
A Robust Automated Cataract Detection Algorithm Using Diagnostic Opinion Based Parameter Thresholding for Telemedicine Application


Abstract
:1. Introduction
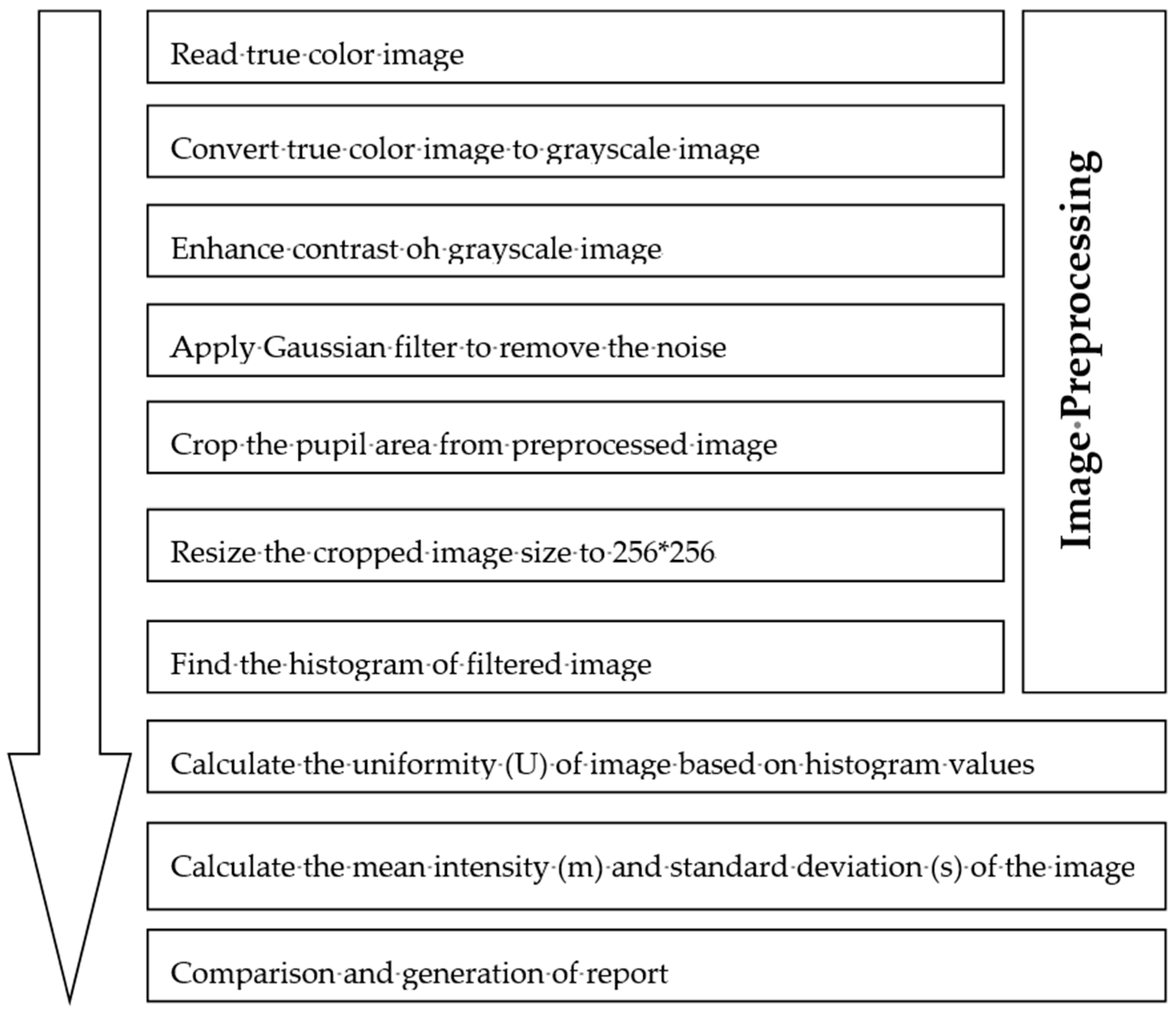
2. Robust and Efficient Automated Cataract Detection Algorithm
3. Experimental Outcomes and Diagnostic Validation
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Cost of Vision Problems. Available online: http://costofvision.preventblindness.org/home/introduction (accessed on 20 April 2016).
- Visual Impairment and Blindness. Available online: http://www.who.int/mediacentre/factsheets/fs282/en/ (accessed on 20 April 2016).
- Gary, B.; Taylor, H. Cataract Blindness–Challenges for 21st century. Bull. World Health Organ. 2001. Available online: http://www.who.int/bulletin/archives/79(3)249.pdf (accessed on 30 April 2016). [Google Scholar]
- Comas, O.; Cotin, S.; Duriez, C. A shell model for real time simulation of intra-ocular implant deployment. In Proceedings of the International Symposium on Biomedical Simulation, Phoenix, AZ, USA, 23–24 January 2010; pp. 160–170.
- Supriyanti, R.; Habe, H.; Kidode, M.; Nagata, S. A simple and robust method to screen cataract using specular reflection appearance. In Proceedings of the Medical Imaging International Conference of International Society for Optics and Photonics (SPIE), San Diego, CA, USA, 17 March 2008. [CrossRef]
- Supriyanti, R.; Habe, H.; Kidode, M.; Nagata, S. Cataract Screening by Specular Reflection and Texture Analysis. In Proceedings of the Systemics and Informatics World Network (SIWN 2009), Leipzig, Germany, 23–25 March 2009.
- Supriyanti, R.; Habe, H.; Kidode, M.; Nagata, S. Compact cataract screening system: Design and practical data acquisition. In Proceedings of the International Conference on Instrumentation, Communication, Information Technology and Biomedical Engineering (ICICI-BME), Bandung, Indonesia, 23–25 November 2009. [CrossRef]
- Shen, H.; Hao, H.; Wei, L.; Wang, Z. An image based classification method for cataract. In Proceedings of the International Symposium on Computer Science and Computational Technology, Shanghai, China, 20–22 December 2008. [CrossRef]
- Yang, M.; Yang, J.-J.; Zhang, Q.; Niu, Y.; Li, J. Classification of retinal image for automatic cataract detection. In Proceedings of the e-Health Networking, Applications & Services (Healthcom), Lisbon, Portugal, 9–12 October 2013. [CrossRef]
- Nayak, J. Automated classification of normal, cataract and post cataract optical eye images using SVM classifier. In Proceedings of the World Congress on Engineering and Computer Science, San Francisco, CA, USA, 23–25 October 2013; pp. 542–545.
- Li, H.; Lim, J.H.; Liu, J.; Mitchell, P.; Tan, A.G.; Wang, J.J.; Wong, T.Y. A Computer-Aided Diagnosis System of Nuclear Cataract. IEEE Trans. Biomed. Eng. 2010, 57, 1690–1698. [Google Scholar] [PubMed]
- Caixinha, M.; Velte, E.; Santos, M.; Santos, J.B. New approach for objective cataract classification based on ultrasound techniques using multiclass svm classifiers. In Proceedings of the IEEE International Ultrasonics Symposium (IUS), Chicago, IL, USA, 3–6 September 2014. [CrossRef]
- Caxinha, M.; Velte, E.; Santos, M.; Perdigão, F.; Amaro, J.; Gomes, M.; Santos, J. Automatic cataract classification based on ultrasound technique using machine learning: A comparative study. Phys. Procedia 2015, 70, 1221–1224. [Google Scholar] [CrossRef]
- Srivastava, R.; Gao, X.; Yin, F.; Wong, D.W.; Liu, J.; Cheung, C.Y.; Wong, T.Y. Automatic nuclear cataract grading using image gradients. J. Med. Imaging 2014, 1, 014502. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.-J.; Li, J.; Shen, R.; Zeng, Y.; He, J.; Bi, J.; Li, Y.; Zhang, Q.; Peng, L.; Wang, Q. Exploiting ensemble learning for automatic cataract detection and grading. Comput. Methods Progr. Biomed. 2016, 124, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Rashmi; Kumar, M.; Saxena, R. Algorithm and Technique on Various Edge Detection: A Survey. Signal Image Process. 2013, 4, 65. [Google Scholar] [CrossRef]
- Deng, G.; Cahill, L.W. An adaptive Gaussian filter for noise reduction and edge detection. In Proceedings of the 1993 IEEE Conference Record, Nuclear Science Symposium and Medical Imaging Conference, San Francisco, CA, USA, 31 October–6 November 1993. [CrossRef]
- Sepasian, M.; Balachandran, W.; Mares, C. Image enhancement for fingerprint minutiae based algorithm using CLAHE, standard deviation analysis and sliding neighbourhood. In Proceedings of the World congress on Engineering and Computer Science (WCECS 2008), San Francisco, CA, USA, 22–24 October 2008.
- Kanungo, T.; Mount, D.M.; Netanyahu, N.S.; Piatko, C.D.; Silverman, R.; Wu, A.Y. An efficient k-means clustering algorithm: Analysis and implementation. In Proceedings of the Sixteenth ACM Symposoium on Computational Geometry, Hong Kong, China, 12–14 June 2000; pp. 100–109.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Texture Information | Doctor’s Opinion | ||
|---|---|---|---|
| Healthy | Mild | Severe | |
| Mean Intensity (I) | 12.93 < I < 125.31 | 125.31 < I < 134 | I > 134 |
| Uniformity (U) | U > 0.17 | 0.0927 < U < 0.11 | U < 0.09 |
| Standard Deviation(s) | s < 1.59 | 2.64< s < 3.18 | s > 3.18 |
| Image No. | Calculated Texture Information | Doctor’s Opinion | System’s Output (Y/N) | ||
|---|---|---|---|---|---|
| m | U | s | |||
| 1. | 12.41 | 0.13 | 1.17 | Healthy | N |
| 2. | 18.78 | 0.15 | 1.41 | Healthy | N |
| 3. | 13.85 | 0.15 | 1.69 | Healthy | N |
| 4. | 144.59 | 0.10 | 3.27 | Severe | Y |
| 5. | 122.19 | 0.11 | 2.32 | Mild | Y |
| 6. | 114.66 | 0.10 | 2.41 | Mild | Y |
| 7. | 136.41 | 0.09 | 2.92 | Severe | Y |
| 8. | 11.69 | 0.18 | 1.80 | Healthy | N |
| 9. | 8.75 | 0.15 | 1.16 | Healthy | N |
| 10. | 172.12 | 0.14 | 3.76 | Severe | Y |
| 11. | 153.48 | 0.10 | 3.49 | Severe | Y |
| 12. | 132.52 | 0.09 | 3.18 | Severe | Y |
| 13. | 152.38 | 0.13 | 2.70 | Mild | Y |
| 14. | 132.11 | 0.08 | 2.32 | Mild | Y |
| 15. | 137.17 | 0.10 | 3.73 | Severe | Y |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pathak, S.; Kumar, B. A Robust Automated Cataract Detection Algorithm Using Diagnostic Opinion Based Parameter Thresholding for Telemedicine Application. Electronics 2016, 5, 57. https://doi.org/10.3390/electronics5030057
Pathak S, Kumar B. A Robust Automated Cataract Detection Algorithm Using Diagnostic Opinion Based Parameter Thresholding for Telemedicine Application. Electronics. 2016; 5(3):57. https://doi.org/10.3390/electronics5030057
Chicago/Turabian StylePathak, Shashwat, and Basant Kumar. 2016. "A Robust Automated Cataract Detection Algorithm Using Diagnostic Opinion Based Parameter Thresholding for Telemedicine Application" Electronics 5, no. 3: 57. https://doi.org/10.3390/electronics5030057