
A Non-Derivatized Assay for the Simultaneous Detection of Amino Acids, Acylcarnitines, Succinylacetone, Creatine, and Guanidinoacetic Acid in Dried Blood Spots via Tandem Mass Spectrometry


Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagents
2.2. Dried Blood Spots
2.3. Sample Preparation
2.3.1. Non-Derivatized AAAC Method
2.3.2. Derivatized GAMT Method
2.3.3. Non-Derivatized AAAC-GAMT Method
2.4. Instrumentation and Data Analysis
3. Results
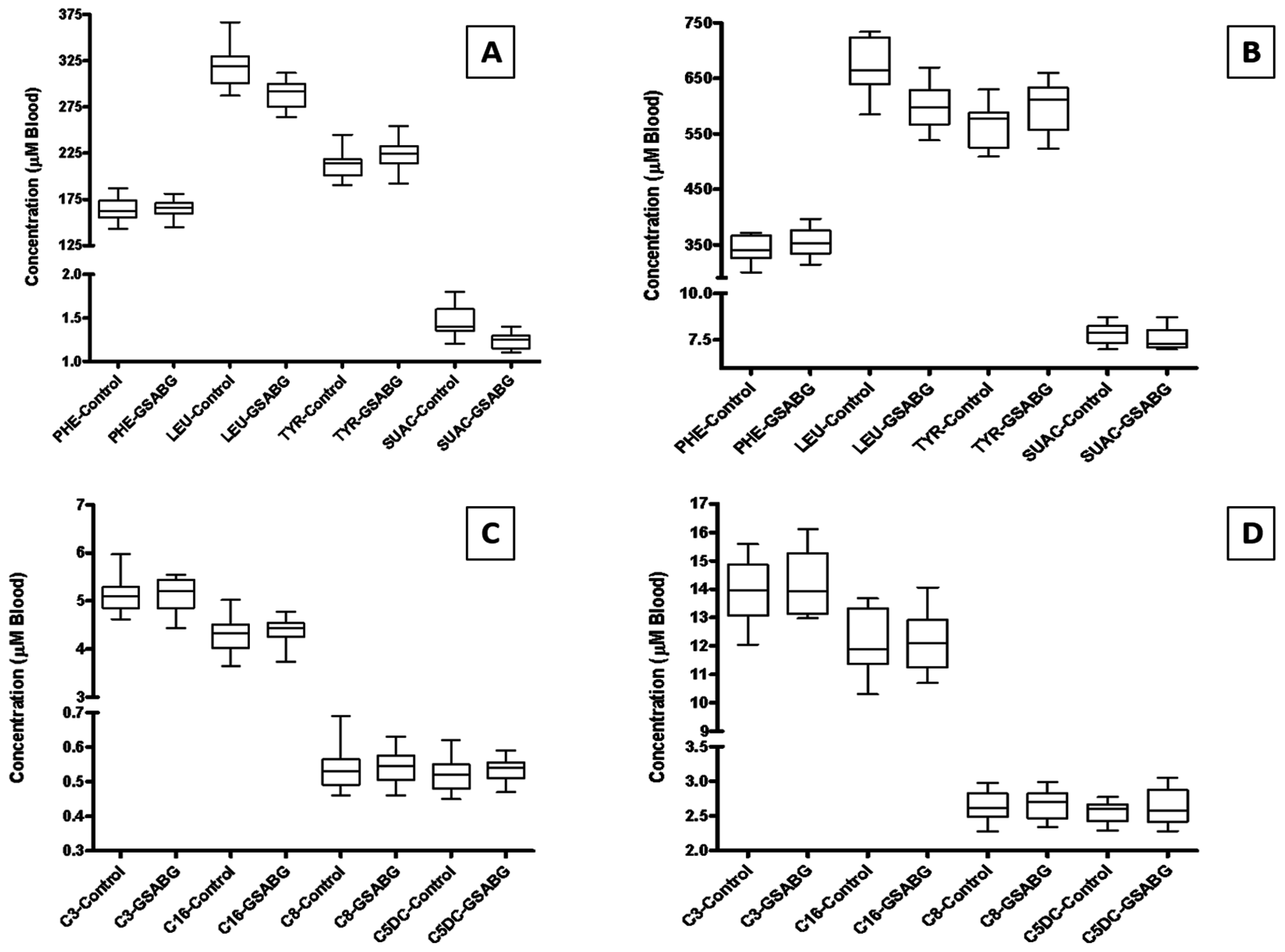
3.1. Amino Acids and Acylcarnitines Analysis Comparison
3.2. Creatine and Guanidinoacetic Acid Analysis Comparison
3.3. Non-Derivatized AAAC-GAMT Analytical Method Validation
3.3.1. Precision
3.3.2. Linearity, Limit of Blank, Limit of Detection
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Pasquali, M.; Schwarz, E.; Jensen, M.; Yuzyuk, T.; DeBiase, I.; Randall, H.; Longo, N. Feasibility of newborn screening for guanidinoacetate methyltransferase (gamt) deficiency. J. Inherit. Metab. Dis. 2014, 37, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Longo, N.; Ardon, O.; Vanzo, R.; Schwartz, E.; Pasquali, M. Disorders of creatine transport and metabolism. Am. J. Med. Genet. C Semin. Med. Genet. 2011, 157C, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Schulze, A.; Mayatepek, E.; Bachert, P.; Marescau, B.; De Deyn, P.P.; Rating, D. Therapeutic trial of arginine restriction in creatine deficiency syndrome. Eur. J. Pediatr. 1998, 157, 606–607. [Google Scholar] [CrossRef] [PubMed]
- Gordon, N. Guanidinoacetate methyltransferase deficiency (gamt). Brain Dev. 2010, 32, 79–81. [Google Scholar] [CrossRef] [PubMed]
- El-Gharbawy, A.H.; Goldstein, J.L.; Millington, D.S.; Vaisnins, A.E.; Schlune, A.; Barshop, B.A.; Schulze, A.; Koeberl, D.D.; Young, S.P. Elevation of guanidinoacetate in newborn dried blood spots and impact of early treatment in gamt deficiency. Mol. Genet. Metab. 2013, 109, 215–217. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services, Advisory Committe on Heritable Disorders in Newborns and Children. Guanidinoacetate Methyltransferase Deficiency (gamt)—Update from the Nomination and Priotization Workgroup. Available online: http://www.hrsa.gov/advisorycommittees/mchbadvisory/heritabledisorders/meetings/2016/eleventh/index.html (accessed on 30 June 2016).
- Slazyk, W.E.; Hannon, W.H. Quality assurance in the newborn screening laboratory. In Laboratory Methods for Neonatal Screening; Therrell, B.L., Ed.; American Public Health Association: Washington, DC, USA, 1993. [Google Scholar]
- Mei, J.V.; Alexander, J.R.; Adam, B.W.; Hannon, W.H. Use of filter paper for the collection and analysis of human whole blood specimens. J. Nutr. 2001, 131, 1631S–1636S. [Google Scholar] [PubMed]
- Clinical & Laboratory Standards Institute (CLSI). Evaluation of Detection Capability for Clinical Laboratory Measurement Procedures, Approved Guideline-Second Edition; EP17-A2; CLSI: Wayne, PA, USA, 2012. [Google Scholar]


{kind=link}
| Analyte | GAMT Derivatized (Control) Method | AAAC-GAMT Non-Derivatized (New) Method | ||||
|---|---|---|---|---|---|---|
| Low | Medium | High | Low | Medium | High | |
| QC | QC | QC | QC | QC | QC | |
| Creatine (CRE) | 264.88 | 394.42 | 675.47 | 277.98 | 414.01 | 685.32 |
| Guanidinoacetic Acid (GAA) | 3.04 | 7.33 | 11.88 | 3.25 | 7.98 | 12.56 |
| Analyte | 95% Confidence Intervals | ||
|---|---|---|---|
| Low | Med | High | |
| QC | QC | QC | |
| Creatine (CRE) | 120.30–366.36 | 195.18–513.68 | 273.01–906.63 |
| Guanidinoacetic Acid (GAA) | 2.47–3.69 | 6.25–9.11 | 10.36–14.56 |
| Analyte | Expected Concentration | Mean Concentration | Intraday Variability | Interday Variability | ||
|---|---|---|---|---|---|---|
| Std. Dev. | CV (%) | Std. Dev. | CV (%) | |||
| Creatine (CRE) | QC Low—249.35 | 232.58 | 11.63 | 5.0 | 24.44 | 10.5 |
| QC High—499.35 | 463.60 | 23.01 | 5.0 | 53.08 | 11.4 | |
| Guanidinoacetic Acid (GAA) | QC Low—5.22 | 3.95 | 0.54 | 13.8 | 0.36 | 9.0 |
| QC High—10.22 | 8.38 | 0.78 | 9.3 | 0.87 | 10.4 | |
| Analyte | AAAC-GAMT LoB | AAAC-GAMT LoD |
|---|---|---|
| Creatine (CRE) | 0.21 | 31.38 |
| Guanidinoacetic Acid (GAA) | 2.21 | 2.95 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asef, C.K.; Khaksarfard, K.M.; De Jesús, V.R. A Non-Derivatized Assay for the Simultaneous Detection of Amino Acids, Acylcarnitines, Succinylacetone, Creatine, and Guanidinoacetic Acid in Dried Blood Spots via Tandem Mass Spectrometry. Int. J. Neonatal Screen. 2016, 2, 13. https://doi.org/10.3390/ijns2040013
Asef CK, Khaksarfard KM, De Jesús VR. A Non-Derivatized Assay for the Simultaneous Detection of Amino Acids, Acylcarnitines, Succinylacetone, Creatine, and Guanidinoacetic Acid in Dried Blood Spots via Tandem Mass Spectrometry. International Journal of Neonatal Screening. 2016; 2(4):13. https://doi.org/10.3390/ijns2040013
Chicago/Turabian StyleAsef, Carter K., Kameron M. Khaksarfard, and Víctor R. De Jesús. 2016. "A Non-Derivatized Assay for the Simultaneous Detection of Amino Acids, Acylcarnitines, Succinylacetone, Creatine, and Guanidinoacetic Acid in Dried Blood Spots via Tandem Mass Spectrometry" International Journal of Neonatal Screening 2, no. 4: 13. https://doi.org/10.3390/ijns2040013