
The Potential of Three Computer-Based Communication Activities for Supporting Older Adult Independent Living

Abstract
:1. Introduction
1.1. Technology and Older Adults
1.2. Technology and Safety
1.3. The Advent of Computer Tools
2. Method
2.1. Participants
2.2. Implementation of the Daily Diary and Skype
2.3. Installation
2.4. Procedure and Compliance
2.4.1. Check-in
2.4.2. Daily Health Diary
2.4.3. Skype Chat
2.5. Focus Group Discussion
2.6. Data Analysis
3. Results
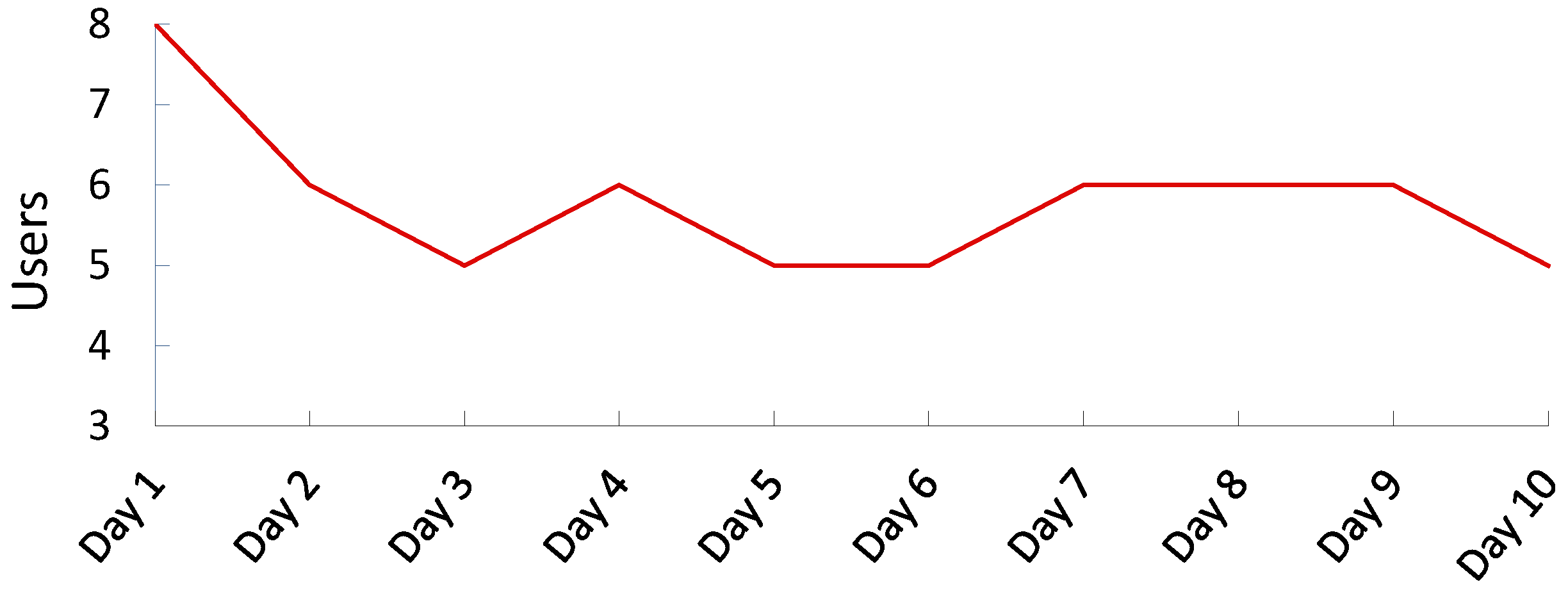
3.1. Older Adults’ Abilities and Compliance Rate in Health Monitoring
3.2. Three Themes from a Focus Group
3.2.1. Accessibility
“Not criticizing your question, but…if you carried this thing a step further and it was being used by professionals, your questions wouldn’t be of such a general nature and ultimately the questions would have to be refined to the person.”
“Some will have quite the detailed questionnaire and others will have a relatively simple one. There is a lot of relativity as you move to one person to the other.”
3.2.2. Awareness
3.2.3. Safety and Intrusion
“But, uh, any kind of signal that we came up with [at the independent living apartment complex] …either people didn’t want us to be checking on them or they figured it wasn’t a good enough plan and we’ve never done anything. And, generally speaking, we know what the next-door neighbor’s doing or some person we are in touch with. But it failed once. I mean we lost somebody over a weekend…”
4. Discussion
4.1. Design Best Practices
4.2. Limitations
4.3. Implications and Future Research
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Burdick, D.C.; Kwon, S. (Eds.) Gerontechnology: Research and Practice in Technology and Aging; Springer: New York, NY, USA, 2004; pp. xxv–xxvii.
- Rogers, E. Diffusion of Innovations, 5th ed.; Free Press: New York, NY, USA, 2003. [Google Scholar]
- Czaja, S.J.; Lee, C. The impact of aging on access to technology. Univers. Access Inf. Soc. 2007, 5, 341–349. [Google Scholar] [CrossRef]
- Demeris, G.; Rantz, M.J.; Aud, M.A.; Marek, K.D.; Tyrer, H.W.; Skubic, M.; Hussam, A.A. Older adults’ attitudes towards and perceptions of “smart home” technologies: A pilot study. Med. Inf. Internet Med. 2004, 29, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, L.; Hanson, E. Supporting frail older people and their family carers at home using information and communication technology: Cost analysis. J. Adv. Nurs. 2005, 51, 645–657. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Redington, L.; Steinmetz, V.; Lindeman, D. The ADOPT model: Accelerating diffusion of proven technologies for older adults. Ageing Int. 2011, 36, 39–45. [Google Scholar] [CrossRef]
- Pew, R.; Van Hemel, S. (Eds.) Technology for Adaptive Aging; National Academy Press: Washington, DC, USA, 2004.
- Cutler, S.J. Ageism and technology. Generations 2005, 29, 67–72. [Google Scholar]
- Eisma, R.; Dickinson, A.; Goodman, J.; Syme, A.; Tiwari, L.; Newell, A.F. Early user involvement in the development of information technology-related products for older people. Univers. Access Inf. Soc. 2004, 3, 131–140. [Google Scholar] [CrossRef]
- Charness, N.; Boot, W.R. Aging and information technology use: Potential and barriers. Curr. Dir. Psychol. Sci. 2009, 18, 253–258. [Google Scholar] [CrossRef]
- de Moraes Barros, G.D.V. Falls in elderly people. Lancet 2006, 367, 729–730. [Google Scholar] [CrossRef]
- Scanaill, C.N.; Garattini, C.; Greene, B.R.; McGrath, M.J. Technology innovation enabling falls risk assessment in a community setting. Ageing Int. 2011, 36, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Kannus, P.; Sievanen, H.; Palvanen, M.; Jarvinen, T.; Parkkari, J. Prevention of falls and consequent injuries in elderly people. Lancet 2005, 366, 1885–1893. [Google Scholar] [CrossRef]
- Dishman, E.; Matthews, J.; Dunbar-Jacob, J. Everyday health: Technology for adaptive aging. In Technology for Adaptive Aging; Pew, R.W., Van Hemel, S.B., Eds.; National Academy Press: Washington, DC, USA, 2004; pp. 179–208. [Google Scholar]
- Fallon, L.F., Jr.; Awosika-Olumo, A.; Fulks, J.S. Factors related to accidents and falls among older individuals. Traumatology 2002, 8, 205–210. [Google Scholar] [CrossRef]
- Nehmer, J.; Becker, M.; Kleinberger, T.; Pruckner, S. Electronic emergency safeguards: Sensor-based detection and prevention of critical health conditions. GeroPsych 2010, 23, 91–98. [Google Scholar] [CrossRef]
- Dishman, E. Inventing wellness systems for aging in place. Computer 2004, 37, 34–41. [Google Scholar] [CrossRef]
- Rogers, W.A.; Mayhorn, C.B.; Fisk, A.D. Technology in everyday life for older adults. In Gerontechnology: Research and Practice in Technology and Aging; Burdick, D.C., Kwon, S., Eds.; Springer: New York, NY, USA, 2004; pp. 3–17. [Google Scholar]
- Virzi, R.A. Refining the test phase of usability evaluation: How many subjects is enough? J. Hum. Factors Ergon. Soc. 1992, 34, 457–468. [Google Scholar]
- Merriam, S.B. Qualitative Research, a Guide to Design and Implementation; Jossey-Bass: San Francisco, CA, USA, 2009. [Google Scholar]
- Terrell, S. Mixed-methods research methodologies. Qual. Rep. 2012, 17, 254–280. [Google Scholar]
- Creswell, J.W. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches; Sage Publications Ltd.: Thousand Oaks, CA, USA, 2008. [Google Scholar]
- Klasnja, P.; Consolvo, S.; McDonald, D.W.; Landay, J.A.; Pratt, W. Using mobile and personal sensing technologies to support health behavior change in everyday life: Lessons learned. AMIA Annu. Symp. Proc. 2009, 2009, 338–342. [Google Scholar] [PubMed]
- Wright, P. The internet’s potential for enhancing healthcare. Gerontechnology 2012, 11, 35–45. [Google Scholar] [CrossRef]
- Preschl, B.; Wagner, B.; Forstmeier, S.; Maercker, A. E-health interventions for depression, anxiety disorder, dementia, and other disorders in adults: A review. J. CyberTher. Rehabil. 2011, 4, 371–385. [Google Scholar]

{kind=link}
| Category | Frequency | Percent | |
|---|---|---|---|
| Age (M = 85.13, SD = 3.09) | |||
| Gender | Male | 5 | 62.5 |
| Female | 3 | 37.5 | |
| Total | 8 | 100.0 | |
| Ethnicity | White | 8 | 100.0 |
| Marital Status | Married | 6 | 75.0 |
| Widowed | 2 | 25.0 | |
| Total | 8 | 100.0 | |
| Employment Status | Retired | 8 | 100.0 |
| General Questions |
|
| Check-In Task |
|
| Skype |
|
| Daily Health Diary |
|
| Accessibility | Awareness | Safety and Intrusion |
|---|---|---|
| Finances | Eating | Privacy |
| Specificity | Routine | Security |
| Flexibility | Remembering | Emergency |
| Rural areas | Tech savvy | - |
| Timing | Socialization | - |
| Category | Frequency | Percent | |
|---|---|---|---|
| General Computer Skill | Very Confident (= 5) | 0 | 0.0 |
| Somewhat Confident (= 4) | 3 | 37.5 | |
| Neutral (= 3) | 2 | 25.0 | |
| Somewhat Uncertain (= 2) | 0 | 0.0 | |
| Very Uncertain (= 1) | 3 | 37.5 | |
| Total | 8 | 100.0 | |
| Computer Usage | Every day | 2 | 25.0 |
| Several Times a Day | 4 | 50.0 | |
| Several Times a Week | 1 | 12.5 | |
| Once a Month | 1 | 12.5 | |
| Total | 8 | 100.0 | |
| User 1 | User 2 | User 3 | User 4 | User 5 | User 6 | User 7 | User 8 | |
|---|---|---|---|---|---|---|---|---|
| Compliance Rates | 90% | 90% | 40% | 100% | 80% | 100% | 70% | 10% |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heinz, M.; Cho, J.; Kelly, N.; Martin, P.; Wong, J.; Franke, W.; Hsieh, W.-H.; Blaser, J. The Potential of Three Computer-Based Communication Activities for Supporting Older Adult Independent Living. Information 2016, 7, 26. https://doi.org/10.3390/info7020026
Heinz M, Cho J, Kelly N, Martin P, Wong J, Franke W, Hsieh W-H, Blaser J. The Potential of Three Computer-Based Communication Activities for Supporting Older Adult Independent Living. Information. 2016; 7(2):26. https://doi.org/10.3390/info7020026
Chicago/Turabian StyleHeinz, Melinda, Jinmyoung Cho, Norene Kelly, Peter Martin, Johnny Wong, Warren Franke, Wen-Hua Hsieh, and Joan Blaser. 2016. "The Potential of Three Computer-Based Communication Activities for Supporting Older Adult Independent Living" Information 7, no. 2: 26. https://doi.org/10.3390/info7020026