A Classic Herbal Formula Guizhi Fuling Wan for Menopausal Hot Flushes: From Experimental Findings to Clinical Applications


1
School of Health and Biomedical Sciences, RMIT University, Bundoora, VIC 3083, Australia
2
School of Science, RMIT University, Melbourne, VIC 3001, Australia
*
Author to whom correspondence should be addressed.
Biomedicines 2019, 7(3), 60; https://doi.org/10.3390/biomedicines7030060
Submission received: 30 June 2019
/
Revised: 10 August 2019
/
Accepted: 15 August 2019
/
Published: 18 August 2019
(This article belongs to the Section Drug Discovery and Development)
Abstract
:A classic herbal formula Guizhi Fuling Wan (GFW) has been used for managing menopausal hot flushes (MHFs), but the evidence across different study types has not been systematically summarized. This project investigated the clinical effects, phytochemistry, pharmacodynamics, and potential mechanisms of actions of GFW on the causative target proteins potentially driving MHFs. Twenty English and Chinese databases were searched for relevant clinical and experimental studies. A total of 12,988 studies were identified, of which 46 were included. Seven clinical studies demonstrated GFW had no statistically significant changes in the frequency and severity of MHFs; however, it could improve peripheral blood flow in the fingertips, jaw, and toes. Thirty-five studies on phytochemistry identified 169 chemical compounds of GFW. Four experimental studies revealed GFW’s therapeutic effects (e.g., normalize calcitonin gene-related peptide (CGRP) level) and potential target protein/cytokine (estrogen receptor beta (ESR2) with genetic variation, CGRP receptor, and interleukin-8) on MHFs. Therapeutic effects across different study types were inconsistent, possibly due to the dose difference and genotype variety of ESR2 in the human population. Further clinical and experimental studies, as well as biochemical investigation on the mechanisms of actions of GFW, are recommended.
1. Introduction
A menopausal hot flush (MHF) is a sudden and transient onset of erythema and warmth or burning sensation on the face and skin of the neck which appears during the transition to (pre-menopausal and peri-menopausal), and through, menopause (menopausal and post-menopausal) [1,2]. The onset commonly lasts for seconds to five minutes, but its persistence duration is unpredictable [3]. MHFs significantly impact the quality of life of both the sufferers and their families [3]. Its mechanism has not been fully investigated. The sudden reduction in estrogen level, the narrowed central thermoneutral zone, changes of the certain neurotransmitter synthesis (e.g., noradrenaline and serotonin), and peripheral vascular reactivity are linked to MHF onset [4,5,6,7,8,9]. Menopausal hormone therapy is the most popular and effective MHF management [10,11]. However, adverse effects, such as nausea, dizziness, dry mouth, and contraindication, with hormone-dependent diseases (e.g., breast cancer) exist [12]. Thus, more than half of all middle-aged menopausal women have taken non-hormonal therapies [13], such as Chinese herbal medicine (CHM).
Guizhi Fuling Wan (GFW, also known as Keishibukuryogan) is a classic Chinese herbal formula that has been used for MHFs in modern clinical practice [14,15]. In ancient China, there was no specific terminology used for MHFs. One Classic book, Ying Er Lun (Treatise on Infants), advocated that GFW could be used to treat flushed complexion in females of which the description is similar to MHF symptoms. As recorded in Jin Gui Yao Lue Fang Lun (Synopsis of Prescriptions of the Golden Chamber) [16], GFW consists of five herbal ingredients, including Gui Zhi (Cinnamomi Ramulus), Shao Yao (Paeoniae Radix Alba or Paeoniae Radix Rubra), Mu Dan Pi (Moutan Cortex), Tao Ren (Persicae Semen), and Fu Ling (Poria) [16]. The 2015 edition of the Chinese Pharmacopeia indicates that Bai Shao (Paeoniae Radix Alba) is used in tablet and capsule form GFW, whereas Chi Shao (Paeoniae Radix Rubra) is used in honey pill form [17]. In 2006, a GFW product (capsule) was approved by the US Food and Drug Administration to enter Phase II clinical trials [18]. Recently, more experimental studies have been conducted to investigate the pharmacodynamic effects of GFW [19,20,21]. However, GFW’s application and mechanisms of actions on MHFs have not been systematically reviewed. This paper investigated the therapeutic effects of GFW on the management of MHFs from clinical and experimental perspectives.
2. Clinical Application of GFW on MHFs
The formula name and its synonyms were searched as keywords in 20 electronic databases (Cochrane Library, PubMed, EMBASE, AMED, CINAHL, Informit, Science Direct, LILACS, ProQuest, Wiley Online Library, PsycINFO, IndMED, AcuBriefs, Ingenta, KoreaMed, ERIC, CNKI, CQVIP, Wanfang Data, and sinoMed) for English or Chinese language papers from the earliest records available in each database, up to April 2019. The reference lists of articles with relevant topics were manually screened to identify potentially relevant studies. After removal of duplicates, the titles and abstracts of identified potential studies were screened. Full-texts were obtained for eligibility assessment against the selection criteria. All types of clinical studies (including randomized controlled trials (RCTs), non-randomized parallel controlled studies, and case series) were considered for inclusion as long as they recruited patients with MHFs or used MHFs as one of the outcome measures. To ensure comparability of the intervention, only studies using GFW in non-modified forms (e.g., decoction, pills, granules, and capsules with acceptable variations of Bai Shao/Chi Shao/Shao Yao) were considered. For studies involving control groups, only those that compared GFW with placebo, no treatment, or conventional medicine were considered. Studies utilizing any co-interventions were excluded.
A predesigned form was used to record extracted data, including study design, setting, sample size, the age, and diagnosis of the participants, intervention, duration, and outcome measures (including frequency and severity of MHFs, level of hormones/cytokines, and peripheral blood flow). Corresponding authors of potential articles were contacted by email, Research Gate (www.researchgate.net), and LinkedIn (www.linkedin.com) for missing data. Replies with unpublished data were received from corresponding authors of two papers [22,23]. The quality of included studies was analyzed according to study types. For RCTs, the quality was assessed using Cochrane’s risk of bias assessment tool [24] with focus on the following domains: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), and selective reporting (reporting bias). Quality was categorized as “Low risk”, “Unclear risk”, and “High risk” of bias. The quality of parallel controlled studies was evaluated by ROBINS-I (“Risk Of Bias In Non-randomised Studies - of Interventions”) [25], and the assessed domains included confounding, participant selection, intervention classification, deviations from intended interventions, missing data, outcome measurement, and reported results. Quality was classified as “Low risk”, “Moderate risk”, “Serious risk”, and “Critical risk” of bias. The quality of case series was assessed in four domains according to the Instrument for Evaluating the Quality of case series in CHM, including study aims and design (two questions), descriptions of treatment protocol (three questions), descriptions of methods and therapeutic/side-effects (two questions), and conduct of the study (six questions) [26]. A score of “1” was given when ‘Yes’ was applied to one item. Any article with a total score ≥ 7 was considered to have good quality.
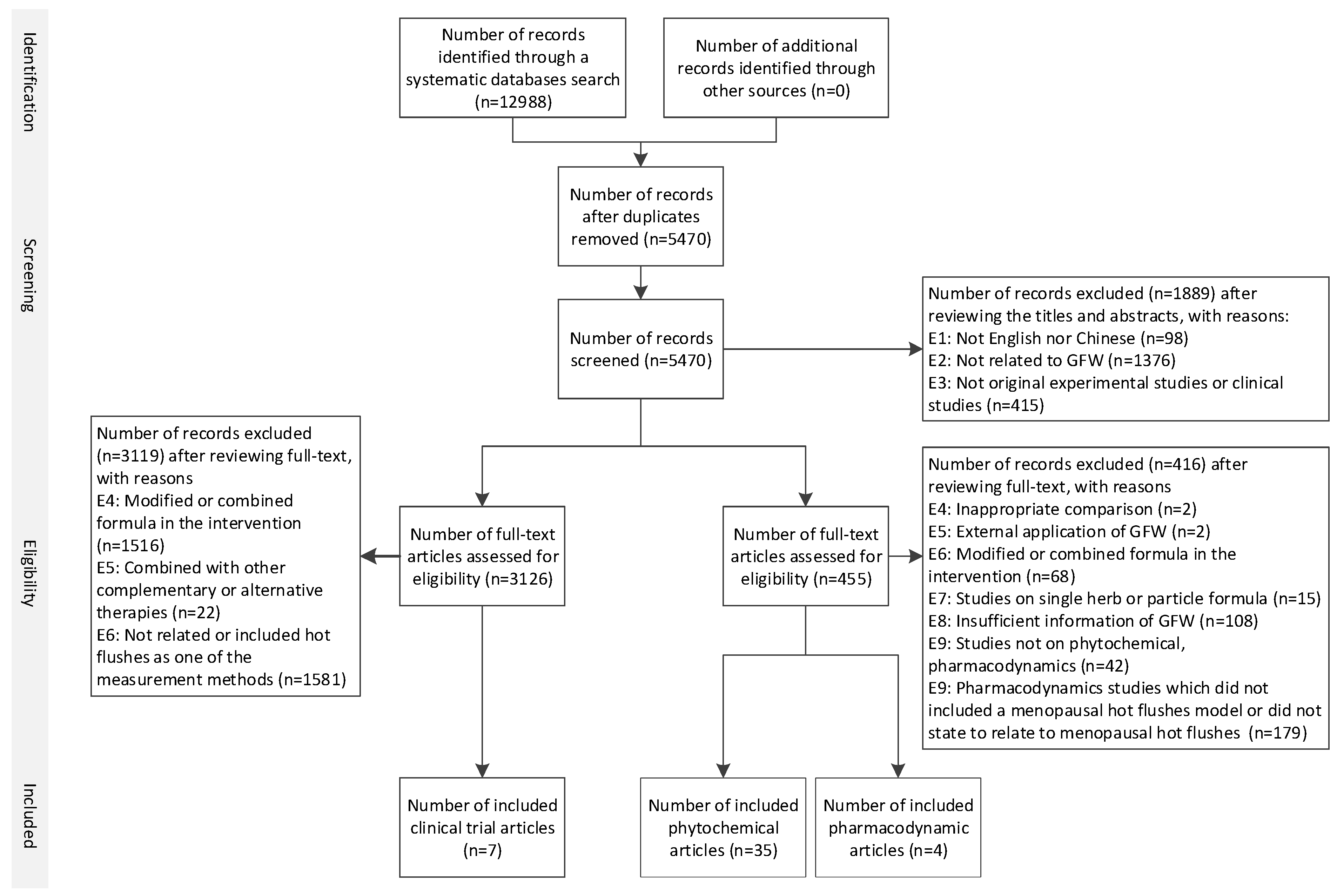
A total of 12988 records were identified, and seven of them met the inclusion criteria. Figure 1 illustrates the selection process of the included studies. Two RCTs [14,15], one parallel controlled study [27], and two case series [28,29] were included in this review. Another two studies [22,23] were claimed as controlled trials; however, two intervention groups were incomparable. Thus, the treatment groups of these two studies were considered as case series studies, and only data from GFW groups were extracted for analyses in this review. The characteristics of the included studies are summarized in Table 1.
2.1. RCTs
One RCT [15] reported that both low dosage (7.5 g/day) and high dosage (12.5 g/day) GFW could significantly reduce MHF frequency and severity when comparing between before and after the 12-week intervention. When compared to placebo, there was no statistical significance. However, the reduction may be dose-dependent, as the results from the high dosage group demonstrated a greater reduction, which provided a direction for future research on the relationship between GFW dosage and clinical effects. Another RCT [14] reported that the peripheral blood flow in postmenopausal females with MHFs in the GFW group (n = 67) was significantly decreased compared to the menopausal hormone therapy group (n = 64) under the jaw (mean difference (MD) –3.56, 95% confidence interval (CI) –5.17 to –1.95) and in the middle fingertip (MD –7.10, 95% CI –10.99 to –3.21) at the end of one-month treatment. Opposite effects on the blood flow in the third toe were observed in two groups: GFW increased the blood flow in the toe, whereas menopausal hormone therapy caused a decrease.
2.2. Parallel Controlled Study
The parallel controlled study [27] reported positive results, concluding that the severity of MHFs in 73.7% of the participants improved from severe to mild or moderate after six-month GFW intake. It was significantly higher than the control group. No significant difference in estradiol (E2) and follicle-stimulating hormone (FSH) levels was observed between groups. Results of serum cytokine level indicated that serum monocyte chemotactic protein-1 (MCP-1) level in women treated with keishibukuryogan decreased significantly (–16.3%) compared to the no treatment group (3.8%). Further analysis of the GFW responder group (n = 28) indicated that concentrations of serum interleukin (IL)-8 and macrophage inflammatory protein (MIP)-1β were reduced significantly, whereas those in the non-responders were increased dramatically. Sub analysis results on menopausal transition status showed that GFW decreased the IL-8 and MIP-1β levels in perimenopausal GFW responders and MCP-1 in postmenopausal GFW responders.
2.3. Case Series
One case series study [29] revealed that the improvement of MHF severity was related to genetic variation of the polymorphic dinucleotide (CA) repeat of the estrogen receptor beta (ESR2) gene on chromosome 14, which include three types: two short alleles (SS), two long alleles (LL), and a short and long allele (SL) [30,31]. MHF severity in participants with LL genotype improved significantly after the intervention. FSH level changes also depended on genotype: FSH levels decreased in participants with SS genotype but increased in participants with SL or LL genotypes. E2 level decreased in all genotype groups. Another case series [28] reported that the plasma calcitonin gene-related peptide (CGRP) level in eight post-menopausal participants significantly decreased after the four-week GFW intervention when compared to baseline data (MD –2.88, 95% Cl –4.07 to –1.69). CGRP is a potent vasodilator neuropeptide, and it is hypothesized to be a specific vasodilation neuropeptide of MHFs, which significantly rose in concentration during MHF onset [32]. However, GFW’s effects on changes of frequency before and after intervention in three case series had no statistically significant difference (standardized mean difference (SMD) –1.15, 95% CI –2.49 to 0.20) [22,23,28].
3. Experimental Studies on Phytochemistry and Pharmacodynamics of GFW on MHFs
We searched the 20 English and Chinese databases, detailed in Section 2, to identify experimental studies that have investigated the chemical compounds of GFW. Studies were excluded if they did not provide the following details: (1) plants with valid plant specimen voucher numbers, ingredients and ratios for raw herbs (decoction), or (2) company names and batch/lot numbers for purchased patent products (pills, granules, or capsules).
For pharmacodynamics, the same set of 20 databases was searched to identify experimental studies that have investigated GFW on MHFs. To be eligible to be included, the studies must provide the details as specified in (1) and (2) as above. Also, experiments were required to have (3) utilized cell or animal models related to MHFs; (4) compared GFW’s effects with the blank model control group (i.e., no treatment); (5) evaluated the pharmacodynamic effects on MHFs. Studies involving any co-interventions were excluded.
The structures of chemical compounds were drawn using BIOVIA Draw 2019 [33] or Avogadro [34]/Discovery Studio Visualizer 2019 [35]. Molecular weight was calculated by Lenntech Molecular Weight Calculator (https://www.lenntech.com/calculators/molecular/molecular-weight-calculator.htm). The quality of in vivo studies was assessed based on 20 domains specified in the Animal Research: Reporting of In Vivo Experiments (ARRIVE) guidelines [36].
As a result, 35 studies on phytochemistry, and four studies on pharmacodynamics met the inclusion criteria. Figure 1 illustrates the selection process of the included studies.
3.1. Phytochemistry of GFW
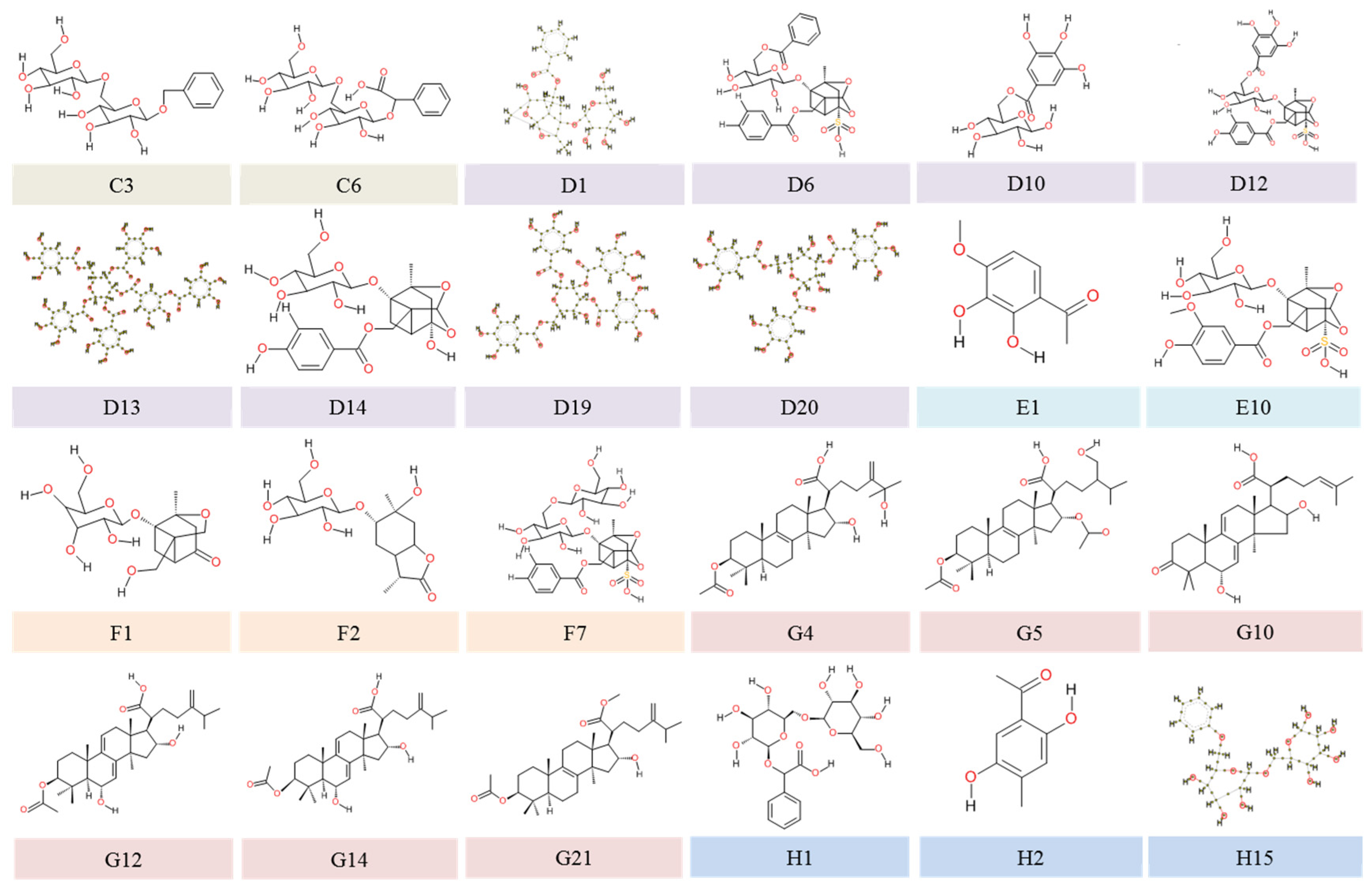
The included studies on phytochemicals from GFW reported 169 compounds: four from Cinnamomi Ramulus (A1 and B1–B3), 13 from Persicae Semen (A1 and C1–C12), 41 from Moutan Cortex (A1, D1–D20, and E1–E20), 31 from Paeoniae Radix (A1, D1–D20, and F1–F10), 31 from Poria (A1 and G1–G30), 44 without clearly defined resources (H1–H44), and 29 inorganic elements. Table 2 outlines the characteristics of chemical constituents isolated from GFW. The molecular structures of 144 phytochemicals could be identified with their corresponding PubChem CIDs (compound identification number)/SIDs (substance identification number), whereas 25 constituents were not available in the PubChem database. Among those 25 chemical components, structures of 23 phytochemicals (C3, C6, D1, D6, D10, D12, D13, D14, D19, D20, E1, E10, F1, F2, F7, G4, G5, G12, G14, G21, H1, H2, H15) were provided in the included studies. One compound structure (G10) was available in a reference paper (as cited in Table 2), whereas one (G11) could not be found in any known data source. Details of the 24 molecular structures are presented in Figure 2.
The latest standards for different GFW forms established by high-performance liquid chromatography (HPLC) to guarantee the quality of GFW were cinnamic acid (B2) ≥72 µg and paeonol (E14) ≥6 mg per pill in honey pill form; paeonol (E14) ≥1.8 mg, paeoniflorin (F9) ≥3 mg, and amygdalin (C2) ≥1.5 mg per tablet in tablet form; paeonol (E14) ≥1.8 mg, paeoniflorin (F9) ≥3 mg, and amygdalin (C2) ≥ 0.9 mg per capsule in capsule form [17].
3.2. Pharmacodynamic Effects of GFW on MHFs
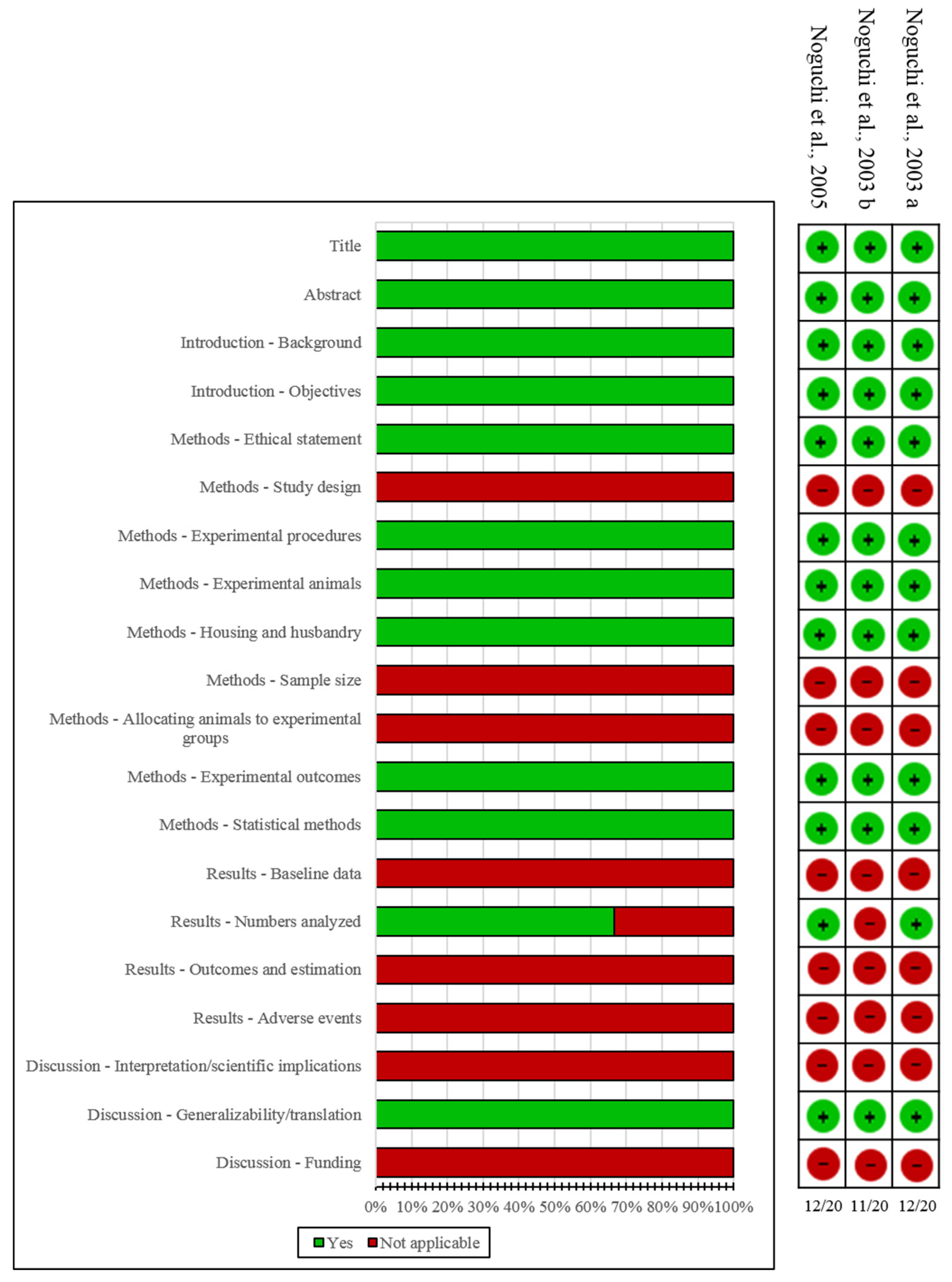
Characteristics and results of included in vivo studies are summarized in Table 3. The results from the quality assessment of included in vivo experimental studies are presented in Figure 3. The results suggested that GFW had a similar action to E2 on managing skin temperature by restoring the plasma level of CGRP: it increased the ovariectomy-induced CGRP reduction [66,67] and reduced CGRP-induced elevation of skin temperature in GnRH (gonadotropin-releasing hormone) analog-treated rats [67,68]. A dose-dependent skin temperature change was detected, showing that a significant inhibition effect on elevated skin temperature was observed at a dose of 1000 mg/kg [67,68]. However, GFW had no significant effects on CGRP concentrations and CGRP mRNA levels in the dorsal root ganglia [66], which suggested minor effects on CGRP synthesis in an ovariectomized rat model. GFW had no significant effects on CGRP concentrations in the spinal cord [66], which suggested that it may have an inconsequential influence on CGRP’s effects on the central nervous system in the ovariectomized rat model.
One in vitro experimental study [69] utilized an ESR-dependent cell proliferation bioassay and an ESR-dependent reporter assay to investigate the potential estrogenic activity of GFW and its metabolites. The results demonstrated that GFW showed no estrogenic activity and low ER β-dependent estrogenic activity before or after metabolization with a concentration at 100 μg/mL. Findings from two in vivo studies concluded that E2 could significantly reduce the levels of pituitary LH (luteinizing hormone) and FSH, as well as the weights of uterus and ovaries, whereas GFW did not influence those factors [67,68]. Thus, GFW did not confer estrogen activity on plasma and might exert pharmacodynamic effects against MHFs via other pathways.
4. Translation from Experimental Studies to Clinical Practice
4.1. Therapeutic Effects
A well-designed RCT is considered as the gold standard when evaluating the effects of an intervention [70]. However, its limitations have triggered extensive discussion as RCTs may be unnecessary, inappropriate, inadequate, or even impossible in the clinic, and methodological problems can cause bias in the results [71,72,73]. Besides, CHM involves a holistic therapeutic approach. However, most of the published RCTs on CHM were designed to only investigate the therapeutic aspects (i.e., Chinese medicine intervention + western medicine diagnosis) instead of the holistic therapeutic approach (i.e., Chinese medicine intervention + Chinese medicine diagnosis) [74]. The importance of integration of various study designs was highlighted to accommodate the evaluation of various research questions and for the outcome of interest [75,76]. Therefore, the therapeutic effects of a range of study designs were systematically reviewed (Figure 4).
As shown in Figure 4, the study types and outcome measures varied across all the included studies. Most outcomes were measured in different study designs. GFW demonstrated overall no statistically significant changes in the frequency and severity of MHFs between before and after treatment and no statistically significant differences between GFW and control groups. However, dose-dependent skin temperature changes were detected in both clinical [15] and experimental studies [69,70]. The effective dose suggested in the in vivo study was 1000 mg/kg [69,70], which was four times the dose in the RCT (12.5 g/day) when the participant weighed in at 50 kg [15]. Thus, more dose variation should be considered in further RCTs. The influence of GFW on FSH and E2 was unclear based on the included studies due to the limitation of study design. Results of experimental studies indicated that GFW had no effects on LH, FSH, and E2 in Sprague-Dawley rats and no estrogenic effects on the rat liver S9 fraction. However, case series studies pointed out that GFW might target a specific human ESR2 beta genotype. GFW was found to affect CGRP level in both case series and in vivo studies [28,66,67,69]. GFW had similar effects to E2 on normalizing CGRP level but without affecting its synthesis in the dorsal root ganglia. Only peripheral blood flow and cytokines were reported in one study design, which should be further investigated in various studies.
4.2. Potential Multi-Targeting Actions
Three potential target proteins/cytokine could be proposed based on findings from the above-mentioned clinical and experimental studies: estrogen beta receptor, IL-8, and CGRP receptor.
There are significant associations between the ESR2 CA dinucleotide repeat length and other menopausal-related symptoms. For example, low bone mineral density has been reported previously in pre- and post-menopausal women [31,77,78]. This genetic variation was characterized by Tsukamoto and co-workers in 1998 [79]. Recently, ESR2 CA dinucleotide repeat length was reported to be closely related to clinical effects of GFW on MHFs and that it had better performance on participants with the LL genotype [29]. Women with the SS genotype had significantly higher values of circulation estrone concentration (highest) when compared to those harboring the LL genotype (lowest) after adjustment for other confounding factors, including age, hormone replacement status, and circulating levels of sex hormone-binding globulin [31]. Thus, genetic variation should be considered as an essential factor of using GFW for MHFs to achieve precision treatment. The prevalence of the SS and SL genotypes was approximately 47.79% (108/226) and 22.56% (51/226), respectively [31]. The sum of these two genotypes was much higher than that of the LL genotype (29.65%, 67/226). Thus, patients without targeting genotype might contribute to the negative results in the RCT. It is suggested that future research focus on the three genotypes of ESR2 for precision medicine.
IL-8, also known as CXCL8, is a cytokine potentially involved in thermoregulation and was detected to be higher in premenopausal and menopausal women with MHFs than in those without MHFs [80,81]. GFW could significantly reduce concentrations of serum IL-8, whereas those in the non-responders were increased dramatically [27]. Thus, GFW might selectively influence the synthesis of IL-8. However, the underlying mechanism of this selective effect in different MHF sufferers is not fully understood.
CGRP is a widely expressed sensory neuropeptide, which plays a major role in modulating metabolism, inflammatory response, and blood pressure, as well as contributing to nerve development and function [82,83,84,85,86]. In the sympathetic nervous system, CGRP is believed to be the specific vasodilator responsible for MHFs [4,84]. Recently, Liang et al. [86] have determined the structure of the human CGRP receptor in complex with CGRP, with the Gs-protein heterotrimer at 3.3 Å global resolution, which makes it possible for future investigation of the potential herb-target relationship between GFW and MHF-related target protein.
4.3. Safety
Inorganic elements that may have vital biological activities in the human body were traced in GFW, including calcium, sodium, magnesium with a dose over 300 µg/g, followed by iron, manganese, and strontium with a dose over 10 µg/g [65]. The dosage of toxic inorganic elements detected in the included studies included beryllium, arsenic, cadmium, antimony, mercury, thallium, and bismuth, which were under 0.03 µg/g and were lower than the maximum limit level listed in the Chinese Pharmacopoeia [65]. GFW is believed to be a safe herbal product as only a small number of minor gastrointestinal symptoms were reported as adverse effects: two studies reported adverse events, including diarrhea (n = 15) [15] and abnormal feeling in the gastrointestinal tract (n = 2) [27]. They were the main causes leading to drop out. Additionally, an in vivo study on Sprague-Dawley rats indicating that GFW was not carcinogenic after a continuous 24-month intervention [87]. Results from another in vitro experiment [68] on estrogen-dependent human breast cancer (MCF-7) cells showed that GFW at concentrations of 10.6–10.4 mg/mL did not activate the proliferation of MCF-7 cell, which suggested that GFW did not exhibit estrogen activity. Therefore, GFW might be a potential therapeutic option for MHFs in women who are undergoing breast cancer treatment.
4.4. Implications for Future Research
In total, 169 compounds from GFW and three potential target proteins/cytokine (estrogen beta receptor, IL-8, and CGRP receptor) were identified based on findings from the above-mentioned clinical and experimental studies. However, at this stage, a clear understanding of their interactions could not be obtained based on current literature. The bioactivities of the phytochemicals and their mechanisms of actions on MHF were not fully investigated. Although quality control is improving during the last two decades, evidenced by the increased quantitative index from one in the 2005 edition to two or three in the 2015 edition of the Chinese Pharmacopeia [17], not all the herbal ingredients have a quantitative index. The clinical effects of CHM are often regarded as the result of the multi-targeting interaction of various phytochemical compounds. Thus, more research on the mechanism of actions of CHM on a condition at the molecular level (ligand-target interaction) and the therapeutic dose of the bioactive compounds are warranted.
5. Conclusions
This study identified 169 compounds from GFW pills, tablets, and capsules. Therapeutic effects, including frequency and severity of MHFs, peripheral blood flow, hormones, neurotransmitter, and cytokines, were not consistent across different study types. ESR2 with genetic variation, CGRP receptor, and IL-8 were identified to be related to the mechanisms of actions of GFW on MHFs. The differences in therapeutic effects could be potentially due to dose variations among clinical and experimental studies and ESR2 gene differences in rats and homo species. Further clinical and experimental studies, as well as biochemical investigation on the mechanisms of actions of GFW, are warranted. It is recommended that the dose-dependent effects and ESR2 expression at the participant recruitment stage are considered in future investigation.
Author Contributions
Conceptualization, M.L., A.W.H.Y., and A.H.; Formal Analysis, M.L., A.W.H.Y., A.H., and H.L.; Data curation, M.L., A.W.H.Y., A.H., and H.L.; Writing—Original Draft Preparation, M.L.; Writing—Review and Editing, A.W.H.Y., A.H., and H.L.; Visualization, M.L. and H.L.; Supervision, A.W.H.Y., and A.H.; Project Administration, M.L., A.W.H.Y., and A.H.
Funding
This research received no external funding.
Acknowledgments
We thank Mathew Guo from the Nanjing University of Chinese Medicine and Chunlan Wang from the Ocean University of China for their assistance in searching the SinoMed and CNKI database.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Freeman, E.W.; Sherif, K. Prevalence of hot flushes and night sweats around the world: A systematic review. Climacteric 2007, 10, 197–214. [Google Scholar] [CrossRef] [PubMed]
- Berek, J.S.; Novak, E. Berek Novak’s Gynecology, 15th ed.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Jha, U.P. Hot flushes. In Differential Diagnosis in Obstetrics and Gynaecology: An a-z; Hollingworth, T., Ed.; Hodder Arnold: London, UK, 2008; pp. 43–48. [Google Scholar]
- Gupta, P.; Harte, A.L.; da Silva, N.F.; Khan, H.; Barnett, A.H.; Kumar, S.; Sturdee, D.W.; McTernan, P.G. Expression of calcitonin gene-related peptide, adrenomedullin, and receptor modifying proteins in human adipose tissue and alteration in their expression with menopause status. Menopause 2007, 14, 1031–1038. [Google Scholar] [CrossRef] [PubMed]
- Chakravarti, S.; Collins, W.P.; Newton, J.R.; Oram, D.H.; Studd, J.W.W. Endocrine changes and symptomatology after oophorectomy in premenopausal women. BJOG 1977, 84, 769–775. [Google Scholar] [CrossRef]
- Schuiling, K.D.; Likis, F.E. Women’s Gynecologic Health, 3rd ed.; Jones & Bartlett Learning: Burlington, MA, USA, 2017. [Google Scholar]
- Freedman, R.R.; Krell, W. Reduced thermoregulatory null zone in postmenopausal women with hot flashes. AJOG 1999, 181, 66–70. [Google Scholar] [CrossRef]
- Freedman, R.R. Biochemical, metabolic, and vascular mechanisms in menopausal hot flashes. Fertil. Steril. 1998, 70, 332–337. [Google Scholar] [CrossRef]
- Berendsen, H.H.G. The role of serotonin in hot flushes. Maturitas 2000, 36, 155–164. [Google Scholar] [CrossRef]
- Mintziori, G.; Lambrinoudaki, I.; Goulis, D.G.; Ceausu, I.; Depypere, H.; Erel, C.T.; Pérez-López, F.R.; Schenck-Gustafsson, K.; Simoncini, T.; Tremollieres, F. EMAS position statement: Non-hormonal management of menopausal vasomotor symptoms. Maturitas 2015, 81, 410–413. [Google Scholar] [CrossRef]
- Wnuk, A.; Korol, D.L.; Erickson, K.I. Estrogens, hormone therapy, and hippocampal volume in postmenopausal women. Maturitas 2012, 73, 186–190. [Google Scholar] [CrossRef] [Green Version]
- National Guideline Clearinghouse. Menopause: Diagnosis and Management. Available online: https://www.guideline.gov/summaries/summary/49904/menopause-diagnosis-and-management?q=menopausal (accessed on 8 November 2017).
- Peng, W.; Adams, J.; Hickman, L.; Sibbritt, D.W. Longitudinal analysis of associations between women’s consultations with complementary and alternative medicine practitioners/use of self-prescribed complementary and alternative medicine and menopause-related symptoms, 2007–2010. Menopause 2016, 23, 74–80. [Google Scholar] [CrossRef]
- Ushiroyama, T.; Ikeda, A.; Sakuma, K.; Ueki, M. Comparing the effects of estrogen and an herbal medicine on peripheral blood flow in post-menopausal women with hot flashes: Hormone replacement therapy and Gui-Zhi-Fu-Ling-Wan, a Kampo medicine. AJCM 2005, 33, 259. [Google Scholar] [CrossRef]
- Plotnikoff, G.A.; Watanabe, K.; Torkelson, C.; La Valleur, J.; Radosevich, D.M.; Plotnikoff, G.A.; Watanabe, K.; Torkelson, C.; La Valleur, J.; Radosevich, D.M. The TU-025 keishibukuryogan clinical trial for hot flash management in postmenopausal women: Results and lessons for future research. Menopause 2011, 18, 886–892. [Google Scholar] [CrossRef]
- Zhang, Z.J. Gui Zhi Fu Ling Wan. In Jin Guì Yào Lüè Essential Prescriptions of the Golden Cabinet: Translation and Commentaries; Wiseman, N., Wilms, S., Eds.; Paradigm Publications: Taos, NM, USA, 2013; pp. 493–497. [Google Scholar]
- Chinese Pharmacopoeia Commission. Chinese Pharmacopoeia, 2015 ed.; China Medical Science Press: Beijing, China, 2015. [Google Scholar]
- ClinicalTrials, ClinicalTrials.gov. Effect of KYG0395 on Primary Dysmenorrhea. Available online: https://clinicaltrials.gov/ct2/show/study/NCT01588236?term=KYG0395&rank=1 (accessed on 6 August 2019).
- Ni, H.; Matsumoto, T.; Watanabe, J.; Makino, T. Inhibitory Effect of Japanese Traditional Kampo Formula Frequently Prescribed in Gynecological Clinics on CYP3A4. eCAM 2018, 2018, e4259603. [Google Scholar] [CrossRef]
- Lee, H.S.; Shin, H.J.; Cho, M.; Lee, S.H.; Oh, D.S. Inhibitory effects of Kampo medicines, Keishibukuryogan and Shakuyakukanzoto, on the substrate uptake activities of solute carrier organic anion transporters. JPS 2018, 138, 279–283. [Google Scholar] [CrossRef]
- Furue, M.; Fuyuno, Y.; Mitoma, C.; Uchi, H.; Tsuji, G. Therapeutic agents with AHR inhibiting and NRF2 activating activity for managing chloracne. Antioxidants 2018, 7, 90. [Google Scholar] [CrossRef] [PubMed]
- Terauchi, M.; Hiramitsu, S.; Akiyoshi, M.; Owa, Y.; Kato, K.; Obayashi, S.; Matsushima, E.; Kubota, T. Effects of three Kampo formulae: Tokishakuyakusan (TJ-23), Kamishoyosan (TJ-24), and Keishibukuryogan (TJ-25) on Japanese peri- and postmenopausal women with sleep disturbances. Arch. Gynecol. Obstet. 2010, 284, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Terauchi, M.; Akiyoshi, M.; Owa, Y.; Kato, K.; Obayashi, S.; Kubota, T. Effects of the Kampo medication keishibukuryogan on blood pressure in perimenopausal and postmenopausal women. Int. J. Gynaecol. Obstet. 2011, 114, 149–152. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Wiley Blackwell: Chichester, UK; Hoboken, NJ, USA, 2011. [Google Scholar]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. Br. Med. J. 2016, 355, i4919. [Google Scholar] [CrossRef]
- Yang, A.W.; Li, C.G.; Da Costa, C.; Allan, G.; Reece, J.; Xue, C.C. Assessing quality of case series studies: Development and validation of an instrument by herbal medicine CAM researchers. J. Altern. Complement. Med. 2009, 15, 513–522. [Google Scholar] [CrossRef]
- Yasui, T.; Matsui, S.; Yamamoto, S.; Uemura, H.; Tsuchiya, N.; Noguchi, M.; Yuzurihara, M.; Kase, Y.; Irahara, M. Effects of Japanese traditional medicines on circulating cytokine levels in women with hot flashes. Menopause 2011, 18, 85–92. [Google Scholar] [CrossRef]
- Chen, J.T.; Shiraki, M. Menopausal hot flash and calciotonin gene-related peptide; effect of Keishi-bukuryo-gan, a kampo medicine, related to plasma calciotonin gene-related peptide level. Maturitas 2003, 45, 199–204. [Google Scholar] [CrossRef]
- Namiki, T.; Sato, H.; Matsumoto, Y.; Kakikura, H.; Ueno, K.; Chino, A.; Okamoto, H.; Hisanaga, A.; Kaneko, A.; Kita, T.; et al. Identification of a predictive biomarker for the beneficial effect of Keishibukuryogan, a Kampo (Japanese traditional) medicine, on patients with climacteric syndrome. eCAM 2014, 2014, e962109. [Google Scholar] [CrossRef]
- Westberg, L.; Baghaei, F.; Rosmond, R.; Hellstrand, M.; Landen, M.; Jansson, M.; Holm, G.; Bjorntorp, P.; Eriksson, E. Polymorphisms of the androgen receptor gene and the estrogen receptor beta gene are associated with androgen levels in women. J. Clin. Endocrinol. Metab. 2001, 86, 2562–2568. [Google Scholar]
- Scariano, J.K.; Simplicio, S.G.; Montoya, G.D.; Garry, P.J.; Baumgartner, R.N. Estrogen receptor β dinucleotide (CA) repeat polymorphism is significantly associated with bone mineral density in postmenopausal women. Calcif. Tissue Int. 2004, 74, 501–508. [Google Scholar] [CrossRef]
- Sturdee, D.W.; Hunter, M.S.; Maki, P.M.; Gupta, P.; Sassarini, J.; Stevenson, J.C.; Lumsden, M.A. The menopausal hot flush: A review. Climacteric 2017, 20, 296–305. [Google Scholar] [CrossRef]
- Dassault Systèmes BIOVIA. BIOVIA Draw; Dassault Systèmes: San Diego, CA, USA, 2019. [Google Scholar]
- Hanwell, M.D.; Curtis, D.E.; Lonie, D.C.; Vandermeersch, T.; Zurek, E.; Hutchison, G.R. Avogadro: An advanced semantic chemical editor, visualization, and analysis platform. J. Cheminform. 2012, 4, 17. [Google Scholar] [CrossRef]
- Dassault Systèmes BIOVIA. Discovery Studio Visualizer; Dassault Systèmes: San Diego, CA, USA, 2019. [Google Scholar]
- Kilkenny, C.; Browne, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Improving bioscience research reporting: The ARRIVE guidelines for reporting animal research. PLoS Biol. 2010, 8, e1000412. [Google Scholar] [CrossRef]
- Zhang, Y.; Cheng, Y.; Liu, Z.; Ding, L.; Qiu, T.; Chai, L.; Qiu, F.; Wang, Z.; Xiao, W.; Zhao, L.; et al. Systematic screening and characterization of multiple constituents in Guizhi Fuling capsule and metabolic profiling of bioactive components in rats using ultra-high-performance liquid chromatography/quadrupole-time-of-flight mass spectrometry. J. Chromatogr. B 2017, 1061, 474–486. [Google Scholar] [CrossRef]
- Feng, C.P. Determination of cinnamic acid, cinnamaldehyde and paeonol in Guizhi Fuling pills by HPLC. Guid. J. Tradit. Chin. Med. Pharm. 2009, 15, 76–78. [Google Scholar]
- Hua, J.; Wu, C. Determination of cinnamic acid, cinnamaldehyde and paeonol in Guizhi Fuling capsules by HPLC. Anhui Med. Pharm. J. 2006, 10, 30–31. [Google Scholar]
- Yang, Q.; Guo, Y.R. Simultaneous determination of cinnamaldehyde and paeonol in Guizhi Fuling capsules by SPE-HPLC. Chin. Pharm. 2010, 13, 1312–1314. [Google Scholar]
- He, Y.M.; Lin, X.; Wang, X.; Li, J.C.; Huang, W.Z.; Xiao, W. Determination of dissolution of eight active ingredients in Guizhi Fuling capsules by UPLC. Chin. J. Exp. Tradit. Med. Formulae 2018, 24, 14–19. [Google Scholar]
- Xie, X.; Zhang, H.D.; Wen, J.H.; Song, Y.L.; Wang, X.J.; Zhao, W.W.; Huang, W.Z.; Wang, Z.Z.; Xiao, W. Study on chemical constituents of Guizhi Fuling capsules (VI). Chin. Tradit. Herb. Drugs 2016, 47, 3795–3797. [Google Scholar]
- Li, W.S.; Huang, L.L.; Li, Z.J.; Tang, M.H.; Guo, K. Optimization of extraction solvent in the chemical composition analysis of Guizhi Fuling capsules by HPLC-ESI-QTOF/MS. Chin. J. Bioproc. E 2016, 14, 59–64. [Google Scholar]
- Zhang, Y.H.; Zhang, D.W.; Meng, Z.Q.; Liu, L.Y.; Jin, Y. Rapid determination of paeoniflorin, paeonol, amygdalin and cinnamic acid in Guizhi Fuling capsules by online two-dimensional liquid chromatography. Zhongguo Zhong Yao Za Zhi 2013, 38, 4088–4093. [Google Scholar]
- Sui, Y.; Zhao, L.S.; Wang, Z.Z.; Zhao, Y.T.; Xiao, W.; Xiong, Z.L. Simultaneous determination of seven bioactive components in Guizhi Fuling capsule by microwave-assisted extraction combined with ultra performance liquid chromatography tandem mass spectrometry. Nat. Prod. Res. 2016, 30, 354–357. [Google Scholar] [CrossRef]
- Yin, Q.W.; Wang, J.L.; Yang, S.D.; Huang, W.Z.; Xiao, W. Analysis of α-linolenic acid, linoleic acid and oleic acid in Guizhi Fuling capsules. Pharm. Clin. Res. 2016, 24, 110–112. [Google Scholar]
- Zhang, Q.; Chen, M.L.; Sun, Y.L.; Zhang, Y.; Gao, X.Y. Simultaneous measurement of amygdalin, paeonol and paeoniflorin in Guizhi Fuling tablets by HPLC. World Latest Med. Inf. 2017, 17, 113–114. [Google Scholar]
- Jin, Q.X.; Huang, Y.F. Determination of amygdalin in ethanol treatment of Guizhi Fuling capsules by HPLC. Chin. Arch. Tradit. Chin Med. 2012, 30, 381–382. [Google Scholar]
- Wang, H.Y.; Huang, Y.F. ANOVA for optimization of amygdalin leaching rate in Guizhi Fuling capsules. Zhongguo Zhong Yao Za Zhi 2011, 29, 2700–2701. [Google Scholar]
- Fang, L.Q. Simultaneous determination of paeonol, paeoniflorin and amygdalin in Guizhi Fuling capsules by HPLC. J. North Pharm. 2015, 12, 5–6. [Google Scholar]
- Liao, Z.G.; Jiang, Q.Y.; Liang, X.L.; Ping, Q.N. Comparative study on the dissolution of three active ingredients in Guizhi Fuling capsules in vitro. Chin. Tradit. Patent Med. 2008, 30, 1141–1144. [Google Scholar]
- Ma, T.T.; Chen, X.H.; Lin, X.Y.; Guo, D.A.; Bi, K.S. Simultaneous determination of three components in Guizhi Fuling capsules by RP-HPLC. J. Shenyang Pharm. Univ. 2010, 27, 216–219. [Google Scholar]
- Wang, X.J.; Xie, X.; Luo, X.; Zhao, W.W.; Huang, W.Z.; Wang, Z.Z.; Xiao, W. Study on chemical constituents of Guizhi Fuling capsules (V). Chin. Tradit. Herb. Drugs 2015, 46, 812–816. [Google Scholar]
- Wang, H.Q.; Liu, C.; Fang, L.H.; Wang, Z.Z.; Xiao, W.; Chen, R.Y. Study on chemical constituents of Guizhi Fuling capsules (IV). Chin. Tradit. Herb. Drugs 2013, 44, 1386–1390. [Google Scholar]
- Yang, P.F.; Wang, Z.Z.; Wang, H.Q.; Li, J.C.; Chen, R.Y. Study on chemical constituents of Guizhi Fuling capsules (III). Chin. Tradit. Herb. Drugs 2012, 43, 463–466. [Google Scholar]
- Shi, X.Q. Determination of paeonol in Guizhi Fuling capsules by gas chromatography. Guangzhou Chem. Ind. 2015, 43, 145–146, 173. [Google Scholar]
- Pan, H.P.; Chen, Y.; Fu, C.L. Determination of paeonol in Guizhi Fuling capsules by HPLC. Zhongguo Zhong Yao Za Zhi 2002, 27, 34–36. [Google Scholar]
- Mao, J.X. Determination of paeonol in Guizhi Fuling capsules by HPLC. Lishizhen Med. Mater. Med. Res. 2009, 20, 2112. [Google Scholar]
- Wu, X.H.; Fang, H.; Pu, C.Y.; Yang, D.X.; Wang, F.S.; He, L.W.; Zhang, N. Study of Guizhi Fuling pills using HPLC Fingerprint. J. Anal. Sci. 2014, 30, 100–102. [Google Scholar]
- Niu, S.L.; Guo, Y.L.; Liu, X.; Zhang, X.N. Determination of paeoniflorin in Guizhi Fuling capsules by HPLC. Herald Med. 2004, 23, 863. [Google Scholar]
- Ma, Y.; Zheng, W.R.; Wang, Z.Z.; Xiao, W.; Huang, W.Z.; Zhang, Y.W. UPLC/Q-TOF-MS fingerprint of triterpenic acids in Guizhi Fuling capsules. Chin. Tradit. Herb. Drugs 2019, 50, 626–631. [Google Scholar]
- Yang, P.F.; Li, B.M.; Wang, Z.Z.; Xiao, W.; Chen, R.Y. Simultaneous determination of four barium tridecanoic acids in Guizhi Fuling capsules by HPLC. Chin. Tradit. Herb. Drugs 2016, 47, 3215–3218. [Google Scholar]
- Wu, L.-F.; Wang, K.-F.; Mao, X.; Liang, W.-Y.; Chen, W.-J.; Li, S.; Qi, Q.; Cui, Y.-P.; Zhang, L.-Z. Screening and analysis of the potential bioactive components of Poria cocos (Schw.) wolf by HPLC and HPLC-MSn with the aid of chemometrics. Molecules 2016, 21, 227. [Google Scholar] [CrossRef]
- Ma, Y.; Li, J.C.; Huang, W.Z.; Wang, Z.Z.; Xiao, W.; Song, Y.L.; Zhang, Y.W. Simultaneous determination of six triterpenoids in Guizhi Fuling capsules by UPLC-MS/MS. Zhongguo Zhong Yao Za Zhi 2017, 42, 1–12. [Google Scholar]
- Kang, Y.; Liu, X.H.; Wang, B. Analysis of inorganic elements in Guizhi Fuling capsules based on ICP-MS. Chin. Tradit. Herb. Drugs 2018, 49, 3292–3297. [Google Scholar]
- Noguchi, M.; Ikarashi, Y.; Yuzurihara, M.; Kase, Y.; Takeda, S.; Aburada, M. Effects of 17b-estradiol and the japanese herbal medicine keishi-bukuryo-gan on the release and synthesis of calcitonin gene-related peptide in ovariectomized rats. J. Pharmacol. Sci. 2003, 93, 80–86. [Google Scholar] [CrossRef]
- Noguchi, M.; Ikarashi, Y.; Yuzurihara, M.; Kase, Y.; Chen, J.T.; Takeda, S.; Aburada, M.; Ishige, A. Effects of the Japanese herbal medicine Keishi-bukuryo-gan and 17beta-estradiol on calcitonin gene-related peptide-induced elevation of skin temperature in ovariectomized rats. J. Endocrinol. 2003, 176, 359–366. [Google Scholar] [CrossRef] [Green Version]
- Noguchi, M.; Ikarashi, Y.; Yuzurihara, M.; Kase, Y.; Watanabe, K.; Plotnikoff, G.A.; Takeda, S.; Aburada, M. Skin temperature rise induced by calcitonin gene-related peptide in gonadotropin-releasing hormone analogue-treated female rats and alleviation by Keishi-bukuryo-gan, a Japanese herbal medicine. Life Sci. 2005, 76, 2079–2090. [Google Scholar] [CrossRef]
- Wang, Z.; Kanda, S.; Shimono, T.; Enkh-Undraa, D.; Nishiyama, T. The in vitro estrogenic activity of the crude drugs found in Japanese herbal medicines prescribed for menopausal syndrome was enhanced by combining them. BMC Complement. Altern. Med. 2018, 18, 107. [Google Scholar] [CrossRef]
- Akobeng, A. Understanding randomised controlled trials. Arch. Dis. Child. 2005, 90, 840–844. [Google Scholar] [CrossRef] [Green Version]
- Earl-Slater, A. The Handbook of Clinical Trials and Other Research; Radcliffe Medical: Abingdon, UK, 2002. [Google Scholar]
- Greenhalgh, T.A. How to Read a Paper: The Basics of Evidence-Based Medicine, 5th ed.; John Wiley & Sons: Chichester, UK; Hoboken, NJ, USA, 2014. [Google Scholar]
- Liu, J.P. Clinical Research Methodology for Evidence-Based Chinese Medicine; China Agriculture Press: Beijing, China, 2006. [Google Scholar]
- Liu, J.P. The system of evidence levels in Chinese Medicine clinical trial. In Clinical Research Methodology for Evidence-Based Chinese Medicine; People’s Medicine Publishing House: Beijing, China, 2006; pp. 11–31. [Google Scholar]
- Peinemann, F.; Tushabe, D.A.; Kleijnen, J. Using multiple types of studies in systematic reviews of health care interventions–a systematic review. PLoS ONE 2013, 8, e85035. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P. Observational research, randomised trials, and two views of medical science. PLoS Med. 2008, 5, e67. [Google Scholar] [CrossRef]
- Lau, H.H.; Ho, A.Y.; Luk, K.D.; Kung, A.W. Estrogen receptor beta gene polymorphisms are associated with higher bone mineral density in premenopausal, but not postmenopausal southern Chinese women. Bone 2002, 31, 276–281. [Google Scholar] [CrossRef]
- Ogawa, S.; Hosoi, T.; Shiraki, M.; Orimo, H.; Emi, M.; Muramatsu, M.; Ouchi, Y.; Inoue, S. Association of estrogen receptor beta gene polymorphism with bone mineral density. Biochem. Biophys. Res. Commun. 2000, 269, 537–541. [Google Scholar] [CrossRef]
- Tsukamoto, K.; Inoue, S.; Hosoi, T.; Orimo, H.; Emi, M. Isolation and radiation hybrid mapping of dinucleotide repeat polymorphism at the human estrogen receptor beta locus. J. Hum. Genet. 1998, 43, 73–74. [Google Scholar] [CrossRef]
- Yasui, T.; Uemura, H.; Tomita, J.; Miyatani, Y.; Yamada, M.; Kuwahara, A.; Matsuzaki, T.; Maegawa, M.; Tsuchiya, N.; Yuzurihara, M. Association of interleukin-8 with hot flashes in premenopausal, perimenopausal, and postmenopausal women and bilateral oophorectomized women. J. Clin. Endocrinol. Metab. 2006, 91, 4805–4808. [Google Scholar] [CrossRef]
- Malutan, A.; Costin, N.; Duncea, I.; Pepene, C.; Mihu, D.; Rada, M. Interleukin-8 and vasomotor symptoms in natural and surgically induced menopause. Acta Endocrinol. 2013, 9, 133–144. [Google Scholar] [CrossRef]
- Walker, C.S.; Li, X.; Whiting, L.; Glyn-Jones, S.; Zhang, S.; Hickey, A.J.; Sewell, M.A.; Ruggiero, K.; Phillips, A.R.; Kraegen, E.W.; et al. Mice lacking the neuropeptide alpha-calcitonin gene-related peptide are protected against diet-induced obesity. Endocrinology 2010, 151, 4257–4269. [Google Scholar] [CrossRef]
- Dickerson, I.M.; Bussey-Gaborski, R.; Holt, J.C.; Jordan, P.M.; Luebke, A.E. Maturation of suprathreshold auditory nerve activity involves cochlear CGRP-receptor complex formation. Physiol. Rep. 2016, 4, e12869. [Google Scholar] [CrossRef] [Green Version]
- Russell, F.A.; King, R.; Smillie, S.J.; Kodji, X.; Brain, S.D. Calcitonin gene-related peptide: Physiology and pathophysiology. Physiol. Rev. 2014, 94, 1099–1142. [Google Scholar] [CrossRef]
- Hay, D.L.; Garelja, M.L.; Poyner, D.R.; Walker, C.S. Update on the pharmacology of calcitonin/CGRP family of peptides: IUPHAR Review 25. Br. J. Pharmacol. 2018, 175, 3–17. [Google Scholar] [CrossRef]
- Liang, Y.-L.; Khoshouei, M.; Deganutti, G.; Glukhova, A.; Koole, C.; Peat, T.S.; Radjainia, M.; Plitzko, J.M.; Baumeister, W.; Miller, L.J.; et al. Cryo-EM structure of the active, Gs-protein complexed, human CGRP receptor. Nature 2018, 561, 492–497. [Google Scholar] [CrossRef]
- Kanitani, M.; Nishimura, N.; Edamoto, H.; Kase, Y. Keishibukuryogan is not carcinogenic in Sprague-Dawley rats. J. Toxicol. Pathol. 2016, 29, 103–110. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Flowchart of study selection procedures of Guizhi Fuling Wan on menopausal hot flushes.

Figure 2.
Molecular structures of the 24 chemical constituents of Guizhi Fuling Wan. Note: C3: Benzol-β-gentiobioside, C6: Mandelic acid gentiobioside/isomer, D1: 4′-O-galloypaeoniflorin, D6: Benzoylpaeoniflorin sulfate, D10: Galloyglucose/isomer, D12: Galloylpaeoniflorin sulfonate, D13: Hexagalloyl glucose, D14: Isoxypaeoniflora, D19: Tetragalloy glucose, D20: Trigalloy glucose, E1: 3-hydroxypaeonol, E10: Mudanpioside E sulfonate, F1: 1-O-β-d-glucopyranosyl-paeonisuffrone, F2: 6-O-β-d-glucopyranosyl lactinolide, F7: Isomaltopaeoniflorin sulfonate, G4: 25-Hydroxypachymic acid, G5: 31-Hydroxyl-16-O-acetylpachymic acid, G10: 3-oxo-6,16α-dihydroxy-lanosta-7,9(11),24(31)-trien-21-oic acid, G12: 3β,16α-Dihydroxy-lanosta-7,9(11),24-trien-21-oic acid, G14: 6α-Hydroxydehydropachymic acid, G21: Pachymic acid methyl ester, H1: (2R)-[(6-O-β-d-glucopyranosyl-β-d-glucopyranosyl) oxy] (phenyl) ethanoic acid, H2: 2,5-dihydroxy-4-methylacetophenone, H15: Benzyl-β-d-glucopyranosyl-(1→6)-β-d-glucopyranoside.
Figure 2.
Molecular structures of the 24 chemical constituents of Guizhi Fuling Wan. Note: C3: Benzol-β-gentiobioside, C6: Mandelic acid gentiobioside/isomer, D1: 4′-O-galloypaeoniflorin, D6: Benzoylpaeoniflorin sulfate, D10: Galloyglucose/isomer, D12: Galloylpaeoniflorin sulfonate, D13: Hexagalloyl glucose, D14: Isoxypaeoniflora, D19: Tetragalloy glucose, D20: Trigalloy glucose, E1: 3-hydroxypaeonol, E10: Mudanpioside E sulfonate, F1: 1-O-β-d-glucopyranosyl-paeonisuffrone, F2: 6-O-β-d-glucopyranosyl lactinolide, F7: Isomaltopaeoniflorin sulfonate, G4: 25-Hydroxypachymic acid, G5: 31-Hydroxyl-16-O-acetylpachymic acid, G10: 3-oxo-6,16α-dihydroxy-lanosta-7,9(11),24(31)-trien-21-oic acid, G12: 3β,16α-Dihydroxy-lanosta-7,9(11),24-trien-21-oic acid, G14: 6α-Hydroxydehydropachymic acid, G21: Pachymic acid methyl ester, H1: (2R)-[(6-O-β-d-glucopyranosyl-β-d-glucopyranosyl) oxy] (phenyl) ethanoic acid, H2: 2,5-dihydroxy-4-methylacetophenone, H15: Benzyl-β-d-glucopyranosyl-(1→6)-β-d-glucopyranoside.

Figure 3.
Quality assessment of included in vivo studies according to ARRIVE (Animal Research: Reporting of In Vivo Experiments) guideline.
Figure 3.
Quality assessment of included in vivo studies according to ARRIVE (Animal Research: Reporting of In Vivo Experiments) guideline.

Figure 4.
Therapeutic effects of Guizhi Fuling Wan on menopausal hot flushes across different types of studies. Notes: CGRP: calcitonin gene-related peptide; E2: estradiol; ESR: estrogen receptor; FSH: follicle-stimulating hormone; 1IL: interleukin; LH: luteinizing hormone; LL: two long alleles; MIP: macrophage inflammatory protein; MCP: serum monocyte chemotactic protein; RCT: randomized controlled trial.
Figure 4.
Therapeutic effects of Guizhi Fuling Wan on menopausal hot flushes across different types of studies. Notes: CGRP: calcitonin gene-related peptide; E2: estradiol; ESR: estrogen receptor; FSH: follicle-stimulating hormone; 1IL: interleukin; LH: luteinizing hormone; LL: two long alleles; MIP: macrophage inflammatory protein; MCP: serum monocyte chemotactic protein; RCT: randomized controlled trial.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Characteristics and quality assessment of included studies of Guizhi Fuling Wan for menopausal hot flushes.
Table 1.
Characteristics and quality assessment of included studies of Guizhi Fuling Wan for menopausal hot flushes.
| Study Name | Setting (Country) | Sample Size; Age | Diagnosis | Interventions | Duration | Outcomes Involved in this Review | Quality Assessment |
|---|---|---|---|---|---|---|---|
| RCT | |||||||
| Plotnikoff et al. 2011 [15] | University (US) | 178; 45–58 | Post-menopausal | T1: GFW at 7.5 g/day (n = 62); T2: GFW at 12.5 g/day (n = 57); C: Placebo (n = 59) | 12 weeks (12 weeks duration + 1-week placebo run-in period) | Frequency and severity of MHFs | L, L, L, L, L, H |
| Ushiroyama et al. 2005 [14] | College (Japan) | 140; T: 53.1 ± 6.5; C: 53.5 ± 6.2 | Post-menopausal | T: GFW 7.5 g/day (n = 70); C: oral HT (Premarin R 0.625 mg/day + Provera R: 2.5 mg/day) (n = 70) | 1 month | Blood flow in peripheral tissue | U, U, H, U, H, L |
| Parallel Controlled Study | |||||||
| Yasui et al. 2011 [27] | Outpatient clinic of a university hospital (Japan) | 77; T: 52 (39.3–58.7); C: 51 (43.4–57) | Pre-menopausal, peri-menopausal, post-menopausal, and bilateral oophorectomized | T: GFW 7.5 g/day (n = 38); C: No treatment (n = 39) | 6 months | The severity of MHFs, FSH, and E2 levels, IL-8, MCP-1, MIP-1β | L, L, L, L, M, S, L |
| Case Series | |||||||
| Chen and Shiraki 2003 [28] | Clinic (Japan) | 8; 53.59 ± 0.58 | Post-menopausal | GFW at 7.5 g/day (n = 8) | 4 weeks | Frequency of MHFs, plasma CGRP level | High-quality (score = 8) |
| Namiki et al. 2014 [29] | Hospital and clinic of university (Japan) | 39; 49.5 ± 4.69 (for 34 patients) | Post-menopausal (n = 18), ‘not yet menopausal’ (n = 21) | GFW at 2.5 g, 3 times/day (n = 39) | 12 weeks | Severity of MHFs, FSH, and E2 levels | High-quality (score = 10) |
| Terauchi et al. 2010 [22] | Hospital and clinic of university (Japan) | 16; 51.1 ± 2.4 | Peri- and post-menopausal | Education + GFW 7.5 g/day (n = 16) | 144 ± 58 days | Frequency of MHFs | High-quality (score = 8) |
| Terauchi et al. 2011 [23] | Hospital and clinic of university (Japan) | 30; 50.5 ± 5.2 | Peri- and post-menopausal | Education + GFW 7.5 g/day (n = 30) | 182 ± 76 days | Frequency of MHFs | High-quality (score = 7) |
Notes: C: control group; CGRP: calcitonin gene-related peptide; E2: estradiol; FSH: follicle-stimulating hormone; GFW: Guizhi Fuling Wan; H: high risk; MHFs: menopausal hot flushes; L: low risk; M: moderate risk; RCT: randomized controlled trial; S: serious risk; T: treatment group; U: unclear risk. Quality of RCTs was assessed Cochrane’s risk of bias assessment tool [24], quality of parallel controlled studies was evaluated by ROBINS-I (“Risk Of Bias In Non-randomised Studies - of Interventions”) [25], and case series were assessed according to the Instrument for Evaluating the Quality of case series in Chinese herbal medicine [26].
Table 2.
Chemical compounds from Guizhi Fuling Wan.
| ID | List of Chemical Compounds | Form of GFW | Molecular Formula | Molecular Weight (g/mol) | PubChem CID/SID | Methods |
|---|---|---|---|---|---|---|
| A | All ingredients (n = 1) | |||||
| A1 | Sucrose/isomer (isomer only in Paeoniae radix) | Capsule | C12H22O11 | 342.297 | 5988 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| B | Cinnamomi Ramulus (n = 3) | |||||
| B1 | Cinnamaldehyde | Capsule, pill | C9H8O | 132.162 | 637511 | HPLC [38,39], SPE-HPLC [40], UPLC [41] |
| B2 | Cinnamic acid | Capsule, pill | C9H8O2 | 148.161 | 444539 | HPLC [38,39], multiple chromatographic methods [42], HPLC-ESI-Q-TOF/MS [43], DGLC [44], UPLC [41], HPLC-MS/MS [45] |
| B3 | Protocatechuic acid | Capsule | C7H6O4 | 154.121 | 72 | LC-MS/UPLC-ESI-Q-TOF-MS [37], multiple chromatographic methods [42] |
| C | Persicae Semen (n = 12) | |||||
| C1 | A-Linolenic acid | C18H30O2 | 278.436 | 5280934 | HPLC [46] | |
| C2 | Amygdalin | Capsule, tablet | C20H27NO11 | 457.432 | 656516 | LC-MS/UPLC-ESI-Q-TOF-MS [37], HPLC [47,48,49,50,51], HPLC-ESI-Q-TOF/MS [43], DGLC [44], UPLC [41], HPLC-MS/MS [45] |
| C3 | Benzol-β-gentiobioside | Capsule | C19H28O11 | 432.42 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| C4 | Betulinic acid | Capsule | C30H48O3 | 456.711 | 64971 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| C5 | Linoleic acid | Capsule | C18H32O2 | 280.452 | 5280450 | LC-MS/UPLC-ESI-Q-TOF-MS [34], HPLC [46] |
| C6 | Mandelic acid gentiobioside/isomer | Capsule | C20H28O13 | 476.43 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| C7 | Mandelic acid-β-d-glucopyranoside | Capsule | C14H18O8 | 314.29 | 73229629 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| C8 | Oleic acid | Capsule | C18H34O2 | 282.468 | 445639 | LC-MS/UPLC-ESI-Q-TOF-MS [37], HPLC [46] |
| C9 | Palmitic acid | Capsule | C16H32O2 | 256.43 | 985 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| C10 | Prunasin | Capsule | C14H17NO6 | 295.291 | 119033 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| C11 | Stearic acid | Capsule | C18H36O2 | 284.484 | 5281 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| C12 | Trametenolic acid | Capsule | C30H48O3 | 456.711 | 12309443 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| D | Paeoniae Radix + Moutan Cortex (n = 20) | |||||
| D1 | 4′-O-galloypaeoniflorin | Capsule | C30H32O15 | 632.56 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| D2 | 4-hydroxybenzoic acid | Capsule | C7H6O3 | 138.122 | 135 | LC-MS/UPLC-ESI-Q-TOF-MS [37], multiple chromatographic methods [42] |
| D3 | 4-O-galloylalbiflorin | Capsule | C30H32O15 | 632.571 | 135397096 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| D4 | Albiflorin | Capsule | C23H28O11 | 480.466 | 51346141 | LC-MS/UPLC-ESI-Q-TOF-MS [37], RP-HPLC [52], chromatography on silica gel, Sephdex LH-20 columns and prep-HPLC-NMR [53], HPLC-ESI-Q-TOF/MS [43], HPLC-MS/MS [45] |
| D5 | Benzoylpaeoniflorin/isomer | Capsule | C30H32O12 | 584.574 | 21631106 | LC-MS/UPLC-ESI-Q-TOF-MS [37], chromatography on silica gel, Sephdex LH-20 columns and prep-HPLC-NMR [53], HPLC-ESI-Q-TOF/MS [43] |
| D6 | Benzoylpaeoniflorin sulfate | Capsule | C30H32O14S | 648.63 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| D7 | Desbenzoylalbiflorin/ isomer | Capsule | C16H24O10 | 376.358 | 71452333 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| D8 | Digalloylglucose | Capsule | C20H20O14 | 484.366 | 129628549 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| D9 | Gallic acid | Capsule | C7H6O5 | 170.12 | 370 | LC-MS/UPLC-ESI-Q-TOF-MS [37], RP-HPLC [52], HPLC-ESI-Q-TOF/MS [43], UPLC [41], HPLC-MS/MS [45] |
| D10 | Galloyglucose/isomer | Capsule | C13H16O10 | 332.26 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| D11 | Galloyl paeoniflorin | Capsule | C30H32O15 | 632.571 | 494717 | LC-MS/UPLC-ESI-Q-TOF-MS [37], chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54], HPLC-ESI-QTOF/MS [43] |
| D12 | Galloylpaeoniflorin sulfonate | Capsule | C30H32O17S | 696.63 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| D13 | Hexagalloyl glucose | Capsule | C48H36O30 | 1092.78 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| D14 | Isoxypaeoniflora | Capsule | C23H28O12 | 496.46 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| D15 | Methyl gallate | Capsule | C8H8O5 | 184.147 | 7428 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| D16 | Methyl vanillate | Capsule | C9H10O4 | 182.175 | 19844 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| D17 | Oxypaeoniflorin | Capsule | C23H28O12 | 496.465 | 21631105 | LC-MS/UPLC-ESI-Q-TOF-MS [37], chromatography on silica gel, Sephdex LH-20 columns and prep-HPLC-NMR [53], chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [55] |
| D18 | Pentagalloylglucose | Capsule | C41H32O26 | 940.681 | 65238 | LC-MS/UPLC-ESI-Q-TOF-MS [37], HPLC-ESI-Q-TOF/MS [43] |
| D19 | Tetragalloy glucose | Capsule | C34H28O22 | 788.57 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| D20 | Trigalloy glucose | Capsule | C27H24O18 | 636.47 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| E | Moutan Cortex (n = 20) | |||||
| E1 | 3-hydroxypaeonol | Capsule | C9H10O4 | 182.17 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| E2 | Apiopaeonoside | Capsule | C20H28O12 | 460.432 | 127509 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| E3 | Benzoyloxypaeoniflorin | Capsule | C30H32O13 | 600.573 | 21631107 | LC-MS/UPLC-ESI-Q-TOF-MS [37], HPLC-ESI-Q-TOF/MS [43] |
| E4 | Galloyloxypaeoniflorin | Capsule | C30H32O16 | 648.56 | 3036133 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| E5 | Mudanpioside A | C31H34O13 | 614.6 | 21631101 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54], HPLC-ESI-Q-TOF/MS [43] | |
| E6 | Mudanpioside B | Capsule | C31H34O14 | 630.599 | 21631102 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| E7 | Mudanpioside C | Capsule | C30H32O13 | 600.573 | 21631098 | LC-MS/UPLC-ESI-Q-TOF-MS [37], chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54], HPLC-ESI-QTOF/MS [43] |
| E8 | Mudanpioside D | Capsule | C24H30O12 | 510.492 | 21631103 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| E9 | Mudanpioside E | Capsule | C24H30O13 | 526.491 | 21631104 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| E10 | Mudanpioside E sulfonate | Capsule | C24H30O14S | 574.55 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| E11 | Mudanpioside F | Capsule | C16H24O8 | 344.36 | 21631108 | LC-MS/UPLC-ESI-Q-TOF-MS [37], chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [55] |
| E12 | Mudanpioside H/ isomer | Capsule | C30H32O14 | 616.572 | 71457654 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| E13 | Mudanpioside J | Capsule | C31H34O14 | 630.599 | 21593828 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| E14 | Paeonol | Capsule, pill, tablet | C9H10O3 | 166.176 | 11092 | LC-MS/UPLC-ESI-Q-TOF-MS [37], HPLC [38,39,47,50,51], gas chromatography [56], RP-HPLC [57,58], SPE-HPLC [40], HPLC-ESI-QTOF/MS [43], DGLC [44], UPLC [41], HPLC-MS/MS [45] |
| E15 | Paeonolide | Capsule | C20H28O12 | 460.432 | 442923 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| E16 | Paeonoside | Capsule | C15H20O8 | 328.317 | 53384347 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| E17 | Suffruticoside A | Capsule | C27H32O16 | 612.537 | 9986231 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| E18 | Suffruticoside B | Capsule | C27H32O16 | 612.537 | 10258205 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| E19 | Suffruticoside C | Capsule | C27H32O16 | 612.537 | 10258206 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| E20 | Suffruticoside D | Capsule | C27H32O16 | 612.537 | 5321547 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| F | Paeoniae Radix (n = 10) | |||||
| F1 | 1-O-β-d-glucopyranosyl-paeonisuffrone | Capsule | C16H24O9 | 360.36 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| F2 | 6-O-β-d-glucopyranosyl lactinolide | Capsule | C16H26O9 | 362.37 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| F3 | Albiflorin R1 | Capsule | C23H28O11 | 480.466 | 5317181 (CID), 50163461(SID) | LC-MS/UPLC-ESI-Q-TOF-MS [37], chromatography on silica gel, Sephdex LH-20 columns and prep-HPLC-NMR [53] |
| F4 | Digallic acid | Capsule | C14H10O9 | 322.225 | 341 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| F5 | Ethyl gallate | Capsule | C9H10O5 | 198.174 | 13250 | LC-MS/UPLC-ESI-Q-TOF-MS [37], multiple chromatographic methods [42] |
| F6 | Galloylsucrose/isomer | Capsule | C19H26O15 | 494.402 | 129629059 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| F7 | Isomaltopaeoniflorin sulfonate | Capsule | C29H38O18S | 706.66 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| F8 | Oxypaeoniflorin sulfonate | Capsule | C23H28O14S | 560.523 | 71455848 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| F9 | Paeoniflorin | Capsule, pill, tablet | C23H28O11 | 480.466 | 442534 | LC-MS/UPLC-ESI-Q-TOF-MS [37], HPLC [47,50,51,59,60], RP-HPLC [52], chromatography on silica gel, Sephdex LH-20 columns and prep-HPLC-NMR [53], HPLC-ESI-QTOF/MS [43], DGLC [44], UPLC [41], HPLC-MS/MS [45] |
| F10 | Paeoniflorin sulfonate | Capsule | C23H28O14S | 560.523 | 101382399 | LC-MS/UPLC-ESI-Q-TOF-MS [37], HPLC-ESI-QTOF/MS [43] |
| G | Poria (n = 30) | |||||
| G1 | 16α-Hydroxytrametenolic acid | Capsule | C30H48O4 | 472.71 | 132285301 | LC-MS/UPLC-ESI-Q-TOF-MS [37], UPLC/Q-TOF-MS [61] |
| G2 | 16α-Hydroxydehydrotrametenolic acid | Capsule | C30H46O4 | 470.694 | 10743008 | UPLC/Q-TOF-MS [61] |
| G3 | 2,3,6-Trimethylbenzoic acid | Capsule | C10H12O2 | 164.204 | 17314 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| G4 | 25-Hydroxypachymic acid | Capsule | C33H52O6 | 544.76 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| G5 | 31-Hydroxyl-16-O-acetylpachymic acid | Capsule | C38H52O5 | 588.81 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| G6 | 3-epidehydropachymic acid | Capsule | C33H50O5 | 526.758 | 15226716 | Chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [55], HPLC [62], UPLC/Q-TOF-MS [61] |
| G7 | 3-Epidehydrotumulosic acid | Capsule | C31H48O4 | 484.721 | 10005581 | LC-MS/UPLC-ESI-Q-TOF-MS [37], chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [55], UPLC/Q-TOF-MS [61] |
| G8 | 3-O-acetyl-16α hydroxytrametenolic acid | Capsule | C32H50O5 | 514.747 | 9958136 | LC-MS/UPLC-ESI-Q-TOF-MS [37], UPLC/Q-TOF-MS [61] |
| G9 | 3-O-acetyl-16α-hydroxydehydrotrametenolic acid | Capsule | C32H48O5 | 512.731 | 15226714 | LC-MS/UPLC-ESI-Q-TOF-MS [37], UPLC/Q-TOF-MS [61] |
| G10 | 3-oxo-6,16α-dihydroxy-lanosta-7,9(11),24(31)-trien-21-oic acid | Capsule | C30H44O5 | 484.67 | NF (Figure 2) (structure found in [63]) | UPLC/Q-TOF-MS [61] |
| G11 | 3-oxo-6,16α-dihydroxy-lanosta-8,24-diene-21-oic acid | Capsule | NF | NF | NF (structure not available) | UPLC/Q-TOF-MS [61] |
| G12 | 3β,16α-Dihydroxy-lanosta-7,9(11),24-trien-21-oic acid | Capsule | C30H46O4 | 470.68 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| G13 | 3β-O-p-Hydroxybenzoyl-dehydro tumulosic acid | Capsule | C38H52O6 | 604.828 | 5318155 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| G14 | 6α -Hydroxydehydropachymic acid | Capsule | C33H50O6 | 542.74 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| G15 | Dehydroeburicoic acid | Capsule | C31H48O3 | 468.722 | 15250826 | LC-MS/UPLC-ESI-Q-TOF-MS [37], UPLC-MS/MS [64], UPLC/Q-TOF-MS [61] |
| G16 | Dehydropachymic acid | Capsule | C33H50O5 | 526.758 | 15226717 | LC-MS/UPLC-ESI-Q-TOF-MS [37], UPLC-MS/MS [64], HPLC [62], UPLC/Q-TOF-MS [61] |
| G17 | Dehydrotrametenolic acid | Capsule | C32H48O3 | 480.733 | 129539661 | LC-MS/UPLC-ESI-Q-TOF-MS [37], UPLC-MS/MS [64], UPLC/Q-TOF-MS [61] |
| G18 | Dehydrotumulosic acid | Capsule | C31H48O4 | 484.721 | 15225964 | LC-MS/UPLC-ESI-Q-TOF-MS [37], UPLC-MS/MS [64], chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [55], HPLC [62], UPLC/Q-TOF-MS [61] |
| G19 | Eburicoic acid | Capsule | C31H50O3 | 470.738 | 73402 | LC-MS/UPLC-ESI-Q-TOF-MS [37], UPLC/Q-TOF-MS [61] |
| G20 | Pachymic acid | Capsule | C33H52O5 | 528.774 | 5484385 | LC-MS/UPLC-ESI-Q-TOF-MS [37], UPLC-MS/MS [64], HPLC-MS/MS [45], UPLC/Q-TOF-MS [61] |
| G21 | Pachymic acid methyl ester | Capsule | C34H54O5 | 542.79 | NF (Figure 2) | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| G22 | Polyporenic acid C | Capsule | C31H46O4 | 482.705 | 9805290 | LC-MS/UPLC-ESI-Q-TOF-MS [37], UPLC-MS/MS [64], chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [55], HPLC [62], UPLC/Q-TOF-MS [61] |
| G23 | Poricoic acid A | Capsule | C31H46O5 | 498.704 | 5471851 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| G24 | Poricoic acid AE | Capsule | C33H50O5 | 526.758 | 102480392 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| G25 | Poricoic acid AM | Capsule | C32H48O5 | 512.731 | 46882717 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| G26 | Poricoic acid B | Capsule | C30H44O5 | 484.677 | 5471852 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| G27 | Poricoic acid BM | Capsule | C31H46O5 | 498.704 | 15225967 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| G28 | Poricoic acid C | Capsule | C31H46O4 | 482.705 | 16757534 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| G29 | Poricoic acid DM | Capsule | C32H48O6 | 528.73 | 44424830 | LC-MS/UPLC-ESI-Q-TOF-MS [37] |
| G30 | Tumulosic acid | Capsule | C31H50O4 | 486.737 | 12314446 | LC-MS/UPLC-ESI-Q-TOF-MS [37], UPLC/Q-TOF-MS [61] |
| H | Unclarified (n = 44) | |||||
| H1 | (2R)-[(6-O-β-d-glucopyranosyl-β-d-glucopyranosyl) oxy] (phenyl) ethanoic acid | Capsule | C20H28O13 | 475. 145 | NF (Figure 2) | HPLC-ESI-Q-TOF/MS [43] |
| H2 | 2,5-dihydroxy-4-methylacetophenone | Capsule | C9H10O3 | 166.174 | NF (Figure 2) | Multiple chromatographic methods [42] |
| H3 | 4-o-methylbenzoylpaeoniflorin | Capsule | C31H34O12 | 598.601 | 46883517 | Chromatography on silica gel, Sephdex LH-20 columns and prep-HPLC-NMR [53] |
| H4 | 4-o-methylgalloylpaeoniflorin | Capsule | C31H34O15 | 646.598 | 46883518 | Chromatography on silica gel, Sephdex LH-20 columns and prep-HPLC-NMR [53] |
| H5 | Adenosine | Capsule | C10H13N5O4 | 267.245 | 60961 | Chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [55] |
| H6 | Affinoside | Capsule | C20H28O12 | 460.432 | 11972427 | Multiple chromatographic methods [42] |
| H7 | Alanine | Capsule | C3H7NO2 | 89.094 | 5950 | Chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [55] |
| H8 | A-Amyrin acetate | Capsule | C32H52O2 | 468.766 | 92842 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H9 | A-D-Glucose | Capsule | C6H12O6 | 180.156 | 79025 | Chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [56] |
| H10 | Apigenin | Capsule | C15H10O5 | 270.24 | 5280443 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H11 | Arginine | Capsule | C6H14N4O2 | 174.204 | 6322 | Chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [56] |
| H12 | Astragalin | Capsule | C21H20O11 | 448.38 | 5282102 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H13 | Benzoic acid | Capsule | C7H6O2 | 122.123 | 243 | HPLC-ESI-QTOF/MS [43], UPLC [41] |
| H14 | Benzoylpaeoniflorin | Capsule | C30H32O12 | 584.574 | 21631106 | HPLC-ESI-QTOF/MS [43], UPLC [41] |
| H15 | Benzyl-β-D-glucopyranosyl-(1→6)-β-D-glucopyranoside | Capsule | C18H26O10 | 402.39 | NF (Figure 2) | Multiple chromatographic methods [42] |
| H16 | Β-Amyrin acetate | Capsule | C32H52O2 | 468.766 | 92156 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H17 | Caffeic acid | Capsule | C9H8O4 | 180.159 | 689043 | Chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [55] |
| H18 | Campesterol | Capsule | C28H48O | 400.691 | 173183 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H19 | Catechin | Capsule | C15H14O6 | 290.271 | 9064 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H20 | Cinnamyl alcohol | Capsule | C9H10O | 134.178 | 5315892 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H21 | Coumarin | Capsule | C9H6O2 | 146.145 | 323 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H22 | Epicatechin | Capsule | C15H14O6 | 290.271 | 72276 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H23 | Ergosta-4, 6, 8 (14), 22-tetraen-3-one | Capsule | C28H40O | 392.627 | 6441416 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H24 | Ergosterol | Capsule | C28H44O | 396.659 | 444679 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H25 | Galactitol | Capsule | C6H14O6 | 182.172 | 11850 | Chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [55] |
| H26 | Guanosine | Capsule | C10H13N5O5 | 283.244 | 6802 | Chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [55] |
| H27 | Heneicosanoic acid | Capsule | C21H42O2 | 326.565 | 16898 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H28 | Hyperoside | Capsule | C21H20O12 | 464.379 | 5281643 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H29 | Isomaltopaeoniflorin | Capsule | C29H38O16 | 642.607 | 101001429 | Chromatography on silica gel, Sephdex LH-20 columns and prep-HPLC-NMR [53] |
| H30 | Kaemferol | Capsule | C15H10O6 | 286.239 | 5280863 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H31 | Leucine | Capsule | C6H13NO2 | 131.175 | 6106 | Chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [55] |
| H32 | O-β-D-Gentiobiosyl-d-(−)-mandelamide | Capsule | C20H29NO12 | 498. 158 | 181802 | HPLC-ESI-QTOF/MS [43] |
| H33 | Paeonidanin A | Capsule | C31H34O12 | 598.601 | 44253993 | Chromatography on silica gel, Sephdex LH-20 columns and prep-HPLC-NMR [53] |
| H34 | Paeonidanin B | Capsule | C31H34O15 | 646.598 | 102417825 | Chromatography on silica gel, Sephdex LH-20 columns and prep-HPLC-NMR [53] |
| H35 | Paeoniflorin B | Capsule | C36H42O17 | 746.715 | 71452334 | Chromatography on silica gel, Sephdex LH-20 columns and prep-HPLC-NMR [53] |
| H36 | P-Coumaric acid | Capsule | C9H8O3 | 164.16 | 637542 | Multiple chromatographic methods [42] |
| H37 | Proline | Capsule | C5H9NO2 | 115.132 | 145742 | Chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [55] |
| H38 | Quercetin | Capsule | C15H10O7 | 302.238 | 5280343 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H39 | Syringaresinol | Capsule | C22H26O8 | 418.442 | 443023 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H40 | Syringic acid | Capsule | C9H10O5 | 198.174 | 10742 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54], HPLC-ESI-QTOF/MS [43] |
| H41 | Trans-2-Methoxycinnamic acid | Capsule | C10H10O3 | 178.187 | 734154 | Multiple chromatographic methods [42] |
| H42 | Trehalose | Capsule | C12H22O11 | 342.297 | 7427 | Chromatography on silica gel, Sephdex LH-20 columns, D-101 macroporous resin column, and reverse RP-18 column and HPLC-NMR/MS [55] |
| H43 | Umbelliferone | Capsule | C9H6O3 | 162.144 | 5281426 | Chromatography on silica gel and polydextran gel columns and prep-HPLC-NMR/MS [54] |
| H44 | Vanillic acid | Capsule | C8H8O4 | 168.148 | 8468 | Multiple chromatographic methods [42] |
| J | Inorganic Elements (n = 29) | |||||
| J1 | Aluminum | Capsule | Al | 26.982 | 5359268 | ICP-MS [65] |
| J2 | Arsenic | Capsule | As | 74.922 | 5359596 | ICP-MS [65] |
| J3 | Boron | Capsule | B | 10.81 | 5462311 | ICP-MS [65] |
| J4 | Barium | Capsule | Ba | 137.327 | 5355457 | ICP-MS [65] |
| J5 | Beryllium | Capsule | Be | 9.012 | 5460467 | ICP-MS [65] |
| J6 | Bismuth | Capsule | Bi | 208.98 | 5359367 | ICP-MS [65] |
| J7 | Calcium | Capsule | Ca | 40.078 | 5460341 | ICP-MS [65] |
| J8 | Cadmium | Capsule | Cd | 112.414 | 23973 | ICP-MS [65] |
| J9 | Cobalt | Capsule | Co | 58.933 | 104730 | ICP-MS [65] |
| J10 | Chromium | Capsule | Cr | 51.996 | 23976 | ICP-MS [65] |
| J11 | Copper | Capsule | Cu | 63.546 | 23978 | ICP-MS [65] |
| J12 | Iron | Capsule | Fe | 55.845 | 23925 | ICP-MS [65] |
| J13 | Gallium | Capsule | Ga | 69.723 | 5360835 | ICP-MS [65] |
| J14 | Mercury | Capsule | Hg | 200.592 | 23931 | ICP-MS [65] |
| J15 | Lithium | Capsule | Li | 6.94 | 3028194 | ICP-MS [65] |
| J16 | Magnesium | Capsule | Mg | 24.305 | 5462224 | ICP-MS [65] |
| J17 | Manganese | Capsule | Mn | 54.938 | 23930 | ICP-MS [65] |
| J18 | Molybdenum | Capsule | Mo | 95.95 | 23932 | ICP-MS [65] |
| J19 | Sodium | Capsule | Na | 22.99 | 5360545 | ICP-MS [65] |
| J20 | Nickel | Capsule | Ni | 58.693 | 935 | ICP-MS [65] |
| J21 | Lead | Capsule | Pb | 207.2 | 5352425 | ICP-MS [65] |
| J22 | Antimony | Capsule | Sb | 121.76 | 5354495 | ICP-MS [65] |
| J23 | Selenium | Capsule | Se | 78.971 | 6326970 | ICP-MS [65] |
| J24 | Tin | Capsule | Sn | 118.71 | 5352426 | ICP-MS [65] |
| J25 | Strontium | Capsule | Sr | 87.62 | 5359327 | ICP-MS [65] |
| J26 | Titanium | Capsule | Ti | 47.867 | 23963 | ICP-MS [65] |
| J27 | Thallium | Capsule | Tl | 204.38 | 5359464 | ICP-MS [65] |
| J28 | Vanadium | Capsule | V | 50.941 | 23990 | ICP-MS [65] |
| J29 | Zinc | Capsule | Zn | 65.38 | 23994 | ICP-MS [65] |
Notes: CID: compound identification number; DGLC: dual gradient liquid chromatography; ESI: electrospray ionization; ICP: inductively coupled plasma; LC: liquid chromatography; MS: mass spectrometry; NF: Not found; NMR: nuclear magnetic resonance spectroscopy; Q: quadrupole; RP: reverse phase; SID: substance identification number; SPE: solid-phase extraction; TOF: time of flight; UPLC: ultra performance liquid chromatography. Corresponding molecular structures refer to PubChem and Figure 2.
Table 3.
Characteristics of in vivo studies.
| Study ID | Language; Location | Model | Inducer | Age (week) | Weight (g) | Experiments | Sample Size | Interventions (Daily Dose, Administration) | Duration (days) | Included Outcome Measure and Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Noguchi et al., 2003 a [66] | English, Japan | Sprague-Dawley rats | OVX, capsaicin (1 mg/kg, i.p.) injection | 10 | 200–250 | 1 | 32 (8/8/8/8) | 1. E2 (0.010 mg/kg, s.c.); 2. GFW (1000mg/kg, p.o.); 3. Distilled water (10 mL/kg, p.o.) to OVX rats; 4. Distilled water (10 mL/kg, p.o.) to sham-operated rats. | 7 | CGRP concentrations in plasma ↑ (restore) |
| OVX | 2 | 27 (7/7/7/7) | CGRP concentrations in the spinal cord and dorsal root ganglia (no sig) | |||||||
| 3 | 20 (5/5/5/5) | CGRP mRNA levels in dorsal root ganglia (no sig) | ||||||||
| Noguchi et al., 2003 b [67] | English, Japan | Sprague-Dawley rats | OVX | 10 | 200–250 | 4 | NS | 1. GFW (100, 300, or 1000 mg/10 mL per kg, p.o., n = 7 or 8 in each group); 2. E2 (0.010 mg/mL per kg, s.c., n = 7); 3. Distilled water (10 mg/kg, p.o., n = 8) to OVX rats; 4. GFW (1000 mg/10 mL per kg, p.o., n = 8) to sham-operated rats. | 7 | CGRP-induced elevation of skin temperature ↓ |
| 5 | 45 (11/13/12/9) | 1. GFW (1000 mg/10 mL per kg, p.o.); 2. E2 (0.010 mg/mL per kg, s.c.); 3. Distilled water (10 mL/kg, p.o.) to OVX rats; 4. Distilled water (10 mL/kg, p.o.) to sham-operated rats. | CGRP-induced relaxation of Prostaglandin F2α-induced vasoconstriction in isolated mesenteric vascular beds ↓ | |||||||
| 6 | 32 (8/8/8/8) | 125I-CGRP binding in isolated mesenteric arteries ↓ | ||||||||
| 7 | 38 (10/9/10/9) | Plasma concentration of CGRP ↑ | ||||||||
| 8 | 29 (7/7/8/7) | Plasma concentration of E2 (no sig); uterine weight (no sig) | ||||||||
| Noguchi et al., 2005 [68] | English, Japan | Sprague-Dawley rats | GnRH analog Leupline (1 mg/kg) injection | 9 | 200–240 | 9 | 36 (6/6/5/7/7/5) | 1. GFW (100 mg/kg, p.o.); 2. GFW (300 mg/kg, p.o.); 3. GFW (1,000 mg/kg, p.o.); 4. E2 (0.010 mg/kg, s.c.); 5. Distilled water (10 mL/kg, p.o.) to injected rats; 6. Distilled water (10 mL/kg, p.o.) to sham-injected rats. | 14 | CGRP-induced elevation of skin temperature ↓ |
| 52 (13/13/13/13) | 1. GFW (1000 mg/kg, p.o.); 2. E2 (0.010 mg/kg, s.c.); 3. Distilled water (10 mL/kg, p.o.) to injected rats; 4. Distilled water (10 mL/kg, p.o.) to sham-injected rats. | Plasma concentration of CGRP ↑ | ||||||||
| 28 (8/7/7/6) | Pituitary LH and FSH, plasma E2 and weights of uterus and ovaries (no sig) |
Notes: ↑: increased; ↓: decreased; CGRP: calcitonin gene-related peptide; E2: estradiol; FSH: follicle-stimulating hormone; GFW: Guizhi Fuling Wan; GnRH: gonadotropin-releasing hormone; i.p.: intraperitoneal injection; LH: luteinizing hormone; NS: not specified; OVX: ovariectomized; p.o.: oral administration; s.c.: subcutaneous injection; sig: significance.
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Li, M.; Hung, A.; Li, H.; Yang, A.W.H. A Classic Herbal Formula Guizhi Fuling Wan for Menopausal Hot Flushes: From Experimental Findings to Clinical Applications. Biomedicines 2019, 7, 60. https://doi.org/10.3390/biomedicines7030060
AMA Style
Li M, Hung A, Li H, Yang AWH. A Classic Herbal Formula Guizhi Fuling Wan for Menopausal Hot Flushes: From Experimental Findings to Clinical Applications. Biomedicines. 2019; 7(3):60. https://doi.org/10.3390/biomedicines7030060
Chicago/Turabian StyleLi, Mingdi, Andrew Hung, Hong Li, and Angela Wei Hong Yang. 2019. "A Classic Herbal Formula Guizhi Fuling Wan for Menopausal Hot Flushes: From Experimental Findings to Clinical Applications" Biomedicines 7, no. 3: 60. https://doi.org/10.3390/biomedicines7030060
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.