
Creating the Evidence through Comparative Effectiveness Research for Interprofessional Education and Collaborative Practice by Deploying a National Intervention Network and a National Data Repository

Abstract
:1. Background
- Interprofessional education “occurs when two or more professions learn about, from, and with each other to enable effective collaboration and (to) improve health outcomes.” [6].
- Interprofessional Collaborative Practice “…happens when multiple health-related workers from different professional backgrounds work together with patients, families, care givers and communities to deliver the highest quality of care.” [7].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Change Level | Clinical | Education | Nexus |
|---|---|---|---|
| Micro | Provides care of patients and operates within its own environment and ecology; participants are committed to working together | Teaching environment to education learners | Intentionally create relationship at the practice and education microsystem level to achieve the Triple Aim |
| Meso | Senior leadership and governing structures in clinical systems; corporate offices, governing boards | University/college presidents, provosts, deans and senior administration; governing boards and trustees, regents | Greater understanding of synergies between health system transformation and meeting higher education needs; support IPECP implementation at micro level |
| Macro | Political, financial, accreditation and policy environment; state, regional and/or national level; increasingly complex | Political, financial, accreditation and policy environment; state, regional and/or national level; increasingly complex | Political, financial, accreditation and policy environment; state, regional and/or national level; increasingly complex |
2. Methods: The Research Strategies of the National Center
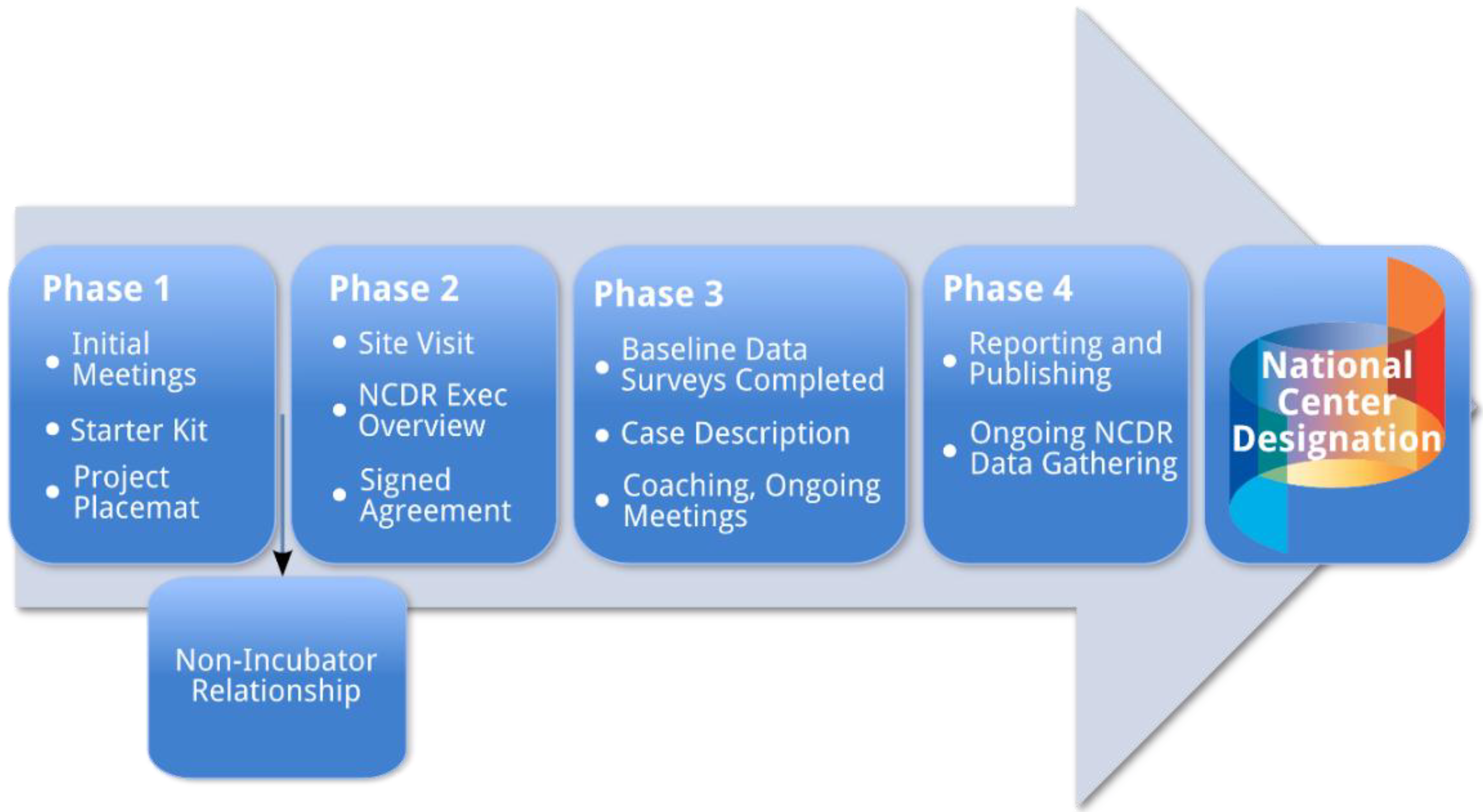
2.1. The Incubator Strategy
| Project Intervention Type | Team Composition | Outcomes Measured |
|---|---|---|
Transitions of Care:
| Staff: physicians, nurse practitioners, pharmacists, physician assistants, dentists, social workers, physical therapists, occupational therapists, speech therapists, nutritionists, behavioral health, patients and family members | Clinical: error reduction, reduced upstream hospital readmission, reduced resource use, improved patient satisfaction with care, improved staff satisfaction with care provision, cost reductions |
| Students: medical, advanced practice nursing, pharmacy, behavioral health, allied health, social work | Educational: changes in knowledge and skills, IPECP * team competencies, meaningful participation in care process | |
Disease Related:
| Staff: physicians, nurse practitioners, pharmacists, behavior health, dentistry, social work, patient family, administrators | Clinical: improved disease markers, reduced cost of care, reduced resource use, reduced disease complications, improved clinic efficiency, improved team function |
| Students: medical, advanced practice nursing, pharmacy, behavioral health, dentistry, social work, physician assistants | Educational: IPECP * skills, assessment of readiness to practice | |
Primary Care:
| Staff: physicians, nurse practitioners, pharmacists, behavior health, medical assistants, social work, clinic coordinators, clinic administrators, patients and family members, academic faculty, community partners | Clinical: improved patient satisfaction with care, improved staff satisfaction with care provision, improved process of efficiency, improved care coordination, reduced cost of care, reduced emergency department use, reduced use of inpatient services |
| Students: medical, pharmacy, behavior health, social work, medical technicians, dental | Education: assessing team care in a learning environment, complex health care experience, assessment of team competencies and readiness for practice | |
Education Institution Process Improvement:
| Staff: physicians, nurse practitioners, pharmacy, dentistry | Clinical: TeamSTEPPS as a team training tool for hospital staff, additional knowledge and skills needed in curriculum, more effective collaborative care, improved patient satisfaction with care, improved staff satisfaction with care provision |
| Students: medical, advanced practice nursing, pharmacy, physical therapy, occupational therapy | Education: TeamSTEPPS as a team training tool for students, assessing meaningful roles for students in team care, assessment tool validation, improved IPECP * learning environment, improved role modeling, behavior change, knowledge and skill acquisition | |
Expanding Roles of Advanced Practice Providers (APN, PA):
| Staff: nurse practitioners, physician assistants, allied health, care coordinators, patients and family members, physicians as needed | Clinical: team performance, patient/provider satisfaction, care quality, cost and resource use reductions, comparative assessment of model performance |
| Students: advanced practice nursing, physician assistant, social work, physical therapy, occupational therapy, dentistry | Education: Assessing value added and meaningful use of students on clinical care provision teams, identification of additional skills and knowledge needed, assessment of team transfer skills |
- A collaborative team approach to care could reduce healthcare cost.
- Collaborative training could result in better healthcare quality by developing interdependencies, mutual respect and understanding for scope of work among health professionals.
- Health professionals trained in understanding population health could enhance primary prevention ultimately leading to reduced prevalence of (at the very least) modifiable risk factors that may result in chronic disease. This can happen at the point of care one person at a time, a disease-based population intervention, or a population health status intervention.
- A collaborative team approach to care could facilitate cost effectiveness with appropriate level providers working at the top of their licenses to provide care at the appropriate level of prevention (primary, secondary, or tertiary).
- Integrating community members (patients and families) into healthcare delivery planning could enhance engagement in personal health, leading to reduced chronic disease and improved population health.
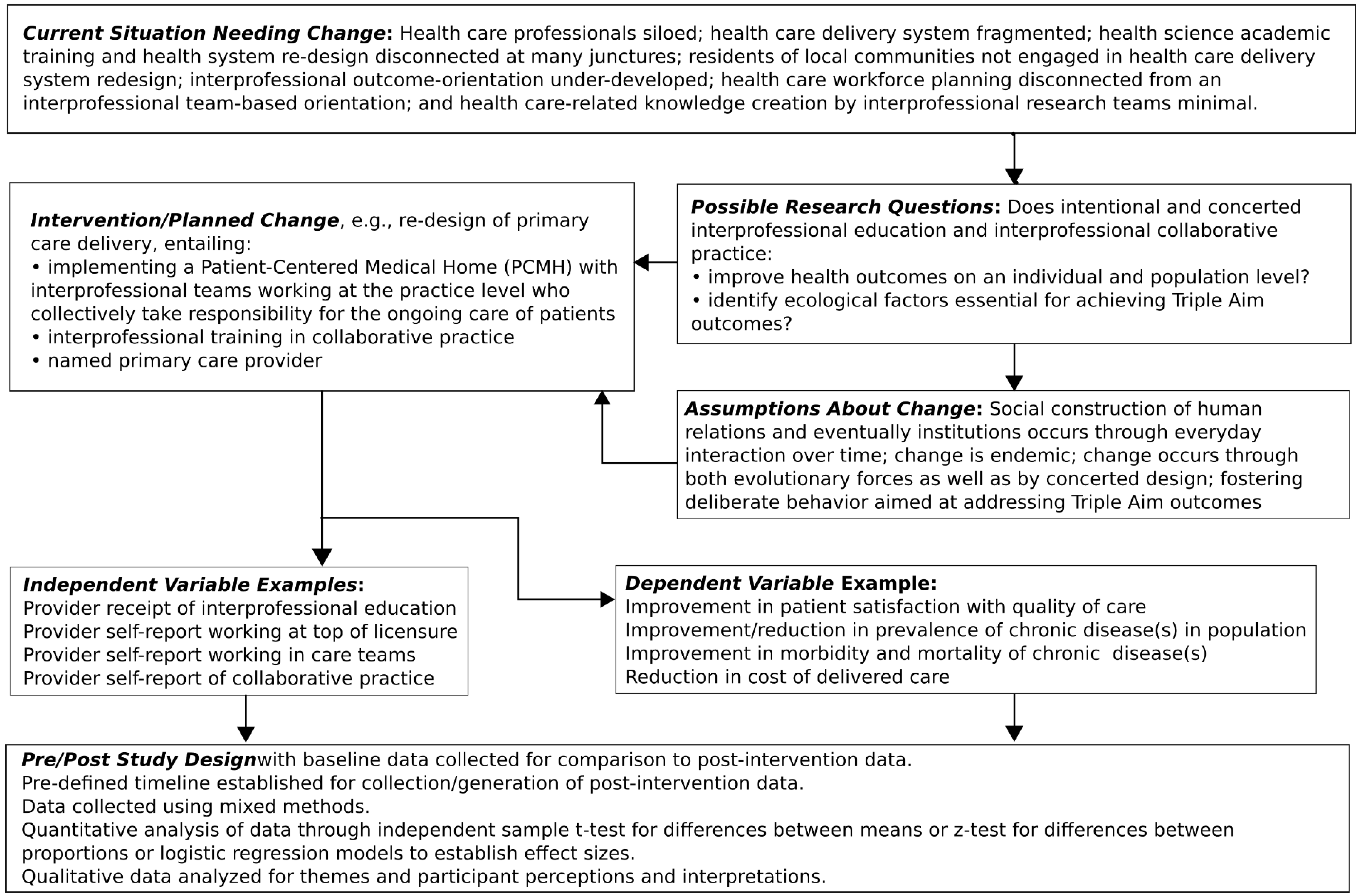

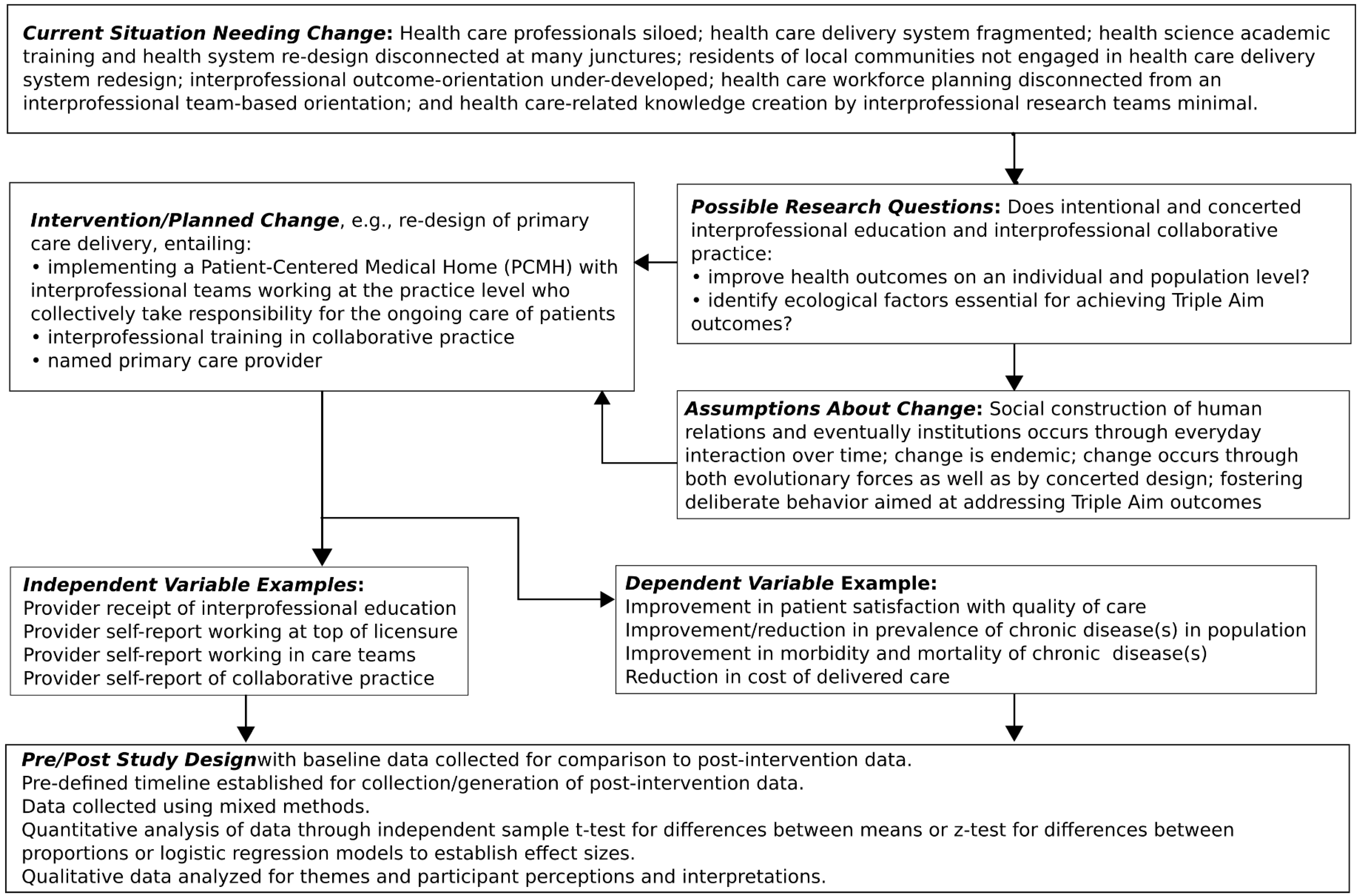
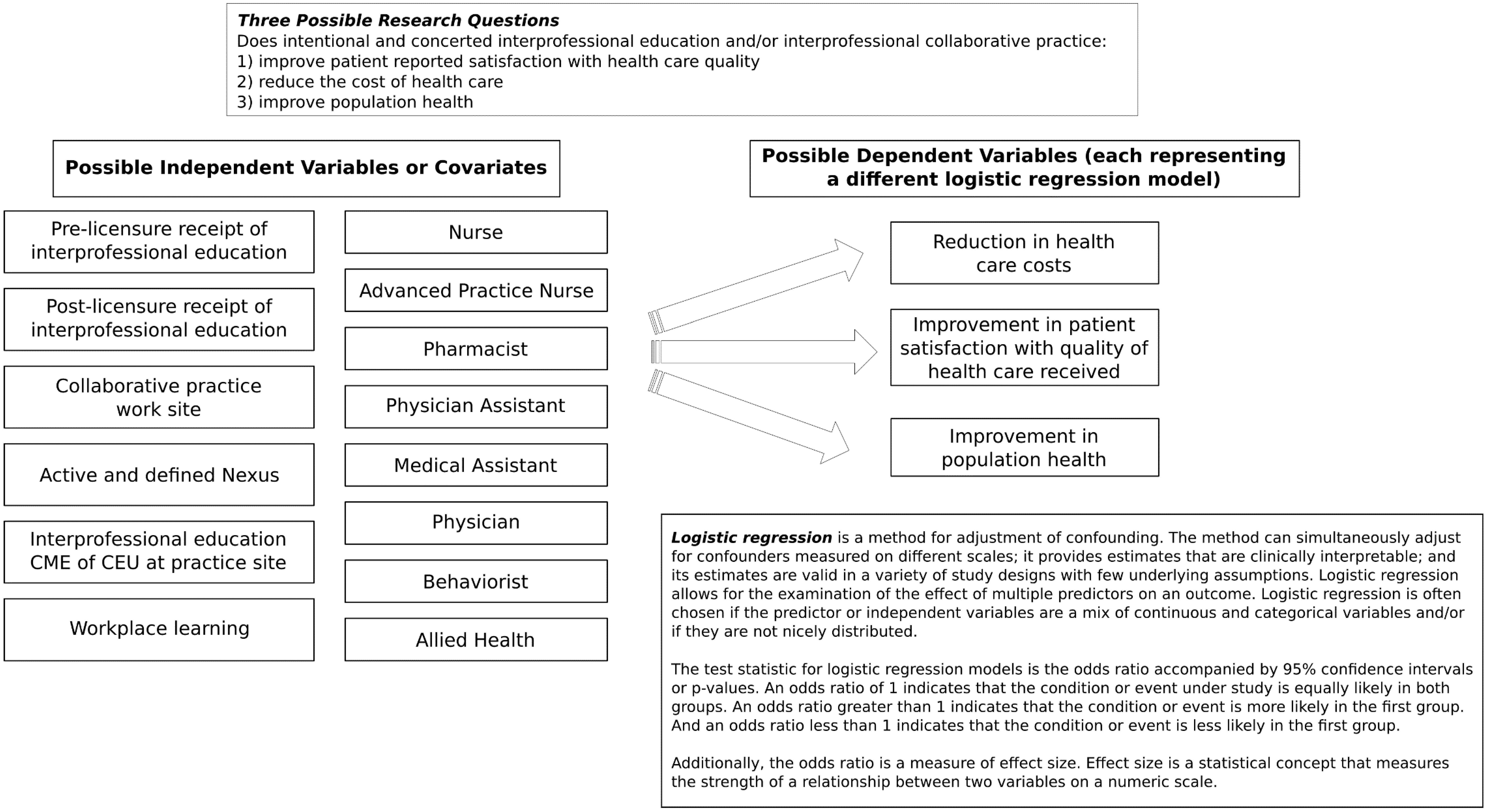
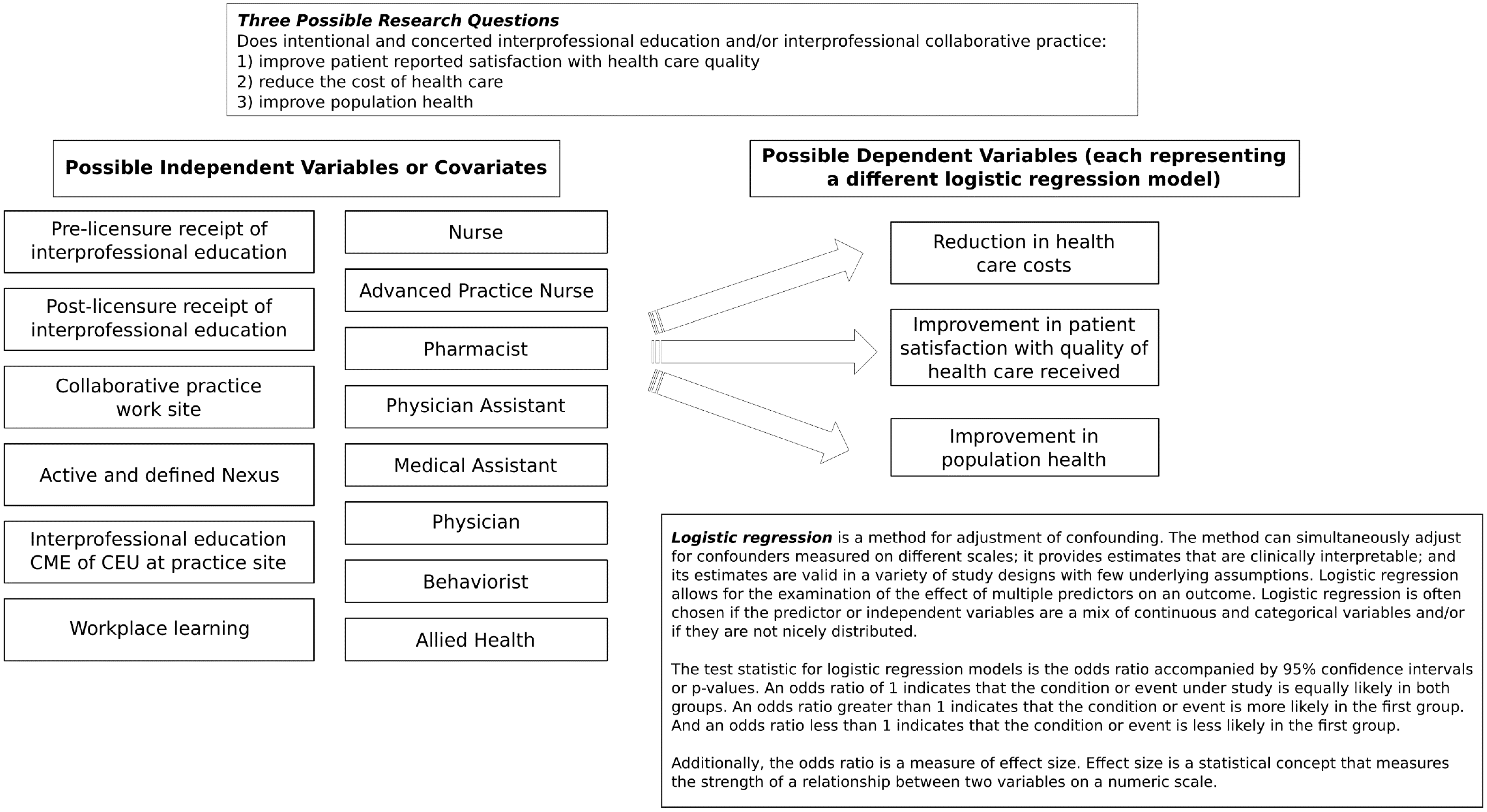
2.2. The CER Strategy
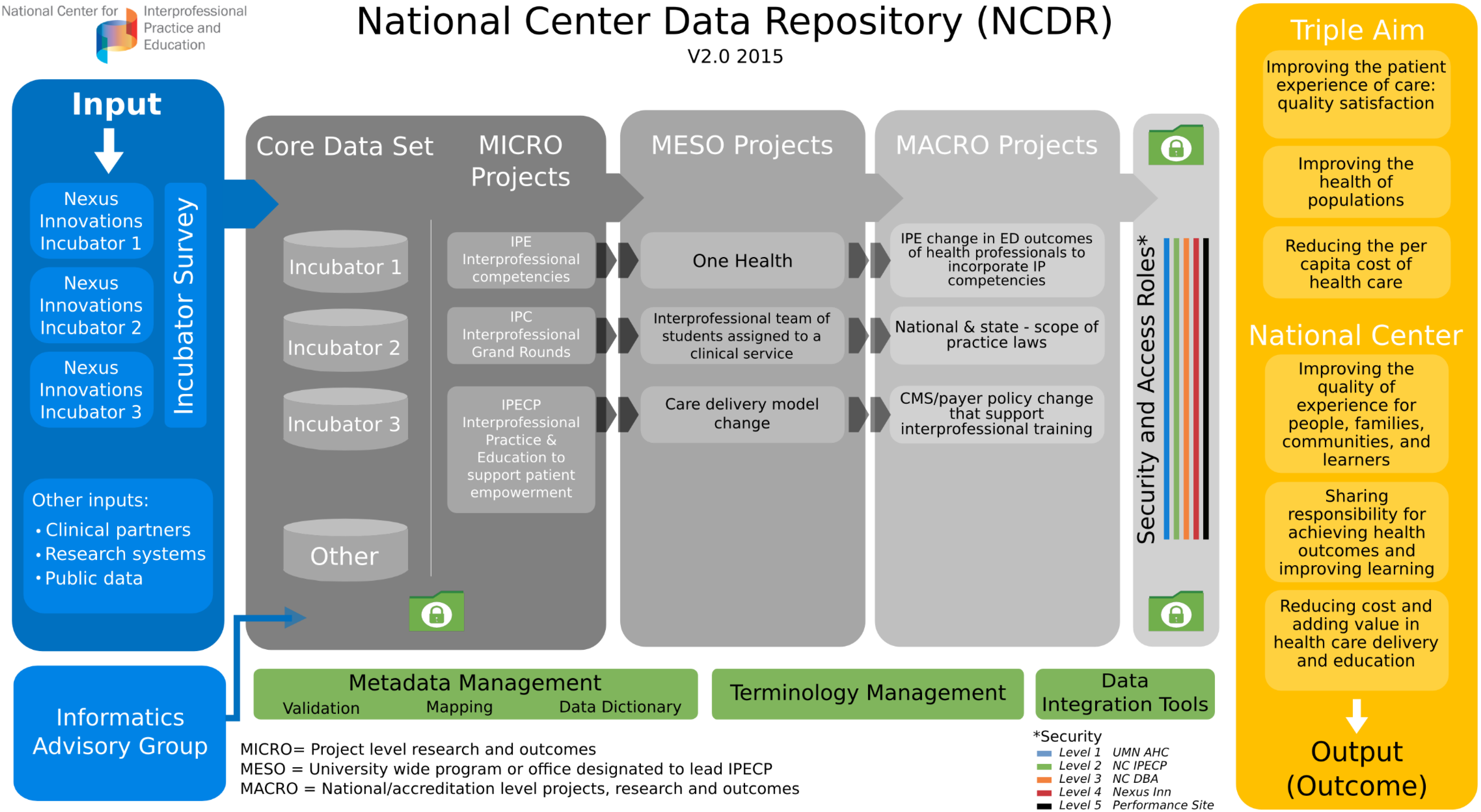
2.3. The National Center Data Repository (NCDR) Strategy
3. Projected Results: The Deliverables of the Nexus Incubator Network and the NCDR

- Improve the Health Outcomes (Triple Aim) on an individual and population level?
- Result in improvement in educational outcomes?
- Identify ecological and/or environmental factors essential for or barriers to achieving Triple Aim health outcomes?
- Identify factors essential for or barriers to sustaining the transformation of the process of care?
- Identify changes needed in policy, accreditation, credentialing and licensing?
4. Discussion
5. Conclusions
Acknowledgements
Author Contributions
Conflicts of Interest
References
- National Center for Interprofessional Practice and Education. Available online: http://nexusipe.org/about (accessed on 3 December 2014).
- Cerra, F.; Brandt, B. Renewed focus in the United States links interprofessional education with redesigning healthcare. J. Interprof. Care 2011, 25, 394–396. [Google Scholar] [CrossRef] [PubMed]
- The Patient Protection and Affordable Care Act Detailed Summary. Available online: http://www.dpc.senate.gov/healthreformbill/healthbill04.pdf (accessed on 8 September 2014).
- Berwick, D.M.; Nolan, T.W.; Whittington, J. The triple aim: Care, health, and cost. Health Aff. 2008, 27, 759–769. [Google Scholar] [CrossRef]
- Chen, F.M.; Williams, S.D.; Gardner, D.B. The case for a National Center for Interprofessional Practice and Education. J. Interprof. Care 2013, 27, 356–357. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Department of Human Resources for Health. Framework for action on interprofessional education and collaborative practice; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Barr, H.; Waterton, S. Interprofessional Education in Health and Social Care in the United Kingdom: Report of a CAIPE Survey; Centre for the Advancement of Interprofessional Education in Primary Health and Community Care: London, UK, 1996. [Google Scholar]
- Zwarenstein, M.; Goldman, J.; Reeves, S. Interprofessional collaboration: Effects of practice-based interventions on professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2009. [Google Scholar] [CrossRef]
- Reeves, S.; Zwarenstein, M.; Goldman, J.; Barr, H.; Freeth, D.; Hammick, M.; Koppel, I. Interprofessional education: Effects on professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2008. [Google Scholar] [CrossRef]
- Reeves, S.; Perrier, L.; Goldman, J.; Freeth, D.; Zwarenstein, M. Interprofessional education: Effects on professional practice and healthcare outcomes (update). Cochrane Database Syst. Rev. 2013, 3. [Google Scholar] [CrossRef]
- Brandt, B.F.; Lutfiyya, M.N.; King, J.A.; Chioreso, C. A scoping review of interprofessional collaborative practice and education using the lens of the Triple Aim. J. Interprof. Care 2014, 28, 393–399. [Google Scholar] [CrossRef] [PubMed]
- D’Amour, D.; Oandasan, I. Interprofessionality as the field of interprofessional practice and interprofessional education: An emerging concept. J. Interprof. Care 2005, Supplement 1, 8–20. [Google Scholar] [CrossRef]
- Hall, P.; Weaver, L. Interdisciplinary education and teamwork: A long and winding road. Med. Educ. 2001, 35, 867–875. [Google Scholar] [CrossRef] [PubMed]
- Frenk, J.; Chen, L.; Bhutta, Z.; Cohen, J.; Crisp, N.; Evans, T.; Fineberg, H.V.; Garcia, P.; Ke, Y.; Kelley, P.; et al. Health professionals for a new century: Transforming education to strengthen health systems in an interdependent world. Lancet 2010, 376, 1923–1958. [Google Scholar] [CrossRef]
- Fraser, M.W.; Galinsky, M.J. Steps in intervention research: Designing and developing social programs. Res. Soc. Work Pract. 2010, 20, 459–466. [Google Scholar] [CrossRef]
- Moore, L.; Moore, G. Public health evaluation: Which designs work, for whom and under what circumstances? J. Epidemiol. Community Health 2011, 65, 596–597. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337. [Google Scholar] [CrossRef]
- Safford, M.M. Comparative effectiveness research and outcomes of diabetes treatment. JAMA 2014, 311, 2275–2276. [Google Scholar] [CrossRef] [PubMed]
- Dreyer, N.A.; Tunis, S.R.; Berger, M.; Ollendorf, D.; Mattox, P.; Gliklich, R. Why observational studies should be among the tools used in comparative effectiveness research. Health Aff. 2010, 29, 1818–1825. [Google Scholar] [CrossRef]
- Sox, H.C. Defining comparative effectiveness research: The importance of getting it right. Med. Care 2010, 48, S7–S8. [Google Scholar] [CrossRef] [PubMed]
- Bravman, P.A. Monitoring equity in health and healthcare: A conceptual framework. J. Health Popul. Nutr. 2003, 21, 181–192. [Google Scholar] [PubMed]
- Braveman, P.A.; Egerter, S.A.; Woolf, S.H.; Marks, J.S. When do we know enough to recommend action on the social determinants of health? Am. J. Prev. Med. 2011, 40, S58–S66. [Google Scholar] [CrossRef] [PubMed]
- Peek, C.J.; Glasgow, R.E.; Stange, K.C.; Klesges, L.M.; Purcell, E.P.; Kessler, R.S. The 5 R’s: An emerging bold standard for conducting relevant research in a changing world. Ann. Fam. Med. 2014, 12, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Ewigman, B. Could 5R research help achieve the Triple Aim? Ann. Fam. Med. 2014, 12, 399–401. [Google Scholar] [CrossRef] [PubMed]
- Peek, C.J.; Cohen, D.J.; de Gruy, F.V. Research and evaluation in the transformation of primary care. Am. Psychol. 2014, 69, 430–442. [Google Scholar] [CrossRef] [PubMed]
- Phelan, J.C.; Link, B.G.; Tehranifar, P. Social conditions as fundamental causes of health inequities: Theory, evidence, and policy implications. J. Health Soc. Behav. 2010, 51, S28–S40. [Google Scholar] [CrossRef] [PubMed]
- University of Minnesota Academic Health Center Information Exchange. AHCIE Program Update. Available online: http://www.ahc.umn.edu/prod/groups/ahc/@pub/@ahc/documents/content/ahc_content_262677.pdf (accessed on 3 December 2014).
- Nason, E. Return on Investment and a Research Agenda for Interprofessional Education and Collaborative Practice: Overview Document; Institute on Government: Ottawa, Canada, 2012.
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pechacek, J.; Cerra, F.; Brandt, B.; Lutfiyya, M.N.; Delaney, C. Creating the Evidence through Comparative Effectiveness Research for Interprofessional Education and Collaborative Practice by Deploying a National Intervention Network and a National Data Repository. Healthcare 2015, 3, 146-161. https://doi.org/10.3390/healthcare3010146
Pechacek J, Cerra F, Brandt B, Lutfiyya MN, Delaney C. Creating the Evidence through Comparative Effectiveness Research for Interprofessional Education and Collaborative Practice by Deploying a National Intervention Network and a National Data Repository. Healthcare. 2015; 3(1):146-161. https://doi.org/10.3390/healthcare3010146
Chicago/Turabian StylePechacek, Judith, Frank Cerra, Barbara Brandt, May Nawal Lutfiyya, and Connie Delaney. 2015. "Creating the Evidence through Comparative Effectiveness Research for Interprofessional Education and Collaborative Practice by Deploying a National Intervention Network and a National Data Repository" Healthcare 3, no. 1: 146-161. https://doi.org/10.3390/healthcare3010146