Changes in Endothelial Function after Acute Resistance Exercise Using Free Weights



Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Approach to the Problem
2.2. Subjects
2.3. Procedures
2.3.1. Anthropometric Measurement
2.3.2. Muscle Strength
2.3.3. Hemodynamics
2.3.4. Forearm Blood Flow
2.3.5. Acute Bout of Resistance Exercise
2.4. Data Analysis
3. Results
3.1. Hemodynamics
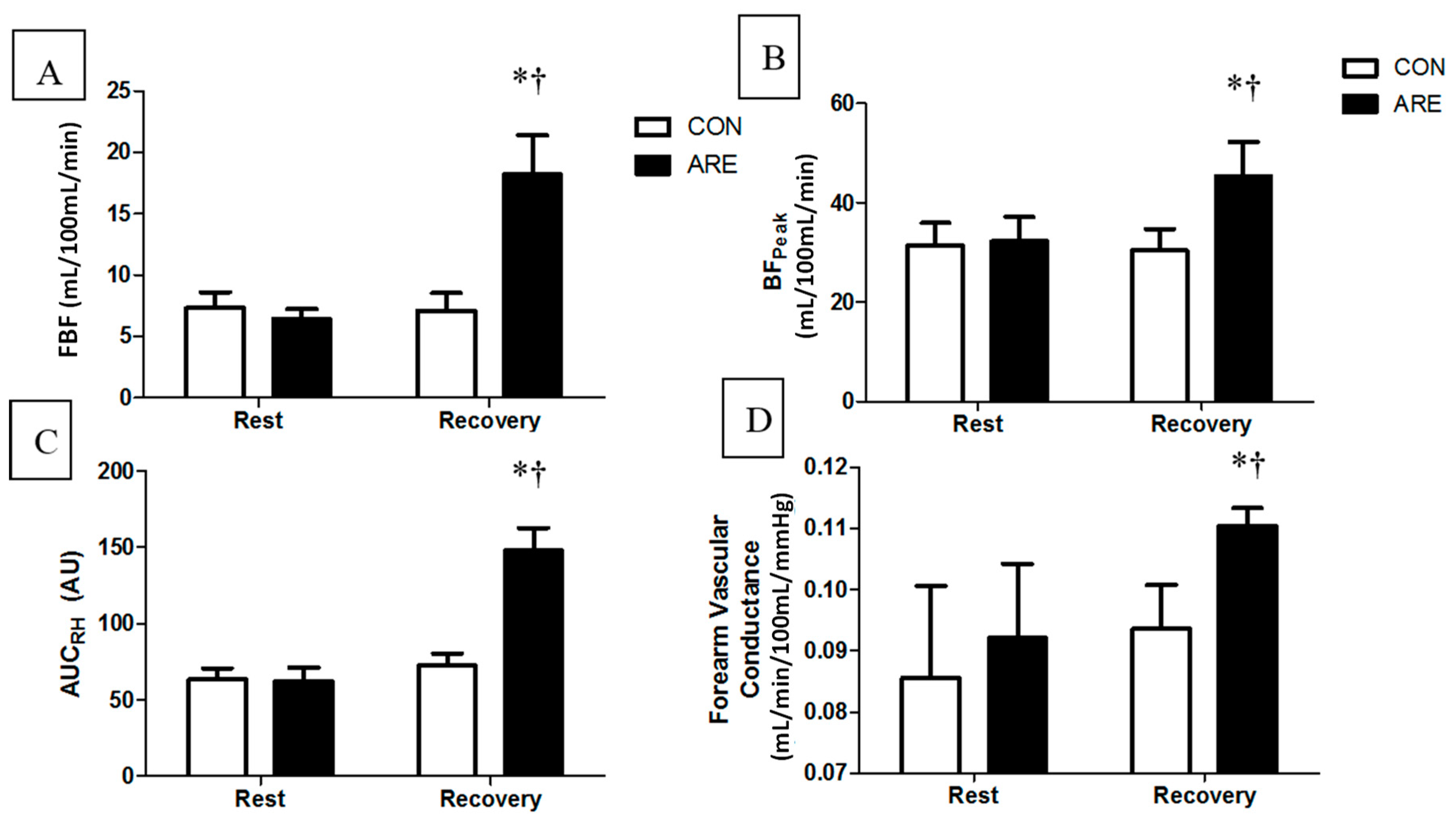
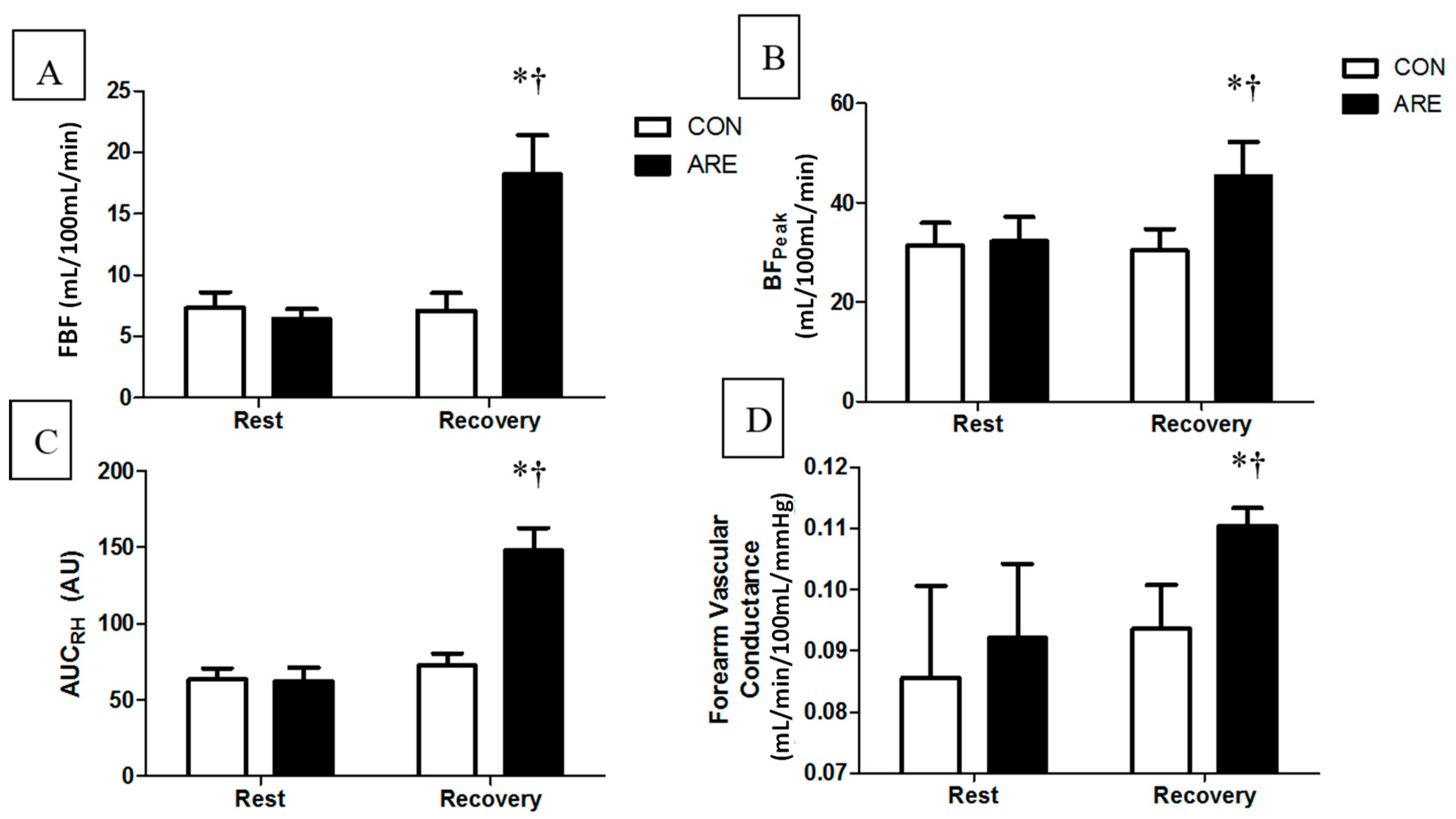
3.2. Endothelial Function
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Positon-Stand, American College of Sports Medicine Position Stand. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar]
- Kraemer, W.J.; Ratamess, N.A.; French, D.N. Resistance training for health and performance. Curr. Sports Med. Rep. 2002, 1, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Milliken, L.A.; Going, S.B.; Houtkooper, L.B.; Flint-Wagner, H.G.; Figueroa, A.; Metcalfe, L.L.; Blew, R.M.; Sharp, S.C.; Lohman, T.G. Effects of exercise training on bone remodeling, insulin-like growth factors, and bone mineral density in postmenopausal women with and without hormone replacement therapy. Calcif. Tissue Int. 2003, 72, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Hurley, B.F.; Roth, S.M. Strength training in the elderly: Effects on risk factors for age-related diseases. Sports Med. 2000, 30, 249–268. [Google Scholar] [CrossRef] [PubMed]
- Collier, S.R.; Diggle, M.D.; Heffernan, K.S.; Kelly, E.E.; Tobin, M.M.; Fernhall, B. Changes in arterial distensibility and flow-mediated dilation after acute resistance vs. aerobic exercise. J. Strength Cond. Res. 2010, 24, 2846–2852. [Google Scholar] [CrossRef] [PubMed]
- Yoon, E.S.; Jung, S.J.; Cheun, S.K.; Oh, Y.S.; Kim, S.H.; Jae, S.Y. Effects of acute resistance exercise on arterial stiffness in young men. Korean Circ. J. 2010, 40, 16–22. [Google Scholar] [CrossRef] [PubMed]
- DeVan, A.E.; Anton, M.M.; Cook, J.N.; Neidre, D.B.; Cortez-Cooper, M.Y.; Tanaka, H. Acute effects of resistance exercise on arterial compliance. J. Appl. Physiol. 2005, 98, 2287–2291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fahs, C.A.; Heffernan, K.S.; Fernhall, B. Hemodynamic and vascular response to resistance exercise with l-arginine. Med. Sci. Sports Exerc. 2009, 41, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Escamilla, R.F.; Fleisig, G.S.; Zheng, N.; Lander, J.E.; Barrentine, S.W.; Andrews, J.R.; Bergemann, B.W.; Moorman, C.T. Effects of technique variations on knee biomechanics during the squat and leg press. Med. Sci. Sports Exerc. 2001, 33, 1552–1566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCaw, S.T.; Friday, J.J. A comparison of muscle activity between a free weight and machine bench press. J. Strength Cond. Res. 1994, 8, 259. [Google Scholar]
- Santana, J.C.; Vera-Garcia, F.J.; McGill, S.M. A kinetic and electromyographic comparison of the standing cable press and bench press. J. Strength Cond. Res. 2007, 21, 1271–1277. [Google Scholar] [PubMed]
- Harrison, G.G.; Buskirk, E.R.; Lindsay Carter, J.E.; Johnston, F.E.; Lohman, T.G.; Pollock, M.L.; Roche, A.F.; Wilmore, J.H. Skinfold thickness and measurement technique. In Athropommetric Standardization Reference Manual; Lohman, T.G., Roche, A.F., Martorell, R., Eds.; Human Kinetics: Champaign, IL, USA, 1988; pp. 55–70. [Google Scholar]
- Brozek, J.; Grande, F.; Anderson, J.T.; Keys, D.A. Densitometric analysis of body composition: Revision of some quantative assumptions. Ann. N. Y. Acad. Sci. 1963, 110, 113–140. [Google Scholar] [CrossRef] [PubMed]
- Haff, G.G.; Triplett, N.T. Essentials of Strength Training and Conditioning, 4th ed.; Human Kinetics: Champaign, IL, USA, 2016. [Google Scholar]
- Eeftinck Schattenkerk, D.W.; van Lieshout, J.J.; van den Meiracker, A.H.; Wesseling, K.R.; Blanc, S.; Wieling, W.; van Montfrans, G.A.; Settels, J.J.; Wesseling, K.H.; Westerhof, B.E. Nexfin noninvasive continuous blood pressure validated against Riva-Rocci/Korotkoff. Am. J. Hypertens. 2009, 22, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, J.; Tanabe, T.; Miyachi, M.; Yamamoto, K.; Takahashi, K.; Iemitsu, M.; Otsuki, T.; Homma, S.; Maeda, S.; Ajisaka, R.; et al. Non-invasive assessment of cardiac output during exercise in healthy young humans: Comparison between Modelflow method and Doppler echocardiography method. Acta Physiol. Scand. 2003, 179, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Higashi, Y.; Sasaki, S.; Nakagawa, K.; Matsuura, H.; Kajiyama, G.; Oshima, T. A noninvasive measurement of reactive hyperemia that can be used to assess resistance artery endothelial function in humans. Am. J. Cardiol. 2001, 87, 121–125. [Google Scholar] [CrossRef]
- Tagawa, T.; Imaizumi, T.; Endo, T.; Shiramoto, M.; Harasawa, Y.; Takeshita, A. Role of nitric oxide in reactive hyperemia in human forearm vessels. Circulation 1994, 90, 2285–2290. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J.T.E. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Duncan, M.J.; Birch, S.L.; Oxford, S.W. The effect of exercise intensity on postresistance exercise hypotension in trained men. J. Strength Cond. Res. 2014, 28, 1706–1713. [Google Scholar] [CrossRef] [PubMed]
- Halliwill, J.R.; Taylor, J.A.; Eckberg, D.L. Impaired sympathetic vascular regulation in humans after acute dynamic exercise. J. Physiol. 1996, 495, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Kingsley, J.D.; Mayo, X.; Tai, Y.L.; Fennell, C. Arterial stiffness and autonomic modulation following free-weight resistance exercises in resistance trained individuals. J. Strength Cond. Res. 2016, 30, 3373–3380. [Google Scholar] [CrossRef] [PubMed]
- Mayo, X.; Iglesias-Soler, E.; Carballeira-Fernandez, E.; Fernandez-Del-Olmo, M. A shorter set reduces the loss of cardiac autonomic and baroreflex control after resistance exercise. Eur. J. Sport Sci. 2015, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Tatro, D.L.; Dudley, G.A.; Convertino, V.A. Carotid-cardiac baroreflex response and LBNP tolerance following resistance training. Med. Sci. Sports Exerc. 1992, 24, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Polito, M.D.; da Nobrega, A.C.; Farinatti, P. Blood pressure and forearm blood flow after multiple sets of a resistive exercise for the lower limbs. Blood Press. Monit. 2011, 16, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Polito, M.D.; Farinatti, P.T. The effects of muscle mass and number of sets during resistance exercise on postexercise hypotension. J. Strength Cond. Res. 2009, 23, 2351–2357. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, T.; Willardson, J.M.; Miranda, H.; Bentes, C.M.; Reis, V.M.; Simao, R. Influence of Load Intensity on Postexercise Hypotension and Heart Rate Variability after a Strength Training Session. J. Strength Cond. Res. 2015, 29, 2941–2948. [Google Scholar] [CrossRef] [PubMed]
- Rezk, C.C.; Marrache, R.C.; Tinucci, T.; Mion, D., Jr.; Forjaz, C.L. Post-resistance exercise hypotension, hemodynamics, and heart rate variability: Influence of exercise intensity. Eur. J. Appl. Physiol. 2006, 98, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Hutcheson, I.R.; Griffith, T.M. Release of endothelium-derived relaxing factor is modulated both by frequency and amplitude of pulsatile flow. Am. J. Physiol. 1991, 261, H257–H262. [Google Scholar] [CrossRef] [PubMed]
- Busse, R.; Edwards, G.; Feletou, M.; Fleming, I.; Vanhoutte, P.M.; Weston, A.H. EDHF: Bringing the concepts together. Trends Pharmacol. Sci. 2002, 23, 374–380. [Google Scholar] [CrossRef]
- Koller, A.; Huang, A.; Sun, D.; Kaley, G. Exercise training augments flow-dependent dilation in rat skeletal muscle arterioles. Role of endothelial nitric oxide and prostaglandins. Circ. Res. 1995, 76, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.M.; Beltran-Del-Rio, A.; Albrecht, A.; Lorenz, R.R.; Joyner, M.J. Local cholinergic mechanisms mediate nitric oxide-dependent flow-induced vasorelaxation in vitro. Am. J. Physiol. 1996, 270, H442–H446. [Google Scholar] [CrossRef] [PubMed]
- Rakobowchuk, M.; McGowan, C.L.; de Groot, P.C.; Hartman, J.W.; Phillips, S.M.; MacDonald, M.J. Endothelial function of young healthy males following whole body resistance training. J. Appl. Physiol. 2005, 98, 2185–2190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heffernan, K.S.; Fahs, C.A.; Iwamoto, G.A.; Jae, S.Y.; Wilund, K.R.; Woods, J.A.; Fernhall, B. Resistance exercise training reduces central blood pressure and improves microvascular function in African American and white men. Atherosclerosis 2009, 207, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Engelke, K.A.; Halliwill, J.R.; Proctor, D.N.; Dietz, N.M.; Joyner, M.J. Contribution of nitric oxide and prostaglandins to reactive hyperemia in human forearm. J. Appl. Physiol. 1996, 81, 1807–1814. [Google Scholar] [CrossRef] [PubMed]
- Collier, S.R.; Frechette, V.; Sandberg, K.; Schafer, P.; Ji, H.; Smulyan, H.; Fernhall, B. Sex differences in resting hemodynamics and arterial stiffness following 4 weeks of resistance versus aerobic exercise training in individuals with pre-hypertension to stage 1 hypertension. Biol. Sex Differ. 2011, 2, 9. [Google Scholar] [CrossRef] [PubMed]
- Ketel, I.J.; Stehouwer, C.D.; Serne, E.H.; Poel, D.M.; Groot, L.; Kager, C.; Hompes, P.G.; Homburg, R.; Twisk, J.W.; Smulders, Y.M.; et al. Microvascular function has no menstrual-cycle-dependent variation in healthy ovulatory women. Microcirculation 2009, 16, 714–724. [Google Scholar] [CrossRef] [PubMed]
- Adkisson, E.J.; Casey, D.P.; Beck, D.T.; Gurovich, A.N.; Martin, J.S.; Braith, R.W. Central, peripheral and resistance arterial reactivity: Fluctuates during the phases of the menstrual cycle. Exp. Biol. Med. 2010, 235, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Su, S.Y.; Wei, C.C.; Hsieh, C.L.; Tsao, J.Y.; Li, T.C.; Lin, T.H.; Chang, H.H.; Lo, L.C. Influence of menstrual cycle on pulse pressure waveforms measured from the radial artery in biphasic healthy women. J. Altern. Complement. Med. 2009, 15, 645–652. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | CON | ARE | ||
|---|---|---|---|---|
| Rest | Recovery | Rest | Recovery | |
| MAP (mm Hg) | 80 ± 5 | 84 ± 7 | 81 ± 7 | 79 ± 7 *,† |
| TPR (mm Hg/mL/min) | 0.12 ± 0.013 | 0.13 ± 0.014 | 0.13 ± 0.03 | 0.10 ± 0.13 *,† |
| HR (bpm) | 61 ± 10 | 58 ± 9 | 60 ± 9 | 89 ± 12 *,† |
| SV (mL/beat) | 86 ± 7 | 86 ± 7 | 86 ± 6 | 83 ± 3.3 *,† |
| CO (L/min) | 6.8 ± 0.9 | 6.5 ± 0.7 | 6.7 ± 0.9 | 7.8 ± 0.7 *,† |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tai, Y.L.; Marshall, E.M.; Parks, J.C.; Mayo, X.; Glasgow, A.; Kingsley, J.D. Changes in Endothelial Function after Acute Resistance Exercise Using Free Weights. J. Funct. Morphol. Kinesiol. 2018, 3, 32. https://doi.org/10.3390/jfmk3020032
Tai YL, Marshall EM, Parks JC, Mayo X, Glasgow A, Kingsley JD. Changes in Endothelial Function after Acute Resistance Exercise Using Free Weights. Journal of Functional Morphology and Kinesiology. 2018; 3(2):32. https://doi.org/10.3390/jfmk3020032
Chicago/Turabian StyleTai, Yu Lun, Erica M. Marshall, Jason C. Parks, Xian Mayo, Alaina Glasgow, and J. Derek Kingsley. 2018. "Changes in Endothelial Function after Acute Resistance Exercise Using Free Weights" Journal of Functional Morphology and Kinesiology 3, no. 2: 32. https://doi.org/10.3390/jfmk3020032