
Food Safety Information Processing and Teaching Behavior of Dietitians: A Mental Model Approach

Abstract
:1. Introduction
1.1. The Risk Information Seeking and Processing (RISP) Communication Theory
1.2. Mental Models
1.3. Study Objectives
2. Results and Discussion
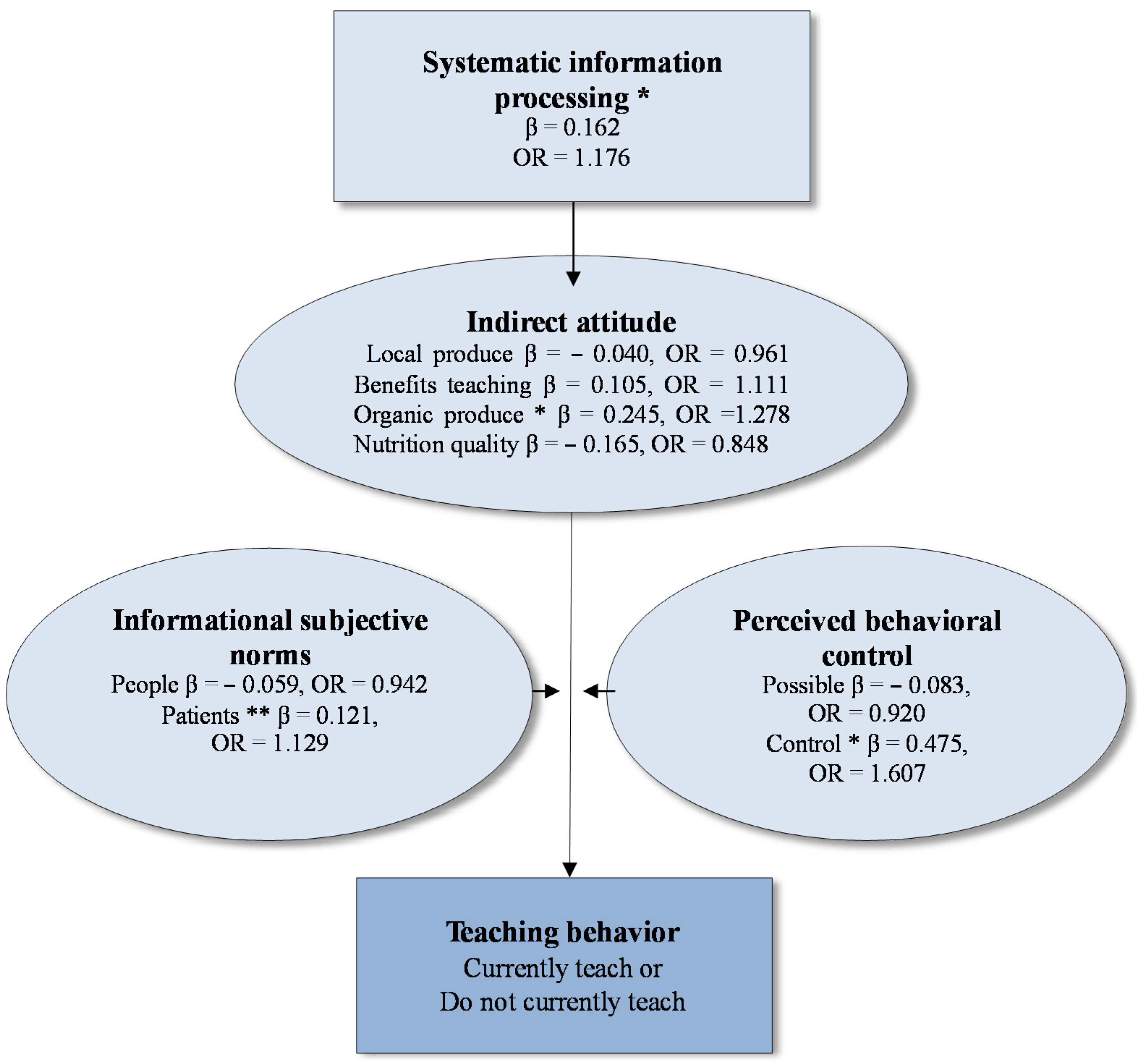
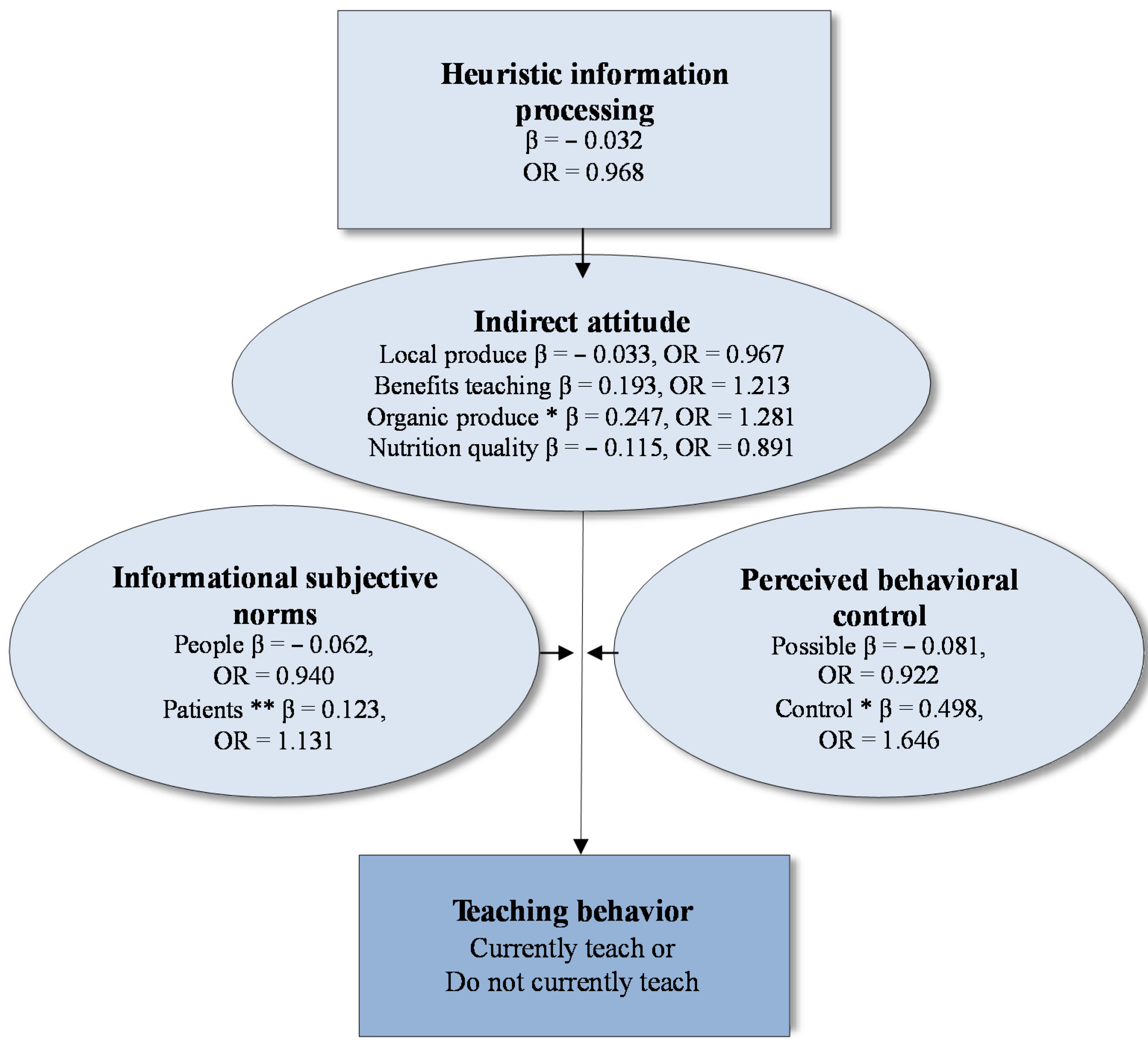
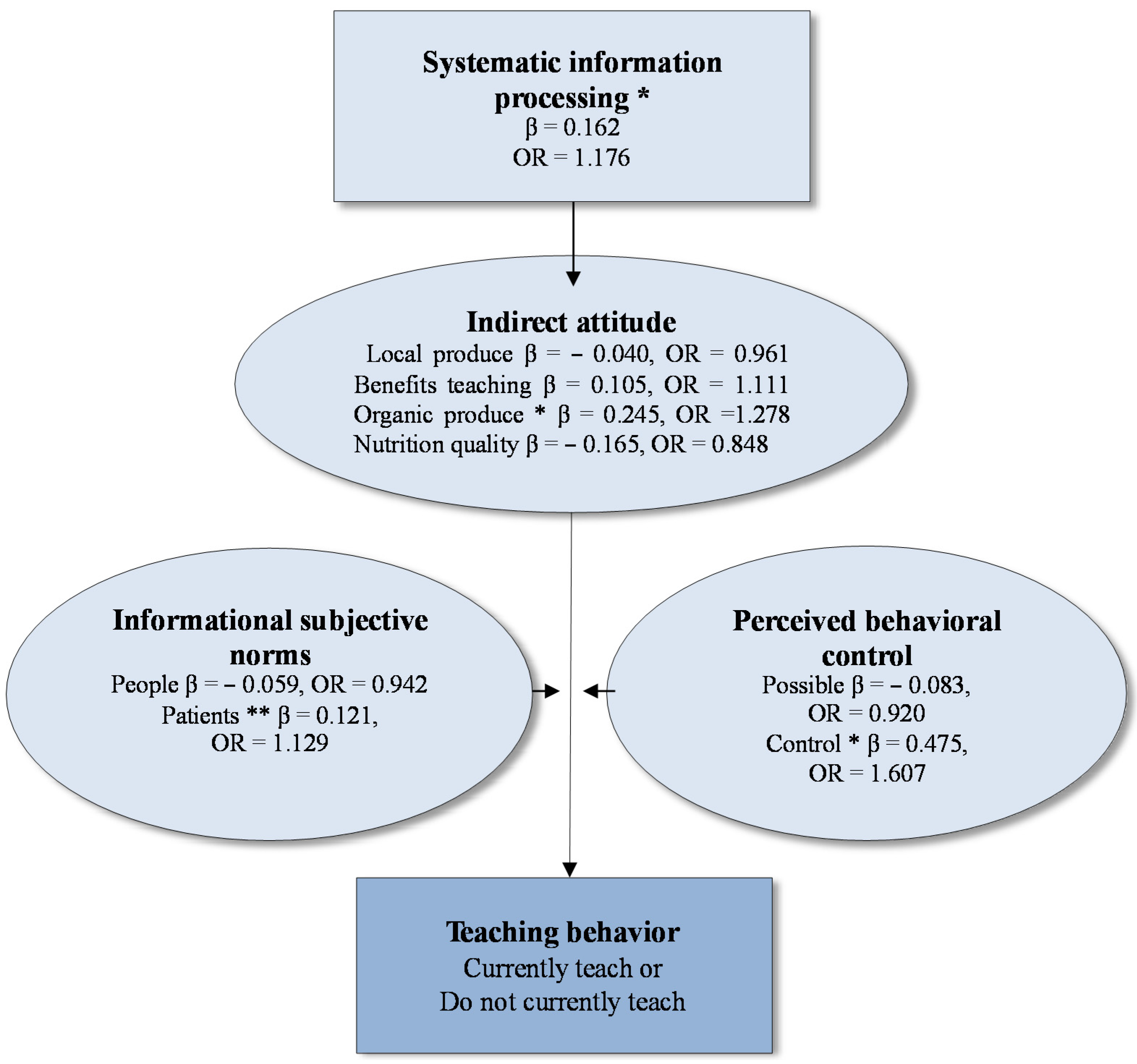
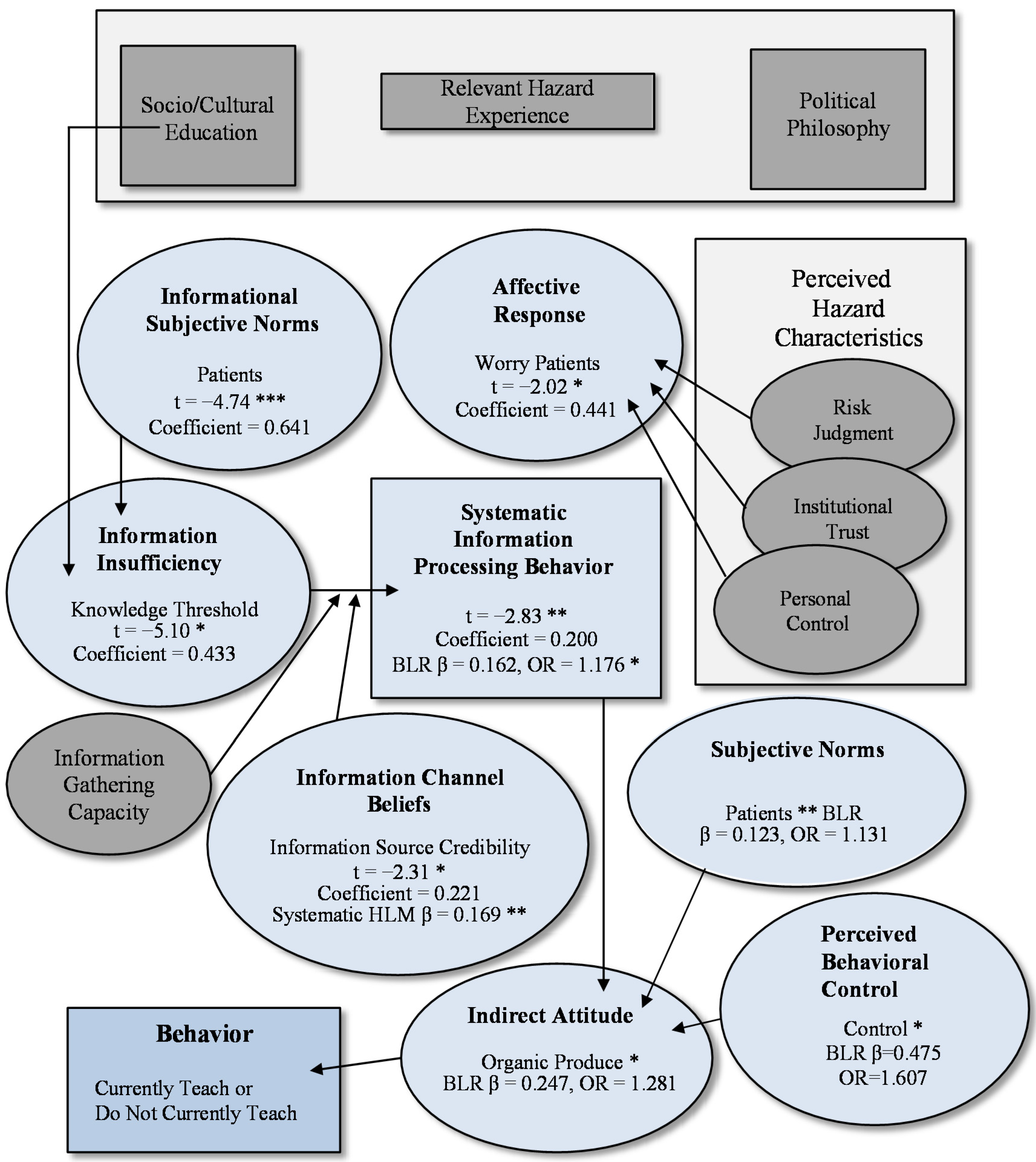
2.1. The RISP Communication Theory

{kind=link}
{kind=link}
{kind=link}
| Variables | Systematic information processing | ||||
|---|---|---|---|---|---|
| Do not Currently Teach (n = 144) | Currently Teach (n = 155) | Overall (n = 299) | |||
| Individual characteristics | |||||
| Caucasian ethnic group | 0.223 | 0.314 | 0.265 * | ||
| Other ethnic group | 0.220 | 0.279 | 0.224 * | ||
| Income $64K or less | 0.159 | −0.004 | 0.020 | ||
| Income $65K to $ 99K | 0.169 | −0.071 | 0.008 | ||
| Income $100K or more | 0.055 | −0.033 | −0.066 | ||
| Age 18–29 years | ------- | −0.142 | −0.077 | ||
| Age 30–44 years | 0.096 | −0.145 | ------- | ||
| Age 45 years and older | 0.158 | ------- | 0.072 | ||
| Liberal political philosophy | −0.008 | −0.027 | −0.013 | ||
| Neutral political philosophy | −0.053 | −0.010 | −0.027 | ||
| Conservative political philosophy | −0.058 | 0.153 | 0.035 | ||
| FBI-self, medical | 0.111 | 0.021 | 0.039 | ||
| FBI-self, no medical | −0.097 | 0.101 | 0.039 | ||
| FBI-others, medical | 0.129 | −0.062 | 0.009 | ||
| FBI-others, no medical | 0.057 | −0.135 | −0.052 | ||
| FBI-patients, medical | −0.035 | −0.071 | −0.060 | ||
| FBI-patients, no medical | 0.080 | 0.003 | 0.028 | ||
| Perceived hazard characteristics | |||||
| Risk judgment | 0.001 | 0.119 | 0.091 | ||
| Institutional trust | 0.055 | −0.037 | 0.017 | ||
| Personal control-self | 0.155 | 0.125 | 0.141 * | ||
| Personal control-patients | 0.094 | −0.123 | −0.009 | ||
| Informational subjective norms | |||||
| People | 0.022 | −0.016 | 0.030 | ||
| Patients | 0.145 | 0.049 | 0.063 | ||
| Affect, worry | |||||
| Self | 0.121 | −0.175 | −0.083 | ||
| Patient | −0.032 | 0.149 | 0.013 | ||
| Channel beliefs | |||||
| Media bias beliefs | −0.106 | −0.189 * | −0.131 * | ||
| Validity cues beliefs | 0.077 | 0.189 * | 0.131 * | ||
| Information source credibility | 0.248 ** | 0.079 | 0.169 ** | ||
| Information gathering capacity | |||||
| Capacity | 0.038 | −0.043 | 0.002 | ||
| Current knowledge | |||||
| General food safety knowledge | −0.005 | −0.001 | −0.027 | ||
| Pathogen awareness | 0.060 | −0.008 | 0.036 | ||
| Pathogen understanding | −0.124 | 0.206 | 0.056 | ||
| Information insufficiency | |||||
| Knowledge threshold | −0.093 | 0.158 | 0.070 | ||
| Final model statistics | P = 0.019 R2 = 0.126 | P = 0.023 R2 = 0.114 | P < 0.000 R2 = 0.139 | ||
| Variables | Heuristic information processing | ||||
|---|---|---|---|---|---|
| Do not Currently Teach (n = 144) | Currently Teach (n = 156) | Overall (n = 300) | |||
| Individual Characteristics | |||||
| Caucasian ethnic group | 0.167 | −0.083 | −0.005 | ||
| Other ethnic group | 0.038 | −0.085 | −0.022 | ||
| Income $64K or less | 0.105 | −0.064 | 0.005 | ||
| Income $65K to $ 99K | 0.082 | 0.054 | 0.065 | ||
| Income $100K or more | 0.054 | −0.142 | −0.037 | ||
| Age 18–29 years | ------- | 0.104 | 0.044 | ||
| Age 30–44 years | −0.018 | 0.127 | ------- | ||
| Age 45 years and older | −0.153 | ------- | −0.105 | ||
| Liberal political philosophy | 0.140 | 0.166 | 0.118 | ||
| Neutral political philosophy | 0.018 | 0.174 | 0.084 | ||
| Conservative political philosophy | 0.070 | 0.210 | 0.102 | ||
| FBI-self, medical | −0.040 | −0.067 | −0.055 | ||
| FBI-self, no medical | 0.089 | −0.086 | 0.004 | ||
| FBI-others, medical | −0.124 | 0.037 | −0.035 | ||
| FBI-others, no medical | −0.054 | −0.055 | −0.073 | ||
| FBI-patients, medical | 0.000 | −0.060 | −0.037 | ||
| FBI-patients, no medical | 0.084 | 0.204 ** | 0.152 ** | ||
| Perceived hazard characteristics | |||||
| Risk judgment | 0.087 | 0.067 | 0.056 | ||
| Institutional trust | −0.062 | 0.145 | 0.032 | ||
| Personal control-self | −0.043 | 0.162 | 0.102 | ||
| Personal control-patients | 0.012 | −0.156 | −0.081 | ||
| Informational subjective norms | |||||
| People | −0.066 | -0.248 * | −0.156 * | ||
| Patients | −0.014 | 0.088 | 0.049 | ||
| Affect, worry | |||||
| Self | −0.239 | 0.038 | −0.034 | ||
| Patient | 0.055 | 0.019 | 0.000 | ||
| Channel beliefs | |||||
| Media bias beliefs | 0.062 | 0.193 * | 0.143 ** | ||
| Validity cues beliefs | −0.033 | 0.047 | 0.011 | ||
| Information source credibility | −0.288 ** | −0.365 *** | −0.330 *** | ||
| Information gathering capacity | |||||
| Capacity | 0.178 * | 0.082 | 0.133 * | ||
| Current knowledge | |||||
| General food safety knowledge | −0.117 | −0.053 | −0.122 * | ||
| Pathogen awareness | −0.079 | −0.132 | −0.082 | ||
| Pathogen understanding | 0.039 | 0.096 | 0.039 | ||
| Information insufficiency | |||||
| Knowledge threshold | −0.035 | −0.080 | −0.088 | ||
| Final model statistics | P < 0.000 R2 = 0.232 | P < 0.000 R2 = 0.311 | P < 0.000 R2 = 0.286 | ||
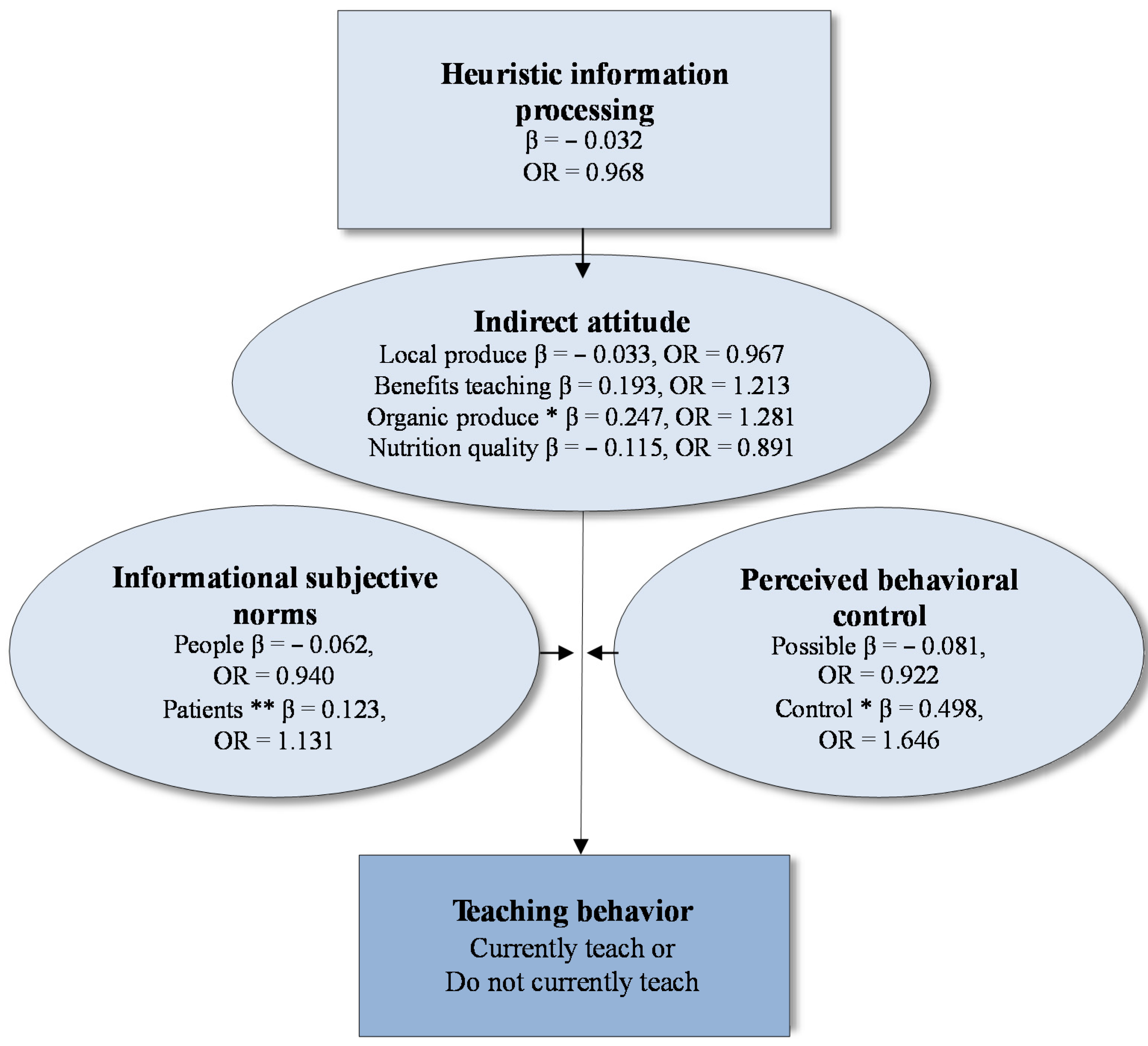
2.2. The Theory of Planned Behavior
| Indirect Attitude Measures | Factor Loading b | |||
|---|---|---|---|---|
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | |
| Local Produce | Benefits Teaching | Organic Produce | Nutrition Quality | |
| Total nutrition content important | 0.723 | |||
| Total fiber content important | 0.777 | |||
| Vitamin content important | 0.727 | |||
| Choose easy to prepare vegetables | 0.549 | |||
| Fresh vegetable cost important | 0.540 | |||
| Less foodborne illness among patients | 0.640 | |||
| More thankful patients | 0.737 | |||
| Teaching food safety good for dietitian’s reputation | 0.732 | |||
| More awareness about food safety in community | 0.681 | |||
| Food safety necessary for highly susceptible patients | 0.503 | |||
| Local produce has less bacterial contamination | 0.583 | |||
| Local produce tastes better | 0.904 | |||
| Local produce is better quality | 0.914 | |||
| Local produce helps the local economy | 0.876 | |||
| Being organically grown is important | 0.583 | |||
| Organic produce tastes better | 0.833 | |||
| Organic produce is more nutritious | 0.855 | |||
| Organic produce has less bacterial contamination | 0.780 | |||
| Organic produce has less pesticide contamination | 0.548 | |||
| Cronbach alpha | 0.89 | 0.79 | 0.79 | 0.76 |
| Variance explain by factor (%) | 11.62 | 11.31 | 10.14 | 9.11 |
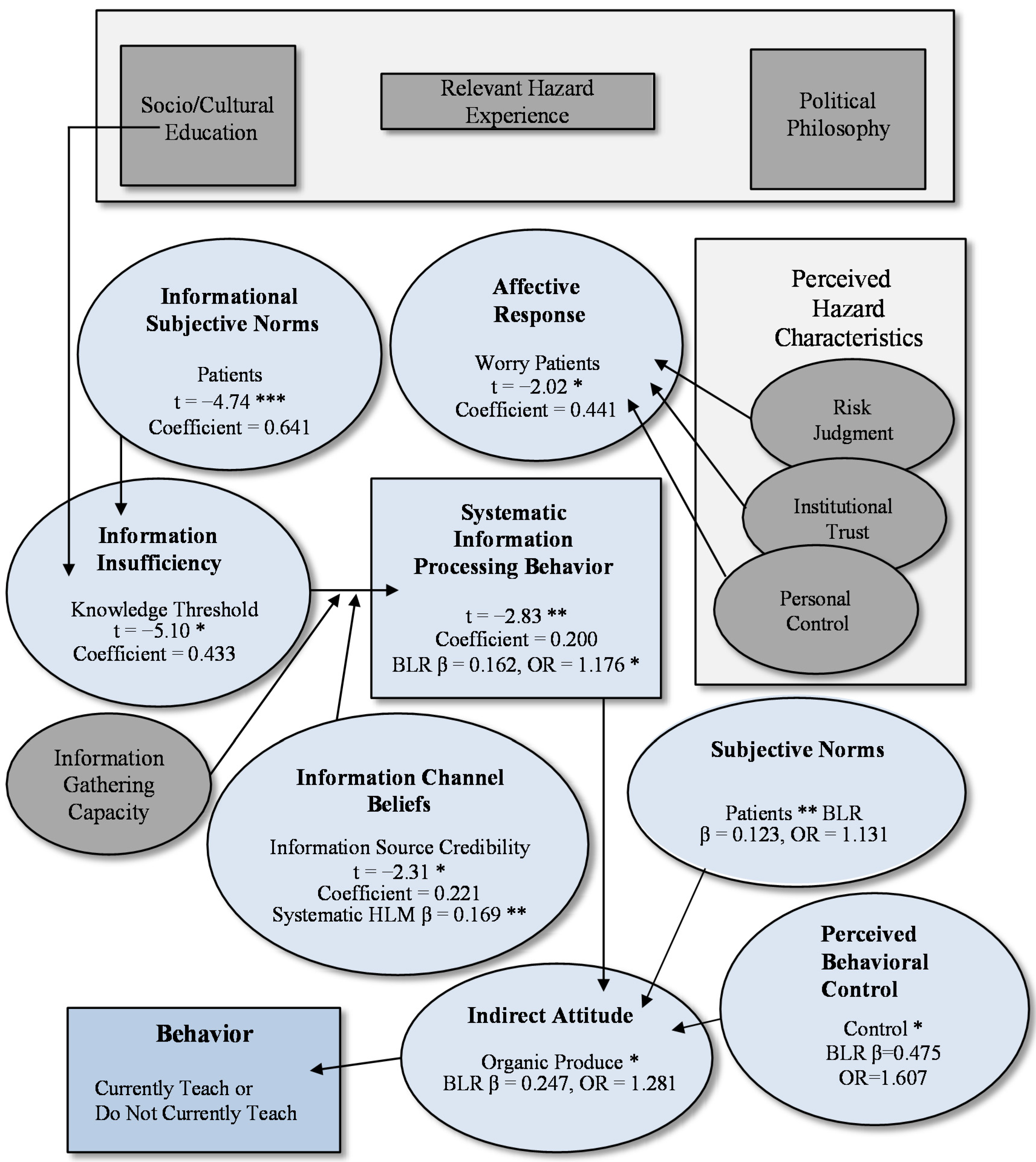
2.3. The Mental Model
3. Experimental Section
3.1. Respondent Recruitment
3.2. The Survey
3.3. Control Variables
3.4. RISP Communication Theory Variables
3.5. Theory of Planned Behavior Variables
3.6. Data Analyses
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mazzocchi, M.; Lobb, A.; Bruce Traill, W.; Cavicchi, A. Food scares and trust: A European study. J. Agric. Econ. 2008, 59, 2–24. [Google Scholar] [CrossRef]
- Shepherd, J.; Saghaian, S. Consumer response to and trust of information about food-safety events in the chicken and beef markets in Kentucky. J. Food Distri. Res. 2008, 39, 123–129. [Google Scholar]
- Kersting, A.L.; Medeiros, L.C.; LeJeune, J.T. Differences in Listeria monocytogenes contamination of rural Ohio residences with and without livestock. Foodborne Pathog. Dis. 2010, 7, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Kendall, P.; Medeiros, L.C.; Hillers, V.; Chen, G.; DiMascola, S. Food handling behaviors of special importance for pregnant women, infants and young children, the elderly and immune compromised people. J. Am. Diet. Assoc. 2003, 103, 1646–1649. [Google Scholar] [CrossRef] [PubMed]
- Athearn, P.N.; Kendall, P.A.; Hillers, V.; Schroeder, M.; Bergman, V.; Chen, G.; Medeiros, L. Awareness and acceptance of current food safety recommendations during pregnancy. Matern. Child Hlth. J. 2004, 8, 149–162. [Google Scholar] [CrossRef]
- Hoffman, E.W.; Bergmann, V.; Schultz, J.S.; Kendall, P.; Medeiros, L.D.; Hillers, V.N. Application of a five-step message development model for food safety education materials targeting people with HIV/AIDS. J. Am. Diet. Assoc. 2005, 105, 1597–1604. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, L.C.; Chen, G.; Hillers, V.N.; Kendall, P.A. Discovery and development of educational strategies to encourage safe food handling behaviors in cancer patients. J. Food Protect. 2008, 71, 1666–1672. [Google Scholar]
- Chen, G.; Kendall, P.A.; Hillers, V.N.; Medeiros, L.C. Qualitative studies of the food safety knowledge and perceptions of transplant patients. J. Food Protect. 2010, 73, 327–335. [Google Scholar]
- WebMD. Available online: http://www.webmd.com/ (accessed on 13 March 2015).
- Accreditation Council for Education in Nutrition and Dietetics, Academy of Nutrition and Dietetics. ACEND Accreditation Standards for Dietitian Education Programs Leading to the RD Credential. Available online: http://www.eatrightacend.org/WorkArea/DownloadAsset.aspx?id=6442468848 (accessed on 15 March 2015).
- Van Duyn, M.A.S.; Pivonka, E. Overview of the health benefits of fruit and vegetable consumption for the dietetics professional: Selected literature. J. Am. Diet. Assoc. 2000, 100, 1511–1521. [Google Scholar] [CrossRef] [PubMed]
- Hanning, I.B.; Nutt, J.D.; Ricke, S.C. Salmonellosis outbreaks in the United States due to fresh produce: Sources and potential intervention measures. Foodborne Pathog. Dis. 2009, 6, 635–648. [Google Scholar] [CrossRef] [PubMed]
- French, M.R.; Levy-Milne, R.; Zibrik, D. A survey of the use of low microbial diets in pediatric bone marrow transplant programs. J. Am. Diet. Assoc. 2001, 101, 1194–1198. [Google Scholar] [CrossRef] [PubMed]
- Eagly, A.H.; Chaiken, S. The Psychology of Attitudes; Harcourt Brace: San Diego, CA, USA, 1993. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Dec. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Griffin, R.J.; Dunwoody, S.; Neuwirth, K. Proposed model of the relationship of risk information seeking and processing to the development of preventive behaviors. Environ. Res. Sec. A 1999, 80, S230–S245. [Google Scholar] [CrossRef]
- Lynam, T.; Brown, K. Mental models in human-environment interactions: Theory, policy implications, and methodological explorations. Ecol. Soc. 2011, 17, 24. Available online: http://dx.doi.org/10.5751/ES-04257-170324 (accessed on 13 March 2015). [Google Scholar]
- Jones, J.A.; Ross, H.; Lynam, T.; Perez, P.; Leitch, A. Mental models: An interdisciplinary synthesis of theory and methods. Ecol. Soc. 2011, 16, 46. Available online: http://www.ecologyandsociety.org/vol16/iss1/art46/ (accessed on 13 March 2015). [Google Scholar]
- Lynam, T.; Mathevet, R.; Etienne, M.; Stone-Jovicich, S.; Leitch, A.; Jones, N.; Ross, H.; Du Toit, D.; Pollard, S.; Biggs, H.; et al. Waypoints on a journey of discovery: Mental models in human-environment interactions. Ecol. Soc. 2012, 17, 23. Available online: http://www.ecologyandsociety.org/vol17/iss3/art23/ (accessed on 13 March 2015). [Google Scholar]
- Frewer, L.J.; Fischer, A.R.H.; Brennan, M.; Bánáti, D.; Lion, R.; Meertens, R.M.; Rowe, G.; Siegrist, M.; Verbeke, W.; Vereijken, C.M.J.L. Risk/benefit communication about food—A systematic review of the literature. Crit. Rev. Food Sci. Nutr. 2013. in press. Available online: http://www.tandfonline.com/doi/abs/10.1080/10408398.2013.801337#.VQMibeG3qf5 (accessed on 13 March 2015).
- Casagrande, G.; LeJeune, J.; Belury, M.; Medeiros, L.C. Registered dietitian’s personal beliefs and characteristics predict their teaching or intention to teach fresh vegetable food safety. Appetite 2011, 56, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, L.C.; Buffer, J. Current food safety knowledge of registered dietitians. Food Protect. Trends 2012, 32, 688–696. [Google Scholar]
- Ward, B. Compensation and benefits survey 2009: Despite overall downturn in economy, RD and DTR salaries rise. J. Am. Diet. Assoc. 2010, 110, 25–36. [Google Scholar] [CrossRef] [PubMed]
- U.S. Public Health Service Food and Drug Administration. 2013; Food Code 2013 Recommendations of the United States Public Health Service Food and Drug Administration. Report number PB2013–C110462. Available online: http://www.fda.gov/downloads/Food/GuidanceRegulation/RetailFoodProtection/FoodCode/UCM374510.pdf (accessed on 6 February 2015). [Google Scholar]
- Slovic, P.; Finucane, M.L.; Peters, E.; MacGregor, D.G. Risk as analysis and risk as feelings: Some thoughts about affect, reason, risk, and rationality. Risk Anal. 2004, 24, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Peters, E.; Slovic, P.; Hibbard, J.H.; Tusler, M. Why worry? Worry, risk perceptions, and willingness to act to reduce medical errors. Health Psychol. 2006, 25, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Griffin, R.J.; Zheng, Y.; ter Huurne, E.; Boerner, F.; Ortiz, S.; Dunwoody, S. After the flood: Anger, attribution, and the seeking of information. Sci. Commun. 2008, 29, 285–315. [Google Scholar] [CrossRef]
- Dangour, A.D.; Dodhia, S.K.; Hayter, A.; Allen, E.; Lock, K.; Uauy, R. Nutritional quality of organic foods. A systematic review. Am. J. Clin. Nutr. 2009, 90, 680–685. [Google Scholar] [CrossRef] [PubMed]
- Griffin, R.J.; Neuwirth, K.; Giese, J.; Dunwoody, S. Linking the heuristic-systematic model and depth of processing. Commun. Res. 2002, 29, 705–732. [Google Scholar] [CrossRef]
- Griffin, R.; Neuwirth, K.; Dunwoody, S.; Giese, J. Information sufficiency and risk communication. Media Psychol. 2004, 6, 23–61. [Google Scholar] [CrossRef]
- Medeiros, L.; Hillers, V.; Chen, G.; Bergmann, V.; Kendall, P.; Schroeder, M. Design and development of food safety knowledge and attitude scales for consumer food safety education. J. Am. Diet. Assoc. 2004, 104, 1671–1677. [Google Scholar] [CrossRef] [PubMed]
- Kendall, P.; Elsbernd, A.; Sinclair, K.; Schroeder, M.; Chen, G.; Bergman, V.; Hillers, V.; Medeiros, L. Observation versus self-report: Validation of a consumer food behavior questionnaire. J. Food Protect. 2004, 67, 2578–2586. [Google Scholar]
- Parmenter, K.; Wardle, J. Evaluation and design of nutrition knowledge measures. J. Nutr. Educ. Behav. 2000, 32, 269–277. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Medeiros, L.C.; LeJeune, J.T. Food Safety Information Processing and Teaching Behavior of Dietitians: A Mental Model Approach. Agriculture 2015, 5, 132-154. https://doi.org/10.3390/agriculture5010132
Medeiros LC, LeJeune JT. Food Safety Information Processing and Teaching Behavior of Dietitians: A Mental Model Approach. Agriculture. 2015; 5(1):132-154. https://doi.org/10.3390/agriculture5010132
Chicago/Turabian StyleMedeiros, Lydia C., and Jeffrey T. LeJeune. 2015. "Food Safety Information Processing and Teaching Behavior of Dietitians: A Mental Model Approach" Agriculture 5, no. 1: 132-154. https://doi.org/10.3390/agriculture5010132