
Direct Oral Anticoagulants in Dental Patients Including the Frail Elderly Population

Abstract
:1. Introduction
2. The Evidence for Direct Oral Anticoagulants (DOAC)
3. Concerns with DOACs
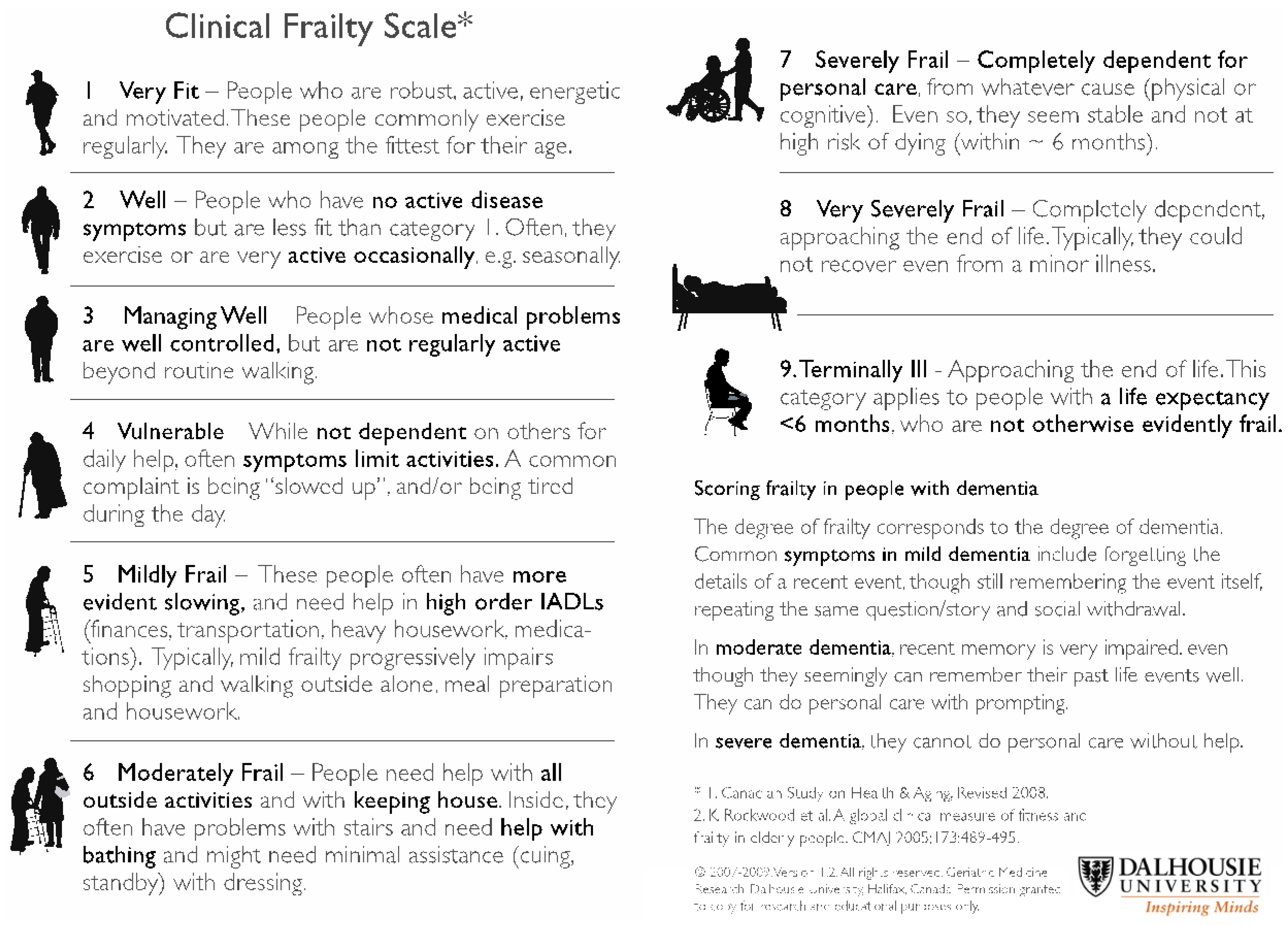
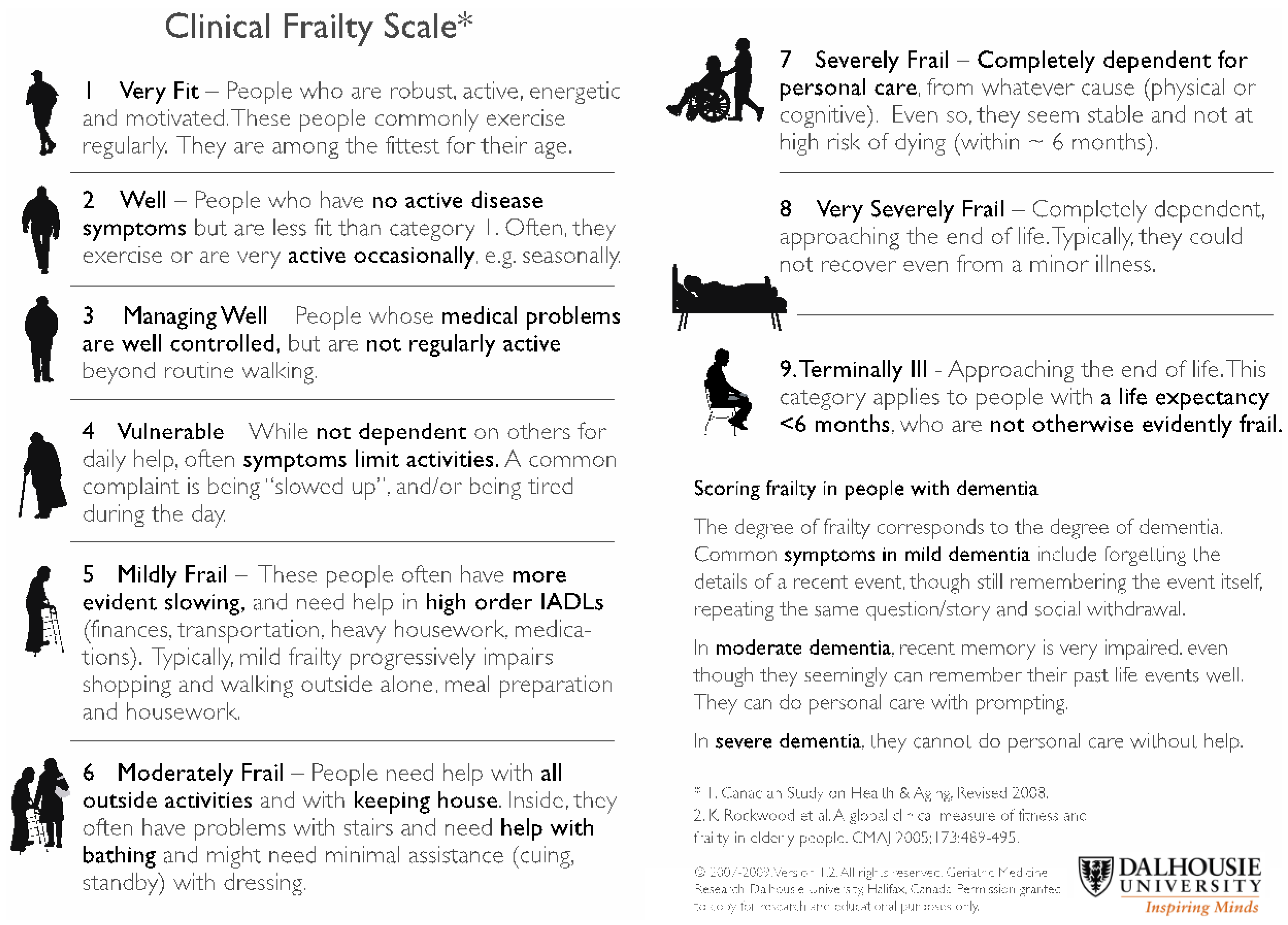
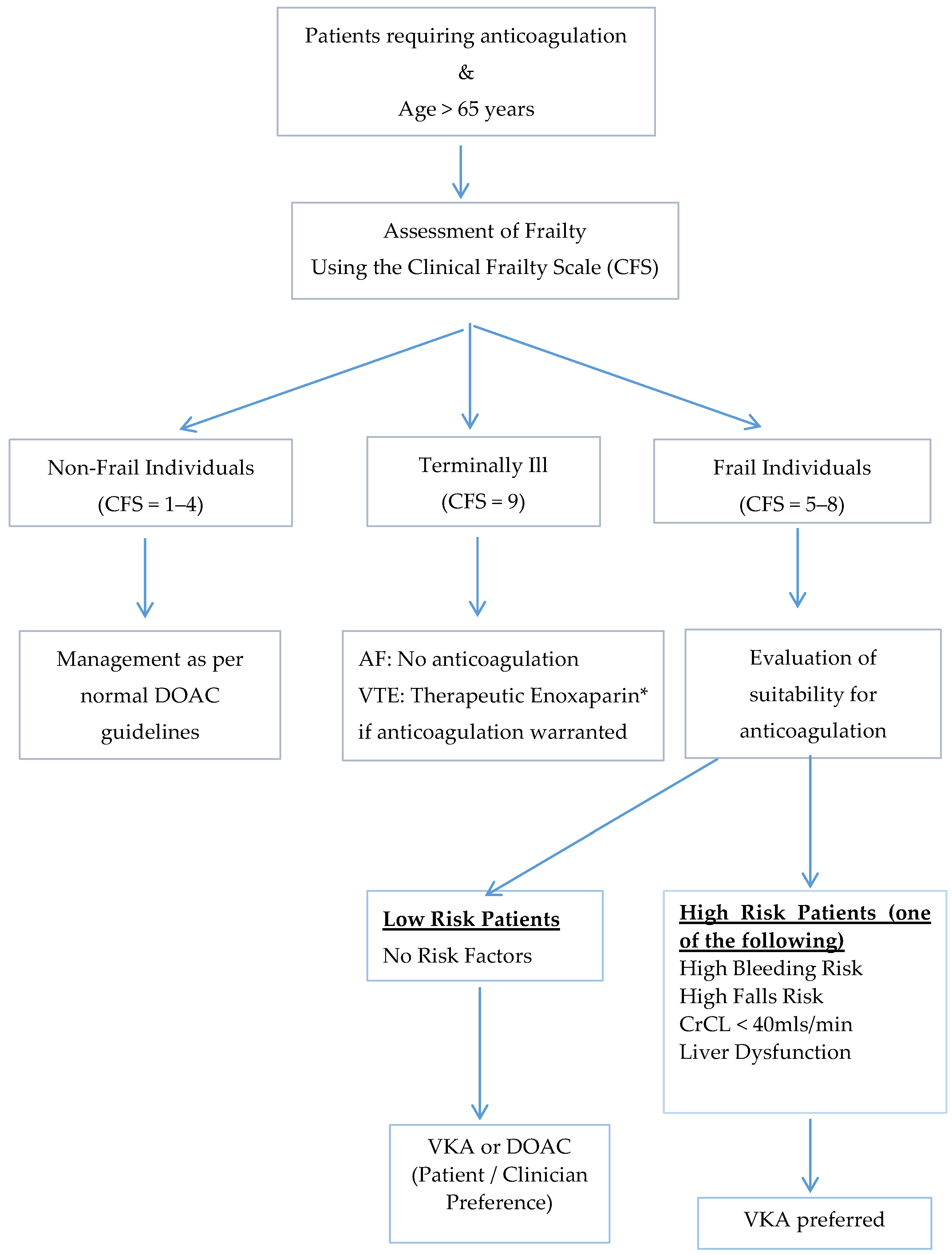
4. Use in Frail Elderly Patients
5. Approach to Decision-Making
6. Conclusions
Conflicts of Interest
References
- Fuster, V.; Rydén, L.E.; Cannom, D.S.; Crijns, H.J.; Curtis, A.B.; Ellenbogen, K.A.; Halperin, J.L.; Le Heuzey, J.Y.; Kay, G.N.; Lowe, J.E.; et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation—executive summary. Circulation 2006, 114, 700–752. [Google Scholar] [CrossRef] [PubMed]
- Wai Khoon, H.; Hankey, G.; Eikelboom, G.J.; Eikelboom, J.W. The incidence of venous thromboembolism: A prospective, community-based study in Perth, Western Australia. Med. J. Aust. 2008, 189, 144–147. [Google Scholar]
- Breithardt, G.; Baumgartner, H.; Berkowitz, S.D.; Hellkamp, A.S.; Piccini, J.P.; Stevens, S.R.; Lokhnygina, Y.; Patel, M.R.; Halperin, J.L.; Singer, D.E.; et al. Clinical characteristics and outcomes with rivaroxaban vs. warfarin in patients with nonvalvular atrial fibrillation but underlying native mitral and aortic valve disease participating in the ROCKET AF trial. Eur. Heart J. 2014, 35, 3377–3385. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.J.; Wallentin, L.; Ezekowitz, M.D.; Eikelboom, J.; Oldgren, J.; Reilly, P.A.; Brueckmann, M.; Pogue, J.; Alings, M.; Amerena, J.V.; et al. The Long-Term Multicenter Observational Study of Dabigatran Treatment in Patients With Atrial Fibrillation (RELY-ABLE) Study. Circulation 2013, 128, 237–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granger, C.B.; Lopes, R.D.; Hanna, M.; Ansell, J.; Hylek, E.M.; Alexander, J.H.; Thomas, L.; Wang, J.; Bahit, M.C.; Verheugt, F.; et al. Clinical events after transitioning from apixaban versus warfarin to warfarin at the end of the Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) trial. Am. Heart J. 2015, 169, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Agnelli, G.; Buller, H.R.; Cohen, A.; Curto, M.; Gallus, A.S.; Johnson, M.; Masiukiewicz, U.; Pak, R.; Thompson, J.; Raskob, G.E.; et al. Oral apixaban for the treatment of acute venous thromboembolism. New Engl. J. Med. 2013, 369, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Prins, M.H.; Lensing, A.W.; Bauersachs, R.; van Bellen, B.; Bounameaux, H.; Brighton, T.A.; Cohen, A.T.; Davidson, B.L.; Decousus, H.; Raskob, G.E.; et al. Oral rivaroxaban versus standard therapy for the treatment of symptomatic venous thromboembolism: A pooled analysis of the EINSTEIN-DVT and PE randomized studies. Thromb. J. 2013, 11, 21. [Google Scholar] [CrossRef] [PubMed]
- Fang, M.C.; Chang, Y.; Hylek, E.M.; Rosand, J.; Greenberg, S.M.; Go, A.S.; Singer, D.E. Advanced age, anticoagulation intensity, and risk for intracranial hemorrhage among patients taking warfarin for atrial fibrillation. Annals Intern. Med. 2004, 141, 745–752. [Google Scholar] [CrossRef]
- Hylek, E.M.; Evans-Molina, C.; Shea, C.; Henault, L.E.; Regan, S. Major hemorrhage and tolerability of warfarin in the first year of therapy among elderly patients with atrial fibrillation. Circulation 2007, 115, 2689–2696. [Google Scholar] [CrossRef] [PubMed]
- Kitchen, S.; Gray, E.; Mackie, I.; Baglin, T.; Makris, M. Measurement of non-coumarin anticoagulants and their effects on tests of Haemostasis: Guidance from the British Committee for Standards in Haematology. Br. J. Haematol. 2014, 166, 830–841. [Google Scholar] [CrossRef] [PubMed]
- Van Diermen, D.E.; van der Waal, I.; Hoogstraten, J. Management recommendations for invasive dental treatment in patients using oral antithrombotic medication, including novel oral anticoagulants. Oral surg. oral med. oral pathol. oral radiol. 2013, 116, 709–716. [Google Scholar] [CrossRef] [PubMed]
- New oral anticoagulants (NOACs) and management of dental patients—Dabigatran, rivaroxaban and apixaban. Available online: http://www.eryldc.co.uk/download/i/mark_dl/u/4012071383/4615740784/New_oral_anticoagulants_and_management_of_dental_patients_-_distribution__(Nov_2.pdf (accessed on 12 November 2015).
- UC Davis Health System anticoagulation services recommendations for anticoagulation management before and after dental procedure. Available online: http://www.ucdmc.ucdavis.edu/anticoag/links_and_resources.html (accessed on 12 November 2015).
- Ruff, C.T.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B.; Deenadayalu, N.; Ezekowitz, M.D.; Camm, A.J.; Weitz, J.I.; Lewis, B.S.; Parkhomenko, A.; et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A metaanalysis of randomised trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef]
- Capodanno, D.; Capranzano, P.; Giacchi, G.; Calvi, V.; Tamburino, C. Novel oral anticoagulants versus warfarin in non-valvular atrial fibrillation: A meta-analysis of 50,578 patients. Int. J. Cardiol. 2013, 167, 1237–1241. [Google Scholar] [CrossRef] [PubMed]
- Hankey, G.J. Intracranial hemorrhage and novel anticoagulants for atrial fibrillation: What have we learned? Curr. Cardiol. Rep. 2014, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Pokorney, S.D.; Simon, D.N.; Thomas, L.; Fonarow, G.C.; Kowey, P.R.; Chang, P.; Singer, D.E.; Ansell, J.; Blanco, R.G.; Gersh, B.; et al. Patients’ time in therapeutic range on warfarin among US patients with atrial fibrillation: Results from ORBIT-AF registry. Am. Heart J. 2015, 170, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Bauer, K.A. Recent progress in anticoagulant therapy: Oral direct inhibitors of thrombin and factor Xa. J. Thromb. Haemost. 2011, 9, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Tran, H.; Joseph, J.; Young, L.; McRae, S.; Curnow, J.; Nandurkar, H.; Wood, P.; McLintock, C. New oral anticoagulants: A practical guide on prescription, laboratory testing and peri-procedural/bleeding management. Intern. Med. J. 2014, 44, 525–536. [Google Scholar] [CrossRef] [PubMed]
- Dale, B.J.; Chan, N.C.; Eikelboom, J.W. Laboratory measurement of the direct oral anticoagulants. Br. J. Haematol. 2016, 172, 315–536. [Google Scholar] [CrossRef] [PubMed]
- Pollack, C.V., Jr.; Reilly, P.A.; Eikelboom, J.; Glund, S.; Verhamme, P.; Bernstein, R.A.; Dubiel, R.; Huisman, M.V.; Hylek, E.M.; Kamphuisen, P.W.; et al. Idarucizumab for Dabigatran Reversal. New Engl. J. Med. 2015, 373, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Siegal, D.M.; Curnutte, J.T.; Connolly, S.J.; Lu, G.; Conley, P.B.; Wiens, B.L.; Mathur, V.S.; Castillo, J.; Brons, M.D.; Leeds, J.M.; et al. Andexanet Alfa for the Reversal of Factor Xa Inhibitor Activity. New Engl. J. Med. 2015, 373, 2413–2414. [Google Scholar] [CrossRef] [PubMed]
- Douxfils, J.; Mullier, F.; Robert, S.; Chatelain, C.; Chatelain, B.; Dogne, J.M. Impact of dabigatran on a large panel of routine or specific coagulation assays. Thromb. Haemost. 2012, 107, 985–997. [Google Scholar] [CrossRef] [PubMed]
- Lessire, S.; Douxfils, J.; Baudar, J.; Bailly, N.; Dincq, A.S.; Gourdin, M.; Dogné, J.M.; Chatelain, B.; Mullier, F. Is Thrombin Time useful for the assessment of dabigatran concentrations? An in vitro and ex vivo study. Thromb. Res. 2015, 136, 693–696. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.H.; Ageno, W.; Chan, N.C.; Crowther, M.; Verhamme, P.; Weitz, J.I. When and how to use antidotes for the reversal of direct oral anticoagulants: Guidance from the SSC of the ISTH. J. Thromb. Haemost. 2015, in press. [Google Scholar] [CrossRef] [PubMed]
- Eikelboom, J.W.; Quinlan, D.J.; van Ryn, J.; Weitz, J.I. Idarucizumab The Antidote for Reversal of Dabigatran. Circulation 2015, 132, 2412–2422. [Google Scholar] [CrossRef] [PubMed]
- Harenberg, J.; Erdle, S.; Marx, S.; Kramer, R. Determination of rivaroxaban in human plasma samples. Semin. Thromb. Hemost. 2012, 38, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Douxfils, J.; Chatelain, C.; Chatelain, B.; Dogne, J.M.; Mullier, F. Impact of apixaban on routine and specific coagulation assays: A practical laboratory guide. Thromb. Haemost. 2013, 110, 283–294. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Kim, J.Y.; Mun, H.S.; Lee, H.Y.; Roh, Y.H.; Uhm, J.S.; Pak, H.N.; Lee, M.H.; Joung, B. Heparin bridging in warfarin anticoagulation therapy initiation could increase bleeding in non-valvular atrial fibrillation patients: A multicenter propensity-matched analysis. J. Thromb. Haemost. 2015, 13, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Douketis, J.D.; Spyropoulos, A.; Kaatz, S.; Becker, R.C.; Caprini, J.A.; Dunn, A.S.; Garcia, D.A.; Jacobson, A.; Jaffer, A.K.; Kong, D.F.; et al. Perioperative bridging anticoagulation in patients with atrial fibrillation. New Engl. J. Med. 2015, 373, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Brotman, D.J.; Streiff, M.B. Overuse of bridging anticoagulation for patients with venous thromboembolism: First, do no harm. JAMA Intern. Med. 2015, 175, 1169–1170. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, B.A.; Peterson, E.D.; Kim, S.; Thomas, L.; Gersh, B.J.; Fonarow, G.C.; Kowey, P.R.; Mahaffey, K.W.; Sherwood, M.W.; Chang, P.; et al. Use and outcomes associated with bridging during anticoagulation interruptions in patients with atrial fibrillation: Findings from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF). Circulation 2015, 131, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Pather, M. The prevalence of renal impairment in the elderly hospitalized population. Int. J. Gen. Med. 2009, 2, 117–119. [Google Scholar] [CrossRef] [PubMed]
- Heidbuchel, H.; Verhamme, P.; Alings, M.; Antz, M.; Diener, H.C.; Hacke, W.; Oldgren, J.; Sinnaeve, P.; Camm, A.J.; Kirchhof, P. European Heart Rhythm Association Practical Guide on the use of new oral anticoagulants in patients with non-valvular atrial fibrillation. Eurospace 2013, 15, 625–651. [Google Scholar] [CrossRef] [PubMed]
- Ho, P.; La Brooy, B.; Hayes, L.; Lim, W.K. Direct oral anticoagulants in frail older adults: A geriatric perspective. Semin. Thromb. Hemost. 2015, 41, 389–394. [Google Scholar] [PubMed]
- Sabate, E. (Ed.) Adherence to Long-Term Therapies: Evidence for Action; World Health Organization (WHO): Geneva, Switzerland, 2003. Available online: http://apps.who.int/medicinedocs/en/d/Js4883e/ (accessed on 1 December 2015).
- Osterberg, L.; Blaschke, T. Adherence to medication. New Engl. J. Med. 2005, 535, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Alberio, L. The new direct oral anticoagulants in special indications: Rationale and preliminary data in cancer, mechanical heart valves, anti-phospholipid syndrome, and heparin-induced thrombocytopenia and beyond. Semin. Hematol. 2014, 51, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Eikelboom, J.W.; Connolly, S.J.; Brueckmann, M.; Granger, C.B.; Kappetein, A.P.; Mack, M.J.; Blatchford, J.; Devenny, K.; Friedman, J.; Guiver, K.; et al. Dabigatran versus Warfarin in Patients with Mechanical Heart Valves. New Engl. J. Med. 2013, 369, 1206–1214. [Google Scholar] [CrossRef] [PubMed]
- La Brooy, B.; Ho, P. New oral anticoagulants: An approach in older people. J. Pharm. Pract. Res. 2015, 45, 217–225. [Google Scholar] [CrossRef]
- Sardar, P.; Chartterjee, S.; Chaudhari, S.; Lip, G.Y.H. New oral anticoagulants in elderly adults: Evidence from a meta-analysis of randomized trials. J. Am. Geriatr. Soc. 2014, 62, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Australian and New Zealand Society of Geriatric Medicine. Position Statement No. 6—Under-Nutrition and the Older Person. Australas. J. Ageing 2009, 28, 99–105. [Google Scholar]
- Robert-Ebadi, H.; Righini, M. Anticoagulation in elderly. Pharmaceuticals 2010, 3, 3543–3569. [Google Scholar] [CrossRef]
- Coresh, J.; Selvin, E.; Stevens, L.A.; Manzi, J.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Levey, A.S. Prevalence of chronic kidney disease in the United States. JAMA 2007, 298, 2038–2047. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in the elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Lane, D.A.; Lip, G.Y. Use of the CHA(2)DS(2)-VASc and HAS-BLED scores to aid decision making for thromboprophylaxis in non-valvular atrial fibrillation. Circulation 2012, 126, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Rider, O.J.; Rider, E.B. The changing face of oral anticoagulants. Br. Dent. J. 2013, 215, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Thean, D.; Alberghini, M. Anticoagulant therapy and its impact on dental patients: A review. Aust. Dent. J. 2015, in press. [Google Scholar] [CrossRef] [PubMed]
- Nematullah, A.; Alabousi, A.; Blanas, N.; Douketis, J.; Sutherland, S. Dental surgery for patients on anticoagulant therapy with warfarin: A systematic review and meta-analysis. J. Can. Dent. Assoc. 2009, 75, 41–41i. [Google Scholar] [PubMed]
- Perry, D.J.; Noakes, T.C.; Helliwell, P.S. Guidelines for the management of patients on oral anticoagulants requiring dental surgery. Br. Dent. J. 2007, 203, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Dinkova, A.; Kirova, D.; Delev, D. Management of patients on anticoagulant therapy undergoing dental procedures. J. IMAB 2013, 19, 321–326. [Google Scholar]
- Anticoagulant and Antiplatelet Medications and Dental Procedures. Available online: http://www.ada.org/en/member-center/oral-health-topics/anticoagulant-antiplatelet-medications-and-dental- (accessed on 12 November 2015).
- Elad, S.; Marshall, J.; Meyerowitz, C.; Connolly, G. Novel anticoagulants: General overview and practical considerations for dental practitioners. Oral Dis. 2016, 22, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Van Ryn, J.; Stangier, J.; Haertter, S.; Liesenfeld, K.H.; Wienen, W.; Feuring, M.; Clemens, A. Dabigatran etexilate—A novel, reversible, oral direct thrombin inhibitor: Interpretation of coagulation assays and reversal of anticoagulation activity. Thromb. Haemost. 2010, 103, 1116–1127. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Dabigatran | Rivaroxaban | Apixaban | |
|---|---|---|---|
| Mechanism of action | Direct thrombin inhibitor | Direct factor Xa inhibitor | Direct factor Xa inhibitor |
| Time to peak plasma concentration (in healthy adults) | 2 h | 2.5–4 h | 1–3 h |
| Half-life (in healthy adults) | 12–17 h | 7–13 h | 8–15 h |
| Elimination | Renal 80%, hepatic 20% | Renal 33%, renal metabolite 33%, hepatic 33% | Renal 25%, hepatic 75% |
| Indication | Stroke prevention in non-valvular AF | Stroke prevention in non-valvular AF VTE prophylaxis and treatment | Stroke prevention in non-valvular AF VTE prophylaxis and treatment |
| Dosing regimen | Twice daily | Once daily | Twice daily |
| Potential drug interactions | Potent P-glycoprotein (P-gp) inhibitors and P-gp inducers | Strong dual CYP 3A4 and P-gp inhibitors/inducers | Strong dual CYP 3A4 and P-gp inhibitors/inducers |
| Recommended laboratory tests: | |||
| Significant anticoagulant effect unlikely | APTT is normal, Thrombin time (TT) is more sensitive than APTT and a normal TT results suggests low dabigatran level or absent drug | PT normal | Normal APTT and PT cannot be used to exclude anticoagulant effect. |
| Anticoagulant effect present (screening test) | TT prolonged; APTT prolonged | PT normal/prolonged | PT prolonged—apixaban likely present in excess. PT is only weakly sensitive to apixaban with inter-reagent variability and a normal PT does not rule out the presence of anticoagulant effect |
| Drug effect likely (confirmatory tests) | Dilute thrombin clotting time assay (HEMOCLOT) prolonged Ecarin clot time (ECA) Anti FIIa (chromogenic assay) | Modified specific anti-Xa positive | Modified specific anti-Xa positive |
| Antidote | Idarucuzimab [21] (approved by US FDA on 16 October 2015) | Andexanet alfa [22] (Phase III trial) | Andexanet alfa [22] (Phase III trial) |
| Dental Procedure | Presumed Bleeding Risk | Peri-Procedural Recommendations |
|---|---|---|
| Supragingival scaling Simple restorations Local anaesthetic injections | Low | Continue therapeutic anticoagulation |
| Subgingival scaling Subgingival preparation restoration Standard root canal Simple extractions Regional anaesthetic injections | Moderate | Continue therapeutic anticoagulation |
| Extensive surgery Apicoectomy (root removal) Alevolar surgery (bone removal) | High | Consider reducing anticoagulation |
| Drug | Renal Function | Low Bleeding Risk Surgery | High Bleeding Risk Surgery |
|---|---|---|---|
| Dabigatran | CrCl ≥ 50 mL/min | Last dose: 24 h before surgery | Last dose: 48–72 h before surgery |
| CrCl 30–49 mL/min | Last dose: 48–72 h before surgery | Last dose: 96 h before surgery | |
| CrCl < 30 mL/min* | Last dose: 48–120 h before surgery | Last dose: ≥ 120 h before surgery | |
| Rivaroxaban/Apixaban | CrCl ≥ 50 mL/min | Last dose: 24 h before surgery | Last dose: 48–72 h before surgery |
| CrCl 30–49 mL/min | Last dose: 48 h before surgery | Last dose: 72 h before surgery | |
| CrCl < 30 mL/min* | Last dose: 48 h before surgery | Last dose: 72 h before surgery |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, H.Y.; Ho, P. Direct Oral Anticoagulants in Dental Patients Including the Frail Elderly Population. Dent. J. 2016, 4, 7. https://doi.org/10.3390/dj4010007
Lim HY, Ho P. Direct Oral Anticoagulants in Dental Patients Including the Frail Elderly Population. Dentistry Journal. 2016; 4(1):7. https://doi.org/10.3390/dj4010007
Chicago/Turabian StyleLim, Hui Yin, and Prahlad Ho. 2016. "Direct Oral Anticoagulants in Dental Patients Including the Frail Elderly Population" Dentistry Journal 4, no. 1: 7. https://doi.org/10.3390/dj4010007