Helping Health Services to Meet the Needs of Young People with Chronic Conditions: Towards a Developmental Model for Transition


1
Institute of Applied Health Research, University of Birmingham, Birmingham B15 2TT, UK
2
Centre for Musculoskeletal Research, Division of Musculoskeletal and Dermatological Sciences, The University of Manchester, Manchester M13 9PT, UK
3
NIHR Manchester Musculoskeletal Biomedical Research Centre, Central Manchester University Hospitals NHS Foundation Trust, Manchester M13 9WL, UK
*
Author to whom correspondence should be addressed.
Healthcare 2017, 5(4), 77; https://doi.org/10.3390/healthcare5040077
Submission received: 31 July 2017
/
Revised: 12 October 2017
/
Accepted: 14 October 2017
/
Published: 19 October 2017
(This article belongs to the Special Issue Supporting Emotional Well-Being and Psychological Health Outcomes in Young People with Long-Term Health Needs)
Abstract
:The transition to adult healthcare has been the subject of increased research and policy attention over many years. However, unmet needs of adolescent and young adults (AYAs) and their families continue to be documented, and universal implementation has yet to be realised. Therefore, it is pertinent to re-examine health transition in light of the principles of adolescent medicine from which it emerged, and consider this particular life transition in terms of a developmental milestone rather than a negotiation of structural boundaries between child and adult services. Health transitions are an integral part of AYA development and as such, occur alongside, and in connection with, a range of other important transitions that affect many other areas of life. In this paper, we discuss the interrelated nature of health transitions and AYA development; outline the underpinnings of a developmentally appropriate approach to transitional care; and consider the outcome measurement of such care based on existing evidence. A developmental approach has the potential to refocus transition on the fundamental principles of adolescent medicine, enabling health transition to be integrated along with other life transitions into routine AYA developmental assessments rather than being limited to the geographies of different healthcare settings and a potential health crisis.
1. Introduction
Transition in health literature is often considered synonymous with health transition, i.e., the preparation of young people and their families as they move from child to adult-centred services [1]. Transitional care not only prepares young people and their caregivers for the differences between child and adult services and how to negotiate them but also supports the development of health literacy and self-management skills. Such knowledge and skill development is vital at this life stage as responsibility shifts from parents to a shared responsibility and eventually, if they have capacity, to the young person themselves.
Health transitions have been discussed and debated for many years in the literature [2], resulting in national and international guidance [3,4]. In spite of this however, an evidence base has been slow to be established [1] and reports of unmet needs of young people and their families continue to be reported [5]. Barriers to implementation at professional and system levels also continue to be reported [6,7].
Perhaps it is therefore time to reconnect transition to the principles and practice of adolescent medicine from which it emerged [8] and consider health transition in terms of a developmental milestone rather than a negotiation of structural boundaries between child and adult services [9].
In this paper, we will (1) discuss the interrelated nature of health transitions and adolescent and young adult development; (2) outline the fundamental elements of a developmentally appropriate approach to transitional care; and (3) consider the outcome measurement of such care in light of existing evidence.
2. Health Transition as One of Multiple, Interrelated Transitions
Adolescents and young adults (AYAs) experience health related transitions as they undergo a range of developmental changes during adolescence and young adulthood, which in turn are associated with many other life transitions (Table 1).
Health transition is an integral part of development for all young people, with and without a long-term health condition. Young people frequently remind us that they are young people first and foremost—“it [transition] is not about arthritis, it is about living with it” [10]. Bearing this in mind, it is important to acknowledge the developmental context of health transition and consider how the different aspects of that development, including the transitions listed in Table 1, impact on health transitions and vice versa.
Unfortunately, key aspects of AYA development are not always adequately acknowledged in the health care of this age group. In a study of 290 young people, 227 of whom had a long-term health condition and a mean age of 17 years, key adolescent health-related issues were not universally addressed by staff [11]. There was also a significant discrepancy between reported discussion of psychosocial issues by professionals compared to young people, raising the issue of the efficacy of communication strategies being employed by staff [11]. Such routine psychosocial screening is core to transitional care [8] and yet not always covered by the current transition readiness tools [12].
Adopting a developmental model for transition addresses this by refocussing transitional care on a fundamental principle underpinning the practice of adolescent medicine, i.e., developmentally appropriate healthcare [13,14,15], and placing health transition within the wider context of AYA development—i.e., considering the impact of the biological, psychological, social and vocational aspects of AYA development on health transition as well as the impact of health transition on such development.
3. Developmentally Appropriate Transitional Care for Young People
The increasing knowledge on AYA development [16,17] and the inter-relationships of the different aspects of such development (e.g., impact of pubertal timing on social development [18,19]) offers unprecedented opportunities to develop and reshape health care services to better meet the biopsychosocial developmental needs of AYAs. However, it is important to develop a shared understanding in the clinical and organisational arena about what such adolescent-responsive health services look like in practice [15] including transitional care services.
Developmentally appropriate healthcare (DAH) for young people, a key principle underpinning the practice of adolescent medicine [13,20] is particularly well suited to serve this purpose. DAH is an approach to clinical work with adolescents and young adults, which conveys the dynamic nature of AYA development (rather than chronological age) as a defining characteristic of health services, and offers room to achieve consistency in clinical practice regardless of whether adolescent medicine is recognised as a distinct specialty or not in a particular context [21].
Although a scoping review concluded that there is still the need to further clarify and operationalise the definition of DAH to enable a more consistent use of the term in the literature and future research [14], a subsequent ethnographic study of health professionals and managers responsible for delivering such care identified five conceptual dimensions which potentially provide a framework for such care provision [15]:
- Biopsychosocial development and holistic care. Key developmental milestones of AYAs at biological, psychological, social and vocational levels (across early, mid and late adolescence and emerging adulthood) inform clinical work by either (1) adopting a holistic clinical approach that looks beyond the physical aspect of one’s condition and integrates the biological psychological, social and vocational aspects of development; or (2) incorporating additional care components to otherwise standard paediatric/adult care. Family or trusted others are included as key stakeholders and/or active participants of healthcare provision for AYAs [15].
- Acknowledgement of AYA as a distinct group. Developmental needs of AYAs inform distinct ways of interacting and communicating with them, in terms of (1) what, when and how information is given to and gathered from them; and (2) official communication materials and means (such as appointment letters or text message reminders). Specific/tailored services, spaces and pathways are provided. The distinct needs of the service (e.g., need for longer appointments) and those of the health professionals looking after AYAs (e.g., training in adolescent health) are acknowledged and addressed [15].
- Adjustment of care as the young person develops. The starting point of DAH is a developmental assessment, covering all areas of AYA development and actively involving parents/carers and/or trusted others. Routine follow-up developmental assessments are then undertaken and used to inform the tailoring of particular aspects of clinical work and service delivery as the young person grows up [15].
- Empowerment of the young person by embedding health education and health promotion. AYAs are routinely provided with (1) informal education on self-management skills and (2) health promotion information and lifestyle behaviour change advice relevant to each stage of development to enable AYAs to make informed choices. Health education and health promotion delivered in the context of DAH services is informed by, but not limited to, a health transition agenda. The approach to health education and health promotion delivered in the context of DAH is based on promoting active engagement and autonomy-enabling practices without creating relations of dependency with the service/clinical team [15].
- Interdisciplinary and interorganisational work. Effective multidisciplinary work both within and across services, teams, specialities and organisations [15].
In Table 2, we provide some examples as to how these dimensions are translated into practice.
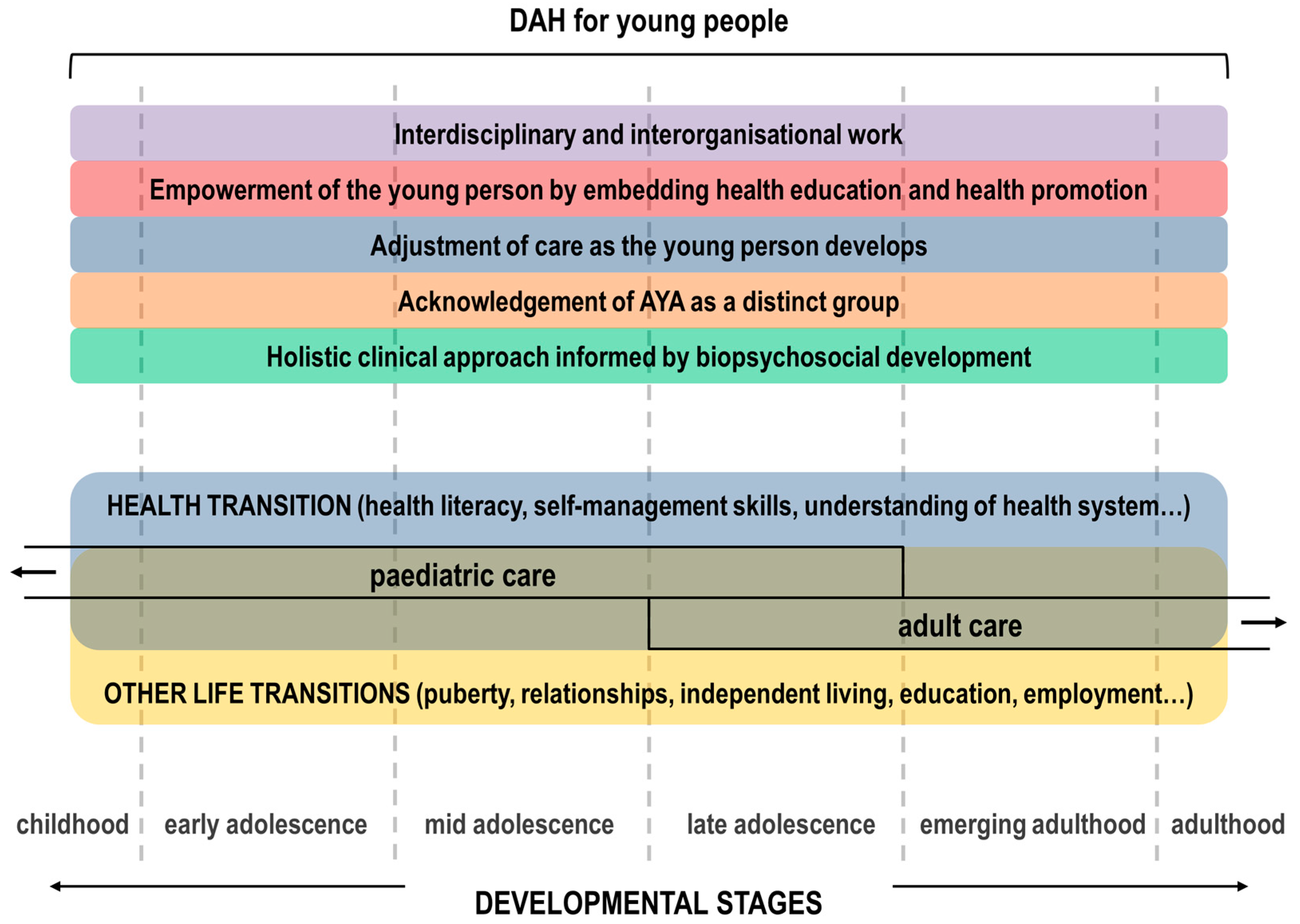
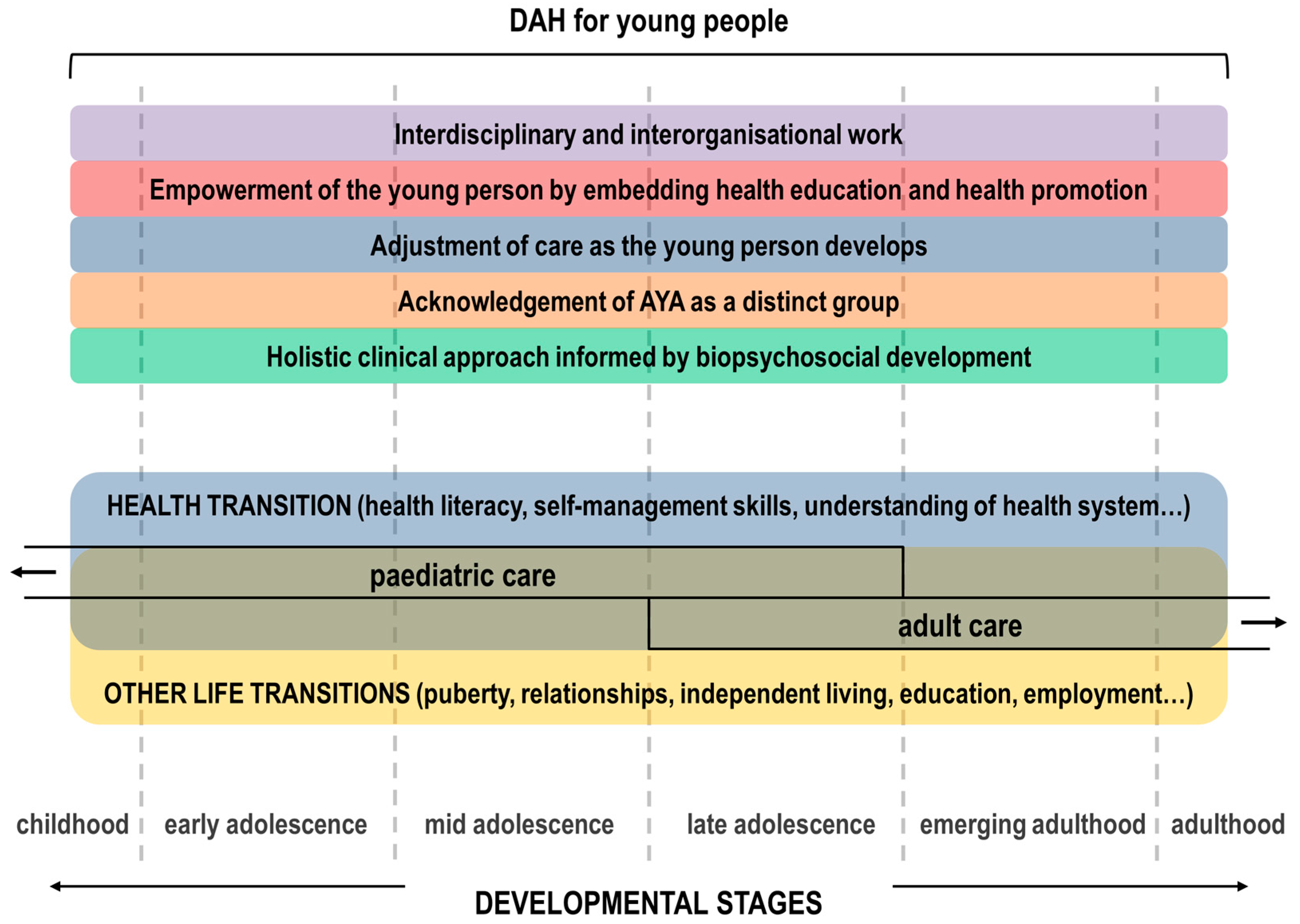
Following the description of the five conceptual dimensions of DAH for young people outlined above and the examples listed in Table 2, it becomes clear that the provision of DAH in paediatric and adult settings encompasses transitional care by definition. Health transitions are an integral part of AYA development that will be integrated along with other life transitions into routine developmental assessments (Figure 1).
Alongside these considerations, it is equally important to consider the perspectives of AYAs themselves. Listening to the views of young people and their caregivers is essential to the development of meaningful services and this is reflected in the literature addressing the principles of youth-friendly health care (YFHC) [24]. As with transitional care, national and international guidance has existed in the literature detailing the core indicators of YFHC [24,25,26], which can be used to ensure that transitional care services are also youth-friendly (Table 3).
Thus, the different emphases of DAH and YFHS (i.e., the emphasis on DAH as compared to YFHC is shifted from the service and centres on the development of the young person) can be combined to provide health services that are youth-friendly and developmentally appropriate, i.e., services that are meaningful and consistent from both the AYA and provider perspectives. This echoes the WHO call to move from adolescent-friendly service delivery into services that can respond to the priority health and development needs of adolescents [27]. Therefore, it is paramount to ensure that transitional care services are adolescent-friendly in the first place and that they continue to be adolescent-friendly as they transform into developmentally appropriate services.
If one adopts the concept of developmentally appropriate transitional care services, when a transition intervention is proven to be ineffective, a new range of potential explanations can be considered:
- Was the intervention concerned with changing the approach to clinical work based on key developmental milestones of AYAs from early adolescence through to emerging adulthood?
- Were the family or AYA’s trusted others included in service provision?
- Was the individual and service level communication strategy tailored to developmental needs?
- Were AYA-specific/tailored services, spaces and pathways provided or engaged with as part of the intervention?
- Were the needs of staff delivering the intervention dealt with (adolescent health training, availability of resources) as part of the intervention?
- Were routine and follow-up biopsychosocial developmental assessments (and tools) built into the intervention and used to inform dynamic changes in clinical work and service delivery as AYAs develop?
- Was the intervention concerned with supporting effective multidisciplinary work both within and across services, teams, specialities and organisations?
These are all questions mainly related to intervention delivery, the ‘whys’ and ‘hows’ of a given set of outcomes, and can be explored through process evaluation designs.
4. Outcome Indicators of Transition
The ultimate aim of both transitional care and/or DAH for young people with long-term conditions is improvement in their health-related outcomes. There is increasing interest in the selection of outcome indicators of transition.
In a recent Delphi process involving professionals from outpatient, community-based and primary care settings, 10 outcomes were identified, with the majority being health service related, except for ‘optimal quality of life’ and ‘a social network’, and none including vocational or psychological outcomes [28]. Similarly, the four randomised controlled trials identified in the recent Cochrane review [1] primarily employed health service related measures, with the exception of the PedsQol, as did Sharma et al. [29]. The proposed indicators from these three contributions are summarised in Table 4, alongside the ones proposed in current NICE guidelines.
The term transition readiness is increasingly prevalent in the literature although still in its infancy [12]. At times, it is unclear as to whether this is truly ‘transition readiness’ or simply ‘transfer readiness’. Furthermore, it is unclear as to whether this readiness is being considered in the context of AYA development. What is the exact nature of this readiness—physical, psychological and/or social readiness? Few measures consider educational and vocational development, which is concerning in view of the finding that poor health in adolescence is associated with poorer education and poorer employment outcomes in adulthood [30]. Although young people with long-term conditions have similar social success to controls, they have lower rates of mastering vocational milestones [31,32].
Many of the readiness tools under development are self-reported measures. This raises the question as to how mastery of the skills is assessed. Fredericks et al. [33] reported the interesting finding that although young people aged 16–20 years with liver transplants perceived greater self-management on a transition readiness survey, they had a higher risk for medication nonadherence.
In addition to consideration of assessment of mastery of skills which are practiced beyond the clinic setting (such as adherence to medication or ability to order medication refills), attention is also required as to whether the setting in which these skills are being practiced is a place where such skills are promoted (including resilience promoting personnel). This includes health care settings as well as the home and school setting. A young person may be ‘transition-ready’ but may be unable to practice their skills due to the lack of promotion of positive youth development in a particular health care setting. For example, if young people are not routinely offered the opportunity to ask their own questions with care givers present (and/or be seen independently of their caregivers), they will be unable to practice asking questions about sensitive topics. Likewise, if caregivers continue to take full responsibility for the administration of daily medication in the absence of any limited capacity of the young person to learn to do so, the young person may never acquire the skills to take responsibility themselves. This is particularly pertinent in view of the reports that self-efficacy and resilience are useful predictors of health transition readiness [34].
Several studies have reported a significant and positive relationship between age and skill acquisition [35,36,37,38,39] with age predicting mastery of skills over time [35]. Previous studies also found that few AYAs achieve mastery of health care transition skills by age 18, especially in the domains of ‘disease self-management’ and ‘understanding of health insurance’ [36,37,38] emphasising the need to acknowledge that health transition does not end with the event of transfer but extends into young adulthood and hence adult services.
It is important to remember that all young people need skill development in health management irrespective of whether they have a long-term condition or not. Eaton et al. [40] reported that AYAs with medical conditions (mean age 19 years) reported significantly higher levels of health transition readiness and self-involvement in completing medical tasks, and lower levels of parental involvement in completing medical tasks, than healthy peers. Equally, it is important to note that as with all developmental milestones, health transition readiness may regress. More prospective research in the area of health transition readiness trajectories is awaited with interest.
Another area of outcome research is consideration of the different perspectives involved, particularly those of AYAs themselves and their parents. In the Fair et al. study [28], there was a low representation of AYAs and their family members beyond stage 1 of the Delphi process, as noted by the authors. A more recent study by Pierce et al. [41] involved 10 young adults and 9 parents, but the study focused on young adults who had recently transferred out of paediatric care. AYAs from a range of ages and backgrounds may have an equally wide range of opinions as to the choice of outcome measures, i.e., what is important, in their opinion at this particular time in their lives, for health professionals to measure.
This relates to another important question: when is the right time to measure? One could argue that readiness is more a process rather than an outcome measure and that there are different stages of readiness just as there are different stages of adolescent and young adult development. Reflecting this, the NICE guidance for health and social care service transition in England emphasises that measurement requires an adequate duration to capture relevant condition-specific and quality of life outcomes [4].
Failure to attend appointments is a familiar outcome measure and is often considered as a negative outcome. However the reason given by young people for this nonattendance may be work and school conflicts [42] or a fear of being judged for “poor control” [43] and therefore more a reflection on the accessibility and developmentally appropriateness of the service rather than a failure of health transition readiness of the young person themselves.
Sharma et al. [29] also included professional and system-related outcome measures, which aligns with the dimensions of DAH detailed above, acknowledging the role of the team and organisation in transitional care (Table 5).
Outcomes, therefore, need to reflect the different aspects of DAH, i.e., medical (health and illness), psychological, social, educational/vocational and acknowledge the different levels, i.e., young person and family, care team, organisation (including setting where care is delivered) and environment in terms of regulatory and policy framework.
5. Conclusions
Transition to adult healthcare has been the subject of increased research and policy attention over many years, and yet unmet needs of young people and their families continue to be documented and universal implementation has yet to be realised. Health transitions are an integral part of AYA development and as such, occur alongside, and in connection with, a range of other important transitions that affect many other areas of life.
Adopting a developmental model for health transition in both clinical practice and research refocuses transitional care on a fundamental principle underpinning the practice of adolescent medicine, i.e., developmentally appropriate healthcare [13,14,15], and places health transition within the wider context of AYA development. The impact of the biological, psychological, social and vocational aspects of AYA development on health transition is therefore routinely considered as well as the impact of health transition on such development. In doing so, health transition is integrated along with other life transitions into routine AYA developmental assessment and ceases being limited to the negotiation of structural boundaries and a potential health crisis.
Acknowledgments
Albert Farre is funded by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care (CLAHRC) West Midlands. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Campbell, F.; Biggs, K.; Aldiss, S.K.; O’Neill, P.M.; Clowes, M.; McDonagh, J.; While, A.; Gibson, F. Transition of care for adolescents from paediatric services to adult health services. Cochrane Database Syst. Rev. 2016, 4, CD009794. [Google Scholar] [CrossRef] [PubMed]
- Barbero, G.J. Leaving the pediatrician for the internist. Ann. Intern. Med. 1982, 96, 673–674. [Google Scholar] [CrossRef]
- American Academy of Pediatrics; American Academy of Family Physicians; American College of Physicians, Transitions Clinical Report Authoring Group. Supporting the Health Care Transition From Adolescence to Adulthood in the Medical Home. Pediatrics 2011, 128, 182–200. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE) NICE guidelines [NG43]. Transition from Children’s to Adults’ Services for Young People Using Health or Social Care Services. Available online: https://www.nice.org.uk/guidance/ng43 (accessed on 31 July 2017).
- Lugasi, T.; Achille, M.; Stevenson, M. Patients’ perspective on factors that facilitate transition from child-centered to adult-centered health care: A theory integrated metasummary of quantitative and qualitative studies. J. Adolesc. Health 2011, 48, 429–440. [Google Scholar] [CrossRef] [PubMed]
- Hepburn, C.M.; Cohen, E.; Bhawra, J.; Weiser, N.; Hayeems, R.Z.; Guttmann, A. Health system strategies supporting transition to adult care. Arch. Dis. Child. 2015, 100, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Sonneveld, H.M.; Strating, M.M.H.; van Staa, A.L.; Nieboer, A.P. Gaps in transitional care: What are the perceptions of adolescents, parents and providers? Transitional care—Perceptions of adolescents, parents and providers. Child Care Health Dev. 2013, 39, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, A.; Sawyer, S. Transition from pediatric to adult services: Are we getting it right? Curr. Opin. Pediatr. August 2008, 20, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Scal, P. Improving health care transition services: Just grow up, will you please. JAMA Pediatr. 2016, 170, 197–199. [Google Scholar] [CrossRef] [PubMed]
- Shaw, K.L.; Southwood, T.R.; McDonagh, J.E. User perspectives of transitional care for adolescents with juvenile idiopathic arthritis. Rheumatology 2004, 43, 770–778. [Google Scholar] [CrossRef] [PubMed]
- Boisen, K.A.; Hertz, P.G.; Blix, C.; Teilmann, G. Is HEADS in our heads? Health risk behavior is not routinely discussed with young people with chronic conditions. Int. J. Adolesc. Med. Health 2016, 28, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Stinson, J.; Kohut, S.A.; Spiegel, L.; White, M.; Gill, N.; Colbourne, G.; Sigurdson, S.; Duffy, K.W.; Tucker, L.; Stringer, E.; et al. A systematic review of transition readiness and transfer satisfaction measures for adolescents with chronic illness. Int. J. Adolesc. Med. Health 2014, 26, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, S.M. Developmentally appropriate healthcare for young people with chronic illness: Questions of philosophy, policy, and practice. Pediatr. Pulmonol. 2003, 36, 363–365. [Google Scholar] [CrossRef] [PubMed]
- Farre, A.; Wood, V.; Rapley, T.; Parr, J.R.; Reape, D.; McDonagh, J.E. Developmentally appropriate healthcare for young people: A scoping study. Arch. Dis. Child. 2014. [Google Scholar] [CrossRef] [PubMed]
- Farre, A.; Wood, V.; McDonagh, J.E.; Parr, J.R.; Reape, D.; Rapley, T.; on behalf of the Transition Collaborative Group. Health professionals’ and managers’ definitions of developmentally appropriate healthcare for young people: Conceptual dimensions and embedded controversies. Arch. Dis Child. 2016, 101, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, S.M.; Afifi, R.A.; Bearinger, L.H.; Blakemore, S.-J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Viner, R. Life stage: Adolescence. In Annual Report of the Chief Medical Officer 2012, Our Children Deserve Better: Prevention Pays; Davies, S.C., Ed.; Department of Health: London, UK, 2013; Chapter 8; pp. 1–11. [Google Scholar]
- Blakemore, S.-J.; Burnett, S.; Dahl, R.E. The role of puberty in the developing adolescent brain. Hum. Brain Mapp. 2010, 31, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Berenbaum, S.A.; Beltz, A.M.; Corley, R. The Importance of Puberty for Adolescent Development. Adv. Child. Dev. Behav. 2015, 48, 53–92. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, S.M.; Aroni, R.A. Self-management in adolescents with chronic illness. What does it mean and how can it be achieved? Med. J. Aust. 2005, 183, 405–409. [Google Scholar] [PubMed]
- Jenkins, R.R. Adolescent medicine in the USA: A perspective on progress and lessons learnt. Arch. Dis. Child. 2016, 101, 510–513. [Google Scholar] [CrossRef] [PubMed]
- Rosen, D.S.; Goldenring, J.M. Getting into adolescent heads: An essential update. Contemp. Pediatr. 2004, 21, 64–90. [Google Scholar]
- Doukrou, M.; Segal, T.Y. Fifteen-minute consultation: Communicating with young people—How to use HEEADSSS, a psychosocial interview for adolescents. Arch. Dis. Child.—Educ. Pract. 2017. [Google Scholar] [CrossRef] [PubMed]
- Ambresin, A.-E.; Bennett, K.; Patton, G.C.; Sanci, L.A.; Sawyer, S.M. Assessment of Youth-Friendly Health Care: A Systematic Review of Indicators Drawn From Young People’s Perspectives. J. Adolesc. Health 2013, 52, 670–681. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. You’re Welcome: Quality Criteria for Young People Friendly Services 2011. Available online: https://www.gov.uk/government/publications/quality-criteria-for-young-people-friendly-health-services (accessed on 10 October 2017).
- Hargreaves, D.S.; McDonagh, J.E.; Viner, R.M. Validation of You’re Welcome Quality Criteria for Adolescent Health Services Using Data from National Inpatient Surveys in England. J. Adolesc. Health 2013, 52, 50–57. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization towards Adolescent-Responsive Health Systems: Steering the Transition from Adolescent-Friendly Projects to Adolescent-Responsive Health Systems. Available online: http://apps.who.int/adolescent/second-decade/section6/page8/sdolescent-responsiveness.html (accessed on 23 March 2017).
- Fair, C.; Cuttance, J.; Sharma, N.; Maslow, G.; Wiener, L.; Betz, C.; Porter, J.; McLaughlin, S.; Gilleland-Marchak, J.; Renwick, A. International and interdisciplinary identification of health care transition outcomes. JAMA Pediatr. 2016, 170, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; O’Hare, K.; Antonelli, R.C.; Sawicki, G.S. Transition Care: Future Directions in Education, Health Policy, and Outcomes Research. Acad. Pediatr. 2014, 14, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Hale, D.R.; Bevilacqua, L.; Viner, R.M. Adolescent Health and Adult Education and Employment: A Systematic Review. Pediatrics 2015, 136, 128–140. [Google Scholar] [CrossRef] [PubMed]
- Maslow, G.R.; Haydon, A.; McRee, A.-L.; Ford, C.A.; Halpern, C.T. Growing Up With a Chronic Illness: Social Success, Educational/Vocational Distress. J. Adolesc. Health 2011, 49, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M. Achievement of Developmental Milestones in Emerging and Young Adults With and Without Pediatric Chronic Illness--A Meta-Analysis. J. Pediatr. Psychol. 2014. [Google Scholar] [CrossRef] [PubMed]
- Fredericks, E.M.; Dore-Stites, D.; Well, A.; Magee, J.C.; Freed, G.L.; Shieck, V.; James Lopez, M. Assessment of transition readiness skills and adherence in pediatric liver transplant recipients. Pediatr. Transpl. 2010, 14, 944–953. [Google Scholar] [CrossRef] [PubMed]
- Carlsen, K.; Haddad, N.; Gordon, J.; Phan, B.L.; Pittman, N.; Benkov, K.; Dubinsky, M.C.; Keefer, L. Self-efficacy and Resilience Are Useful Predictors of Transition Readiness Scores in Adolescents with Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2017, 23, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Stollon, N.; Zhong, Y.; Ferris, M.; Bhansali, S.; Pitts, B.; Rak, E.; Kelly, M.; Kim, S.; van Tilburg, M.A. Chronological age when healthcare transition skills are mastered in adolescents/young adults with inflammatory bowel disease. World J. Gastroenterol. 2017, 23, 3349. [Google Scholar] [CrossRef] [PubMed]
- Gray, W.N.; Holbrook, E.; Morgan, P.J.; Saeed, S.A.; Denson, L.A.; Hommel, K.A. Transition readiness skills acquisition in adolescents and young adults with inflammatory bowel disease: Findings from integrating assessment into clinical practice. Inflamm. Bowel Dis. 2015, 21, 1125–1131. [Google Scholar] [CrossRef] [PubMed]
- Fishman, L.N.; Barendse, R.M.; Hait, E.; Burdick, C.; Arnold, J. Self-management of older adolescents with inflammatory bowel disease: A pilot study of behavior and knowledge as prelude to transition. Clin. Pediatr. 2010, 49, 1129–1133. [Google Scholar] [CrossRef] [PubMed]
- Whitfield, E.P.; Fredericks, E.M.; Eder, S.J.; Shpeen, B.H.; Adler, J. Transition readiness in pediatric patients with inflammatory bowel disease: A patient survey of self-management skills. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 36. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.S.; Tobin, A.; Tompane, T. Clinicians poorly assess health literacy-related readiness for transition to adult care in adolescents with inflammatory bowel disease. Clin. Gastroenterol. Hepatol. 2012, 10, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Eaton, C.K.; Davis, M.F.; Gutierrez-Colina, A.M.; LaMotte, J.; Blount, R.L.; Suveg, C. Different Demands, Same Goal: Promoting Transition Readiness in Adolescents and Young Adults With and Without Medical Conditions. J. Adolesc. Health 2017, 60, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Pierce, J.S.; Aroian, K.; Schifano, E.; Milkes, A.; Schwindt, T.; Gannon, A.; Wysocki, T. Health Care Transition for Young Adults With Type 1 Diabetes: Stakeholder Engagement for Defining Optimal Outcomes. J. Pediatr. Psychol. 2017, 42, 970–982. [Google Scholar] [CrossRef] [PubMed]
- Klosky, J.L.; Cash, D.K.; Buscemi, J.; Lensing, S.; Garces-Webb, D.M.; Zhao, W.; Wiard, S.; Hudson, M.M. Factors influencing long-term follow-up clinic attendance among survivors of childhood cancer. J. Cancer Surviv. 2008, 2, 225. [Google Scholar] [CrossRef] [PubMed]
- Snow, R.; Fulop, N. Understanding issues associated with attending a young adult diabetes clinic: A case study. Diabet. Med. 2012, 29, 257–259. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Schematic representation of the relationship of the five conceptual dimensions of DAH for young people to health transition and adolescent development.
Figure 1.
Schematic representation of the relationship of the five conceptual dimensions of DAH for young people to health transition and adolescent development.

{kind=link}
Table 1.
Some key transitions associated with developmental stages of adolescence and young adulthood.
Table 1.
Some key transitions associated with developmental stages of adolescence and young adulthood.
| Developmental Stage | Transitions |
|---|---|
| Early Adolescence 10–13 years | Biological (e.g., early puberty) |
| Psychological (e.g., concrete thinking to early moral concepts) | |
| Social (e.g., emotional separation from parents) | |
| Health (e.g., early self-management) | |
| Educational (e.g., primary to secondary school) | |
| Mid Adolescence 14–16 years | Biological (e.g., mid-late puberty) |
| Psychological (e.g., early abstract thinking) | |
| Social (e.g., strong peer identification) | |
| Health (e.g., increased self-management) | |
| Educational/Vocational (e.g., school to college) | |
| Late adolescence 17–19 years | Biological (e.g., completion of puberty) |
| Psychological (e.g., complex abstract thinking) | |
| Social (e.g., independent living and travel) | |
| Health (e.g., paediatric to adult healthcare) | |
| Educational/Vocational (e.g., college to further education or training) | |
| Emerging Adulthood 20–24 years | Biological (e.g., completion of brain development) |
| Psychological (e.g., exploration of self-identity) | |
| Social (e.g., independent living and financial independence) | |
| Health (e.g., autonomous self-management) | |
| Educational/Vocational (e.g., further education/training to employment) |
Table 2.
Some examples of how the five conceptual dimensions of developmentally appropriate healthcare (DAH) for young people are translated into practice.
Table 2.
Some examples of how the five conceptual dimensions of developmentally appropriate healthcare (DAH) for young people are translated into practice.
| Conceptual Dimensions of DAH for Young People [15] | Examples of How These Dimensions Are Translated into Practice |
|---|---|
| biopsychosocial development and holistic care |
|
| acknowledgement of young people as a distinct group | Acknowledgement of age and developmental stage-specific issues and how these may change during adolescence and young adulthood:
|
| adjustment of care as the young person develops | Flexibility in approach and acknowledgement of regression during active phases in relapsing conditions:
|
| empowerment of the young person by embedding health education and health promotion |
|
| interdisciplinary and interorganisational work |
|
Table 3.
Summary domains of adolescent-friendly care, with examples of relevant indicators [24].
Table 3.
Summary domains of adolescent-friendly care, with examples of relevant indicators [24].
| Domains of youth-friendly health care (YFHC) | Examples of Relevant Indicators |
|---|---|
| 1. Accessibility of health care | Location, affordability |
| 2. Staff attitude | Respectful, supportive, honest, trustworthy, friendly |
| 3. Communication | Clarity and provision of information, active listening, tone of communication |
| 4. Medical competency | Technical skills (procedures) |
| 5. Guideline-driven care | Confidentiality, autonomy, transition to adult health care services, comprehensive care |
| 6. Age-appropriate environment | Flexibility of appointment times, separate physical space, teen-oriented health information, cleanliness, waiting time, continuity of care, privacy |
| 7. Involvement in own health care | Understanding of one’s medical condition and treatment; acquisition of self-management skills |
| 8. Health outcomes | Pain management, quality of life |
Table 4.
Summary of the proposed outcome indicators of transition in the current literature.
| Outcome | Campbell et al. 2016 [1] | Fair et al. 2015 [28] | Sharma et al. 2014 [29] | NICE 2016 [4] |
|---|---|---|---|---|
| Transition readiness, self efficacy | Transition readiness (TRAQ); Patient Activation Measure; Community Life Skills (CLSS); Self-care practice | Self-management; Adherence to medication/treatment | Transition readiness | Transition readiness; Self-efficacy (YP’s ability to undertake the activities they want to, as independently as possible) |
| Disease-specifc status | HbA1C | − | Condition-specific outcomes | Condition-specific outcomes |
| Well being | Personal Adjustment and role skills (PARS III); Peds Qol | Achieving optimal Quality of life (QoL) | QoL | Qol (health and social care indicators) |
| Knowledge of disease and treatment | MyHeart | Disease knowledge; Medication knowledge | − | − |
| Knowledge of transition | − | − | Transition knowledge | − |
| Transfer from paediatric to adult services | % young people successfully transferred to adult services | − | Gaps in medical care | Continuity of care (loss of contacts with services, lack of appropriate referral, satisfaction, interagency communication, clinical outcomes) |
| Healthcare utilisation | Patient initiated health care communication; Hospitalisation | Attending medical appointments; Having a medical home; Avoiding unnecessary hospitalisations | Health care utilisation; Gaps in medical care | Health and social care resource utilisation |
| Understanding health insurance | − | understanding health insurance options | Loss of health insurance; Health coverage issues | − |
| Having a social network | − | Having a social network of friends | − | − |
Table 5.
Sharma et al.’s [29] outcome indicators for the role of the team and organisation in health transition.
Table 5.
Sharma et al.’s [29] outcome indicators for the role of the team and organisation in health transition.
| Stage of Health Transition | Health Care Professional | Health System |
|---|---|---|
| Preparation | Use of transition care plans | Development of transition policy |
| Assessment of transition readiness | ||
| Young person/family education and counselling | Care coordination | |
| Transfer of care | Preparation of patient summary | Use of patient summary |
| Communication | Communication between paediatric-adult systems | |
| Post transfer | Intake policy for transferring patients | Quality of intake to adult care |
| Care coordination | ||
| Financial costs and savings |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Farre, A.; McDonagh, J.E. Helping Health Services to Meet the Needs of Young People with Chronic Conditions: Towards a Developmental Model for Transition. Healthcare 2017, 5, 77. https://doi.org/10.3390/healthcare5040077
AMA Style
Farre A, McDonagh JE. Helping Health Services to Meet the Needs of Young People with Chronic Conditions: Towards a Developmental Model for Transition. Healthcare. 2017; 5(4):77. https://doi.org/10.3390/healthcare5040077
Chicago/Turabian StyleFarre, Albert, and Janet E. McDonagh. 2017. "Helping Health Services to Meet the Needs of Young People with Chronic Conditions: Towards a Developmental Model for Transition" Healthcare 5, no. 4: 77. https://doi.org/10.3390/healthcare5040077
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.