3.1. Mapping Scaphoid Bone Morphology and Vascular Supply
Radiologic images and 3D representations (
Figure 1) of the adult human hand (
Figure 1A,B) and mini-pig forelimb (
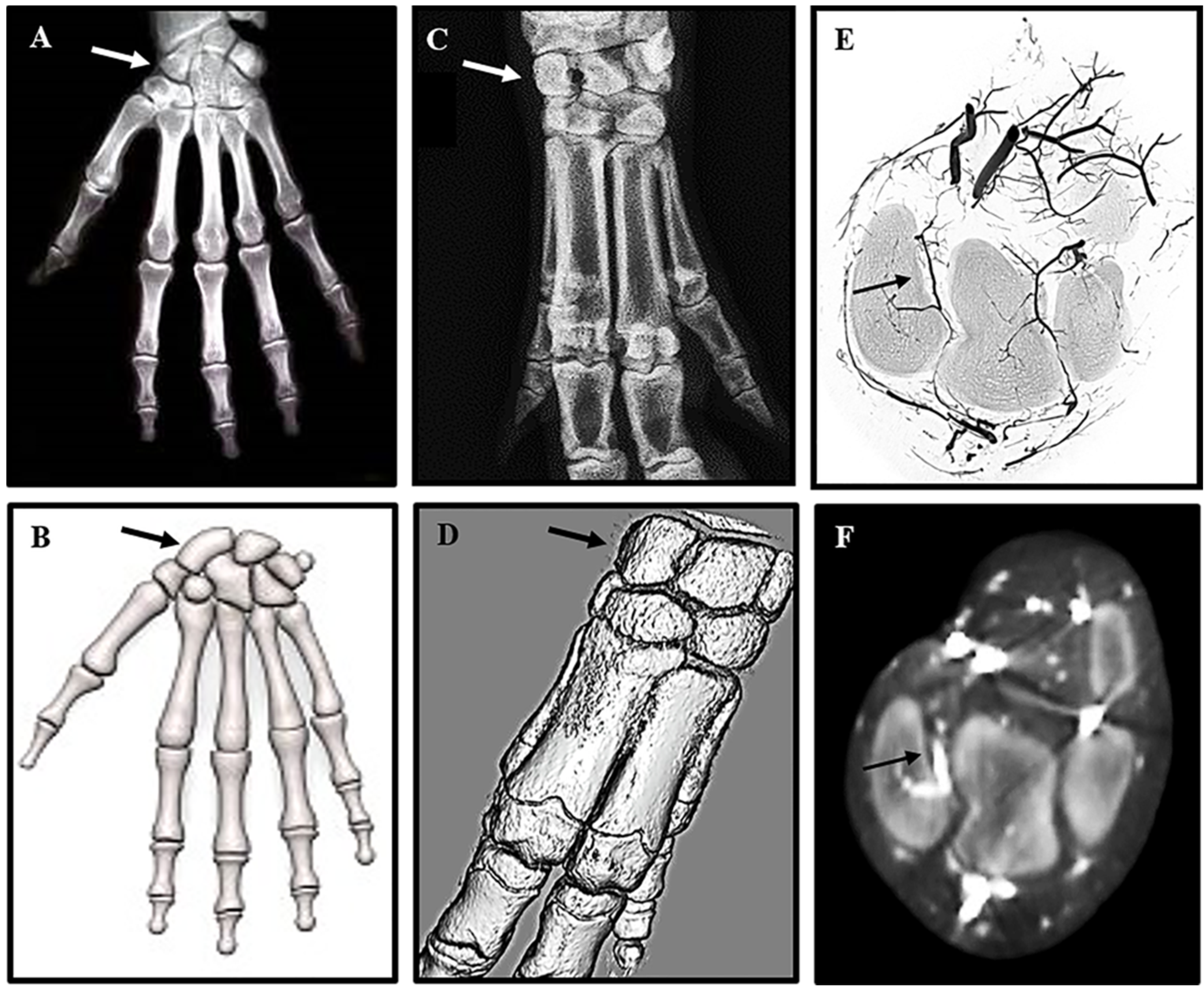
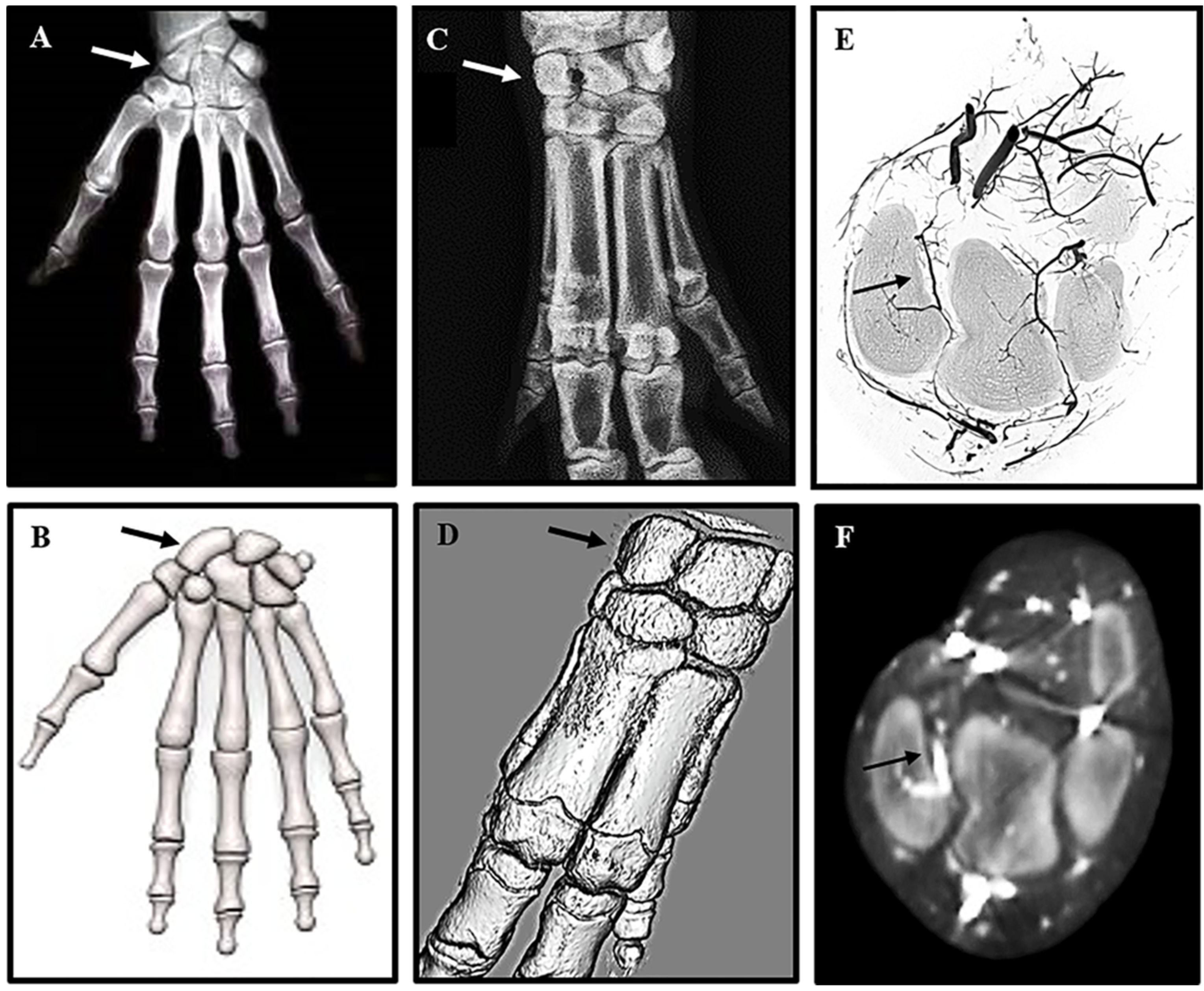
Figure 1C,D) reveal a remarkable similarity in anatomy, particularly of the complex structure of the carpal bones in the wrist. The human scaphoid corresponds to the mini-pig radiocarpal bone (arrows
Figure 1A–D), which is located between the radius and the metacarpal bones. BaSO
4 contrast agent injected into the axillary artery to visualize the vascular feed to the radiocarpal (
Figure 1E,F) confirmed the same organization of retrograde blood supply as seen in the human scaphoid. Reconstruction of high resolution micro CT images (
Figure 1E) confirmed the position of the supply artery, originating from the large vessels on the volar side of the wrist and entering the dorsal aspect of the radiocarpal bone. The intraosseous vessel then runs from dorsal to volar analogous to the retrograde flow of the radial artery blood supply in the human scaphoid, leaving the volar pole vulnerable to avascular necrosis. The course of the blood vessels was confirmed on transaxial CT images captured with the Fidex Animage CT scanner (
Figure 1F). The radiocarpal bone was, thus, shown to resemble the human scaphoid bone and the mini-pig identified as an appropriate pre-clinical model to replicate fracture non-union of the human scaphoid to develop improved therapeutic interventions for repair.
Figure 1.
High resolution radiographs comparing human scaphoid and mini-pig radiocarpal bone: The position of the scaphoid bone in the human wrist (A,B), and the corresponding radiocarpal bone in a porcine forelimb (C,D) are marked by arrows in 2D X-rays (A,C) and 3D models (B,D). For contrast radiography pigs were euthanized, and the forelimbs perfused immediately with BaSO4 via the axillary artery. The carpal bones were scanned at high resolution on a Skyscan 1172 ex vivo instrument (E) and on a Fidex Animage in vivo instrument (F). The position and size of the pig radiocarpal bone closely resemble those of the human scaphoid bone, but differ in orientation of the longitudinal axis. As with the human scaphoid, the pig radiocarpal bone has a limited blood supply to the volar pole indicated by arrows on the 3D reconstructions (E,F).
Figure 1.
High resolution radiographs comparing human scaphoid and mini-pig radiocarpal bone: The position of the scaphoid bone in the human wrist (A,B), and the corresponding radiocarpal bone in a porcine forelimb (C,D) are marked by arrows in 2D X-rays (A,C) and 3D models (B,D). For contrast radiography pigs were euthanized, and the forelimbs perfused immediately with BaSO4 via the axillary artery. The carpal bones were scanned at high resolution on a Skyscan 1172 ex vivo instrument (E) and on a Fidex Animage in vivo instrument (F). The position and size of the pig radiocarpal bone closely resemble those of the human scaphoid bone, but differ in orientation of the longitudinal axis. As with the human scaphoid, the pig radiocarpal bone has a limited blood supply to the volar pole indicated by arrows on the 3D reconstructions (E,F).
3.2. Surgical Outcomes and Bone Repair
High resolution X-rays taken pre-operatively were used to confirm the dimensions of each radiocarpal bone prior to surgical intervention, and post-operative to ensure adequate fixation of the defect (
Figure 2).
Figure 2.
Surgical intervention to generate radiocarpal non-union: X-rays of the forearms of anesthetized mini-pigs were obtained in the coronal (A) and sagittal (B) planes to measure the dimensions (dotted lines) of the radiocarpal bones prior to surgery. Medial-Lateral = 7.4 mm; Volar-Dorsal = 17.5 mm and Proximal-Distal 10.5 mm. 3 mm osteotomies (C arrow) were performed through the mid-radiocarpal bone of both forelimbs. The volar and dorsal pieces of the LEFT radiocarpal (control) were fixed immediately and a dense-collagen spacer (D arrow) inserted in the gap of the RIGHT radiocarpal (non-union). After 7 weeks of healing the LEFT radiocarpal had no further intervention while the spacer in the RIGHT radiocarpal was removed, the volar and dorsal segments re-apposed and fixed with a screw (E). The mini-pigs were left for an addition 12 weeks before termination of the experiment.
Figure 2.
Surgical intervention to generate radiocarpal non-union: X-rays of the forearms of anesthetized mini-pigs were obtained in the coronal (A) and sagittal (B) planes to measure the dimensions (dotted lines) of the radiocarpal bones prior to surgery. Medial-Lateral = 7.4 mm; Volar-Dorsal = 17.5 mm and Proximal-Distal 10.5 mm. 3 mm osteotomies (C arrow) were performed through the mid-radiocarpal bone of both forelimbs. The volar and dorsal pieces of the LEFT radiocarpal (control) were fixed immediately and a dense-collagen spacer (D arrow) inserted in the gap of the RIGHT radiocarpal (non-union). After 7 weeks of healing the LEFT radiocarpal had no further intervention while the spacer in the RIGHT radiocarpal was removed, the volar and dorsal segments re-apposed and fixed with a screw (E). The mini-pigs were left for an addition 12 weeks before termination of the experiment.
The time taken to anesthetize the animals and perform bilateral surgical interventions on each of three mini-pigs varied between 80 min and 110 min. Surgeries were uneventful except for a partial fracture of the volar aspect of the left radiocarpal at the time of screw insertion in the first animal operated. This bone was subsequently excluded from all post-mortem analyses leaving only two animals for direct comparison of bone repair after immediate fixation (IF) and three for delayed fixation (DF). All mini-pigs were fully ambulatory within 48 hours post-operation and had no visible signs of infection or other complications after one week. Micro CT and un-decalcified histological analyses (
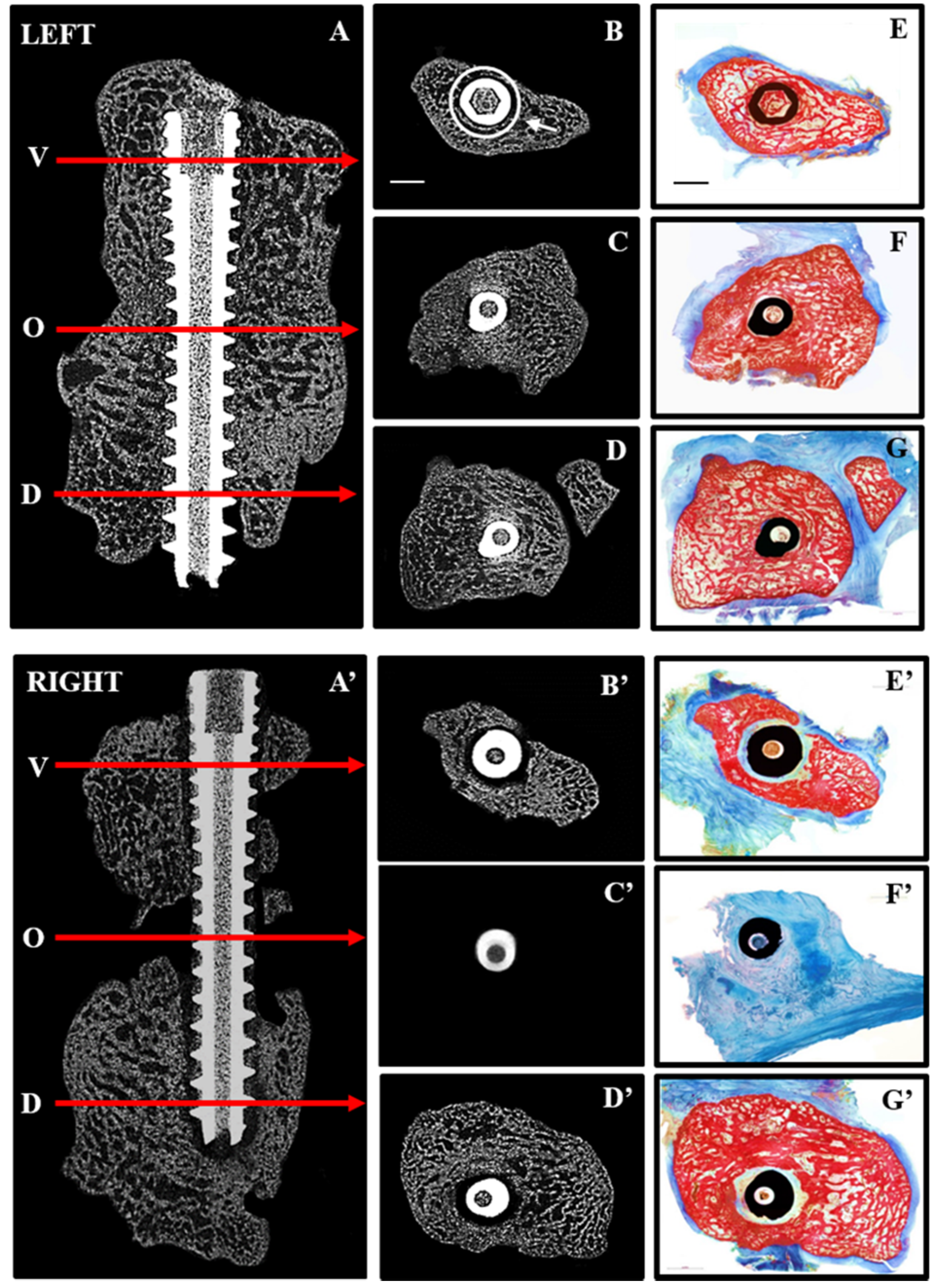
Figure 3) clearly demonstrated mal-union of the right radiocarpal bone at 19 weeks post-operative. The dorsal and volar segments were rigidly fixed at seven weeks after removal of the dense collagen spacer.
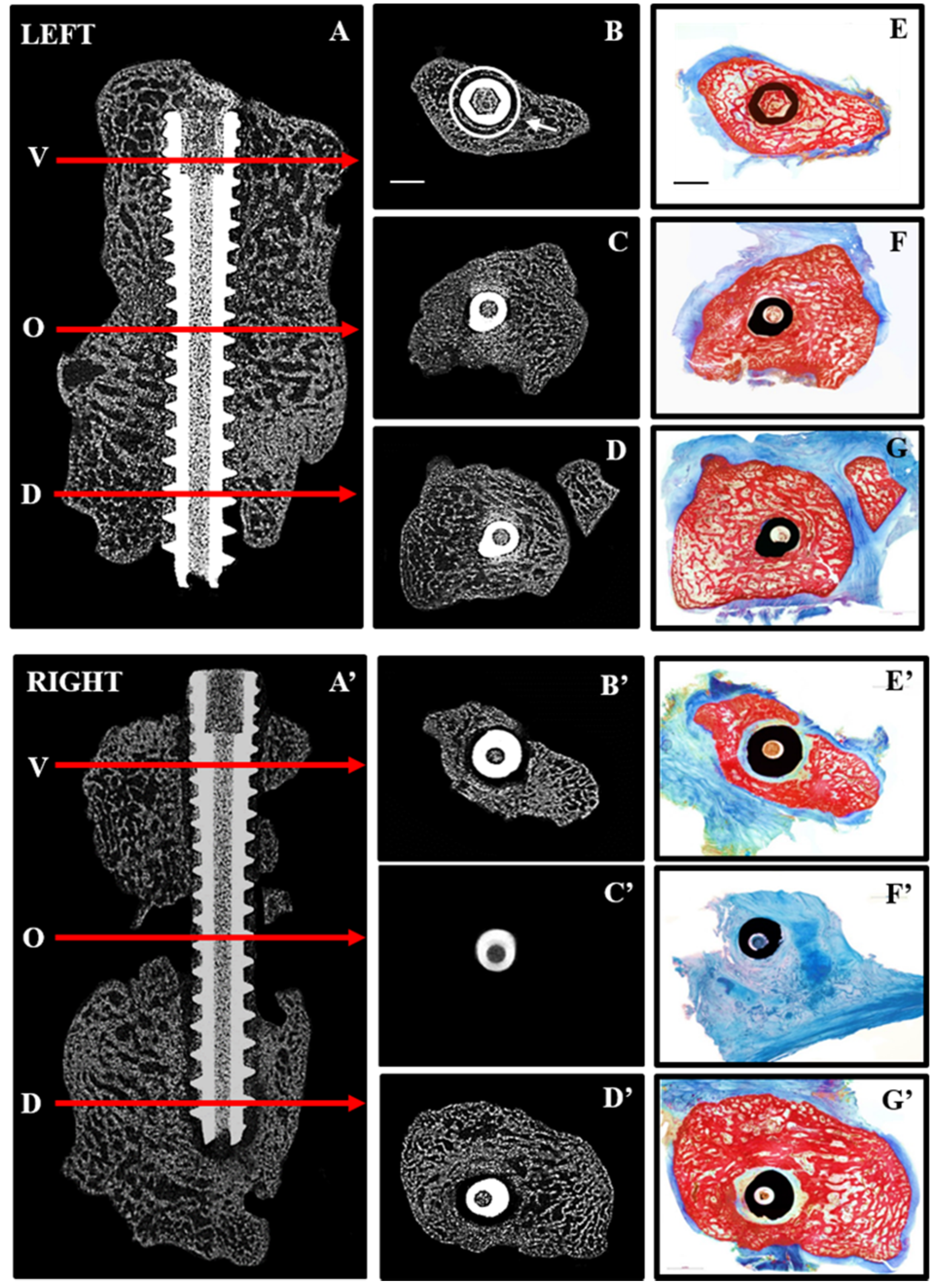
Figure 3.
Repair after immediate (LEFT) and delayed (RIGHT) fixation: 2D micro CT images are shown in the sagittal plane (A,A’) indicating the position along the screw (arrows) at which transaxial 2D images are shown for the volar (V,B,B’), osteotomy site (O,C,C’) and dorsal (D,D,D’) aspects of the radiocarpal bones. Corresponding histological sections from the same levels (E–G,E’–G’) were stained with Alizarin red and Methylene blue to distinguish mineralized (red) from soft (blue) tissue. Complete bridging occurred with immediate fixation (A,C) whereas little bone was seen in the osteotomy site (A’,C’) with delayed fixation. Histological sections confirmed the presence of bone in the osteotomy site with immediate fixation (F) and its absence with delayed fixation (F’). Arrow (B) points to ROI used for quantitative micro CT analyses and scale bars (B,E) represents 2 mm.
Figure 3.
Repair after immediate (LEFT) and delayed (RIGHT) fixation: 2D micro CT images are shown in the sagittal plane (A,A’) indicating the position along the screw (arrows) at which transaxial 2D images are shown for the volar (V,B,B’), osteotomy site (O,C,C’) and dorsal (D,D,D’) aspects of the radiocarpal bones. Corresponding histological sections from the same levels (E–G,E’–G’) were stained with Alizarin red and Methylene blue to distinguish mineralized (red) from soft (blue) tissue. Complete bridging occurred with immediate fixation (A,C) whereas little bone was seen in the osteotomy site (A’,C’) with delayed fixation. Histological sections confirmed the presence of bone in the osteotomy site with immediate fixation (F) and its absence with delayed fixation (F’). Arrow (B) points to ROI used for quantitative micro CT analyses and scale bars (B,E) represents 2 mm.
In contrast to immediate fixation (IF) (
Figure 3A–G), where bone was seen adjacent to the screw along its entire length, delayed fixation (DF) resulted in soft tissue along the length of the screw (
Figure 3A’–G’). This is most noticeable on the histological sections where bone is red and soft tissue blue. Quantitative micro CT (
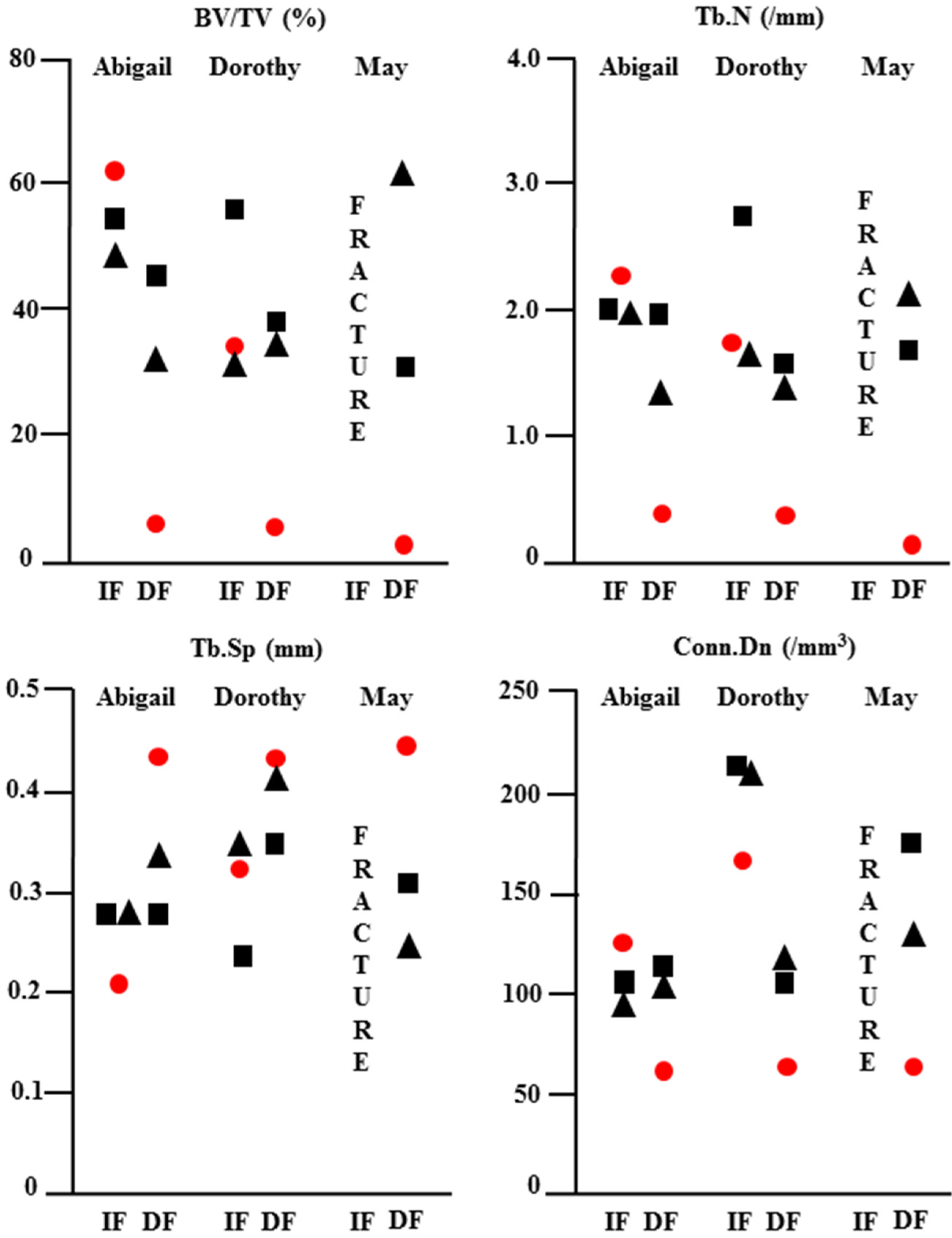
Figure 4) revealed significantly less bone (BV/TV) adjacent to the screw at the osteotomy site (white circle in
Figure 3B) with DF compared with IF.
Figure 4.
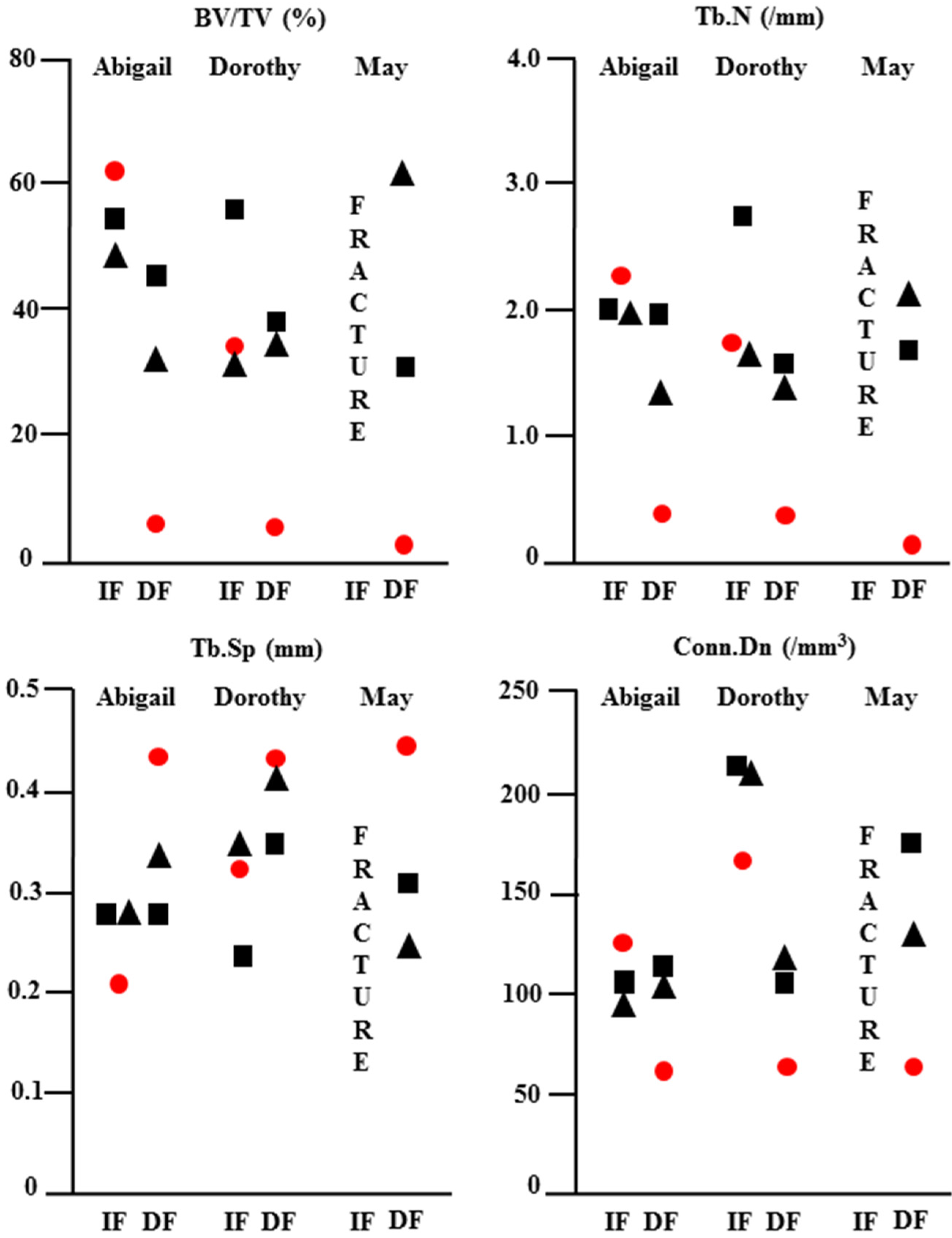
Quantitative micro CT analysis of repair after immediate (IF) and delayed (DF) fixation: The osteotomy site and adjacent bone in the LEFT (IF) and RIGHT (DF) radiocarpal bones of minipigs Abigail, Dorothy and May were scanned at 19 weeks post-operative and the data analysed using CtAn software. Quantitative data for bone volume/tissue volume (BV/TV), trabecular number (Tb.N), trabecular separation (Tb.Sp) and trabecular connectivity (Conn.Dn) are shown for the dorsal (square), osteotomy site (circle) and volar (triangle) aspects of the bone. Delayed fixation resulted in significantly less bone with poor quality at the osteotomy site in all animals.
Figure 4.
Quantitative micro CT analysis of repair after immediate (IF) and delayed (DF) fixation: The osteotomy site and adjacent bone in the LEFT (IF) and RIGHT (DF) radiocarpal bones of minipigs Abigail, Dorothy and May were scanned at 19 weeks post-operative and the data analysed using CtAn software. Quantitative data for bone volume/tissue volume (BV/TV), trabecular number (Tb.N), trabecular separation (Tb.Sp) and trabecular connectivity (Conn.Dn) are shown for the dorsal (square), osteotomy site (circle) and volar (triangle) aspects of the bone. Delayed fixation resulted in significantly less bone with poor quality at the osteotomy site in all animals.
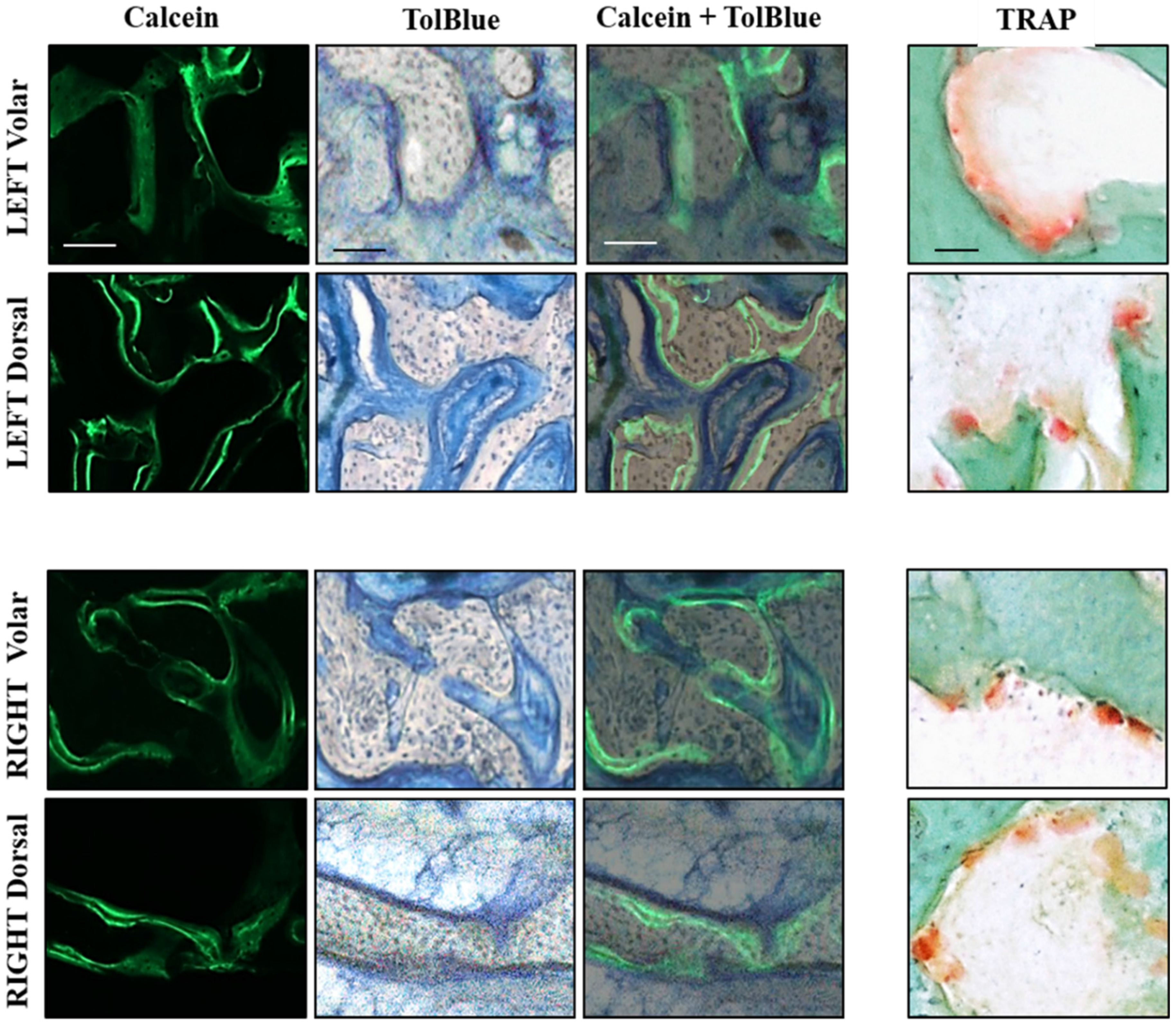
This trend was reflected by a significant reduction in the number (Tb.N) and connectivity (Conn.Dn) of trabeculae at the osteotomy site with DF. Histological analyses of bone formation and resorption are shown in 60 µm thick bone sections from the dorsal and volar aspects of left (IF) and right (DF) radiocarpal bones (
Figure 5). Dynamic labeling of bone formation with calcein, and staining of bone resorbing osteoclasts with TRAP, showed no difference between dorsal and volar aspects or RIGHT (IF) and LEFT (DF) specimens.
Figure 5.
Histological analysis of volar and dorsal aspects of radiocarpal bone: 60 µm sections were cut with a saw microtome from the volar and dorsal aspects of the LEFT (upper) and RIGHT (lower) radiocarpal bones, adjacent to those stained with Alizarin red in
Figure 4. The sections were first visualized under fluorescence microscopy to capture images of calcein labeling before staining with TolBlue to distinguish mineralized (grey) from soft (blue) tissue. The images were then super-imposed (Calcein + TolBlue) to identify active bone-forming surfaces. Adjacent sections were stained with TRAP and Fast Green to identify osteoclasts on surfaces undergoing resorption. No differences were seen in any staining between the Volar and Dorsal aspects or between LEFT and RIGHT radiocarpal bones. Scale bars represent 100 µm for Calcein and TolBlue images and 50 µm for TRAP images.
Figure 5.
Histological analysis of volar and dorsal aspects of radiocarpal bone: 60 µm sections were cut with a saw microtome from the volar and dorsal aspects of the LEFT (upper) and RIGHT (lower) radiocarpal bones, adjacent to those stained with Alizarin red in
Figure 4. The sections were first visualized under fluorescence microscopy to capture images of calcein labeling before staining with TolBlue to distinguish mineralized (grey) from soft (blue) tissue. The images were then super-imposed (Calcein + TolBlue) to identify active bone-forming surfaces. Adjacent sections were stained with TRAP and Fast Green to identify osteoclasts on surfaces undergoing resorption. No differences were seen in any staining between the Volar and Dorsal aspects or between LEFT and RIGHT radiocarpal bones. Scale bars represent 100 µm for Calcein and TolBlue images and 50 µm for TRAP images.
3.3. Discussion
The diagnosis and treatment of scaphoid fractures remains a significant challenge to orthopedic surgeons. Conventional radiography is often insufficient to make a definitive immediate diagnosis, whereas CT scan and MRI scans are often not obtained initially by the clinician without a strong index of suspicion for a suspected scaphoid fracture. In fact, many patients do not even present early to the hospital or clinic, believing they have only sustained a wrist sprain. Therefore, significant delays in treatment are common in patients with scaphoid fractures. Diagnostic capabilities have improved using gadolinium-enhanced MRI imaging in order to evaluate the vascular feed and potential viability of the proximal pole following acute scaphoid fracture [
17]. However, one still requires a clinical suspicion of fracture in order to obtain the test.
Non-displaced fractures with viable proximal and distal fragments can be treated by a prolonged period of immobilization in a cast, thereby avoiding surgery-related complications. However, prolonged immobilization leads to muscle atrophy and stiffness that may require an extended period of physiotherapy to achieve pre-injury function. Since the majority of scaphoid fractures occur in young patients, the need for prolonged immobilization can also have significant consequences related to time required off work. Hence, there has been a recent trend to expedite return to full early activities by treatment with immediate surgical fixation, even for non-displaced fractures, although displacement is commonplace [
18,
19]. The mainstay of treatment for scaphoid fractures is therefore early surgical fixation with a headless compression screw, similar to that used in the current study.
Due to delays in presentation, the low diagnostic yield of routine imaging combined with the inefficiency of immobilization, many patients present with pain and reduced mobility of the wrist arising from an established scaphoid non-union. Non-union of scaphoid fractures leads to a progressive pattern of degeneration of the wrist joint known as scaphoid non-union advanced collapse. Therefore, it is important to treat scaphoid non-union to avoid the development of degenerative changes in the wrist. The management of scaphoid non-union is challenging and complex and must be addressed surgically with internal fixation in a similar manner to the treatment of acute fractures. However, the healing potential of a non-union is significantly reduced compared with acute fractures and can typically require bone grafting and/or revascularization procedures to improve the biology of the healing milieu. In addition, scaphoid non-union also commonly leads to bone loss and deformity, requiring the use of structural bone grafts. All of these adjunct procedures add to the surgical morbidity associated with the treatment of scaphoid non-union, compared with the treatment of an acute fracture. Despite the use of all these adjunct techniques, the healing rate for scaphoid non-union remains lower than for acute fracture. The significant challenges and morbidity involved in the treatment of scaphoid non-union therefore necessitates the development of novel approaches that will simplify the surgical intervention and reduce morbidity. This is best accomplished in an appropriate, reproducible, pre-clinical large animal model, such as the one we have described [
20].
Domestic pigs and miniature swine have been traditionally used to investigate diagnostic and therapeutic interventions for circulatory disorders like avascular necrosis of the femoral head [
21,
22,
23]. Using contrast agent and high resolution micro CT imaging we showed in the current study that the vascular supply to the radiocarpal bone in swine is similar to that in humans. The limited blood supply to the distal pole can be compromised by fracture. In addition, inadequate immobilization after fracture, as in the case of the RIGHT radiocarpal bones in our study leads to the reproducible creation of a radiocarpal non-union. The presence of fibrous tissue at the osteotomy site, 12 weeks after DF, indicated a Type DI established non-union according to the Herbert classification [
24,
25].
An ultra-rapid engineering approach using unconfined compression of hydrated type I collagen gels was developed a decade ago to manufacture biomimetic materials for bone tissue engineering [
26]. The approach allowed us to generate a dense collagen material after plastic compression with mechanical properties similar to osteoid. Studies in the laboratories of colleagues have investigated the enhanced
ex vivo biomineralization properties of dense collagen gels, alone [
27] or in composite materials with silk fibroin [
28]. However, in our previous work using a mouse model of bone healing, it was shown that the dense collagen material formed an effective barrier to
in vivo bone repair [
15] in the absence of an angiogenic agent like VEGF. For this reason we hypothesized that the dense collagen gels would also inhibit neo-vascularization in the 3 mm defect during the early phase of bone regeneration and effectively inhibit repair of the defect in the longer term. In the current study, the absence of bone bridging in the right radiocarpal bones demonstrates that the dense collagen spacer, when inserted in the fracture gap for seven weeks prior to delayed fixation, served as an effective method to promote the reproducible creation of non-union of the radiocarpal bone that can be used to investigate novel therapeutic interventions and/or fixation hardware. For example, this mini-pig non-union model will be used to investigate the
in vivo efficacy of a patented porous titanium screw for improved scaphoid fixation. In recent work, the biomechanical properties and insertion profiles of the screw were shown to compare favorably with those of the commercially available solid titanium screws [
29].


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}