
Mental Health in Cypriot Citizens of the Rural Health Centre Kofinou


Abstract
:1. Introduction
2. Materials and Methodology
Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. HADS Scale
3.3. HADS Multivariate Analysis
3.4. GDS Scale
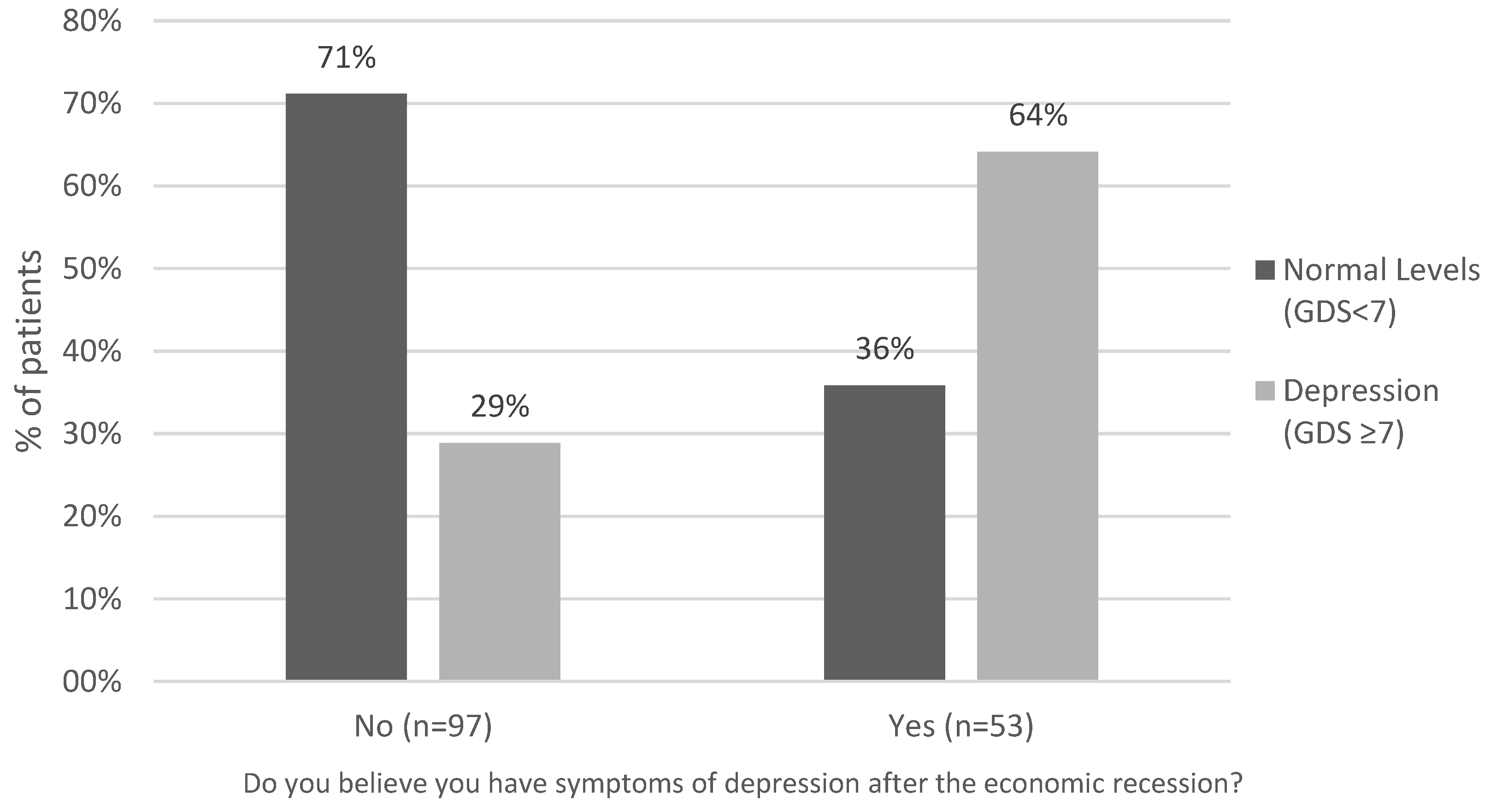
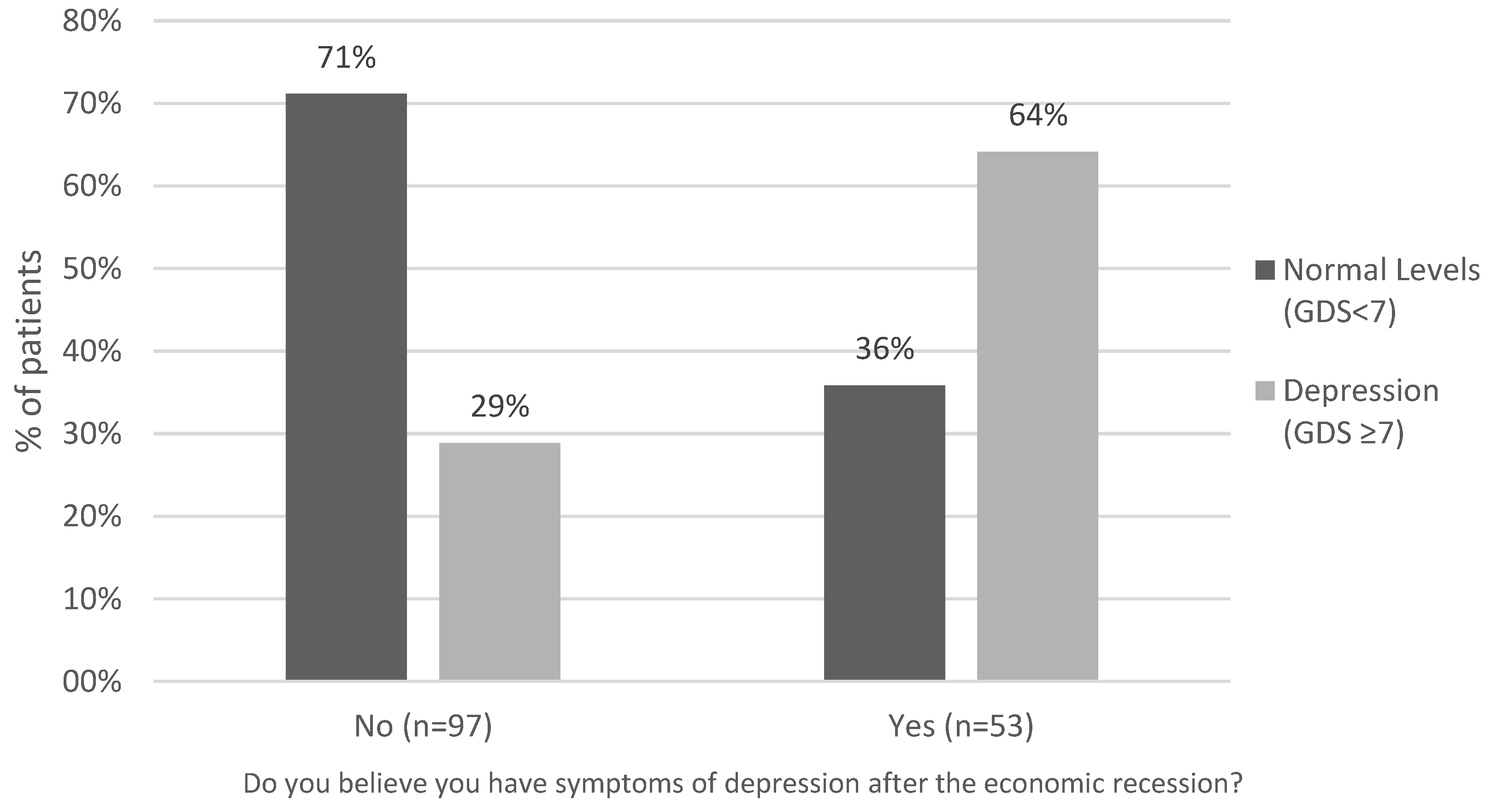
Reference to Depression Symptoms
3.5. GDS Multivariate Analysis
4. Discussion
- (a)
- Appropriate comprehension of the questionnaires by the participants, especially in cases where the patients were uneducated, could not be guaranteed. Senior citizens required guidance throughout the process, either because of a low educational level or because of a physical disability.
- (b)
- This is a cross section of data and thus we cannot interpret any of our findings as causal or generalize for the whole population. It is vital to obtain information from the general population, as this study is limited to people who sought medical help.
5. Future Recommendations
5.1. Political Authority
5.2. Health Practitioners
6. Conclusions
Author Contributions
Conflicts of Interest
References
- Michopoulos, I.; Kalkavoura, C.; Michalopoulou, P.; Fineti, K.; Kalemi, G.; Psara, M.L.; Gournelis, R.; Christodoulou, C.; Douzenis, A.; Patapis, P.; et al. Hospital Anxiety and Depression Scale at General Hospital (HADS): Validation in a Greek hospital sample. Ann. Gen. Psychiatry 2008, 7. (In Greek) [Google Scholar] [CrossRef] [PubMed]
- Fountoulakis, K.; Tsolaki, M.; Iacovides, A.; Yesavage, J.; O’Hara, R.; Kazis, A.; Ierodiakonou, C. The validation of the short form of the Geriatric Depression Scale (GDS) in Greece. Aging Clin. Exp. Res. 1999, 11, 367–372. [Google Scholar] [CrossRef]
- Ng, K.; Agius, M.; Zaman, R. The effects of economic crisis on mental health. Eur. Psychiatry 2011, 26, 663. [Google Scholar] [CrossRef]
- Mousoulos, S. The Santums of the Economic Crisis in Cyprus; Epiphaniou Publications: Nicosia, Italy, 2014. (In Greek) [Google Scholar]
- Burchell, B. Social change and the experience of unemployment. In The Effects of Labour Market Position, Job Insecurity and Unemployment on Phychological Health; Gallie, D., Ed.; Oxford University Press: Oxford, UK, 1994. [Google Scholar]
- Stuckler, D.; Basu, S.; Suhrcke, M.; Coutts, A.; McKee, M. The public health effect of economic crisis and alternative policy responses in Europe: An empirical analysis. Lancet 2009, 374, 315–323. [Google Scholar] [CrossRef]
- Paul, K.; Moser, K. Unemployment impairs mental health: Meta-analyses. J. Vocat. Behav. 2009, 74, 264–282. [Google Scholar] [CrossRef]
- WHO. Impact of Financial Crisis on Health: A Truly Global Solution Is Needed. Available online: http://www.who.int/mediacentre/news/statements/2009/financial_crisis_20090401/en/ (accessed on 24 January 2015).
- Giotakos, O. Financial Crisis and Mental Health. Eur. Psychiatry 2010, 21, 195–204. [Google Scholar]
- Siklaphidou, P.; Zeleni, D.; Leivaditis, M. Transcultural Psychiatry and Depression. Brain Arch. Neurol. Phychiatry 2011, 48, 146–150. (In Greek) [Google Scholar]
- Spyropoulou, A.; Zerva, G. Introduction to “Woman and Mental Health”. Available online: https://entosfylou.wordpress.com/ (accessed on 28 October 2015). (In Greek)
- Kantartzis, S. Disorders. Available online: http://www.kanartzis-soterios.gr/html/katathlipsi.html (accessed on 28 October 2015). (in Greek).
- Marmot, M. Status Syndrome: How Your Social Standing Directly Affects Your Health and Life Expectancy; Bloomsbury Publishing Plc: London, UK, 2004. [Google Scholar]
- Blane, D. Commentary: Explanations of the Difference in Mortality Risk between Different Educational Groups. Int. J. Epidemiol. 2003, 32, 355–356. [Google Scholar] [CrossRef] [PubMed]
- Economou, A.; Nikolaou, A.; Theodossiou, I. Are recessions harmful to health after all? Evidence from the European Union. J. Econ. Stud. 2008, 35, 368–384. [Google Scholar] [CrossRef]
- Falagas, M.E.; Vouloumanou, E.K.; Mavros, M.N.; Karageorgopoulos, D.E. Economic crises and mortality: A review of the literature. Int. J. Clin. Pract. 2009, 63, 1128–1135. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | HADS Scale | GDS Scale | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Gender | Woman | 84 | 56.0% | 77 | 51.3% |
| Man | 66 | 44.0% | 73 | 48.7% | |
| Age | 47 ± 11.5 years/MIN = 23, MAX = 64 | 72.9 ± 5.5 years/MIN = 66, MAX = 90 | |||
| Education level | None | 0 | 0.0% | 11 | 7.3% |
| Primary School | 32 | 21.3% | 99 | 66.0% | |
| Secondary | 12 | 8.0% | 17 | 11.3% | |
| Lyceum | 63 | 42.0% | 19 | 12.7% | |
| Higher Education | 35 | 23.3% | 4 | 2.7% | |
| Master/PhD | 8 | 5.3% | 0 | 0.0% | |
| Annual income | Unemployed | 15 | 10.0% | 0 | 0.0% |
| Until 8000 | 46 | 30.7% | 100 | 66.7% | |
| 8001–12,000 | 21 | 14.0% | 30 | 20.0% | |
| 12,001–18,000 | 25 | 16.7% | 13 | 8.7% | |
| 18,001–30,000 | 26 | 17.3% | 6 | 4.0% | |
| 30,001 and over | 17 | 11.3% | 1 | 0.7% | |
| Reduction of the annual income due to economic crisis in the last year | 116 | 77.3% | 93 | 62.0% | |
| Presence of chronic disease | 70 | 46.7% | 139 | 92.7% | |
| Blood hypertension | 42 | 60.0% | 100 | 66.7% | |
| Diabetes | 22 | 31.4% | 58 | 38.7% | |
| Lipid disorder | 28 | 40.0% | 73 | 48.7% | |
| Autoimmune disease | 0 | 0.0% | 1 | 0.7% | |
| Heart disease | 7 | 10.0% | 32 | 21.3% | |
| Other | 12 | 8.0% | 4 | 2.7% | |
| Do you believe you have symptoms of depression after the economic recession? | - | - | 53 | 35.3% | |
| Variables | Anxiety Level | Depression Level | ||
|---|---|---|---|---|
| n | % | n | % | |
| Normal Level | 65 | 43.3% | 75 | 50.0% |
| Mild Level | 30 | 20.0% | 32 | 21.3% |
| Moderate Level | 35 | 23.3% | 31 | 20.7% |
| Severe Level | 20 | 13.3% | 12 | 8.0% |
| Total | 150 | 100% | 150 | 100.0% |
| Dependent Variable | HADS-Total Score (Emotional Distress) | HADS-Anxiety | HADS-Depression | |||
|---|---|---|---|---|---|---|
| Predictors | b * | p | b * | p | b * | p |
| (Constant) | 25.6 | <0.001 | 14.098 | <0.001 | 11.502 | <0.001 |
| Age | −0.059 | 0.445 | −0.039 | 0.355 | −0.019 | 0.621 |
| Gender (women) | −2.058 | 0.138 | −1.296 | 0.094 | −0.762 | 0.274 |
| Chronic disease | 5.449 | <0.001 | 2.817 | 0.001 | 2.632 | 0.001 |
| Annual Income | −1.066 | 0.017 | −0.642 | 0.01 | −0.425 | 0.058 |
| Education Level | −2.633 | <0.001 | −1.196 | 0.003 | −1.436 | <0.001 |
| Reduction in earnings (>35%) | 2.917 | 0.063 | 1.177 | 0.178 | 1.741 | 0.028 |
| Model fit indices | ||||||
| F (p value) | 11.309 (<0.001) | 8.986 (<0.001) | 11.696 (<0.001) | |||
| Adjusted R2 | 0.293 | 0.243 | 0.301 | |||
| Variables | b | SE | Standardised b | t | p |
|---|---|---|---|---|---|
| (Constant) | −5.338 | 4.505 | −1.185 | 0.238 | |
| Gender (female) | −1.958 | 0.687 | −0.248 | −2.849 | 0.005 |
| Age | 0.161 | 0.058 | 0.223 | 2.778 | 0.006 |
| Annual income: | −0.703 | 0.39 | −0.153 | −1.801 | 0.074 |
| Chromic disease | 1.279 | 1.149 | 0.084 | 1.113 | 0.267 |
| Reduction in earnings (>20%) | 0.739 | 0.665 | 0.086 | 1.112 | 0.268 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stavrou, G.; Paikousis, L.; Jelastopulu, E.; Charalambous, G. Mental Health in Cypriot Citizens of the Rural Health Centre Kofinou. Healthcare 2016, 4, 81. https://doi.org/10.3390/healthcare4040081
Stavrou G, Paikousis L, Jelastopulu E, Charalambous G. Mental Health in Cypriot Citizens of the Rural Health Centre Kofinou. Healthcare. 2016; 4(4):81. https://doi.org/10.3390/healthcare4040081
Chicago/Turabian StyleStavrou, Georgios, Lefkios Paikousis, Eleni Jelastopulu, and Georgios Charalambous. 2016. "Mental Health in Cypriot Citizens of the Rural Health Centre Kofinou" Healthcare 4, no. 4: 81. https://doi.org/10.3390/healthcare4040081