
The Impact of Antenatal Psychological Group Interventions on Psychological Well-Being: A Systematic Review of the Qualitative and Quantitative Evidence


Abstract
:1. Introduction
1.1. Background
1.2. The Theoretical Bases of Interventions
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
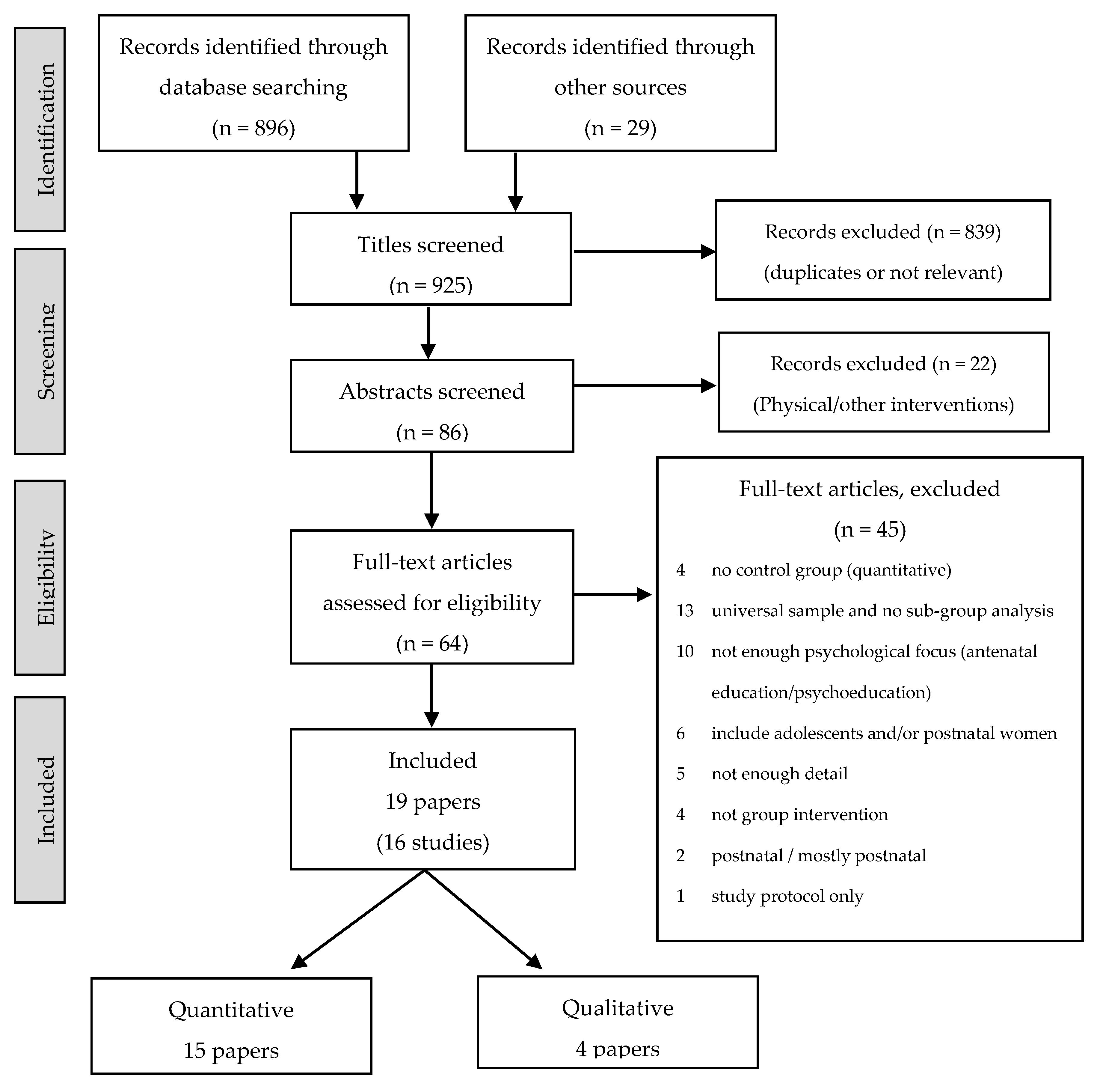
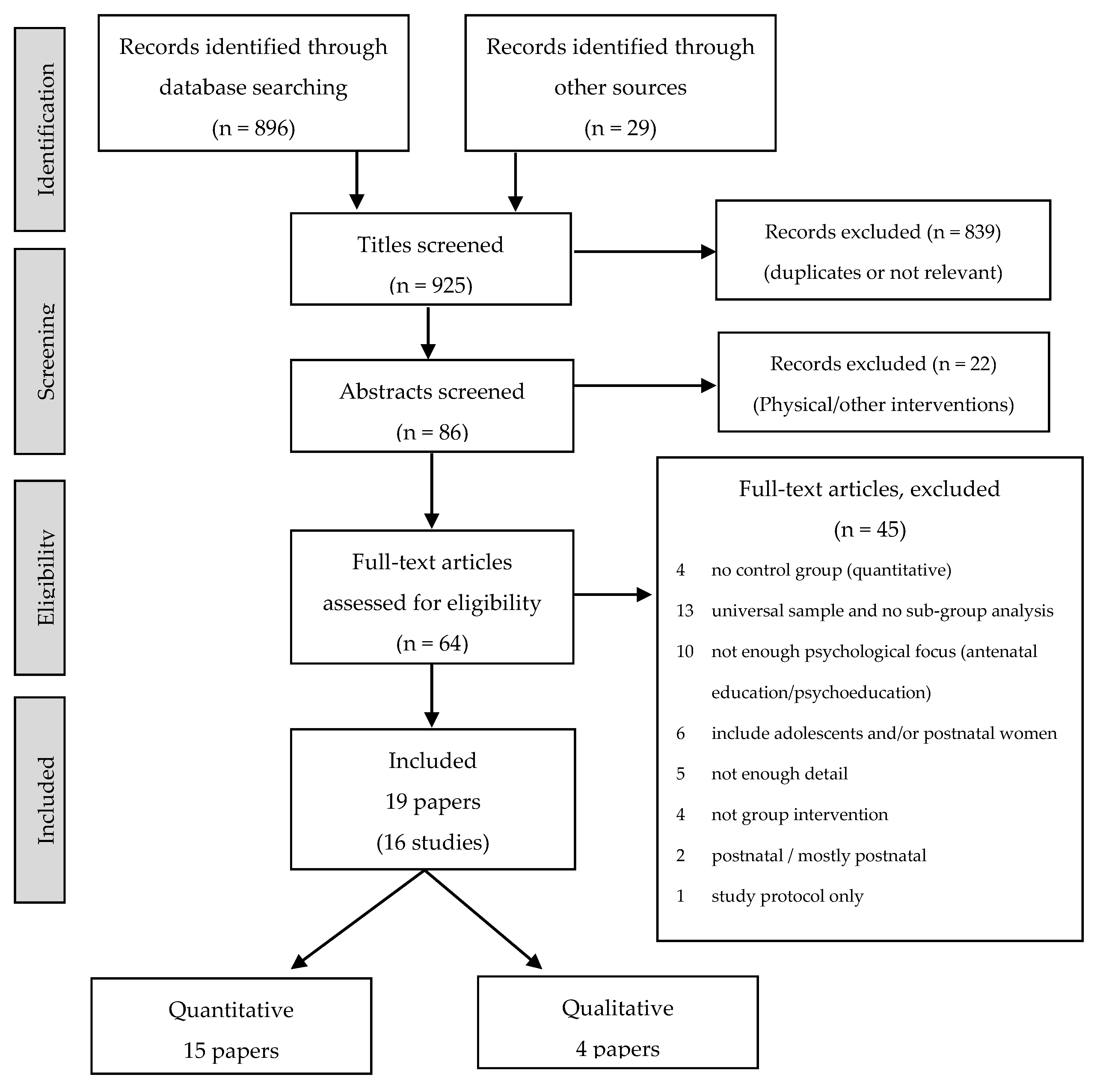
3.1. Identified Studies
3.2. Interventions
3.2.1. Psychological Approaches
3.2.2. Intervention Formats
3.3. Study and Participant Characteristics
3.3.1. Study Characteristics
3.3.2. Participant Characteristics
3.4. Quantitative Studies: Findings
3.4.1. Depressive Symptoms
3.4.2. Depressive Episodes
3.4.3. Anxiety
3.4.4. Stress
3.4.5. Potential Negative Effects of Interventions
3.4.6. Impact of Participant Characteristics
3.4.7. Impact of Intervention Characteristics
3.5. Findings from the Thematic Synthesis of Qualitative Studies
3.5.1. Qualitative Approaches
3.5.2. Analytical Themes
Connecting
“At the “project”, they understood me … I found a family with the people from the project and I liked that a lot. But I couldn’t have done it differently because I felt comfortable with those women [61].” “A lot of the meetings was about making friends, I’ve got a busy life, now if I feel I’m not good at anything we can just ring each other [37].” “It was great being around women who were in a similar situation to me and I liked being able to talk about my own experience [58].” “… the small and large group discussions … provided an opportunity to connect and relate to other women in the programme [58].”
Sharing
“Listening to them made us feel important … that was important … because like I always say, some people may be in the same situation as me [61].” “Sharing experiences and realising that they were not alone in what they felt (especially when these were negative feelings) helped women to normalise their experiences; in this way the course acted as a normalising catalyst [38].” “Being able to talk to someone and listen to advice [61].” “I learned that this is a shared human experience, and I’m not the only one who suffers [58].”
Understanding
“I have learned how to better understand my thoughts and my body. How my thoughts can trigger feelings and how these thoughts are not always factual [58].” “I became aware of my mood and I realised that what I had was not something bad … what I really had was low self-esteem [61].” “Yeah, that was fine, it was good, learning things, you know, social support, turning it down, asking for help … [37].”
Re-Adjusting and Normalising
“This is something that happens to women, after being involved in the project, it became more real to me [61].” “Being more accepting of myself, being more gentle to oneself, appreciating self-kindness, accepting anxiety as part of who I am, accepting my thoughts [58].” “Whenever I feel sad or depressed, I try to think about something nice, something that makes me feel happy, I learned all that there [61].”
4. Discussion
4.1. Interventions
4.2. Heterogeneity and Methodological Limitations
4.3. Effectiveness of Interventions
4.4. Women’s Experiences
4.4.1. Qualitative Studies
4.4.2. Women’s Feedback in Quantitative Studies
4.5. Combining Qualitative and Quantitaive
4.6. Strengths and Limitations of This Review
5. Conclusions
Acknowledgments
Conflicts of Interest
Abbreviations
| BDI | Beck Depression Inventory |
| CASP | Critical Appraisal Skills Programme |
| CBT | Cognitive Behavioural Therapy |
| CES-D | Centre for Epidemiologic Studies Depression scale |
| EPDS | Edinburgh Postnatal Depression Scale |
| IPT | Interpersonal Therapy |
| MFN | Mindfulness |
| NICE | National Institute for Health and Care Excellence |
| PMI | Perinatal Mental Illness |
| PND | Postnatal Depression |
| PSS | Perceived Stress Scale |
| STAI | Spielberger State-Trait Anxiety Inventory |
References
- Diego, M.A.; Field, T.; Hernandez-Reif, M.; Schanberg, S.; Kuhn, C.; Gonzalez-Quintero, V.H. Prenatal depression restricts fetal growth. Early Hum. Dev. 2009, 85, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Gavin, A.R.; Holzman, C.; Siefert, K.; Tian, Y. Maternal depressive symptoms, depression, and psychiatric medication use in relation to risk of preterm delivery. Womens Health Issues 2009, 19, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Grote, N.K.; Bridge, J.A.; Gavin, A.R.; Melville, J.L.; Iyengar, S.; Katon, W.J. A Meta-analysis of depression during pregnancy and the risk of preterm birth, low birth weight, and intrauterine growth restriction. Arch. Gen. Psychiatry 2010, 67, 1012–1024. [Google Scholar] [CrossRef] [PubMed]
- Pawlby, S.; Hay, D.F.; Sharp, D.; Waters, C.S.; O’Keane, V. Antenatal depression predicts depression in adolescent offspring: Prospective longitudinal community-based study. J. Affect. Disord. 2009, 113, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Glover, V.; O’Connor, T.G.; O’Donnell, K. Prenatal stress and the programming of the HPA axis. Neurosci. Biobehav. Rev. 2010, 35, 17–22. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, K.J.; Bugge Jensen, A.; Freeman, L.; Khalife, N.; O’Connor, T.G.; Glover, V. Maternal prenatal anxiety and downregulation of placental 11β-HSD2. Psychoneuroendocrinology 2012, 37, 818–826. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, K.J.; Glover, V.; Jenkins, J.; Browne, D.; Ben-Shlomo, Y.; Golding, J.; O’Connor, T.G. Prenatal maternal mood is associated with altered diurnal cortisol in adolescence. Psychoneuroendocrinology 2013, 38, 1630–1638. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.M.; Lam, S.K.; Sze Mun Lau, S.M.; Chong, C.S.; Chui, H.W.; Fong, D.Y. Prevalence, course, and risk factors for antenatal anxiety and depression. Obstet. Gynecol. 2007, 110, 1102–1112. [Google Scholar] [CrossRef] [PubMed]
- Kieffer, E.C.; Caldwell, C.H.; Welmerink, D.B.; Welch, K.B.; Sinco, B.R.; Guzmán, J.R. Effect of the healthy MOMs lifestyle intervention on reducing depressive symptoms among pregnant latinas. Am. J. Community Psychol. 2013, 51, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Rubertsson, C.; Wickberg, B.; Gustavsson, P.; Radestad, I. Depressive symptoms in early pregnancy, two months and one year postpartum-prevalence and psychosocial risk factors in a national Swedish sample. Arch. Womens Ment. Health 2005, 8, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Milgrom, J.; Gemmill, A.W.; Bilszta, J.L.; Hayes, B.; Barnett, B.; Brooks, J.; Ericksen, J.; Ellwood, D.; Buist, A. Antenatal risk factors for postnatal depression: A large prospective study. J. Affect. Disord. 2008, 108, 147–157. [Google Scholar] [CrossRef] [PubMed]
- NICE. Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance. Available online: https://www.nice.org.uk/guidance/cg45 (accessed on 12 February 2015).
- NICE. Antenatal and Postnatal Mental Health: Clinical Management and Service Guidance. Available online: http://www.nice.org.uk/guidance/cg192/ (accessed on 21 December 2014).
- Coelho, H.F.; Murray, L.; Royal-Lawson, M.; Cooper, P.J. Antenatal anxiety disorder as a predictor of postnatal depression: A longitudinal study. J. Affect. Disord. 2011, 129, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Stowe, Z.N.; Hostetter, A.L.; Newport, D.J. The onset of postpartum depression: Implications for clinical screening in obstetrical and primary care. Am. J. Obstet. Gynecol. 2005, 192, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.L. Peer support within a health-care context: a concept analysis. Int. J. Nurs. Stud. 2003, 40, 321–332. [Google Scholar] [CrossRef]
- Mead, S. Defining peer support. Intentional peer support: An alternative approach. Available online: http://www.intentionalpeersupport.org (accessed on 5 May 2015).
- Davidson, L.; Chinman, M.; Sells, D.; Rowe, M. Peer support among adults with serious mental illness: A report from the field. Schizophr. Bull. 2006, 32, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Corrison, P.W.; Mueser, K.T.; Bond, G.R.; Drake, R.E.; Solomon, P. Principles and Practice of Psychiatric Rehabilitation: An Empirical Approach; Guildford Press: New York, NY, USA, 2008. [Google Scholar]
- Pfeiffer, P.N.; Heisler, M.; Piette, J.D.; Rogers, M.A.; Valenstein, M. Efficacy of peer support interventions for depression: A meta-analysis. Gen. Hosp. Psychiatry 2011, 33, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.C.; Jomeen, J.; Hayter, M. The impact of peer support in the context of perinatal mental illness: A meta-ethnography. Midwifery 2014, 30, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Chabrol, H.; Teissedere, F.; Saint-Jean, M.; Teisseyre, N.; Rogé, B.; Mullet, E. Prevention and treatment of post-partum depression: A controlled randomized study on women at risk. Psychol. Med. 2002, 32, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Austin, M.P.; Frilingos, M.; Lumley, J.; Hadzi-Pavlovic, D.; Roncolato, W.; Acland, S.; Saint, K.; Segal, N.; Parker, G. Brief antenatal cognitive behaviour therapy group intervention for the prevention of postnatal depression and anxiety: A randomised controlled trial. J. Affect. Disord. 2008, 105, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Stuart, S. Interpersonal psychotherapy for postpartum depression. Clin. Psychol. Psychother. 2012, 19, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Sockol, L.E.; Epperson, C.N.; Barber, J.P. A meta-analysis of treatments for perinatal depression. Clin. Psychol. Rev. 2011, 31, 839–849. [Google Scholar] [CrossRef] [PubMed]
- Bledsoe, S.E.; Grote, N.K. Treating depression during pregnancy and the postpartum: A preliminary meta-analysis. Res. Soc. Work Pract. 2006, 16, 109–120. [Google Scholar] [CrossRef]
- O’Hara, M.W.; Stuart, S.; Gorman, L.L.; Wenzel, A. EFficacy of interpersonal psychotherapy for postpartum depression. Arch. Gen. Psychiatry 2000, 57, 1039–1045. [Google Scholar] [CrossRef] [PubMed]
- Guardino, C.M.; Dunkel Schetter, C.; Bower, J.E.; Lu, M.C.; Smalley, S.L. Randomised controlled pilot trial of mindfulness training for stress reduction during pregnancy. Psychol. Health 2014, 29, 334–349. [Google Scholar] [CrossRef] [PubMed]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Grossman, P.; Niemann, L.; Schmidt, S.; Walach, H. Mindfulness-based stress reduction and health benefits: A meta-analysis. J. Psychosom. Res. 2004, 57, 35–43. [Google Scholar] [CrossRef]
- Chiesa, A.; Serretti, A. Mindfulness-based stress reduction for stress management in healthy people: A review and meta-analysis. J. Altern. Complement. Med. 2009, 15, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008. [Google Scholar] [CrossRef] [PubMed]
- NICE. The Guidelines Manual: Appendices B-I. Available online: http://publications.nice.org.uk/pmg6b (accessed on 12 January 2015).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Bittner, A.; Peukert, J.; Zimmermann, C.; Junge-Hoffmeister, J.; Parker, L.S.; Stöbel-Richter, Y.; Weidner, K. Early intervention in pregnant women with elevated anxiety and depressive symptoms: Efficacy of a cognitive-behavioral group program. J. Perinat. Neonatal Nurs. 2014, 28, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Richter, J.; Bittner, A.; Petrowski, K.; Junge-Hoffmeister, J.; Bergmann, S.; Joraschky, P.; Weidner, K. Effects of an early intervention on perceived stress and diurnal cortisol in pregnant women with elevated stress, anxiety, and depressive symptomatology. J. Psychosom. Obstet. Gynecol. 2012, 33, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Wheatley, S.; Brugha, T. ”Just Because I Like it Doesn’t Mean it has to Work”: Personal experiences of an antenatal psychosocial intervention designed to prevent postnatal depression. J. Public Ment. Health 1999, 1, 26–31. [Google Scholar] [CrossRef]
- Wheatley, L.S.; Brugha, S.T.; Shapiro, A.D. Exploring and enhancing engagement to the psychosocial intervention ”Preparing for Parenthood”. Arch. Womens Ment. Health 2003, 6, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Brugha, T.S.; Wheatley, S.; Taub, N.A.; Culverwell, A.; Friedman, T.; Kirwan, P.; Jones, D.R.; Shapiro, D.A. Pragmatic randomized trial of antenatal intervention to prevent post-natal depression by reducing psychosocial risk factors. Psychol. Med. 2000, 30, 1273–1281. [Google Scholar] [CrossRef] [PubMed]
- Kozinszky, Z.; Dudas, R.B.; Devosa, I.; Csatordai, S.; Tóth, É.; Szabó, D.; Sikovanyecz, J.; Barabás, K.; Pál, A. Can a brief antepartum preventive group intervention help reduce postpartum depressive symptomatology? Psychother. Psychosom. 2012, 81, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Leung, S.S. K.; Lam, T.H. Group antenatal intervention to reduce perinatal stress and depressive symptoms related to intergenerational conflicts: A randomized controlled trial. Int. J. Nurs. Stud. 2012, 49, 1391–1402. [Google Scholar] [CrossRef] [PubMed]
- Lara, M.A.; Navarro, C.; Navarrete, L. Outcome results of a psycho-educational intervention in pregnancy to prevent PPD: A randomized control trial. J. Affect. Disord. 2010, 122, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, R.F.; Le, H.N.; Ippen, C.G.; Diaz, M.A.; Urizar, G.G., Jr.; Soto, J.; Mendelson, T.; Delucchi, K.; Lieberman, A.F. Prevention of postpartum depression in low-income women: Development of the Mamás y Bebés/Mothers and babies course. Cogn. Behav. Pract. 2007, 14, 70–83. [Google Scholar] [CrossRef]
- Zlotnick, C.; Miller, I.W.; Pearlstein, T.; Howard, M.; Sweeney, P. A Preventive intervention for pregnant women on public assistance at risk for postpartum depression. Am. J. Psychiatry 2006, 163, 1443–1445. [Google Scholar] [CrossRef] [PubMed]
- Urizar, G.G.; Muñoz, R.F. Impact of a prenatal cognitive-behavioral stress management intervention on salivary cortisol levels in low-income mothers and their infants. Psychoneuroendocrinology 2011, 36, 1480–1494. [Google Scholar] [CrossRef] [PubMed]
- Vieten, C.; Astin, J. Effects of a mindfulness-based intervention during pregnancy on prenatal stress and mood: Results of a pilot study. Arch. Womens Ment. Health 2008, 11, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 1365–1367. [Google Scholar] [CrossRef]
- Spielberger, C.; Gorsuch, R.L.; Lushene, R.E. Manuar for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Ji, S.; Long, Q.; Jeffrey Newport, D.; Na, H.; Knight, B.; Zach, E.B.; Morris, N.J.; Kutner, M.; Stowe, Z.N. Validity of depression rating scales during pregnancy and the postpartum period: Impact of trimester and parity. J. Psychiatr. Res. 2011, 45, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Murray, D.; Cox, J.L. Screening for depression during pregnancy with the edinburgh depression scale (EDDS). J. Reprod. Infant Psychol. 1990, 8, 99–107. [Google Scholar] [CrossRef]
- Holcomb, W.L., Jr.; Stone, L.S.; Lustman, P.J.; Gavard, J.A.; Mostello, D.J. Screening for depression in pregnancy: Characteristics of the beck depression inventory. Obstet. Gynecol. 1996, 88, 1021–1025. [Google Scholar] [PubMed]
- Gunning, M.D.; Denison, F.C.; Stockley, C.J.; Ho, S.P.; Sandhu, H.K.; Reynolds, R.M. Assessing maternal anxiety in pregnancy with the State-Trait Anxiety Inventory (STAI): Issues of validity, location and participation. J. Reprod. Infant Psychol. 2010, 28, 266–273. [Google Scholar] [CrossRef]
- Karam, F.; Bérard, A.; Sheehy, O.; Huneau, M.C.; Briggs, G.; Chambers, C.; Einarson, A.; Johnson, D.; Kao, K.; Koren, G.; et al. Reliability and validity of the 4-item perceived stress scale among pregnant women: Results from the OTIS antidepressants study. Res. Nurs. Health 2012, 35, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Jomeen, J.; Spiteri, C.; Draper, J.; Martin, C. Exploring the relationship between postpartum physical recovery and wellbeing. J. Reprod. Infant Psychol. 2014, 32, 31–33. [Google Scholar]
- Goodman, J.H.; Guarino, A.; Chenausky, K.; Klein, L.; Prager, J.; Petersen, R.; Forget, A.; Freeman, M. CALM Pregnancy: Results of a pilot study of mindfulness-based cognitive therapy for perinatal anxiety. Arch. Womens Ment. Health 2014, 17, 373–387. [Google Scholar] [CrossRef] [PubMed]
- Crockett, K.; Zlotnick, C.; Davis, M.; Payne, N.; Washington, R. A depression preventive intervention for rural low-income African-American pregnant women at risk for postpartum depression. Arch. Womens Ment. Health 2008, 11, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Le, H.N.; Perry, D.F.; Stuart, E.A. Randomized controlled trial of a preventive intervention for perinatal depression in high-risk Latinas. J. Consult. Clin. Psychol. 2011, 79, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Le, H.N.; Perry, D.F.; Genovez, M.; Cardeli, E. In their own voices: Latinas’ experiences with a randomized controlled trial. Qual. Health Res. 2013, 23, 834–846. [Google Scholar] [CrossRef] [PubMed]
- Zlotnick, C.; Johnson, S.L.; Miller, I.W.; Pearlstein, T.; Howard, M. Postpartum depression in women receiving public assistance: Pilot study of an interpersonal-therapy-oriented group intervention. Am. J. Psychiatry 2001, 158, 638–640. [Google Scholar] [CrossRef] [PubMed]
- Kirschbaum, C.; Hellhammer, D.H. Salivary cortisol in psychoneuroendocrine research: Recent developments and applications. Psychoneuroendocrinology 1994, 19, 313–333. [Google Scholar] [CrossRef]
- Hellhammer, D.H.; Wüst, S.; Kudielka, B.M. Salivary cortisol as a biomarker in stress research. Psychoneuroendocrinology 2009, 34, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Hjorskov, N.; Garde, A.H.; Ørbæk, P.; Hansen, Å.M. Evaluation of salivary cortisol as a biomarker of self-reported mental stress in field studies. Stress Health 2004, 20, 91–98. [Google Scholar] [CrossRef]
- Liou, S.R.; Wang, P.; Cheng, C.Y. Longitudinal study of perinatal maternal stress, depressive symptoms and anxiety. Midwifery 2014, 30, 795–801. [Google Scholar] [CrossRef] [PubMed]
- Parcells, D.A. Women’s mental health nursing: Depression, anxiety and stress during pregnancy. J. Psychiatr. Ment. Health Nurs. 2010, 17, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Clatworthy, J. The effectiveness of antenatal interventions to prevent postnatal depression in high-risk women. J. Affect. Disord. 2012, 137, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.L.; Creedy, D. Psychosocial and psychological interventions for preventing postpartum depression (Review). The Cochrane Library 2007, issue 4. Available online: http://apps.who.int/rhl/reviews/langs/CD001134.pdf (accessed on 20 March 2016).
- Simoni, J.M.; Franks, J.C.; Lehavot, K.; Yard, S.S. Peer interventions to promote health: Conceptual considerations. Am. J. Orthopsychiatry 2011, 81, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Mead, S.; MacNeil, C. Peer support: What makes it unique? Int. J. Psychosoc. Rehabil. 2006, 10, 29–37. [Google Scholar]
- Jomeen, J. Women’s psychological status in pregnancy and childbirth—Measuring or understanding (editorial). J. Reprod. Infant Psychol. 2014, 30, 337–340. [Google Scholar] [CrossRef]
- Dennis, C.L.; Hodnett, E.; Kenton, L.; Weston, J.; Zupancic, J.; Stewart, D.E.; Kiss, A. Effect of peer support on prevention of postnatal depression among high risk women: multisite randomised controlled trial. BMJ 2009. [Google Scholar] [CrossRef] [PubMed]
- Austin, M.P. Targeted group antenatal prevention of postnatal depression: A review. Acta Psychiatr. Scand. 2003, 107, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.L. Preventing postpartum depression part II: A critical review of nonbiological interventions. Canadian journal of psychiatry. Can. J. Psychiatry 2004, 49, 526–538. [Google Scholar] [PubMed]

{kind=link}
| Intervention | Participants | Study Design |
|---|---|---|
| Quantitative Studies | ||
| Austin et al. 2008 (Australia) [23] | ||
| Brief CBT intervention Aims: preventing/managing stress, anxiety and low mood Length: 12 h (6 × 2 h) Group size: no information Additional: information booklet, follow-up session Facilitator: clinical psychologist, midwife Evaluation/monitoring: no information | 277 women with depression/anxiety symptoms or at risk of depression/anxiety Characteristics: mean age 31 years; 97.8% partnered; 9.7% low income; 88.1% English speaking; 65.3% first child Mean gestational age: 25.7 weeks (range: 14 to 36 weeks) Baseline symptoms: MINI: depression 19.1%, anxiety 26%, depression or anxiety 32.5%; EPDS > 12 14.3% of completers | RCT; control: information booklet Screening: EPDS > 10/ANRQ > 23/history of depression 1 Allocation: randomisation on 2:1 basis (intervention:control) after screening; concealment unclear Outcome measures: depression (MINI), depressive symptoms (EPDS), anxiety (STAI, MINI) Time points: pre-/post-intervention; 2 and 4 months postnatal Attrition/participation 2: high attrition, low participation Quality assessment: B (differences in EPDS baseline scores; high rate attrition; wide range of gestational ages) Findings 3: No significant difference between groups (trend towards greater reduction in anxiety for intervention) |
| Bittner et al. 2014 (Germany) [35] | ||
| “LOS—Lebensfroh and optimistisch durch die Schwangerschaft“; CBT-based Aims: increased awareness of ongoing emotions, thoughts and behaviours Length: 12 h (8 × 90 min) Group size: 4–6 Factilitator: clinical psychologist Evaluation/monitoring: participant feedback | 160 women with elevated depressive/anxiety symptoms 4 Characteristics: mean age 29.5 years; 100% partnered; medium/high socio-economic status; 64.9% first child Mean gestational age: 16.4 weeks Baseline symptoms: STAI 38; EPDS: 7.4 (int), 5.9 (con) | RCT; control: usual care Screening: PDQ > 14 / STAI > 36 / BDI-S > 20 Allocation: random; concealed Outcome measures: depressive symptoms (EPDS), anxiety (STAI), dysfunctional attitudes (DAS), anxiety sensitivity (ASI), social support (SOZU), quality of relationship (PFB), fear of childbirth (GAS) Time points: pre-/post-intervention; 3 months postnatal Attrition/participation: high attrition, low participation Quality assessment: A (but high drop-out rate) Findings: no intervention effect on anxiety or depression; positive short-term effect on quality of relationship for intervention; women with elevated baseline depressive symptoms: significant decrease in depressive symptoms postnatally in intervention group |
| Brugha et al. 2000 (UK) [39] | ||
| “Preparing for Parenthood“; CBT elements and psychoeducation Aims: Preventing PND Length: 12 h (6 × 2 h) Group size: 8–16 Additional: introductory meeting, PN reunion; one session with partners Facilitator: nurses, occupational therapists Evaluation/montitoring: participant feedback; supervision | 209 women at increased risk of depression Characteristics: median age 19 years; 73% European, others mostly Asian; 100% first child Gestational age: >28 weeks Baseline symptoms: GHQ-D high: 22/23% | RCT; control: usual care Screening: “Pregnancy and You“ screening questionnaire 5; 12–20 weeks Allocation: randomisation after screening (stratification based on 3 diagnostic factors); concealed Outcome measures: depression (SCAN), depressive symptoms (modified GHQ-D, EPDS); various risk factors for PND Time points: pre-intervention; 3 months postnatal Attrition/participation: low attrition, low participation Quality assessment: B (high attrition rates, insufficient detail on baseline comparisons) Findings: no intervention effect on levels of postnatal depression |
| Crockett et al. 2008 (US) [59] | ||
| “Reach Out, Stand Strong: Essentials for New Moms“ (ROSE) Program; IPT-based Aims: preventing PND Length: 6 h (4 × 90 min) Group size: no information Additional: individual PN booster session Facilitator: counsellors Evaluation/monitoring: participant feedback; audiotaping for adherence/supervision | 36 low-income African-American women, at risk of PND Characteristics: mean age 23.4 years; 13.9% partnered; mostly rural, low-income; 100% African American; 61.1% first child Gestational age range: 24–31 weeks Baseline symptoms: CSQ: mean score 34.5 6, no reported previous depressive episodes | Pilot RCT; control: usual care Screening: CSQ ≥ 27 Allocation: randomisation after screening; no further information Outcome measures: depressive symptoms (EPDS), PN adjustment (PPAQ), parenting stress (PSI) Time points: pre-/post-intervention; 2–3 weeks and 3 months postnatally Attrition/participation: medium attrition, high participation Quality assessment: B (no information on allocation; results not presented comprehensively, small sample) Findings: significant increase in PN adjustment for intervention; no difference between groups in EPDS scores |
| Guardino et al. 2014 (US) [28] | ||
| Mindful Awareness Practices (MAPS) course at UCLA Semel Institute’s (ongoing course, not specifically for pregnancy) Aims: Reducing stress Length: 12 h (6 × 2 h) Group size: no information Facilitator: no information Evaluation/monitoring: no information | 47 women with raised stress and/or anxiety Characteristics: mean age 33.1 years; 93.5% partnered; medium-high socio-economic status; 66% white; 78% first child Gestational age range: 10–25 weeks Baseline symptoms: previous diagnosis of depression 30%; previous diagnosis of anxiety disorder 31%; STAI 45.7, PSS 41.8 | Pilot RCT; control: reading (pregnancy book) Screening: PSS > 34 / PSA > 11 Allocation: randomisation (computerised) after screening; concealment unclear Outcome measures: perceived stress (PSS), pregnancy-specific anxiety (PSA), pregnancy-related anxiety (PRA), anxiety (STAI), mindfulness (FFMQ) Time points: pre-/post-intervention; 6 weeks after intervention Attrition/participation: medium attrition, medium participation Quality assessment: C (small sample; wide range of gestational ages; follow-up for some postnatally, others are possibly still pregnant) Findings: significantly larger decreases in pregnancy-specific anxiety pre- to post-intervention than control, not sustained at 6 weeks post-intervention |
| Kozinszky et al. 2012 (Hungary) [40] | ||
| CBT and IPT elements; including partners Aims: preventing PND Length: 12 h (4 × 3 h) Group size: <15 Facilitator: psychiatrists and health visitors Evaluation/monitoring: sessions recorded randomly checked for adherence | 1719 women Characteristics: mean age 27 years; 66% partnered; 14% low-income; 61% first child Gestational age: >25 weeks Baseline symptoms: antenatal depression 18.4%; history of major depression 5.6% | RCT; control: routine antenatal course Screening: none (but subgroup analysis) Allocation: randomisation (computerised) after eligibility criteria met, on ¾:1 (intervention:control) basis; concealment unclear Outcome measures: depression (LQ > 11), depressive symptoms (LQ); questionnaire on various risk factors of PND Time points: pre-intervention; 6-8 weeks postnatal Attrition/participation: low attrition, no information on participation Quality assessment: A (large sample; length of follow-up relatively short; no information on attendance rates) Findings: significantly reduced risk of PND and depressive symptoms in intervention group; women with AN depression: 17.8% risk reduction (without AND: 0.4%); intervention: significantly lower perceived lack of support from partner |
| Lara et al. 2010 (Mexico) [42] | ||
| “Salud Mental de Mamás y Bebés“; CBT-based Aims: preventing PND Length: 16 h (8 × 2 h) Group size: 5–10 Additional: 2 PN individual booster sessions; self-help book on depression (also for control) Facilitator: no information Evaluation/monitoring: participant feedback; sessions filmed and reviewed | 377 women at high risk of depression Characteristics: mean age: 26.9 years; 85.7% partnered; low-middle socio-economic status; 25.5% first child Mean gestational age: 26.9 weeks Baseline symptoms: major depression (SCID) 17.4%, BDI-II ≥ 14 62.7%, anxiety (SCL-90) 14.8% | RCT; control: usual care Screening: CES-D ≥ 16 / self-reported history of depression 7 Allocation: randomisation (block), before or after screening (see “quality assessment“); concealment unclear Outcome measures: depression (SCID), depressive symptoms (BDI-II), anxiety (SCL-90) Time points: baseline; 6 weeks and 4–6 months postnatal Attrition/participation: high attrition, low participation Quality assessment: B (randomisation problematic: for 44% baseline interview took place before randomisation, for others after, resulting in significant differences in depressive symptoms: women who knew which group they had been randomised to reported higher CES-D scores; high attrition rate before start of intervention) Findings: significantly lower cumulative incidence of (new) major depression over all time points for intervention group; no intervention effect on depressive symptoms |
| Le et al. 2011 (US) [60] | ||
| “Mamás y Bebés / Mothers and Babies Course“; cognitive behavioural stress managrement Aims: preventing depression Format: 16 h (8 × 2 h) Group size: no information Additional: 3 individual PN booster sessions Facilitator: researchers Evaluation/monitoring: sessions filmed and selectively reviewed; supervision | 217 low-income women at high risk of depression Characteristics: mean age 25 years; 69.6% (int) / 57.1% (con) partnered; mostly low-income; mostly Central and South American immigrants; 38.4% (int) / 46.7% (con) first child Mean gestational age: ≤24 weeks at baseline Baseline symptoms: BDI-II 15.7 int, 14.9 con, BDI-II ≥ 20 25% int, 24% con | RCT; control: usual care Screening: CES-D ≥ 16 / self-reported personal or family history Allocation: randomization (sealed envelope) after screening; concealed Outcome measures: depressive symptoms (BDI-II), major depressive episodes (MS) Time points: pre-/post-intervention; 6 weeks, 4 and 12 months PN Attrition/participation: high attrition, low participation Quality assessment: C (low participation and high attrition; baseline comparatibility of groups problematic) Findings: significantly fewer depressive symptoms immediately post-intervention (small effect size); fewer cases of moderate depression (BDI-II ≥ 20) post-intervention; stronger size of effects for women who attended more session; no difference postnatally; no difference in cumulative incidence of major depressive episodes |
| Leung & Lam 2012 (China, Hong Kong) [41] | ||
| IPT-based Aims: reducing stress and depressive symptoms, enhancing happiness and self-efficacy in managing conflict Length: 6 h (4 × 90 min) Group size: no information Facilitator: no information Evaluation/monitoring: sessions video taped and reviewed | 156 women Characteristics: mean age 31.2 years; 91.8% partnered; 73.5% first child Mean gestational age: 20 weeks Baseline symptoms: EPDS > 12 41% (int) / 30% (con) | Multisite RCT; control: usual care Screening: none (but subgroup analysis) Allocation: permuted block randomisation (sub-sets of four) after eligibility established; concealed Outcome measures: stress (PSS), depressive symptoms (EPDS), happiness (SHS), self-efficacy in managing conflict (REM), perceived ability to cooperate (single question), perceived health (single question) Time points: pre-/post-intervention; 6–8 weeks postnatal Attrition/participation: low attrition, high participation Quality assessment: A (but intervention very culturally specific, focus on relationship with grandparents) Findings: significantly lower perceived stress (moderate effect size) and smaller decrease in happiness (small/moderate effect size) post-intervention, not sustained postnatally; women with depressive baseline symptoms: lower stress (moderate effect size) and smaller decrease in happiness post-intervention, increased relationship self-efficacy (large effect size); no difference in depressive symptoms |
| Muñoz et al. 2007 (US) [43] | ||
| “Mamás y Bebés / Mothers and Babies Course“; cognitive behavioural stress managrement Aims: preventing depression Length: 24 h (12 × 2 h) Group size: 3–8 Additional: 4 PN booster sessions Facilitator: researchers Evaluation/monitoring: sessions filmed and reviewed, supervision | 41 women at high risk of depression Characteristics: mean age 24.9 years; 71.4% (int) / 80% (con) partnered; mostly low-income; 70% born in Mexico and Central America Mean gestational age: 16.1 (int) / 15.7 (con) weeks Baseline symptoms: CES-D 16.0 (int) / 16.8 (con); history of MDE 47.6% (int) / 60% (con) | RCT; control: usual care Screening: CES-D ≥ 16 / past history of major depressive episode (MMS) Allocation: randomisation after screening; method and concealment unclear Outcome measures: depression (MMS), depressive symptoms (CES-D, EPDS) Time points: pre-/post-intervention; 1, 3, 6 and 12 months postnatal Attrition/participation: low attrition, low participation Quality assessment: B (no information on randomisation, relatively low attendance, no analysis of attenders/non-attenders; postnatal booster sessions may affect outcomes) Findings: no significant differences in depressive symptoms or incidence of MDEs |
| Richter et al. 2012 (Germany) [36] | ||
| See Bittner et al. 2014 [35] | 129 women with elevated stress, anxiety or depression 5 See Bittner et al. 2014 [35] for further details | RCT; control: usual care Screening: PDQ > 14 / STAI > 36 / BDI-S > 20; 10–15 weeks Allocation: random (random allocation sequences); concealed Outcome measures: stress (PDQ, PSS), salivary cortisol Time points: pre-/post-intervention; 3 months postnatal Attrition/participation: high attrition, low participation Quality assessment: A (but high attrition) Findings: intervention: significant change in morning cortisol compared to control post-intervention but not postnatally; no significant difference in perceived stress |
| Urizar & Muñoz 2011 (US) [45] | ||
| See Muñoz et al. 2007 [43] | 86 women at-risk of depression Characteristics: mean age 25.4 years; >72% partnered; mostly low-income; >75% born in Mexico and Central America; mostly second or subsequent child Mean gestational age: 16–17 weeks (range: 6–27 weeks) Baseline symptoms: CES-D 20.6 (int), 23.7 (con1), 9.4 (con2); history of MDE 33.3% (int), 66.% (con1), 0% (con2) | RCT; control 1: usual care, control 2: low risk Screening: CES-D ≥ 16 / past history of major depressive episode (MMS) Allocation: randomization after screening; method and concealment Outcome measures: salivary cortisol levels (mother & infant), perceived stress, depressive symptoms (CES-D), depression (MMS), positive/negative affect (PANAS) Time points: baseline; 6 and 18 months postnatal Attrition/participation: low attrition, low participation Quality assessment: B (postnatal booster sessions may affect outcomes; large variation in gestational age) Findings: intervention and control 2: significantly lower infant cortisol levels at 6 months PN; intervention: lower maternal cortisol levels than control 1 at 18 months PN; significantly higher levels of perceived stress at 6 months PN in intervention group |
| Vieten & Astin 2008 (US) [46] | ||
| “Mindful Motherhood“, based on Mindfulness-Based Stress Reduction Aims: reducing stress and improving mood Length: 16 h (8 × 2 h) Group size: no information Additional: CD with guided meditations Facilitator: clinical psychologist Evaluation/monitoring: no information | 31 women, with “mood concerns“ Characteristics: mean age 33.9 years; 100% partnered; medium-high socio-economic status; 74% white Mean gestational age: 25 weeks Baseline symptoms: perceived stress 20.1 int, 17.1 con; state anxiety 43.8 int, 35.6 con; CES-D 20.4 int, 14.2 con | Pilot RCT; control: wait-list control (postnatal) Screening: positive response to “Have you had a history of mood concerns for which you sought some form of treatment…?“ Allocation: randomisation after screening; concealment not clear Outcome measures: perceived stress (PSS), positive/negative affect (PANAS), depressive symptoms (CES-D), anxiety (STAI), affect regulation (ARM), mindfulness (MAAS) Time points: pre-/post-intervention; 3 months post-intervention Attrition/participation: low attrition, high participation Quality assessment: C (no baseline comparisons between groups but there seem to be differences; no information on attenders / completers; follow-up at different times, postnatally or during pregnancy) Findings: significantly reduced state anxiety and negative affect with large effect sizes post-intervention compared to control, not sustained 3 months post-intervention |
| Zlotnick et al. 2001 (US) [61] | ||
| “Survival Skills for New Moms“; IPT-based Aims: preventing PND Length: 4 h (4 × 1 h) Group size: no information Facilitator: no information Evaluation/monitoring: no information | 37 women on public assistance at risk of PND Characteristics: mean age 23.4 years; 23% partnered; low-income; 45% Caucasian Gestational age range: 20–32 weeks Baseline symptoms: BDI > 10: 70% int, 44% con; history of depression: 70% int, 51% con | Pilot RCT; control: usual care Screening: at least 1 predictor for risk factors for PND 8 Allocation: randomisation after screening; method and concealment unclear Outcome measures: depressive symptoms (BDI), depression (SCID) Time points: pre-/post-intervention; 3 months postnatal Attrition/participation: low attrition, high participation Quality assessment: C (limited details; short intervention; apparent differences at baseline between intervention and control; small sample) Findings: Intervention: women significantly less likely to develop PND |
| Zlotnick et al. 2006 (US) [44] | ||
| “Reach Out, Stand Strong: Essentials for New Moms“ (ROSE) Program; IPT-based Aims: preventing PND Length: 4 h (4 × 1 h) Group size: 3–5 Additional: individual PN booster Facilitator: nurses Evaluation/monitoring: no information | 99 women at risk of PND Characteristics: mean age 22.4 years; 33.3% partnered; low-income; 44% Hispanic Gestational age range: 23–32 weeks Baseline symptoms: previous MDE 31.3%; BDI 15.6 | RCT; control: usual care Screening: CSQ ≥ 27 Allocation: randomisation after screening (stratified for previous episode of depression); concealment unclear Outcome measures: depressive symptoms (BDI), depression (LIFE depression module), social adjustment (RIFT) Time points: pre-intervention; 3 months postnatal Attrition/participation: low attrition, medium participation Quality assessment: B (intervention relatively short, no measurement immediately after the intervention; no detailed description of the intervention) Findings: 3 months PN: fewer women in intervention with PND than in control (4% vs. 20%); no significant difference between groups for depression severity (BDI) or social adjustment at 3 months PN |
| Qualitative Studies | ||
| Goodman et al. 2014 (US) [58] | ||
| Coping with anxiety through Living Mindfully (CALM) Pregnancy; mindfulness-based cognitive therapy adapted for pregnant women with anxiety Aims: coping with anxiety Format: 16 h (8 × 2 h) Group size: 6–12 Additional: MP3s of meditations for home practice Facilitator: clinical social worker Evaluation/monitoring: audiotaped and reviewed for fidelity and supervision | 24 women with elevated anxiety symptoms and no greater than moderate levels of depression Characteristics: mean age 33.5 years; 96% partnered; 75% white/non-Hispanic; 66.6% first child Mean gestational age: 15.5; range: 6–27 weeks Baseline symptoms: 70.8% met criteria for GAD | Qualitative content analysis Screening: PSWQ ≥ 45 / GAD-7 ≥ 10 / BAI ≥ 11 / PHQ-9 < 15 Data collection: written response to open-ended questions Attrition/participation: low attrition, high participation Quality assessment: B (insufficient details of how study was explained to participants, insufficient details of data analysis; limited discussion regarding credibility of findings and value of research) Findings: seven categories: skill building; connection; universality; acceptance and self-kindness; decreased reactivity; cognitive changes; insight |
| Le et al. 2013 (US) [61] | ||
| “Mamás y Bebés / Mothers and Babies Course“; cognitive behavioural stress managrement Aims: preventing depression Format: 16 h (8 × 2 h) Group size: no information Additional: 3 individual PN booster sessions Facilitator: researchers Evaluation/monitoring: sessions filmed and selectively viewed | 39 women (participants in Le et al. 2011 [60]) Characteristics: mean age 27.8 years; 61.5% partnered; mostly Central and South American immigrants Mean gestational age: no information Baseline symptoms: CES-D ≥ 16 23.1%; personal history of depression 69.4% | Inductive comparative analysis Screening: CES-D ≥ 16 / past history of major depressive episode (MMS) Data collection: semi-structured interviews Attrition/participation: low attrition, low participation Quality assessment: B (lacking in detail about recruitment strategy, data collection, relationship between researcher and participants, data analysis) Findings: Women valued participating in the course; support network; awareness of mood; increased maternal efficacy; reduced isolation; child development; group experience; using tool |
| Wheatley & Brugha 1999 (UK) [37] | ||
| See Brugha et al. 2000 [39]; CBT-based | 9 women (subsample of Brugha et al. 2000 [39]) Characteristics: mean age 25.6 years; 68.7% white; 100% first child Gestational age: >28 weeks Baseline symptoms: unable to determine | Grounded theory Screening: “Pregnancy and You“ screening questionnaire 5; 12–20 weeks Data collection: interviews Attrition/participation: low attrition, low participation Quality assessment: B (some detail lacking in how the study was explained to participants and data analysis; limited discussion regarding credibility of findings and value of research) Findings: themes: postnatal depression (lack of knowledge as protective or vulnerable); positive experience |
| Wheatley et al. 2003 (UK) [38] | ||
| See Brugha et al. 2000 [39]; CBT-based | See Wheatley & Brugha 1999 [37] | Grounded theory (focus on engagement with intervention) See Wheatley & Brugha 1999 [37] Quality assessment: B (no clear statement of the aim; lack of detail about aspects relating to the appropriateness of the recruitment strategy, data collection, consideration of the researcher/participant relationship, the ethical issues and data analysis) Findings: Themes: initial engagement (need for information about PND, PND taboo, decision-making, practicalities); maintaining engagement (sharing experiences, normalising, sensitivity of PND, positive experience, practicalities) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wadephul, F.; Jones, C.; Jomeen, J. The Impact of Antenatal Psychological Group Interventions on Psychological Well-Being: A Systematic Review of the Qualitative and Quantitative Evidence. Healthcare 2016, 4, 32. https://doi.org/10.3390/healthcare4020032
Wadephul F, Jones C, Jomeen J. The Impact of Antenatal Psychological Group Interventions on Psychological Well-Being: A Systematic Review of the Qualitative and Quantitative Evidence. Healthcare. 2016; 4(2):32. https://doi.org/10.3390/healthcare4020032
Chicago/Turabian StyleWadephul, Franziska, Catriona Jones, and Julie Jomeen. 2016. "The Impact of Antenatal Psychological Group Interventions on Psychological Well-Being: A Systematic Review of the Qualitative and Quantitative Evidence" Healthcare 4, no. 2: 32. https://doi.org/10.3390/healthcare4020032