Cancer-Related Information Seeking and Scanning Behaviors among Older Chinese Adults: Examining the Roles of Fatalistic Beliefs and Fear


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.3. Data Analysis
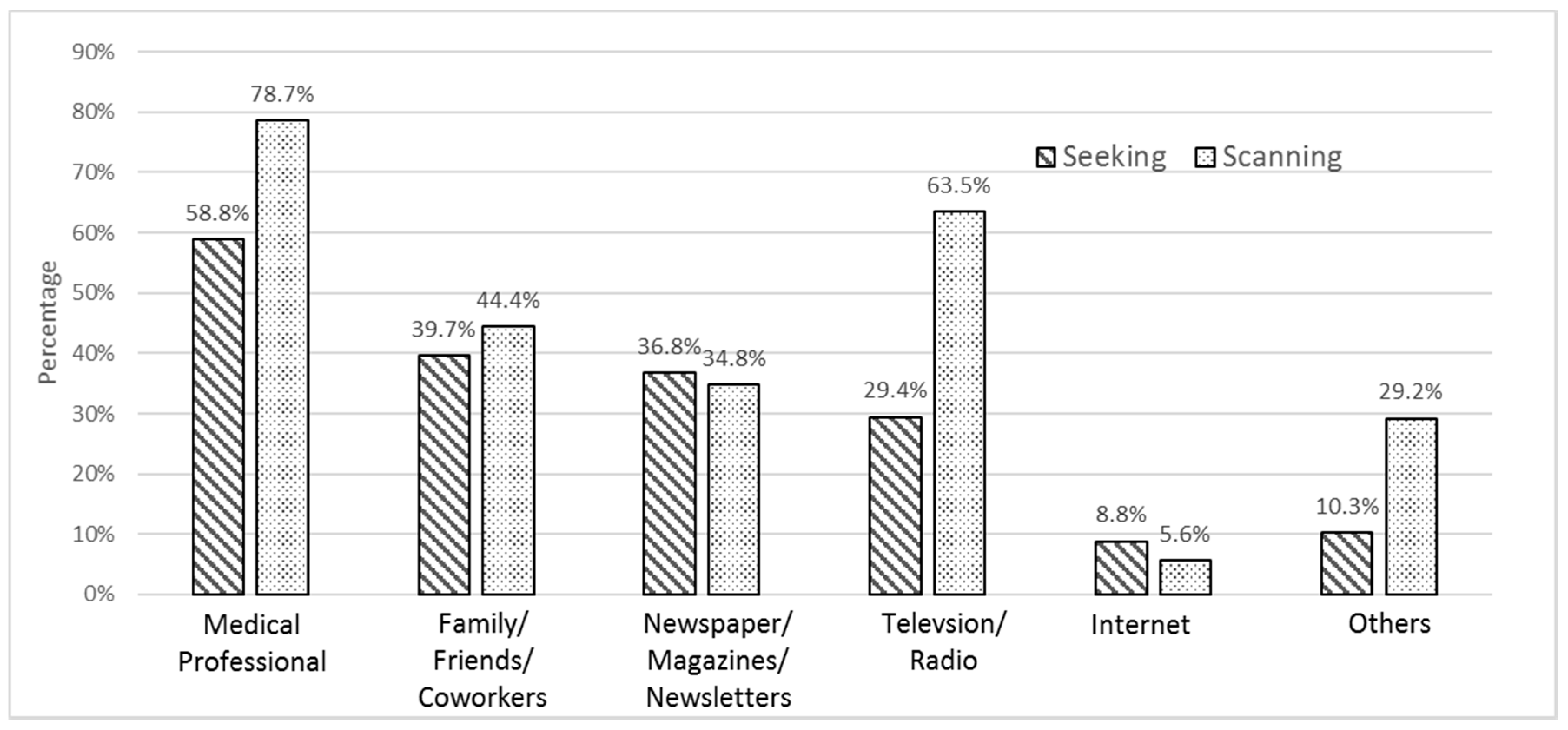
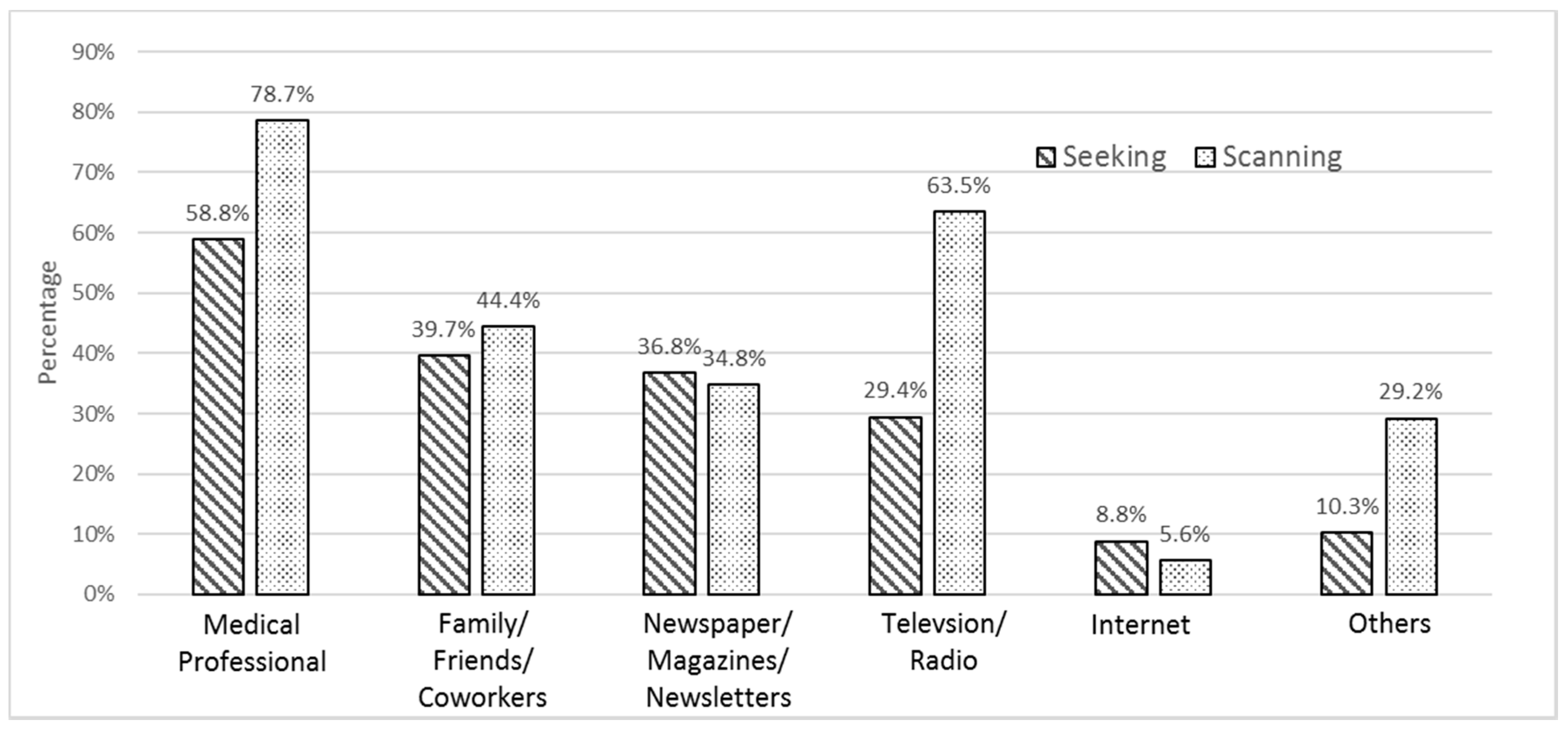
3. Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Bray, F.; Soerjomataram, I. The Changing global burden of cancer: Transition in human development and implications for cancer prevention and control. In Disease Control Priorities: Cancer, 3rd ed.; Gelband, H., Jha, P., Sankaranarayanan, R., Horton, S., Eds.; The World Bank: Washington, DC, USA, 2015; Volume 3, pp. 23–44. ISBN 978-1-4648-0350-5. [Google Scholar]
- World Health Organization. Cancer Fact Sheet. Available online: http://www.who.int/mediacentre/factsheets/fs297/en/ (accessed on 1 November 2017).
- Tsoi, K.F.; Hirai, H.W.; Chan, F.C.H.; Griffiths, S.; Sung, J.J.Y. Cancer burden with ageing population in urban regions in China: Projection on cancer registry data from World Health Organization. Br. Med. Bull. 2017, 121, 83–94. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Intelligence Network. Older People and Cancer. Available online: http://www.ncin.org.uk/publications/older_people_and_cancer (accessed on 1 November 2017).
- Niederdeppe, J.; Hornik, R.C.; Kelly, B.J.; Frosch, D.L.; Romantan, A.; Stevens, A.; Barg, F.K.; Weiner, J.L.; Schwartz, J.S. Examining the dimensions of cancer-related information seeking and scanning behavior. Health Commun. 2007, 22, 153–167. [Google Scholar] [CrossRef] [PubMed]
- Kelly, B.J.; Niederdeppe, J.; Hornik, R.C. Validating measures of scanned information exposure in the context of cancer prevention and screening behaviors. J. Health Commun. 2009, 14, 721–740. [Google Scholar] [CrossRef] [PubMed]
- Kelly, B.; Hornik, R.; Romantan, A.; Schwartz, J.S.; Armstrong, K.; DeMichele, A.; Fishbein, M.; Gray, S.; Hull, S. Cancer information scanning and seeking in the general population. J. Health Commun. 2010, 15, 734–753. [Google Scholar] [CrossRef] [PubMed]
- Shim, M.; Kelly, B.; Hornik, R. Cancer information scanning and seeking behavior is associated with knowledge, lifestyle choices, and screening. J. Health Commun. 2006, 11, 157–172. [Google Scholar] [CrossRef] [PubMed]
- Miles, A.; Vorrwinden, S.; Chapman, S.; Wardle, J. Psychologic predictors of cancer information avoidance among older adults: The roles of cancer fear and fatalism. Cancer Epidem. Biomar. 2008, 17, 1872–1879. [Google Scholar] [CrossRef] [PubMed]
- Ford, B.M.; Kaphingst, K.A. Lay interpersonal sources for health information related to beliefs about the modifiability of cancer risk. Cancer Cause Control 2009, 20, 1975–1983. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.P.L.; Cheung, Y.W. Health and health care. In Indicators of Social Development; Lau, S., Lee, M., Wan, S., Wong, E., Eds.; Chinese University of Hong Kong: Hong Kong, China, 1995; pp. 59–112. [Google Scholar]
- Cheng, H.; Sit, J.W.H.; Twinn, S.F.; Cheng, K.K.F.; Thome, S. Coping with breast cancer survivorship in Chinese women: The role of fatalism or fatalistic voluntarism. Cancer Nurs. 2013, 36, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.Y.P.; Wong, E.M.L.; Ng, J.C.K.; Wong, T.K.S.; Chan, C.W.H. Measuring cancer fatalism in older Chinese adults: An application to colorectal cancer screening. In Proceedings of the 19th Annual Congress of Gerontology, Hong Kong, China, 24 November 2012. [Google Scholar]
- Kim, B.S.K.; Li, L.C.; Ng, G.F. The Asian American value scale-multidimensional: Development, reliability, and validity. Cult. Divers. Ethn. Min. 2005, 11, 187–201. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.Y. Online health information seeking behaviour in Hong Kong: An exploratory study. J. Med. Syst. 2010, 34, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Leung, L. Internet embeddedness: Links with online health information seeking, expectancy value/quality of health information websites, and internet usage patterns. CyberPsychol. Behav. 2008, 1, 565–569. [Google Scholar] [CrossRef] [PubMed]
- Tse, M.M.Y.; Choi, K.C.Y.; Leung, R.S.W. E-health for older people: The use of technology in health promotion. CyberPsychol. Behav. 2008, 11, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.; Ko, P.; Chan, K.S.; Chi, I.; Chow, N. Searching health information via the web: Hong Kong Chinese older adults’ experience. Public Health Nurs. 2007, 24, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.Y.M.; Leung, D.Y.P.; Cheung, M. Preference for online health information among Chinese. J. Health Mass Commun. 2011, 3, 46–60. [Google Scholar]
- Chiu, H.F.K.; Lee, H.C.; Chung, W.S.; Kwong, P.K. Reliability and validity of the Cantonese version of Mini-Mental State Examination: A preliminary study. J. Hong Kong Coll. Psychiatr. 1994, 4, 25–28. [Google Scholar]
- Shen, L.; Condit, C.M.; Wright, L. The psychometric property and validation of a fatalism scale. Psychol. Health 2009, 24, 597–613. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.Y.P.; Wong, E.M.L.; Ho, S.S.M.; Sit, J.W.H. Cancer fatalism in older Chinese adults: A validation study. Support. Care Cancer 2013, 21 (Suppl. 1), S224. [Google Scholar]
- Leung, D.Y.P. Psychometric properties of the 15-item Fatalism Scale in a Chinese older adult sample: A cross-validation study. In Proceedings of the 3rd International Conference on Social Science and Development in 2017, Qingdao, China, 16–17 December 2017. [Google Scholar]
- Chapman, V.L.; Skinner, C.S.; Menon, U.; Rawl, S.; Giesler, B.; Monahan, P.; Daggy, J. A Breast Cancer Scale: Psychometric development. J. Health Psychol. 2004, 9, 753–762. [Google Scholar]
- Leung, D.Y.P.; Wong, E.M.L.; Chan, C.W.H. Adapting Champion’s Breast Cancer Fear Scale to colorectal cancer: Psychometric testing in a sample of older Chinese adults. Eur. J. Oncol. Nurs. 2014, 18, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F. The Mini-Mental State Examination. In Assessment in Geriatric Psychopharmacology; Crook, T., Ferris, S., Bartus, R., Eds.; Mark Powley: New Canaan, CT, USA, 1983; pp. 50–51. [Google Scholar]
- Leung, D.Y.P.; Wong, E.M.L.; Chan, C.W.H. Determinants of participation in colorectal cancer screening among community-dwelling Chinese older people: Testing a comprehensive model using a descriptive correlational study. Eur. J. Oncol. Nurs. 2016, 21, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Heiniger, L.E.; Sherman, K.A.; Shaw, L.K.E.; Costa, D. Fatalism and health promoting behaviors in Chinese and Korean immigrants and Caucasians. J. Immigr. Minor. Health 2003, 17, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Jun, J.; Oh, K.M. Asian and Hispanic Americans’ cancer fatalism and colon cancer screening. Am. J. Health Behav. 2013, 37, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Powe, B.D.; Finnie, R. Cancer fatalism: The state of the science. Cancer Nurs. 2003, 26, 454–467. [Google Scholar] [CrossRef] [PubMed]
- Guessous, I.; Dash, C.; Lapin, P.; Doroshenk, M.; Smith, R.A.; Klabunde, C.N. Colorectal cancer screening barriers and facilitators in older persons. Prev. Med. 2010, 50, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Tran, P.; McComb, D. Internet access and health care information: A survey of the elderly. Gerontologist 2004, 44, 204. [Google Scholar]
- Census and Statistics Department. Thematic Household Survey Report No.52: Information Technology Usage and Penetration and Retirement Planning and the Financial Situation in Old Age; The Government of Hong Kong Special Administrative Region: Hong Kong, China, 2013.
- Wong, N.C.H. Interaction of comparative cancer risk and cancer efficacy perceptions on cancer-related information seeking and scanning behaviors. Commun. Res. Rep. 2012, 29, 193–203. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| n (%) | Mean ± SD | |
|---|---|---|
| Deomgraphic characteristics | ||
| Female | 135 (60.3) | |
| Married | 114 (50.9) | |
| Educational level | ||
| No formal education | 58 (25.9) | |
| Primary education | 95 (42.4) | |
| Secondary 1–Secondary 3 | 26 (11.6) | |
| Secondary 4–Secindary 5 | 24 (10.7) | |
| Secondary 6–Secondary 7 | 8 (3.6) | |
| Tertiary education | 12 (5.4) | |
| Above Tertiary education | 1 (0.4) | |
| No family member had cancer | 183 (81.7) | |
| Age | 77.2 ± 7.0 | |
| Numer of chronic diseases | 1.2 ± 1.2 | |
| Household income 1 | 1.6 ± 1.5 | |
| MMSE score | 26.4 ± 3.3 | |
| Fatalistic beliefs | 43.5 ± 11.3 | |
| Cancer fear | 19.7 ± 4.8 | |
| Outcome variables | ||
| Cancer-related information seeking behaviors | 68 (30.4) | |
| Cancer-related information scanning behaviors | 178 (79.5) |
| Model 1 Adjusted Odds Ratio (95% CI) | Model 2 Adjusted Odds Ratio (95% CI) | |
|---|---|---|
| Fatalistic beliefs | 0.40 (0.25–0.62) | 0.50 (0.30–0.84) |
| Cancer fear | 2.01 (1.18–3.43) | 1.76 (0.97–3.21) |
| Age | 0.97 (0.93–1.02) | |
| Female | 1.85 (0.85–4.04) | |
| Married | 2.24 (1.09–4.62) | |
| Educational level | 1.14 (0.87–1.50) | |
| Household income | 1.01 (0.81–1.27) | |
| No family member has cancer | 0.62 (0.27–1.41) | |
| Number of chronic diseases | 1.01 (0.76–1.35) | |
| MMSE score | 1.13 (1.00–1.28) | |
| Nagelkerke R2 | 0.124 | 0.253 |
| Model 1 Adjusted Odds Ratio (95% CI) | Model 2 Adjusted Odds Ratio (95% CI) | |
|---|---|---|
| Fatalistic beliefs | 0.74 (0.47–1.15) | 0.98 (0.57–1.68) |
| Cancer fear | 0.92 (0.52–1.61) | 0.76 (0.41–1.40) |
| Age | 0.98 (0.92–1.03) | |
| Female | 4.24 (1.77–10.12) | |
| Married | 1.28 (0.57–2.86) | |
| Educational level | 1.36 (0.93–2.00) | |
| Household income | 0.97 (0.68–1.37) | |
| No family member has cancer | 0.24 (0.06–0.94) | |
| Number of chronic diseases | 0.86 (0.63–1.18) | |
| MMSE score | 1.19 (1.05–1.34) | |
| Nagelkerke R2 | 0.015 | 0.233 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leung, D.Y.P.; Chow, T.T.; Wong, E.M.L. Cancer-Related Information Seeking and Scanning Behaviors among Older Chinese Adults: Examining the Roles of Fatalistic Beliefs and Fear. Geriatrics 2017, 2, 38. https://doi.org/10.3390/geriatrics2040038
Leung DYP, Chow TT, Wong EML. Cancer-Related Information Seeking and Scanning Behaviors among Older Chinese Adults: Examining the Roles of Fatalistic Beliefs and Fear. Geriatrics. 2017; 2(4):38. https://doi.org/10.3390/geriatrics2040038
Chicago/Turabian StyleLeung, Doris Y. P., Twiggy T. Chow, and Eliza M. L. Wong. 2017. "Cancer-Related Information Seeking and Scanning Behaviors among Older Chinese Adults: Examining the Roles of Fatalistic Beliefs and Fear" Geriatrics 2, no. 4: 38. https://doi.org/10.3390/geriatrics2040038