentes: Uma adaptação do Self-Administered Physical Activity Checklist. Rev. Bras. Epidemiol. 2012, 15, 198–210. [Google Scholar] [CrossRef]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef]
- Brasil. Associação Brasileira de Empresas de Pesquisa (ABEP). Critério de Classificação Econômica Brasil. 2012. Available online: http://www.abep.org/new/criterioBrasil.aspx (accessed on 5 March 2014).
- Tanner, N.G. Growth at Adolescence; Blackwell Scientificm Publications: Oxford, UK, 1962. [Google Scholar]
- Adami, F.; Vasconcelos, F.D.A.G.D. Obesidade e maturação sexual precoce em escolares de Florianópolis—SC. Rev. Bras. Epidemiol. 2008, 11, 549–560. [Google Scholar] [CrossRef]
- George, D.; Mallery, P. SPSS for Windows Step by Step: A Simple Guide and Reference. 11.0 Update. Available online: http://wps.ablongman.com/wps/media/objects/385/394732/george4answers.pdf (accessed on 8 January 2019).
- Lubans, D.R.; Morgan, P.J.; Callister, R. Potential moderators and mediators of intervention effects in an obesity prevention program for adolescent boys from disadvantaged schools. J. Sci. Med. Sport 2012, 15, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, L.B.; Toftager, M.; Boyle, E.; Kristensen, P.L.; Troelsen, J. Effect of a school environment intervention on adolescent adiposity and physical fitness. Scand. J. Med. Sci. Sports 2013, 23, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Farias, E.S.; Carvalho, W.R.G.; Gonçalves, E.M.; Guerra-Júnior, G. Efeito da atividade física programada sobre a aptidão física em escolares adolescentes. Revista Brasileira Cineantropometria Desempenho Humano 2010, 12, 98–105. [Google Scholar]
- Nahas, M.V.; de Barros, M.V.; de Assis, M.A.; Hallal, P.C.; Florindo, A.A.; Konrad, L. Methods and participant characteristics of a randomized intervention to promote physical activity and healthy eating among brazilian high school students: The Saude na Boa project. J. Phys. Act. Health 2009, 6, 153–162. [Google Scholar] [CrossRef]
- Jago, R.; McMurray, R.G.; Drews, K.L.; Moe, E.L.; Murray, T.; Pham, T.H.; Venditti, E.M.; Volpe, S.L. HEALTHY Intervention: Fitness, Physical Activity, and Metabolic Syndrome Results. Med. Sci. Sports Exerc. 2011, 43, 1513–1522. [Google Scholar] [CrossRef]
- Singh, A.S.; Chin A Paw, M.J.M.; Brug, J.; van Mechelen, W. Short-term effects of school-based weight gain prevention among adolescents. Arch. Pediatr. Adolesc. Med. 2007, 161, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Lonsdale, C.; Rosenkranz, R.R.; Peralta, L.R.; Bennie, A.; Fahey, P.; Lubans, D.R. A systematic review and meta-analysis of interventions designed to increase moderate-to-vigorous physical activity in school physical education lessons. Prev. Med. 2013, 56, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Comprehensive School Physical Activity Programs: A Guide for Schools; U.S. Department of Health and Human Services: Atlanta, GA, USA, 2013; pp. 1–65.
- American Colege of Sports Medicine (ACSM). Guidelines for Exercise Testing and Prescription, 9th ed.; Wolters Kluwer Health; Lippincott Willians & Wilkins: Philadelphia, PA, USA, 2014; p. 456. [Google Scholar]
- Kremer, M.M.; Reichert, F.F.; Hallal, P.C. Intensidade e duração dos esforços físicos em aulas de Educação Física. Rev. Saude Publica 2012, 46, 320–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malina, R.M.; Bouchard, C.; Bar-Or, O. Growth, Maturation and Physical Activity, 2nd ed.; Human Kinetics Books: Champaign, IL, USA, 2004. [Google Scholar]



{kind=link}
{kind=link}
| Actions | Influence Level | Theory | No. Sessions | Duration | WF | Executing Agent |
|---|---|---|---|---|---|---|
| Training for PE teachers | School | EPS | 1 | 4 h | - | Researchers (PE) |
| PE Classes: Stretching exercises (10 min), strength and muscular resistance (10 min), and increased intensity in the main part of the class (MVPA) | Individual | Meta-analysis | 42 * | 45 min | 3 | School PE teachers |
| Active recess | Individual, School | EPS; TSC; Meta-analysis | 70 * | 15 min | 5 | Researchers and School |
| Educational sessions on the following topics: Health, lifestyle, physical activity, and sedentary behaviour | Individual | EPS; TSC | 2 | 45 min | † | School PE teachers |
| Educational sessions on healthy eating and nutrition | Individual | MDES | 6 | 100 min | 1 | Researchers (Nutritionist) |
| Educational sessions related to body image | Individual | TSC; Belief in health | 4 | 45 min | 1 | Researchers (PE) |
| Placement of posters about physical activity and sedentary behaviour in school and health units | School | EPS; MSE | - | - | † | Researchers, students and teachers |
| Distribution of leaflets on physical activity and sedentary behaviour | Individual, Family | EPS; MSE | - | - | †† | School PE teachers Researchers |
| Variables | IG (n = 247) | CG (n = 185) | p-value | All (n = 432) | Dropout (n = 136) | p-value |
|---|---|---|---|---|---|---|
| Mean (sd) | Mean (sd) | Mean (sd) | Mean (sd) | |||
| Age (years) † | 12.4 (1.3) | 12.7 (1.3) | 0.052 | 12.6 (1.3) | 12.8 (1.4) | 0.084 |
| Body mass (kg) * | 47.7 (11.3) | 50.2 (12.4) | 0.047 | 48.8 (11.8) | 52.9 (13.4) | 0.002 |
| Height (cm) * | 155.5 (9.8) | 156.6 (9.9) | 0.237 | 156.0 (9.8) | 157.8 (9.8) | 0.082 |
| TR+SE (mm) * | 22.5 (11.5) | 24.4 (11.5) | 0.042 | 23.3 (11.6) | 26.9 (13.3) | 0.004 |
| MVPA school (min) | 10.8 (6.6) | 10.4 (6.6) | 0.499 | 10.8 (6.6) | 10.1 (5.6) | 0.833 |
| PA general (min) † | 688.6 (913.2) | 648.2 (831.3) | 0.935 | 671.0 (877.7) | 572.4 (902.6) | 0.029 |
| Attendance PE lessons (%) † | 83.8 (13.3) | 92.0 (8.3) | <0.001 | 87.3 (12.2) | 72.4 (23.4) | <0.001 |
| Minutes * | 3.4 (1.8) | 3.0 (1.7) | 0.009 | 3.2 (1.8) | 2.9 (1.5) | 0.093 |
| Laps * | 26.4 (16) | 22.8 (13.9) | 0.013 | 24.8 (15.2) | 21.9 (12.3) | 0.077 |
| Stages † | 3.8 (1.9) | 3.3 (1.7) | 0.007 | 3.6 (1.8) | 3.2 (1.5) | 0.134 |
| VO2max (mL/(kg·min) * | 41.7 (4.8) | 40.0 (4.6) | <0.001 | 41.0 (4.8) | 40.0 (4.5) | 0.075 |
| % (n) | % (n) | p-value ** | % (n) | % (n) | p-value ** | |
| Sex | 0.769 | 0.833 | ||||
| Male | 47.4 (117) | 45.9 (85) | 46.8 (202) | 47.8(65) | ||
| Female | 52.6 (130) | 54.1 (100) | 53.2 (230) | 52.2 (71)\ | ||
| Socioeconomic Status | 0.190 | 0.385 | ||||
| A + B | 54.0 (129) | 47.5 (86) | 51.2 (215) | 46.7 (57) | ||
| C + D + E | 46.0 (110) | 52.5 (95) | 48.8 (205) | 53.3 (65) | ||
| Sexual maturation†† | 0.705 | 0.067 | ||||
| Prepubescent (S1) | 1.7 (4) | 1.1 (2) | 1.4 (6) | 1.0 (1) | ||
| Pubescent (S2 to S4) | 86.8 (210) | 89.4 (160) | 87.9 (370) | 79.8 (79) | ||
| Postpubescent (S5) | 11.6 (28) | 9.5 (17) | 10.7 (45) | 19.2 (19) |
| Differences between Baseline and Follow-Up | Adjusted Differences between Intervention vs. Control Group | Interaction | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Indicator CRF | Intervention (n = 247) | p-value | Control (n = 185) | p-value | Adjusted Difference (n = 432) | p-value | Intention-To-Treat Analysis (n = 518) | p-value | ES | Group vs. Sex | Group vs. Age | Group vs. SM | Group vs. SES |
| Mean (CI 95%) | Mean (CI 95%) | Mean (CI 95%) | Mean (CI 95%) | p-value | p-value | p-value | p-value | ||||||
| Minutes | 0.05 (−0.10; 0.21) | 0.517 | −0.11 (−0.28; 0.06) | 0.206 | 0.17 (−0.07; 0.40) | 0.173 | 0.13 (−0.09; 0.34) | 0.257 | 0.13 | 0.351 | 0.194 | 0.558 | 0.949 |
| Laps | 0.67 (−0.58; 1.91) | 0.224 | −0.83 (−2.24; 0.57) | 0.291 | 1.50 (−0.46; 3.46) | 0.134 | 1.16 (−0.63; 2.95) | 0.202 | 0.16 | 0.477 | 0.179 | 0.759 | 0.963 |
| Stages | 0.07 (−0.09; 0.22) | 0.308 | −0.06 (−0.23; 0.11) | 0.497 | 0.13 (−0.12; 0.37) | 0.307 | 0.09 (−0.13; 0.31) | 0.430 | 0.11 | 0.122 | 0.293 | 0.894 | 0.724 |
| VO2max | −0.27 (−0.72; 0.18) | 0.240 | −0.75 (−1.24; −0.24) | 0.004 | 0.48 (−0.23; 1.19) | 0.186 | 0.40 (−0.26; 1.05) | 0.232 | 0.14 | 0.107 | 0.494 | 0.900 | 0.882 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minatto, G.; Petroski, E.L.; Silva, K.S.d.; Duncan, M.J. School-Based Intervention on Cardiorespiratory Fitness in Brazilian Students: A Nonrandomized Controlled Trial. J. Funct. Morphol. Kinesiol. 2019, 4, 10. https://doi.org/10.3390/jfmk4010010
Minatto G, Petroski EL, Silva KSd, Duncan MJ. School-Based Intervention on Cardiorespiratory Fitness in Brazilian Students: A Nonrandomized Controlled Trial. Journal of Functional Morphology and Kinesiology. 2019; 4(1):10. https://doi.org/10.3390/jfmk4010010
Chicago/Turabian StyleMinatto, Giseli, Edio Luiz Petroski, Kelly Samara da Silva, and Michael J. Duncan. 2019. "School-Based Intervention on Cardiorespiratory Fitness in Brazilian Students: A Nonrandomized Controlled Trial" Journal of Functional Morphology and Kinesiology 4, no. 1: 10. https://doi.org/10.3390/jfmk4010010