Early Detection with Pulse Oximetry of Hypoxemic Neonatal Conditions. Development of the IX Clinical Consensus Statement of the Ibero-American Society of Neonatology (SIBEN)


{kind=link}
Abstract
:1. Introduction and Methodology
2. Background on Screening for Congenital Heart Disease
3. SIBEN’s Consensus on Screening with Pulse Oximetry: An Overview
- Cyanosis and related concepts.
- What is hypoxemia?
- What is hypoxia?
- What is pulse oximetry, and what are the normal values in a healthy term newborn?
- What is the hemoglobin dissociation curve?
- How does altitude influence on the SpO2?
- Which are the lesions that can be detected early?
- How should you do the screening?
- What are normal and abnormal results?
- What are false positive and false negative results?
- How should you interpret the pre- and post-ductal SpO2 difference?
- What should we do with an apparently healthy newborn that fails the screening?
- How should we take care of the family of a newborn that has either a positive or negative screening?
- Is this program cost-effective?
- When should we order an echocardiogram?
- Importance of the information and participation of the healthcare team—what data should you record?
- Who should do the screening?
- What limitations does pulse oximetry have?
- What role can the Perfusion Index (PI) have during the screening?
- Early sepsis
- Congenital pneumonia
- Pulmonary hypertension
- Meconium aspiration
- Transient tachypnea
- Pneumothorax
- Other various less frequent neonatal conditions
4. SIBEN’s Consensus on Screening with Pulse Oximetry: A Summary
4.1. Evaluation with SpO2 Monitors and Sampling Sites
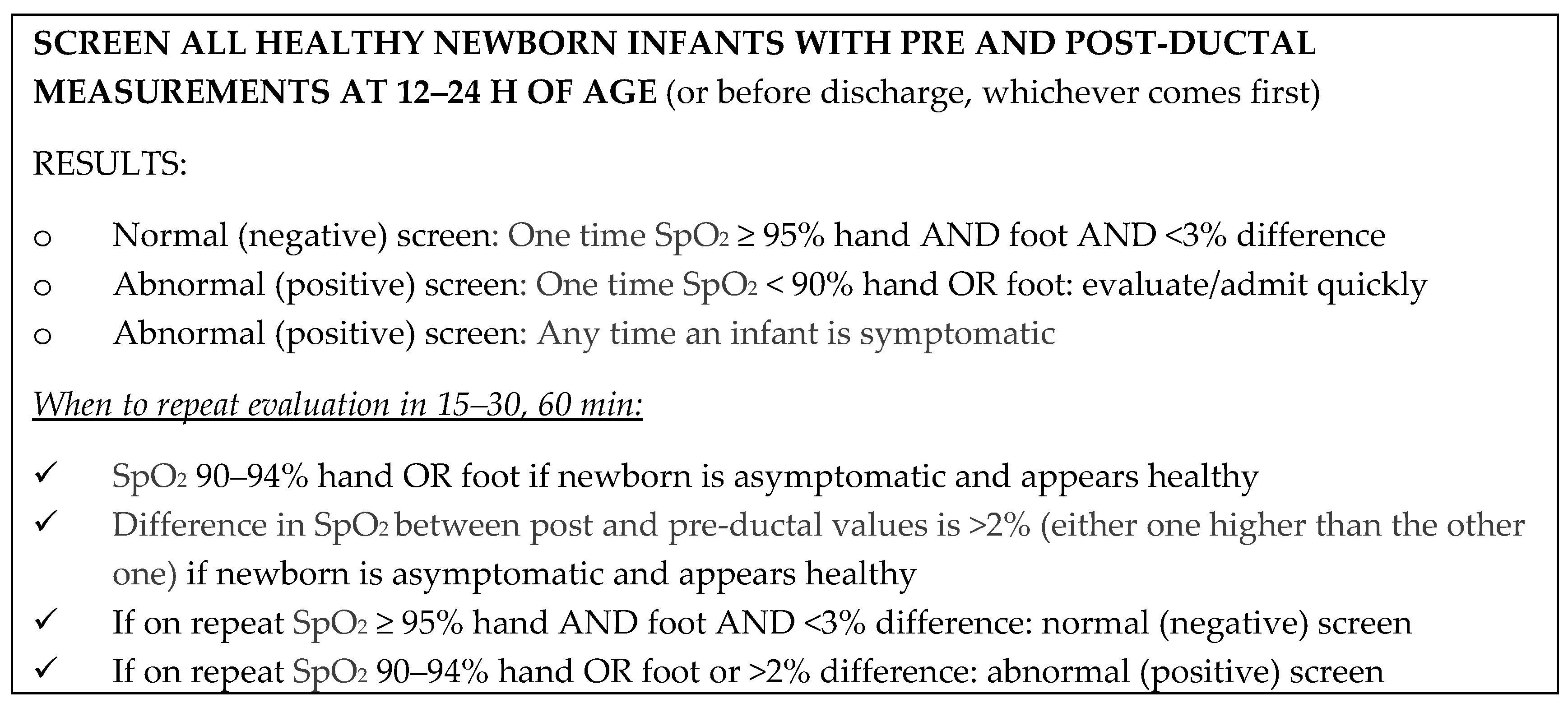
4.2. Clinical Protocol
4.3. What to Do with a Neonate Who Appears Clinically Healthy but Has Abnormal or Positive SpO2?
4.4. Concept of False Positive and False Negative Screening
4.5. Altitude and Neonatal SpO2 Screening
4.6. Care of the Family with an Abnormal or Positive Screening
5. Summary and Discussion
Author Contributions
Conflicts of Interest
References
- Bernier, P.L.; Stefanescu, A.; Samoukovic, G.; Tchervenkov, C.I. The challenge of congenital heart disease worldwide: Epidemiologic and demographic facts. Semin. Thorac. Cardiovasc. Surg. Pediatr. Card. Surg. Annu. 2010, 13, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Reller, M.D.; Strickland, M.J.; Riehle-Colarusso, T.; Mahle, W.T.; Correa, A. Prevalence of congenital heart defects in metropolitan Atlanta, 1998–2005. J. Pediatr. 2008, 153, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.I.E.; Kaplan, S. The incidence of congenital heart disease. J. Am. Coll. Cardiol. 2002, 39, 1890–1900. [Google Scholar] [CrossRef]
- Van der Linde, D.; Konings, E.E.M.; Slager, M.A.; Witsenburg, M.; Helbin, W.A.; Takkenberg, J.J.M.; Roos-Hesselink, J.W. Birth Prevalence of Congenital Heart Disease Worldwide: A Systematic Review and Meta-analysis. J. Am. Coll. Cardiol. 2011, 58, 2241–2247. [Google Scholar] [CrossRef] [PubMed]
- Oster, M.; Lee, K.; Honein, M.; Riehle-Colarusso, T.; Shin, M.; Correa, A. Temporal trends in survival among infants with critical congenital heart defects. Pediatrics 2013, 131, e1502–e1508. [Google Scholar] [CrossRef] [PubMed]
- Chang, R.K.; Gurvitz, M.; Rodriguez, S. Missed diagnosis of critical congenital heart disease. Arch. Pediatr. Adolesc. Med. 2008, 162, 969–974. [Google Scholar] [CrossRef] [PubMed]
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [Google Scholar]
- Hoffman, J.I.E. The global burden of congenital heart disease. Cardiovasc. J. Afr. 2013, 24, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Kuehl, K.S.; Loffredo, C.A.; Ferencz, C. Failure to diagnose congenital heart disease in infancy. Pediatrics 1999, 103, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Meberg, A.; Lindberg, H.; Thaulow, E. Congenital heart defects: The patients who die. Acta Paediatr. 2005, 94, 1060–1065. [Google Scholar] [CrossRef] [PubMed]
- Ailes, E.C.; Honein, M.A. Estimated Number of Infants Detected and Missed by Critical Congenital Heart Defect Screening. Pediatrics 2015, 135, 1000–1008. [Google Scholar] [CrossRef] [PubMed]
- De-Wahl Granelli, A.; Wennergren, M.; Sandberg, K.; Mellander, M.; Bejlum, C.; Inganäs, L.; Eriksson, M.; Segerdahl, N.; Agren, A.; Ekman-Joelsson, B.M.; et al. Impact of pulse oximetry screening on the detection of duct dependent congenital heart disease: A Swedish prospective screening study in 39,821 newborns. BMJ 2009, 338, a3037. [Google Scholar] [CrossRef] [PubMed]
- Ewer, A.K.; Middleton, L.J.; Furmston, A.T.; Bhoyar, A.; Daniels, J.P.; Thangaratinam, S.; Deeks, J.J.; Khan, K.S.; PulseOx Study Group. Pulse oximetry as a screening test for congenital heart defects in newborn infants (PulseOx): A test accuracy study. Lancet 2011, 378, 785–794. [Google Scholar] [CrossRef]
- Hu, X.J.; Ma, X.J.; Zhao, Q.M.; Yan, W.L.; Ge, X.L.; Jia, B.; Liu, F.; Wu, L.; Ye, M.; Liang, X.C.; et al. Pulse Oximetry and Auscultation for Congenital Heart Disease Detection. Pediatrics 2017, 140, e20171154. [Google Scholar] [CrossRef] [PubMed]
- Kemper, A.R.; Mahle, W.T.; Martin, G.R.; Cooley, W.C.; Kumar, P.; Morrow, W.R.; Kelm, K.; Pearson, G.D.; Glidewell, J.; Grosse, S.D.; et al. Strategies for Implementing Screening for Critical Congenital Heart Disease. Pediatrics 2011, 128, 1259–1267. [Google Scholar] [CrossRef] [PubMed]
- Frank, L.H.; Bradshaw, E.; Beekman, R.; Mahle, W.T.; Martin, G.R. Critical Congenital Heart Disease Screening Using Pulse Oximetry. J. Pediatr. 2012, 162, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Glidewell, J.; Olney, R.S.; Hinton, C.; Pawelski, J.; Sontag, M.; Wood, T.; Kucik, J.E.; Daskalov, R.; Hudson, J. Centers for Disease Control and Prevention (CDC). State Legislation, Regulations, and Hospital Guidelines for Newborn Screening for Critical Congenital Heart Defects—United States, 2011–2014. Morb. Mortal. Wkly. Rep. 2015, 64, 625–630. [Google Scholar]
- Thangaratinam, S.; Brown, K.; Zamora, J.; Khan, K.S.; Ewer, A.K. Pulse oximetry screening for critical congenital heart defects in asymptomatic newborn babies: A systematic review and meta-analysis. Lancet 2012, 379, 2459–2464. [Google Scholar] [CrossRef]
- Sola, A.; Fariña, D.; Mir, R.; Garrido, D.; Pereira, A.; Montes Bueno, M.T.; Lemus, L. y Colaboradores del Consenso Clínico SIBEN. In Detección Precoz con Pulsioximetría de Enfermedades que Cursan con Hipoxemia Neonatal; EDISIBEN: Asunción, Paraguay, 2016; ISBN 978-1-5323-0369-2. [Google Scholar]
- Roberts, T.E.; Barton, P.M.; Auguste, P.E.; Middleton, L.J.; Furmston, A.T.; Ewer, A.K. Pulse oximetry as a screening test for congenital heart defects in newborn infants: A cost-effectiveness analysis. Arch. Dis. Child. 2012, 97, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Peterson, C.; Grosse, S.D.; Oster, M.E.; Olney, R.S.; Cassell, C.H. Cost-effectiveness of routine screening for critical congenital heart disease in US newborns. Pediatrics 2013, 132, e595–e603. [Google Scholar] [CrossRef] [PubMed]
- Oster, M.E.; Aucott, S.W.; Glidewell, J.; Hackell, J.; Kochilas, L.; Martin, G.R.; Phillippi, J.; Pinto, N.M.; Saarinen, A.; Sontag, M.; et al. Lessons Learned From Newborn Screening for Critical Congenital Heart Defects. Pediatrics 2016, 137, e20154573. [Google Scholar] [CrossRef] [PubMed]
- Powell, R.; Pattison, H.M.; Bhoyar, A.; Furmston, A.T.; Middleton, L.J.; Daniels, J.P.; Ewer, A.K. Pulse oximetry screening for congenital heart defects in newborn infants: An evaluation of acceptability to mothers. Arch. Dis. Child. Fetal Neonatal Ed. 2013, 98, F59–63. [Google Scholar] [CrossRef] [PubMed]
- Abouk, R.; Grosse, S.D.; Ailes, E.C.; Oster, M.E. Association of US State Implementation of Newborn Screening Policies for Critical Congenital Heart Disease With Early Infant Cardiac Deaths. JAMA 2017, 318, 2111–2118. [Google Scholar] [CrossRef] [PubMed]
- Sola, A.; Urman, J. Cuidados Intensivos Neonatales: Fisiopatología y Terapéutica; Científica Interamericana: Buenos Aires, Argentina, 1987; ISBN 9509428078, 9789509428072. [Google Scholar]
- Sola, A.; Rogido, M. Cuidados Neonatales; Científica Interamericana: Buenos Aires, Argentina, 2000; Volume 2, ISBN 89872427570-4. [Google Scholar]
- Zhang, L.; Mendoza-Sassi, R.; Santos, J.C.; Lau, J. Accuracy of symptoms and signs in predicting hypoxaemia among young children with acute respiratory infection: A meta-analysis. Int. J. Tuberc. Lung Dis. 2011, 15, 317–325. [Google Scholar] [PubMed]
- Niermeyer, S.; Yang, P.; Shanmina; Drolkar; Zhuang, J.; Moore, L.G. Arterial oxygen saturation in Tibetan and Han infants born in Lhasa, Tibet. N. Engl. J. Med. 1995, 333, 1248–1252. [Google Scholar] [CrossRef] [PubMed]
- Laman, M.; Ripa, P.; Vince, J.; Tefuarani, N. Can clinical signs predict hypoxaemia in Papua New Guinean children with moderate and severe pneumonia? Ann. Trop. Paediatr. 2005, 25, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Dawson, A.L.; Cassell, C.H.; Riehle-Colarusso, T.; Grosse, S.D.; Tanner, J.P.; Kirby, R.S.; Watkins, S.M.; Correia, J.A.; Olney, R.S. Factors associated with late detection of critical congenital heart disease in newborns. Pediatrics 2013, 132, e604–e611. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.; Ekström, A.; Frisk, C.; Thio, M.; Roehr, C.C.; Kamlin, C.O.; Donath, S.M.; Davis, P.G.; Giraffe Study Group. Assessing the tongue colour of newly born infants may help predict the need for supplemental oxygen in the delivery room. Acta Paediatr. 2015, 104, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Sola, A.; Chow, L.; Rogido, M. Pulse oximetry in neonatal care in 2005. A comprehensive state of the art review. An. Pediatr. (Barc) 2005, 62, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Barker, S.J. The effects of motion and hypoxemia upon the accuracy of 20 pulse oximeters in human volunteers. Sleep 2001, 24, A406–A407. [Google Scholar]
- Hay, W.; Rodden, D.; Collins, S.; Melaria, D.; Hale, K.; Faushaw, L. Reliability of conventional and new pulse oximetry in neonatal patients. J. Perinatol. 2002, 22, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Sola, A. Monitorización biofísica y saturometría. In Cuidados Neonatales, 3rd ed.; Edimed: Buenos Aires, Argentina, 2011; ISBN 8963252767-5. [Google Scholar]
- Sola, A.; Golombek, S.; Montes Bueno, M.T.; Lemus, L.; Zuluaga, C.; Domínguez, F.; Baquero, H.; Young Sarmiento, A.E.; Natta, D.; Rodriguez Perez, J.M.; et al. Safe oxygen saturation targeting and monitoring in preterm infants: Can we avoid hypoxia and hyperoxia? Acta Paediatr. 2014, 103, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.A.; Vento, M.; Finer, N.N.; Rich, W.; Saugstad, O.D.; Morley, C.J.; Davis, P.G. Managing oxygen therapy during delivery room stabilization of preterm infants. J. Pediatr. 2012, 160, 158–161. [Google Scholar] [CrossRef] [PubMed]
- Davis, P.G.; Dawson, J.A. New concepts in neonatal resuscitation. Curr. Opin. Pediatr. 2012, 24, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Niermeyer, S.; Andrade-M, M.P.; Vargas, E.; Moore, L.G. Neonatal oxygenation, pulmonary hypertension, and evolutionary adaptation to high altitude (2013 Grover Conference series). Pulm. Circ. 2015, 5, 48–62. [Google Scholar] [CrossRef] [PubMed]
- Hill, C.M.; Baya, A.; Gavlak, J.; Carroll, A.; Heathcote, K.; Dimitriou, D.; L’Esperance, V.; Webster, R.; Holloway, J.; Virues-Ortega, J.; et al. Adaptation to Life in the High Andes: Nocturnal Oxyhemoglobin Saturation in Early Development. Sleep 2016, 39, 1001–1008. [Google Scholar] [CrossRef] [PubMed]
- Diaz, G.; Sandoval, J.; Sola, A. Hipertension Pulmonar en Niños; Distribuna: Bogotá, Colombia, 2011; ISBN 9789588379357. [Google Scholar]
- Sendelbach, D.M.; Jackson, G.L.; Lai, S.S.; Fixler, D.E.; Stehel, E.K.; Engle, W.D. Pulse oximetry screening at 4 h of age to detect critical congenital heart defects. Pediatrics 2008, 122, e815–e820. [Google Scholar] [CrossRef] [PubMed]
- Ewer, A.K. Evidence for CCHD screening and its practical application using pulse oximetry. Early Hum. Dev. 2014, 90, S19–S21. [Google Scholar] [CrossRef]
- Ewer, A.K. Pulse oximetry screening: Do we have enough evidence now? Lancet 2014, 30, 725–726. [Google Scholar] [CrossRef]
- Ewer, A.K. Pulse oximetry screening for critical congenital heart defects. Should it be routine? Arch. Dis. Child. Fetal Neonatal Ed. 2014, 99, F93–F95. [Google Scholar] [CrossRef] [PubMed]
- Ewer, A.K. Review of pulse oximetry screening for critical congenital heart defects. Curr. Opin. Cardiol. 2013, 28, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Ma, Z.; Ge, Z.; Liu, F.; Yan, W.L.; Wu, L.; Ye, M.; Liang, X.C.; Zhang, J.; Gao, Y.; et al. Pulse oximetry with clinical assessment to screen for congenital heart disease in neonates in China: A prospective study. Lancet 2014, 384, 747–754. [Google Scholar] [CrossRef]
- Singh, A.; Rasiah, S.V.; Ewer, A.K. The impact of routine predischarge pulse oximetry screening in a regional neonatal unit. Arch. Dis. Child. Fetal Neonatal Ed. 2014, 99, F297–302. [Google Scholar] [CrossRef] [PubMed]
- Piasek, C.Z.; Van Bel, F.; Sola, A. Perfusion index in newborn infants: A noninvasive tool for neonatal monitoring. Acta Paediatr. 2014, 103, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Granelli, A.; Ostman-Smith, I. Noninvasive peripheral perfusion index as a possible tool for screening for critical left heart obstruction. Acta Paediatr. 2007, 96, 1455–1459. [Google Scholar] [CrossRef] [PubMed]
- Ewer, A.K.; Furmston, A.T.; Middleton, L.J.; Deeks, J.J.; Daniels, J.P.; Pattison, H.M.; Powell, R.; Roberts, T.E.; Barton, P.; Auguste, P.; et al. Pulse oximetry as a screening test for congenital heart defects in newborn infants: A test accuracy study with evaluation of acceptability and cost-effectiveness. Health Technol. Assess. 2012, 16, 1–184. [Google Scholar] [CrossRef] [PubMed]
- Ewer, A.K. How to develop a business case to establish a neonatal pulse oximetry screening programme for screening of congenital heart defects. Early Hum. Dev. 2012, 88, 915–919. [Google Scholar] [CrossRef] [PubMed]
- De Wahl Granelli, A.; Mellander, M.; Sunnegårdh, J.; Sandberg, K.; Ostman-Smith, I. Screening for duct-dependant congenital heart disease with pulse oximetry: A critical evaluation of strategies to maximize sensitivity. Acta Paediatr. 2005, 94, 1590–1596. [Google Scholar] [CrossRef] [PubMed]
- Tworetzky, W.; McElhinney, D.B.; Reddy, V.M.; Brook, M.M.; Hanley, F.L.; Silverman, N.H. Improved surgical outcome after fetal diagnosis of hypoplastic left heart syndrome. Circulation 2001, 103, 1269–1273. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, D.; Coltri, A.; Butera, G.; Fermont, L.; Le Bidois, J.; Kachaner, J.; Sidi, D. Detection of transposition of the great arteries in fetuses reduces neonatal morbidity and mortality. Circulation 1999, 99, 916–918. [Google Scholar] [CrossRef] [PubMed]
- Quartermain, M.D.; Pasquali, S.K.; Hill, K.D.; Goldberg, D.J.; Huhta, J.C.; Jacobs, J.P.; Jacobs, M.L.; Kim, S.; Ungerleider, R.M. Variation in Prenatal Diagnosis of Congenital Heart Disease in Infants. Pediatrics 2015, 136, e378–385. [Google Scholar] [CrossRef] [PubMed]
- Narayen, I.C.; Blom, N.A.; Bourgonje, M.S.; Haak, M.C.; Smit, M.; Posthumus, F.; van den Broek, A.J.; Havers, H.M.; te Pas, A.B. Pulse Oximetry Screening for Critical Congenital Heart Disease after Home Birth and Early Discharge. J. Pediatr. 2016, 170, 188–192. [Google Scholar] [CrossRef] [PubMed]
- De-Wahl Granelli, A.; Meberg, A.; Ojala, T.; Steensberg, J.; Oskarsson, G.; Mellander, M. Nordic pulse oximetry screening—Implementation status and proposal for uniform guidelines. Acta Paediatr. 2014, 103, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Narayen, I.C.; Blom, N.A.; Ewer, A.K.; Vento, M.; Manzoni, P.; Te Pas, A.B. Aspects of pulse oximetry screening for critical congenital heart defects: How, when and why? Arch. Dis. Child. Fetal Neonatal Ed. 2016, 101, F162–167. [Google Scholar] [CrossRef] [PubMed]
- Lakshminrusimha, S.; Sambalingam, D.; Carrion, V. Universal pulse oximetry screen for critical congenital heart disease in the NICU. J. Perinatol. 2014, 34, 343–344. [Google Scholar] [CrossRef] [PubMed]
- Teitel, D. Recognition of Undiagnosed Neonatal Heart Disease. Clin. Perinatol. 2016, 43, 81–98. [Google Scholar] [CrossRef] [PubMed]
- Ravert, P.; Detwiler, T.L.; Dickinson, J.K. Mean oxygen saturation in well neonates at altitudes between 4498 and 8150 feet. Adv. Neonatal Care 2011, 11, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, N. Cardiopatías congénitas en Colombia y en el mundo. Rev. Colomb. Cardiol. 2015, 22, 1–2. [Google Scholar] [CrossRef]
- Reducing Neonatal Mortality and Morbidity in Latin America and The Caribbean. An Interagency Strategic Consensus. Available online: http://resourcecentre.savethechildren.se/sites/default/files/documents/2729 (accessed on 30 January 2018).

© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sola, A.; Golombek, S.G. Early Detection with Pulse Oximetry of Hypoxemic Neonatal Conditions. Development of the IX Clinical Consensus Statement of the Ibero-American Society of Neonatology (SIBEN). Int. J. Neonatal Screen. 2018, 4, 10. https://doi.org/10.3390/ijns4010010
Sola A, Golombek SG. Early Detection with Pulse Oximetry of Hypoxemic Neonatal Conditions. Development of the IX Clinical Consensus Statement of the Ibero-American Society of Neonatology (SIBEN). International Journal of Neonatal Screening. 2018; 4(1):10. https://doi.org/10.3390/ijns4010010
Chicago/Turabian StyleSola, Augusto, and Sergio G. Golombek. 2018. "Early Detection with Pulse Oximetry of Hypoxemic Neonatal Conditions. Development of the IX Clinical Consensus Statement of the Ibero-American Society of Neonatology (SIBEN)" International Journal of Neonatal Screening 4, no. 1: 10. https://doi.org/10.3390/ijns4010010