Stereotactic Body Radiation Therapy in the Management of Upper GI Malignancies

Penn State Health Milton S. Hershey Medical Center, Hershey, PA 17033, USA
*
Author to whom correspondence should be addressed.
Biomedicines 2018, 6(1), 7; https://doi.org/10.3390/biomedicines6010007
Submission received: 8 November 2017
/
Revised: 21 December 2017
/
Accepted: 23 December 2017
/
Published: 3 January 2018
(This article belongs to the Special Issue Cancer Biomarkers and Targets in Digestive Organs)
Abstract
:The role of external beam radiation therapy (EBRT) in the management of upper gastrointestinal malignancies is constantly evolving. As radiation therapy techniques improve and are able to deliver more ablative doses of radiotherapy while sparing healthy tissue, radiation can be applied to a wider range of clinical scenarios. Stereotactic body radiation therapy (SBRT) allows a high dose of radiation to be delivered to a highly conformal treatment volume in a short amount of time. Another potential advantage of SBRT is its ability to increase tumor immunogenicity, while also having less of an immunosuppressive effect on the patient, as compared to conventionally fractionated radiation therapy. In so doing, SBRT may potentiate the effects of immune therapy when the two treatments are combined, thus improving therapeutic outcomes. This article provides an overview of the role of SBRT in the management of upper gastrointestinal GI malignancies and the emerging data on immune biomarkers and SBRT, with a focus on pancreatic and liver cancer.
{kind=link}
1. Introduction
The role of external beam radiation therapy in the management of upper gastrointestinal (GI) malignancies is constantly evolving. Surgery has historically been the cornerstone of treatment for a majority of these cancers, particularly for pancreatic and hepatobiliary malignancies, with radiation reserved for palliation of symptoms. However, as radiation therapy techniques improve and are able to deliver more ablative doses of radiotherapy while sparing healthy tissue, radiation can be applied to a wider range of clinical scenarios.
Stereotactic body radiation therapy (SBRT) is a technique that allows a high dose of radiation to be delivered to a highly conformal treatment volume in a short amount of time. This results in a number of advantages. First, it allows for treatment of a higher biologically effective dose (BED), thus improving local tumor control. Second, it allows for a shorter overall treatment time which is both more convenient for patients and treating facilities and, more importantly, prevents delays in systemic treatment and/or surgery. Finally, given the highly conformal nature of SBRT, it allows for increased sparing of adjacent organs at risk (OARs) [1]. While the role of SBRT in the treatment of organs organized in series, such as the esophagus, is not well defined, its use in treating those organized in parallel, such as the liver and pancreas, has been established. This article therefore seeks to review the role of SBRT in the management of upper GI malignancies with a focus on pancreatic and liver cancer.
Another potential advantage of SBRT is its ability to increase tumor immunogenicity while having less of an immunosuppressive effect on the patient, as compared to conventionally fractionated radiation therapy [2]. In so doing, SBRT may potentiate the effects of immune therapy when the two treatments are combined, thus improving therapeutic outcomes. While the available data on tumor biomarkers and SBRT is in its infancy, it is hypothesis-generating and will also be reviewed in this article.
2. SBRT for Pancreatic Cancer
Pancreatic cancer is the 4th leading cause of cancer death in the United States [2]. Currently, surgery is considered the only curative treatment; however, less than 20% of patients are operable at the time of diagnosis [3,4]. Radiation therapy, therefore, plays a role in both the preoperative and definitive management of pancreatic malignancies. However, because the pancreas is considered to be radio-resistant, higher radiation doses are required for tumor control [5]. Indeed, studies have shown that delivering a BED of greater than 70 Gy is associated with improved survival for pancreatic cancer [6]. This poses a challenge for standard radiotherapy treatment planning due to the close proximity of highly radiosensitive organs such as the liver, duodenum, and stomach. SBRT in the management of pancreatic cancer is therefore a highly appealing treatment modality which has been well studied [7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27].
2.1. The Neoadjuvant Setting
The close proximity of the pancreas to critical vascular structures makes it technically challenging to achieve microscopically negative (R0) resections. The presence of positive margins following resection is associated with inferior outcomes [27,28,29,30,31]. Radiation therapy has, therefore, been used in the preoperative setting to downsize tumors intimately associated with vascular structures so as to increase the rate of negative margins at the time of surgery. Given the advantages of SBRT outlined above, there is growing interest in utilizing this technique in the neoadjuvant setting.
In 2015, the Moffitt Center published its experience with SBRT for borderline resectable pancreatic cancer [32]. This was a retrospective institutional review of all patients treated neoadjuvantly with SBRT at their institution. It included 159 patients, the majority of which (110) had borderline resectable disease (BRPC), with the remaining patients (49) having locally advanced unresectable pancreatic cancer (LAPC). Patients were treated with multi-agent systemic chemotherapy, followed by SBRT to a median dose of 40 Gy in five fractions and then surgery in patients who were deemed resectable after neoadjuvant therapy.
Ultimately, 51% of BRPC and 10% of LAPC patients were able to undergo surgery. The R0 resection rate in these patients was 96% and 100%, respectively. Seven percent of patients had a pathologic complete response and none of these patients relapsed at a median follow-up of 14 months. The overall survival and progression free survival rates were 19 months and 12 months, respectively, for those with BRPC, and 15 months and 13 months, respectively, for those with LAPC. Remarkably, the overall survival rate for patients who received neoadjuvant treatment and were then able to undergo surgery was 34 months, versus only 14 months for those who received chemotherapy and radiation but remained unresectable. Overall survival rates for up-front resectable pancreatic cancer patients, historically thought to have the best survival outcomes, has not exceeded 30 months in national randomized controlled trials, including the recently published ESPAC-4 trial [33,34,35,36,37,38,39,40]. Treatment was well tolerated in only 7% of cases with Grade 3+ acute or late toxicity. The results of this study were hypothesis-generating and paved the way for prospective trials of neoadjuvant SBRT for borderline resectable pancreatic cancer, including the ongoing ALLIANCE (NCT01992705) and Pancreatic Cancer Research Study (NCT01926197).
2.2. The Definitive Setting
There have been a number of studies investigating the role of SBRT in the definitive setting [10,12,13,14,16,17,21,22,23,24,25,26]. Most of these were retrospective series and only two were Phase II studies. The first of these two Phase II studies was published by Hoyer et al. in 2005 [16]. It included 22 patients with T1-3N0 LAPC deemed unresectable by a surgeon measuring up to 6 cm in size. The median PTV volume was 136 cm3. Patients were treated with SBRT to a total dose of 45 Gy in three fractions. There was no mention of chemotherapy in the trial or a requirement that patients also undergo systemic chemotherapy. Study results were disappointing with only a 57% local control rate at one year and a median survival of 5.4 months. The toxicity profile was unfavorable with 36% of patients experiencing an increase in pain and analgesic use, 23% of patients with severe mucositis or ulceration, and one gastric perforation requiring emergent surgery. There are a number of reasons why this early experience with SBRT yielded such poor outcomes. These include a lack of fiducials for daily set-up and target localization possibly resulting in tumor miss, a lack of OAR constraints, resulting in high toxicity rates, and no specific requirements for systemic chemotherapy in conjunction with SBRT either before or after treatment, which we know today is a key component of treatment for patients with both resectable and especially unresectable disease.
Ten years after the publication of the Hoyer study, Herman et al. published their Phase II trial of SBRT for unresectable pancreatic cancer [21]. In this study, 49 patients with LAPC were treated with three weeks of gemcitabine, followed by a one-week break, followed by SBRT to the tumor to a total dose of 33 Gy in five fractions. The study included 49 patients with a median PTV volume of 71.4 cm3. Unlike its predecessor study, the results of this trial were encouraging. The freedom from local progression at one year was 78% at one year as compared to 57% in the Moyer study. The median progression free survival was 7.8 months and the median overall survival was 13.9 months—a significant improvement from 5.4 months as reported in the Moyer trial. Ten percent of patients were ultimately able to undergo surgery after completion of SBRT. Overall survival for these patients ranged from 13.6 to 40.2 months. The primary endpoint of the rate of late (>3 months after SBRT) gastritis, fistula, enteritis, or ulcers of Grade 2+ was only seen in 11% of patients.
The superior outcomes reported in the Herman et al. trial as compared to the earlier Moyer trial can be attributed to a number of factors. First, unlike in the Herman trial, and all ongoing protocols, fiducial markers were not required to ensure accurate tumor positioning, which may have led to tumor miss. Second, there was no requirement for gemcitabine-based systemic chemotherapy, unlike in the more recent study, which has been shown to improve survival in patients with locally advanced disease [41,42,43]. Furthermore, the Moyer trial did not specify OAR constraints, which likely explains the poor toxicity profile. Lastly, tumor margins were large (5 mm axially and 1 cm cranio-caudal) and there was no dose reduction for overlap with the duodenum and stomach as was done in the Herman trial, which likely explains the 20% rate of severe mucositis and ulceration and the case of gastric perforation requiring surgery.
As radiation techniques have improved and we have learned more about tissue tolerance for high dose radiation therapy, SBRT has emerged as an appealing and highly effective treatment modality for LAPC. A meta-analysis of 19 trials of SBRT for LAPC published in 2017 showed that the median overall survival was greater than 12 months in the vast majority of studies and was particularly favorable in the subset of patients who became resectable after receiving SBRT [20]. These studies have paved the way for randomized Phase III trials (NCT01926197), which will hopefully establish the role of SBRT for LAPC.
2.3. The Adjuvant Setting
SBRT in the adjuvant setting for resected pancreatic cancer has not been established. However, there is an ongoing Phase II study examining the role of SBRT in resected T3 and N1 patients, which is currently accruing (NCT02461836).
3. SBRT for Hepatocellular Cancer
Hepatocellular carcinoma (HCC) is the second leading cause of cancer death worldwide [44]. The incidence of HCC is approximately equal to the mortality rate, highlighting the aggressive nature of this fatal malignancy. While relatively uncommon in the Unites States (US), it is the fastest growing cause of cancer death in the US [45]. Like with pancreatic cancer, surgery is considered the only curative treatment but most patients either have unresectable disease due to tumor extent or are inoperable due to underlying liver dysfunction. For the latter group of patients, transplant is the ultimate goal because it can cure both the HCC and the underlying liver disease. However, given the limited supply of healthy livers available for transplant, most patients are unable to undergo the procedure right away, thus requiring local treatment as a bridge to liver transplant when an organ becomes available. SBRT for HCC is, therefore, emerging as a safe and effective treatment modality both in the definitive setting for unresectable cancers and as a bridge to transplant for those with underlying liver disease awaiting organ allocation.
Historically, EBRT has been used with caution in the management of hepatic malignancies due to the low tolerance of the liver for radiation [45]. The challenges facing EBRT for HCC have been delivering a sufficiently high dose of radiation to achieve tumor control in an organ that is highly sensitive to radiation and that moves substantially with breathing, making target localization very difficult. Modern-day SBRT techniques make it possible for external beam radiation to overcome these road-blocks by delivering high doses of radiation in a very conformal manner while accounting, and controlling, for tumor motion. Due to a lack of Level I evidence, SBRT is not currently considered a standard treatment for HCC; however, a number of prospective trials have been completed which show its safety and efficacy in the management of this disease [46,47,48,49,50].
The most notable of these prospective trials was a combined analysis of sequential Phase I and II trials conducted at Princess Margaret Hospital published in 2013 [48]. The study included 102 patients with Child–Turcotte–Pugh Class A disease who were unsuitable for other local liver-directed therapy. Median gross tumor volume was 117 mL with a range of 1.3–1913.4 mL. Patients were treated with 30–54 Gy in six fractions, delivered every other day. The treatment was relatively well-tolerated with Grade 3+ toxicity reported in 30% of cases. Local control at one year was 87% and overall survival was 55%.
SBRT has also been combined with trans-arterial chemo-embolization (TACE) with favorable outcomes in the literature so far. There are a number of advantages to combining SBRT with TACE. TACE can shrink tumors, thus creating a smaller treatment volume for SBRT. The combination of the two treatments allows for ablation of vascular components of the tumor with TACE, while the poorly vascularized, necrotic portions can be targeted by SBRT. Finally, SBRT can be used to recanalize tumors with arterial or portal vein thromboses, rendering TACE more effective. A retrospective study of patients with tumors ≥3 cm compared outcomes among patients who received TACE plus SBRT compared to TACE alone [51]. The authors found that, after censoring for liver transplantation, overall survival was significantly better with TACE plus SBRT compared to TACE alone (33 vs. 20 months, respectively).
In conclusion, modern-day SBRT techniques allow for safe and effective delivery of external beam radiation therapy for hepatocellular carcinoma. While more data is needed, available evidence shows that there is a role for radiation in the management of this disease. Specifically, radiation plays a role for lesions unsuitable for other local therapies, for larger lesions in which TACE is less effective, and in cases with portal vein thrombosis in which other therapies are contra-indicated or ineffective [52]. Indeed, there is a randomized Phase III study underway comparing treatment with Sorafenib with or without SBRT in patients with HCC (NCT01730937).
4. SBRT and Immunomodulatory Biomarkers in Upper GI Malignancies and Therapeutic Implications
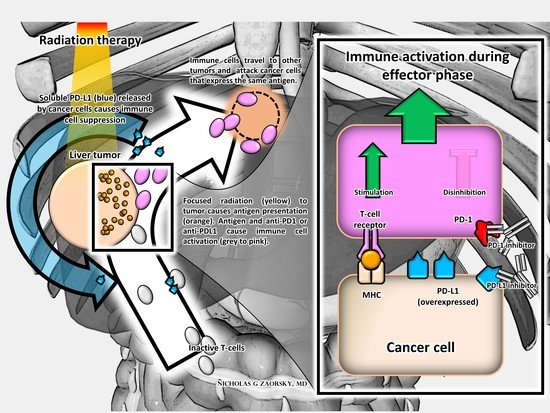
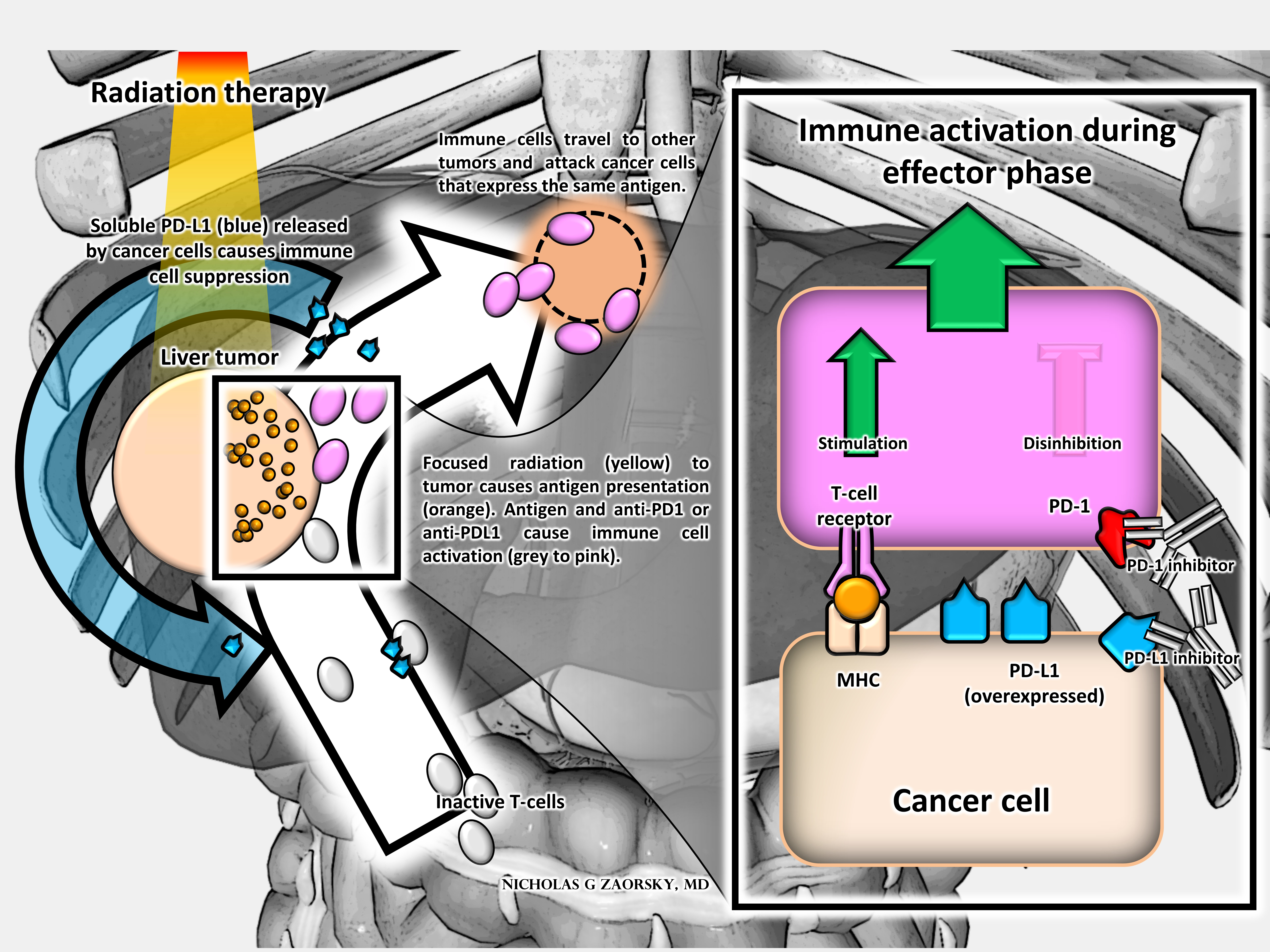
In addition to allowing for higher doses of radiation to be delivered to a more precise target in a shorter treatment time, emerging data shows that radiation, specifically SBRT, has advantageous effects on the immune system, which may have therapeutic implications. The immune-stimulatory effects of radiation have been known for some time. Indeed, Demaria et al. first introduced the concept of radiation as an “in situ vaccine” in 2004 [53]. The authors suggest that radiation turns the radiated tumor into a vaccine by priming the immune system to target cancer cells in other sites in addition to treating the disease locally, a concept known as the abscopal effect. Since then, Formenti and colleagues have been able to site clinical data lending credence to this concept in which radiation delivered locally results in tumor response at the site of radiation as well as decreased tumor burden outside the irradiated field, mediated by the patient’s immune system [54,55,56,57].
While the dose and fractionation needed to optimally prime the immune system is not yet known, SBRT appears to be superior to conventional radiation in terms of its effect on tumor immunogenicity. First, SBRT creates less of an immunosuppressive effect on the host’s immune system as compared to conventionally fractionated radiation, both due to the absence of the concomitant chemotherapy and to the relatively smaller volume of irradiated bone marrow [58,59,60]. In addition, emerging data shows that SBRT has the potential advantage of directly increasing tumor immunogenicity [2,61]. Indeed, numerous pre-clinical models summarized very nicely by Popp et al. have shown that SBRT induces complex changes in the tumor microenvironment [53]. The authors review several preclinical studies showing that SBRT leads to increased recruitment of immune cells, including antigen-presenting-cells and dendritic cells, as well as cytokines and chemokines, which are all involved in the immune response [53]. The authors also summarize existing clinical data demonstrating evidence that SBRT mediates the abscopal effect. However, most of the data they cite involves patients with either melanoma or lung cancer, for which the benefit of immunotherapeutic agents is already widely established [62,63,64].
There is limited clinical data addressing the role of SBRT and its effects on the immune system for gastrointestinal malignancies; however, studies are emerging. Specifically, studies have shown an increase in tumor infiltrating lymphocytes and in soluble PD-L1, involved in T-cell regulatory pathways, following SBRT in pancreatic and hepatic malignancies [61,65]. The immunogenic effect of SBRT on tumors, coupled with the absence of an immunosuppressive effect on the patient, may allow for novel therapeutic approaches to treating upper GI malignancies by combining SBRT with immunotherapy. The combination of these two therapies may be more effective than either treatment alone.
Tumors have varying degrees of immune activity based on their histology. The tumor environment in pancreatic cancer, for instance, is considered to be immunosuppressive with a low degree of infiltration by T cells [66]. As a result, immunotherapy with immune check-point inhibitors has been investigated in this disease, with disappointing results [67,68]. As Foley et al. detail in their paper on immunotherapy for pancreatic cancer, removing immune suppression without providing a means to activate the immune system is likely responsible for these disappointing outcomes [66].
Emerging data show that SBRT has more of an immunogenic effect on the tumor environment when compared to conventionally fractionated radiation therapy delivered concurrently with chemotherapy for pancreatic cancer. In a recent presentation at the American Society for Radiation Oncology (ASTRO) annual meeting, Chen et al. presented their data on tumor infiltrating cells in pancreatic cancer [65]. They showed that there was a statistically significant difference in the ratio of CD8 T-cells to FOXP3 T-regulatory cells (CD8/FOXP3) detected in tumor cells following SBRT as compared to conventionally fractionated therapy. They also showed that a higher CD8/FOXP3 ratio was associated with improved progression free survival. The authors thus show that SBRT may be more effective in terms of local control as compared to conventional fractionation, in addition to showing that SBRT is more immunogenic than conventional radiation. The combination of SBRT and immunotherapy may, therefore, provide novel therapeutic strategies for this disease. Indeed, there are studies underway looking at the efficacy of combining SBRT with immunotherapy in the treatment of pancreatic cancer (NCT 02648282).
Hepatocellular carcinoma, on the other hand, has been shown to be an immune active malignancy with a high infiltration of T cells [66]. Kim et al. recently presented their data on the effects of radiation on soluble PD-L1 in hepatocellular carcinoma and its therapeutic implications [61]. The authors showed that radiation therapy increases the expression of PD-L1 on tumor cells. This increase was noted both after conventionally fractionated radiation and after SBRT; however, the levels after SBRT continued to rise one month following treatment, which was not true following conventionally fractionated radiation. The authors conclude that this data may provide evidence for a novel therapeutic strategy for patients with HCC that combines SBRT with PD-L1 blockade.
5. Conclusions and Future Directions
SBRT has emerged as a highly promising treatment modality in the management of upper GI malignancies. It allows for more curative doses of radiation to be delivered to a highly conformal treatment volume, in a short amount of time, allowing for effective and expedited treatment for these highly aggressive malignancies.
In the case of pancreatic cancer, SBRT has emerged as an effective neoadjuvant treatment to render tumors which are unresectable upfront, resectable after treatment, thus allowing an increased number of patients to undergo potentially curative resection. In the case of LAPC, SBRT also has the potential advantage of rendering some of these initially unresectable tumors resectable, while also providing reasonable long-term survival rates for patients undergoing definitive treatment. Studies are ongoing for SBRT in the adjuvant setting. In the case of HCC, SBRT has emerged as an effective treatment for patients in which other local therapies either cannot be performed or are ineffective as, for example, for large tumors or those with portal venous invasion.
Finally, the effects of SBRT on the immune system and tumor micro-environment is an area of active research with heretofore promising results. Emerging data shows that SBRT can increase tumor immunogenicity, thus providing a rationale for novel therapeutic approaches combining SBRT and immunotherapeutic agents with the hope that the combination of the two treatments will result in better outcomes than either treatment alone. More data is needed to confirm these initial findings. Prospective trials studying the combination of SBRT and immunotherapy in the management of upper GI malignancies are needed to confirm the therapeutic implications of these retrospective studies, and some are already underway.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rosati, L.M.; Kumar, R.; Herman, J.M. Integration of Stereotactic Body Radiation Therapy into the Multidisciplinary Management of Pancreatic Cancer. Semin. Radiat. Oncol. 2017, 27, 256–267. [Google Scholar] [CrossRef] [PubMed]
- Gustafson, M.P.; Bornschlegl, S.; Park, S.S.; Gastineau, D.A.; Roberts, L.R.; Dietz, A.B.; Hallemeier, C.L. Comprehensive assessment of circulating immune cell populations in response to stereotactic body radiation therapy in patients with liver cancer. Adv. Radiat. Oncol. 2017, 2, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Wolfgang, C.L.; Herman, J.M.; Laheru, D.A.; Klein, A.P.; Erdek, M.A.; Fishman, E.K.; Hruban, R.H. Recent progress in pancreatic cancer. CA Cancer J. Clin. 2013, 63, 318–348. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Seshacharyulu, P.; Baine, M.J.; Souchek, J.J.; Menning, M.; Kaur, S.; Yan, Y.; Ouellette, M.M.; Jain, M.; Lin, C.; Batra, S.K. Biological determinants of radioresistance and their remediation in pancreatic cancer. Biochim. Biophys. Acta Rev. Cancer 2017, 1868, 69–92. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, S.; Chadha, A.S.; Suh, Y.; Chen, H.C.; Rao, A.; Das, P. Focal Radiation therapy dose escalation improves overall survival in locally advanced pancreatic cancer patients receiving induction chemotherapy and consolidative chemoradiation. Int. J. Radiat. Oncol. 2016, 94, 755–765. [Google Scholar] [CrossRef] [PubMed]
- Su, T.-S.; Liang, P.; Lu, H.-Z.; Liang, J.-N.; Liu, J.-M.; Zhou, Y.; Gao, Y.-C.; Tang, M.-Y. Stereotactic body radiotherapy using CyberKnife for locally advanced unresectable and metastatic pancreatic cancer. World J. Gastroenterol. 2015, 21, 8156. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Yuan, Z.; Li, F.; Dong, Y.; Zhuang, H.; Wang, J.; Chen, H.; Wang, P. Analysis of clinical efficacy of CyberKnife® treatment for locally advanced pancreatic cancer. Onco Targets Ther. 2015, 8, 1427. [Google Scholar] [CrossRef] [PubMed]
- Moningi, S.; Dholakia, A.S.; Raman, S.P.; Blackford, A.; Cameron, J.L.; Le, D.T.; De Jesus-Acosta, A.M.C.; Hacker-Prietz, A.; Rosati, L.M.; Assadi, R.K.; et al. The role of stereotactic body radiation therapy for pancreatic cancer: A single-institution experience. Ann. Surg. Oncol. 2015, 22, 2352–2358. [Google Scholar] [CrossRef] [PubMed]
- Rwigema, J.-C.M.; Parikh, S.D.; Heron, D.E.; Howell, M.; Zeh, H.; Moser, A.J.; Bahary, N.; Quinn, A.; Burton, S.A. Stereotactic body radiotherapy in the treatment of advanced adenocarcinoma of the pancreas. Am. J. Clin. Oncol. 2011, 34, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, M.S.; Heron, D.E.; Wegner, R.E.; Zeh, H.J.; Bahary, N.; Krasinskas, A.M.; Lembersky, B.; Brand, R.; Moser, A.J.; Quinn, A.E.; et al. Pathologic response with neoadjuvant chemotherapy and stereotactic body radiotherapy for borderline resectable and locally-advanced pancreatic cancer. Radiat. Oncol. 2013, 8, 254. [Google Scholar] [CrossRef] [PubMed]
- Polistina, F.; Costantin, G.; Casamassima, F.; Francescon, P.; Guglielmi, R.; Panizzoni, G.; Febbraro, A.; Ambrosino, G. Unresectable Locally Advanced Pancreatic Cancer: A Multimodal Treatment Using Neoadjuvant Chemoradiotherapy (Gemcitabine Plus Stereotactic Radiosurgery) and Subsequent Surgical Exploration. Ann. Surg. Oncol. 2010, 17, 2092–2101. [Google Scholar] [CrossRef] [PubMed]
- Mahadevan, A.; Miksad, R.; Goldstein, M.; Sullivan, R.; Bullock, A.; Buchbinder, E.; Pleskow, D.; Sawhney, M.; Kent, T.; Vollmer, C.; et al. Induction Gemcitabine and Stereotactic Body Radiotherapy for Locally Advanced Nonmetastatic Pancreas Cancer. Int. J. Radiat. Oncol. 2011, 81, e615–e622. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-C.; Jen, Y.-M.; Li, M.-H.; Chao, H.-L.; Tsai, J.-T. Comparing outcomes of stereotactic body radiotherapy with intensity-modulated radiotherapy for patients with locally advanced unresectable pancreatic cancer. Eur. J. Gastroenterol. Hepatol. 2015, 27, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Ling, D.C.; Wegner, R.E.; Flickinger, J.C.; Heron, D.E.; Zeh, H.; Moser, A.J.; Burton, S.A. Stereotactic body radiotherapy in the treatment of Pancreatic Adenocarcinoma in elderly patients. Radiat. Oncol. 2013, 8, 240. [Google Scholar] [CrossRef] [PubMed]
- Hoyer, M.; Roed, H.; Sengelov, L.; Traberg, A.; Ohlhuis, L.; Pedersen, J.; Nellemann, H.; Berthelsen, A.K.; Eberholst, F.; Engelholm, S.A.; et al. Phase-II study on stereotactic radiotherapy of locally advanced pancreatic carcinoma. Radiother. Oncol. 2005, 76, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Goyal, K.; Einstein, D.; Ibarra, R.A.; Yao, M.; Kunos, C.; Ellis, R.; Brindle, J.; Singh, D.; Hardacre, J.; Zhang, Y.; et al. Stereotactic Body Radiation Therapy for Nonresectable Tumors of the Pancreas. J. Surg. Res. 2012, 174, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Didolkar, M.S.; Coleman, C.W.; Brenner, M.J.; Chu, K.U.; Olexa, N.; Stanwyck, E.; Yu, A.; Neerchal, N.; Rabinowitz, S. Image-Guided Stereotactic Radiosurgery for Locally Advanced Pancreatic Adenocarcinoma Results of First 85 Patients. J. Gastrointest. Surg. 2010, 14, 1547–1559. [Google Scholar] [CrossRef] [PubMed]
- Boone, B.A.; Steve, J.; Krasinskas, A.M.; Zureikat, A.H.; Lembersky, B.C.; Gibson, M.K.; Stoller, R.G.; Zeh, H.J.; Bahary, N. Outcomes with FOLFIRINOX for borderline resectable and locally unresectable pancreatic cancer. J. Surg. Oncol. 2013, 108, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Comito, T.; Ghidini, A.; Torri, V.; Scorsetti, M.; Barni, S. Stereotactic Body Radiation Therapy for Locally Advanced Pancreatic Cancer: A Systematic Review and Pooled Analysis of 19 Trials. Int. J. Radiat. Oncol. 2017, 97, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Herman, J.M.; Chang, D.T.; Goodman, K.A.; Dholakia, A.S.; Raman, S.P.; Hacker-Prietz, A.; Iacobuzio-Donahue, C.A.; Griffith, M.E.; Pawlik, T.M.; Pai, J.S.; et al. Phase 2 multi-institutional trial evaluating gemcitabine and stereotactic body radiotherapy for patients with locally advanced unresectable pancreatic adenocarcinoma. Cancer 2015, 121, 1128–1137. [Google Scholar] [CrossRef] [PubMed]
- Schellenberg, D.; Kim, J.; Christman-Skieller, C.; Chun, C.L.; Columbo, L.A.; Ford, J.M.; Fisher, G.A.; Kunz, P.L.; Van Dam, J.; Quon, A.; et al. Single-Fraction Stereotactic Body Radiation Therapy and Sequential Gemcitabine for the Treatment of Locally Advanced Pancreatic Cancer. Int. J. Radiat. Oncol. 2011, 81, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Koong, A.C.; Le, Q.T.; Ho, A.; Fong, B.; Fisher, G.; Cho, C.; Ford, J.; Poen, J.; Gibbs, I.C.; Mehta, V.K.; et al. Phase I study of stereotactic radiosurgery in patients with locally advanced pancreatic cancer. Int. J. Radiat. Oncol. 2004, 58, 1017–1021. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.T.; Schellenberg, D.; Shen, J.; Kim, J.; Goodman, K.A.; Fisher, G.A.; Ford, J.M.; Desser, T.; Quon, A.; Koong, A.C. Stereotactic radiotherapy for unresectable adenocarcinoma of the pancreas. Cancer 2009, 115, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Mahadevan, A.; Jain, S.; Goldstein, M.; Miksad, R.; Pleskow, D.; Sawhney, M.; Brennan, D.; Callery, M.; Vollmer, C. Stereotactic Body Radiotherapy and Gemcitabine for Locally Advanced Pancreatic Cancer. Int. J. Radiat. Oncol. 2010, 78, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Tozzi, A.; Comito, T.; Alongi, F.; Navarria, P.; Iftode, C.; Mancosu, P.; Reggiori, G.; Clerici, E.; Rimassa, L.; Zerbi, A.; et al. SBRT in unresectable advanced pancreatic cancer: Preliminary results of a mono-institutional experience. Radiat. Oncol. 2013, 8, 148. [Google Scholar] [CrossRef] [PubMed]
- Gurka, M.K.; Collins, S.P.; Slack, R.; Tse, G.; Charabaty, A.; Ley, L.; Berzcel, L.; Lei, S.; Suy, S.; Haddad, N.; et al. Stereotactic body radiation therapy with concurrent full-dose gemcitabine for locally advanced pancreatic cancer: A pilot trial demonstrating safety. Radiat. Oncol. 2013, 8, 44. [Google Scholar] [CrossRef] [PubMed]
- Neoptolemos, J.P.; Stocken, D.D.; Dunn, J.A.; Almond, J.; Beger, H.G.; Pederzoli, P.; Bassi, C.; Dervenis, C.; Fernandez-Cruz, L.; Lacaine, F.; et al. Influence of resection margins on survival for patients with pancreatic cancer treated by adjuvant chemoradiation and/or chemotherapy in the ESPAC-1 randomized controlled trial. Ann. Surg. 2001, 234, 758–768. [Google Scholar] [CrossRef] [PubMed]
- Kinsella, T.J.; Seo, Y.; Willis, J.; Stellato, T.A.; Siegel, C.T.; Harpp, D.; Willson, J.K.; Gibbons, J.; Sanabria, J.R.; Hardacre, J.M.; et al. The Impact of Resection Margin Status and Postoperative CA19-9 Levels on Survival and Patterns of Recurrence after Postoperative High-Dose Radiotherapy With 5-FU—Based Concurrent Chemotherapy for Resectable Pancreatic Cancer. Am. J. Clin. Oncol. 2008, 31, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.K.; Johns, A.L.; Merrett, N.D.; Gill, A.J.; Colvin, E.K.; Scarlett, C.J.; Nguyen, N.Q.; Leong, R.W.L.; Cosman, P.H.; Kelly, M.I.; et al. Margin Clearance and Outcome in Resected Pancreatic Cancer. J. Clin. Oncol. 2009, 27, 2855–2862. [Google Scholar] [CrossRef] [PubMed]
- Campbell, F.; Smith, R.A.; Whelan, P.; Sutton, R.; Raraty, M.; Neoptolemos, J.P.; Ghaneh, P. Classification of R1 resections for pancreatic cancer: The prognostic relevance of tumour involvement within 1 mm of a resection margin. Histopathology 2009, 55, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Mellon, E.A.; Hoffe, S.E.; Springett, G.M.; Frakes, J.M.; Strom, T.J.; Hodul, P.J.; Malafa, M.P.; Chuong, M.D.; Shridhar, R. Long-term outcomes of induction chemotherapy and neoadjuvant stereotactic body radiotherapy for borderline resectable and locally advanced pancreatic adenocarcinoma. Acta Oncol. (Madr) 2015, 54, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Hammel, P.; Huguet, F.; van Laethem, J.-L.; Goldstein, D.; Glimelius, B.; Artru, P.; Borbath, I.; Bouche, O.; Shannon, J.; Andre, T.; et al. Effect of Chemoradiotherapy vs. Chemotherapy on Survival in Patients With Locally Advanced Pancreatic Cancer Controlled after 4 Months of Gemcitabine with or without Erlotinib. JAMA 2016, 315, 1844. [Google Scholar] [CrossRef] [PubMed]
- Klinkenbijl, J.H.; Jeekel, J.; Sahmoud, T.; van Pel, R.; Couvreur, M.L.; Veenhof, C.H.; Arnaud, J.P.; Gonzalez, D.G.; de Wit, L.T.; Hennipman, A.; et al. Adjuvant radiotherapy and 5-fluorouracil after curative resection of cancer of the pancreas and periampullary region: Phase III trial of the EORTC gastrointestinal tract cancer cooperative group. Ann. Surg. 1999, 230, 776. [Google Scholar] [CrossRef] [PubMed]
- Kalser, M.H.; Ellenberg, S.S. Pancreatic cancer. Adjuvant combined radiation and chemotherapy following curative resection. Arch. Surg. 1985, 120, 899–903. [Google Scholar] [PubMed]
- Neoptolemos, J.P.; Palmer, D.H.; Ghaneh, P.; Psarelli, E.E.; Valle, J.W.; Halloran, C.M.; Faluyi, O.; O’Reilly, D.A.; Cunningham, D.; Wadsley, J.; et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): A multicentre, open-label, randomised, phase 3 trial. Lancet (Lond. Engl.) 2017, 389, 1011–1024. [Google Scholar] [CrossRef]
- Regine, W.F.; Winter, K.A.; Abrams, R.A.; Safran, H.; Hoffman, J.P.; Konski, A.; Benson, A.B.; Macdonald, J.S.; Kudrimoti, M.R.; Fromm, M.L.; et al. Fluorouracil vs. gemcitabine chemotherapy before and after fluorouracil-based chemoradiation following resection of pancreatic adenocarcinoma: A randomized controlled trial. JAMA 2008, 299, 1019–1026. [Google Scholar] [CrossRef] [PubMed]
- Valle, J.W.; Palmer, D.; Jackson, R.; Cox, T.; Neoptolemos, J.P.; Ghaneh, P.; Rawcliffe, C.L.; Bassi, C.; Stocken, D.D.; Cunningham, D.; et al. Optimal duration and timing of adjuvant chemotherapy after definitive surgery for ductal adenocarcinoma of the pancreas: Ongoing lessons from the ESPAC-3 study. J. Clin. Oncol. 2014, 32, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Oettle, H.; Neuhaus, P.; Hochhaus, A.; Hartmann, J.T.; Gellert, K.; Ridwelski, K.; Niedergethmann, M.; Zulke, C.; Fahlke, J.; Arning, M.B.; et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: The CONKO-001 randomized trial. JAMA 2013, 310, 1473–1481. [Google Scholar] [CrossRef] [PubMed]
- Neoptolemos, J.P.; Stocken, D.D.; Friess, H.; Bassi, C.; Dunn, J.A.; Hickey, H.; Beger, H.; Fernandez-Cruz, L.; Dervenis, C.; Lacaine, F.; et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N. Engl. J. Med. 2004, 350, 1200–1210. [Google Scholar] [CrossRef] [PubMed]
- Burris, H.A., 3rd; Moore, M.J.; Andersen, J.; Green, M.R.; Rothenberg, M.L.; Modiano, M.R.; Cripps, M.C.; Portenoy, R.K.; Storniolo, A.M.; Tarassoff, P.; et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: A randomized trial. J. Clin. Oncol. 1997, 15, 2403–2413. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.J.; Hamm, J.; Dancey, J.; Eisenberg, P.D.; Dagenais, M.; Fields, A.; Hagan, K.; Greenberg, B.; Colwell, B.; Zee, B.; et al. Comparison of gemcitabine versus the matrix metalloproteinase inhibitor BAY 12-9566 in patients with advanced or metastatic adenocarcinoma of the pancreas: A phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J. Clin. Oncol. 2003, 21, 3296–3302. [Google Scholar] [CrossRef] [PubMed]
- Ishii, H.; Furuse, J.; Boku, N.; Okusaka, T.; Ikeda, M.; Ohkawa, S.; Fukutomi, A.; Hamamoto, Y.; Nakamura, K.; Fukuda, H.; et al. Phase II study of gemcitabine chemotherapy alone for locally advanced pancreatic carcinoma: JCOG0506. Jpn. J. Clin. Oncol. 2010, 40, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Center, M.M.; Jemal, A. International Trends in Liver Cancer Incidence Rates. Cancer Epidemiol. Biomarkers Prev. 2011, 20, 2362–2368. [Google Scholar] [CrossRef] [PubMed]
- Scorsetti, M.; Comito, T.; Cozzi, L.; Clerici, E.; Tozzi, A.; Franzese, C.; Navarria, P.; Fogliata, A.; Tomatis, S.; D’Agostino, G.; et al. The challenge of inoperable hepatocellular carcinoma (HCC): Results of a single-institutional experience on stereotactic body radiation therapy (SBRT). J. Cancer Res. Clin. Oncol. 2015, 141, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Lasley, F.D.; Mannina, E.M.; Johnson, C.S.; Perkins, S.M.; Althouse, S.; Maluccio, M.; Kwo, P.; Cardenes, H. Treatment variables related to liver toxicity in patients with hepatocellular carcinoma, Child-Pugh class A and B enrolled in a phase 1-2 trial of stereotactic body radiation therapy. Pract. Radiat. Oncol. 2015, 5, e443–e449. [Google Scholar] [CrossRef] [PubMed]
- Bujold, A.; Massey, C.A.; Kim, J.J.; Brierley, J.; Cho, C.; Wong, R.K.S.; Dinniwell, R.E.; Kassam, Z.; Ringash, J.; Cummings, B.; et al. Sequential Phase I and II Trials of Stereotactic Body Radiotherapy for Locally Advanced Hepatocellular Carcinoma. J. Clin. Oncol. 2013, 31, 1631–1639. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.-K.; Kim, M.-S.; Cho, C.K.; Yang, K.M.; Yoo, H.J.; Kim, J.H.; Bae, S.H.; Jung, D.H.; Kim, K.B.; Lee, D.H.; et al. Stereotactic body radiation therapy for inoperable hepatocellular carcinoma as a local salvage treatment after incomplete transarterial chemoembolization. Cancer 2012, 118, 5424–5431. [Google Scholar] [CrossRef] [PubMed]
- Méndez Romero, A.; Wunderink, W.; Hussain, S.M.; de Pooter, J.A.; Heijmen, B.J.M.; Nowak, P.C.J.M.; Nuyttens, J.J.; Brandwijk, R.P.; Verhoef, C.; Ijzermans, J.N.M.; et al. Stereotactic body radiation therapy for primary and metastatic liver tumors: A single institution phase i-ii study. Acta Oncol. (Madr) 2006, 45, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Jacob, R.; Turley, F.; Redden, D.T.; Saddekni, S.; Aal, A.K.A.; Keene, K.; Yang, E.; Zarzour, J.; Bolus, D.; Smith, J.K.; et al. Adjuvant stereotactic body radiotherapy following transarterial chemoembolization in patients with non-resectable hepatocellular carcinoma tumours of ≥3 cm. HPB 2015, 17, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Klein, J.; Dawson, L.A. Hepatocellular Carcinoma Radiation Therapy: Review of Evidence and Future Opportunities. Int. J. Radiat. Oncol. 2013, 87, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Popp, I.; Grosu, A.L.; Niedermann, G.; Duda, D.G. Immune modulation by hypofractionated stereotactic radiation therapy: Therapeutic implications. Radiother. Oncol. 2016, 120, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Formenti, S.C.; Demaria, S. Combining Radiotherapy and Cancer Immunotherapy: A Paradigm Shift. J. Natl. Cancer Inst. 2013, 105, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Demaria, S.; Formenti, S. Current clinical trials testing the combination of immunotherapy with radiotherapy. J. Immunother. Cancer 2016, 4, 51. [Google Scholar] [CrossRef] [PubMed]
- Golden, E.B.; Demaria, S.; Schiff, P.B.; Chachoua, A.; Formenti, S.C. An abscopal response to radiation and ipilimumab in a patient with metastatic non-small cell lung cancer. Cancer Immunol. Res. 2013, 1, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Formenti, S.C.; Demaria, S. Radiation therapy to convert the tumor into an in situ vaccine. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 879–880. [Google Scholar] [CrossRef] [PubMed]
- Order, S.E. The effects of therapeutic irradiation on lymphocytes and immunity. Cancer 1977, 39, 737–743. [Google Scholar] [CrossRef]
- Uh, S.; Lee, S.M.; Kim, H.T.; Chung, Y.; Kim, Y.H.; Park, C.; Huh, S.J.; Lee, H.B. The effect of radiation therapy on immune function in patients with squamous cell lung carcinoma. Chest 1994, 105, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Sharabi, A.B.; Tran, P.T.; Lim, M.; Drake, C.G.; Deweese, T.L. Stereotactic radiation therapy combined with immunotherapy: Augmenting the role of radiation in local and systemic treatment. Oncology (Williston Park) 2015, 29, 331–340. [Google Scholar] [PubMed]
- Kim, H.J.; Park, S.; Kim, K.J.; Seong, J. The Clinical Implications of Soluble PD-L1 in Hepatocellular Carcinoma Patients Treated With Radiation Therapy. Int. J. Radiat. Oncol. 2017, 99, S89. [Google Scholar] [CrossRef]
- Patel, K.R.; Shoukat, S.; Oliver, D.E.; Chowdhary, M.; Rizzo, M.; Lawson, D.H.; Khosa, F.; Liu, Y.; Khan, M.K. Ipilimumab and Stereotactic Radiosurgery vs. Stereotactic Radiosurgery Alone for Newly Diagnosed Melanoma Brain Metastases. Am. J. Clin. Oncol. 2017, 40, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Kiess, A.P.; Wolchok, J.D.; Barker, C.A.; Postow, M.A.; Tabar, V.; Huse, J.T.; Chan, T.A.; Yamada, Y.; Beal, K. Stereotactic Radiosurgery for Melanoma Brain Metastases in Patients Receiving Ipilimumab: Safety Profile and Efficacy of Combined Treatment. Int. J. Radiat. Oncol. 2015, 92, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Twyman-Saint Victor, C.; Rech, A.J.; Maity, A.; Rengan, R.; Pauken, K.E.; Stelekati, E.; Benci, J.L.; Xu, B.; Dada, H.; Odorizzi, P.M.; et al. Radiation and dual checkpoint blockade activate non-redundant immune mechanisms in cancer. Nature 2015, 520, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Narang, A.; Thompson, E.; Anders, R.; Waters, K.; Poling, J.; Rosati, L.M.; Huang, C.Y.; Tran, P.T.; Herman, J.M.; et al. Characterizing Tumor Infiltrating Lymphocytes Following Neoadjuvant Chemotherapy and Radiation in Pancreatic Adenocarcinoma. Int. J. Radiat. Oncol. 2017, 99, S91–S92. [Google Scholar] [CrossRef]
- Foley, K.; Kim, V.; Jaffee, E.; Zheng, L. Current progress in immunotherapy for pancreatic cancer. Cancer Lett. 2016, 381, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.R.; Tykodi, S.S.; Chow, L.Q.M.; Hwu, W.-J.; Topalian, S.L.; Hwu, P.; Drake, C.G.; Camacho, L.H.; Kauh, J.; Odunsi, K.; et al. Safety and Activity of Anti–PD-L1 Antibody in Patients with Advanced Cancer. N. Engl. J. Med. 2012, 366, 2455–2465. [Google Scholar] [CrossRef] [PubMed]
- Royal, R.E.; Levy, C.; Turner, K.; Mathur, A.; Hughes, M.; Kammula, U.S.; Sherry, R.M.; Topalian, S.L.; Yang, J.C.; Lowy, I.; et al. Phase 2 Trial of Single Agent Ipilimumab (Anti-CTLA-4) for Locally Advanced or Metastatic Pancreatic Adenocarcinoma. J. Immunother. 2010, 33, 828–833. [Google Scholar] [CrossRef] [PubMed]
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Tchelebi, L.; Zaorsky, N.; Mackley, H. Stereotactic Body Radiation Therapy in the Management of Upper GI Malignancies. Biomedicines 2018, 6, 7. https://doi.org/10.3390/biomedicines6010007
AMA Style
Tchelebi L, Zaorsky N, Mackley H. Stereotactic Body Radiation Therapy in the Management of Upper GI Malignancies. Biomedicines. 2018; 6(1):7. https://doi.org/10.3390/biomedicines6010007
Chicago/Turabian StyleTchelebi, Leila, Nicholas Zaorsky, and Heath Mackley. 2018. "Stereotactic Body Radiation Therapy in the Management of Upper GI Malignancies" Biomedicines 6, no. 1: 7. https://doi.org/10.3390/biomedicines6010007
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.