Left Atrial Strain to Identify Diastolic Dysfunction in Children with Cardiomyopathies

 , ,
, ,
Abstract
:1. Background
2. Methods
2.1. Study Population
2.2. Standard Echocardiography
2.3. Two-Dimensional Speckle-Tracking Analysis
2.4. Cardiac Catheterization
2.5. Reproducibility Study
2.6. Statistical Analysis
3. Results
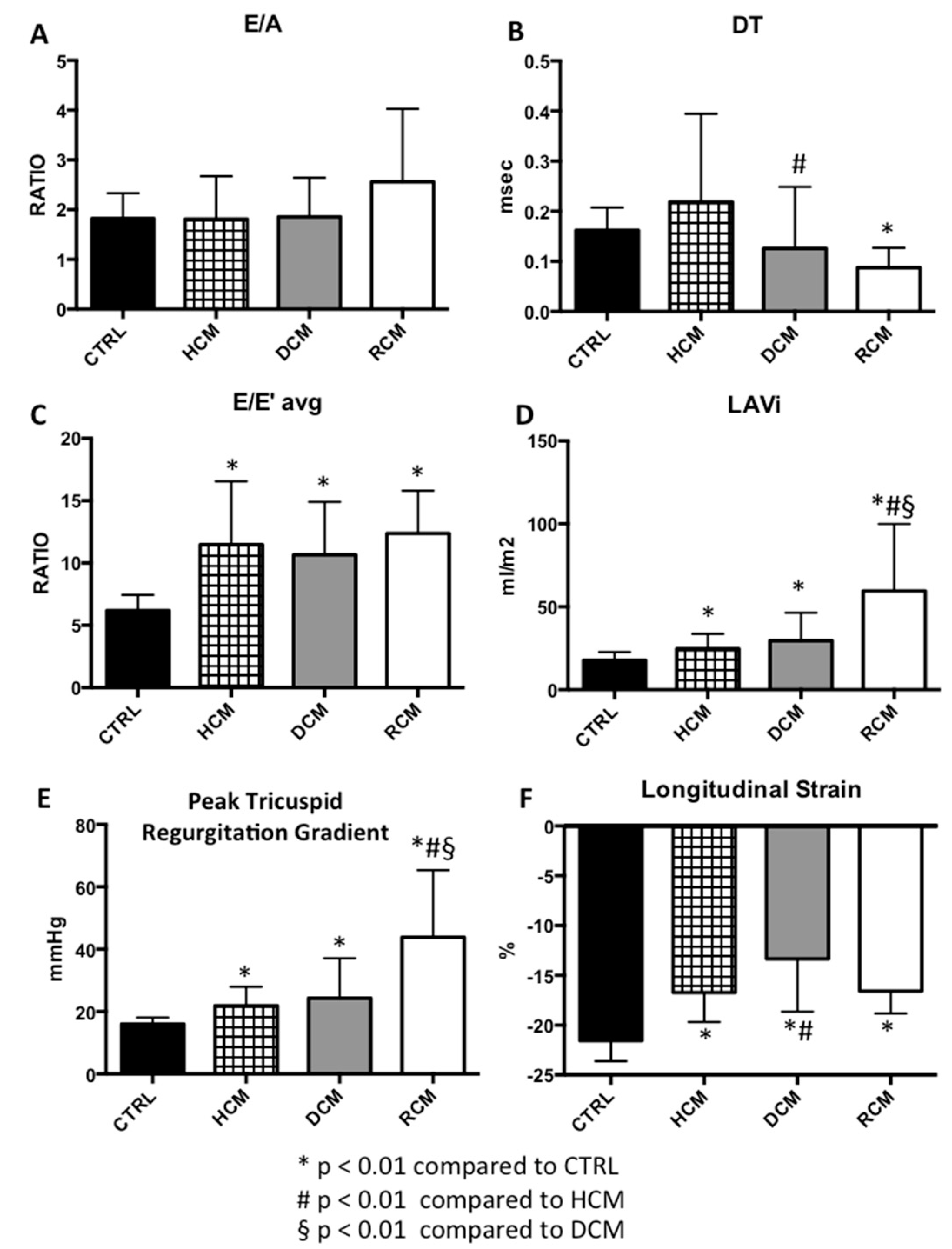
3.1. Traditional Diastolic Parameters
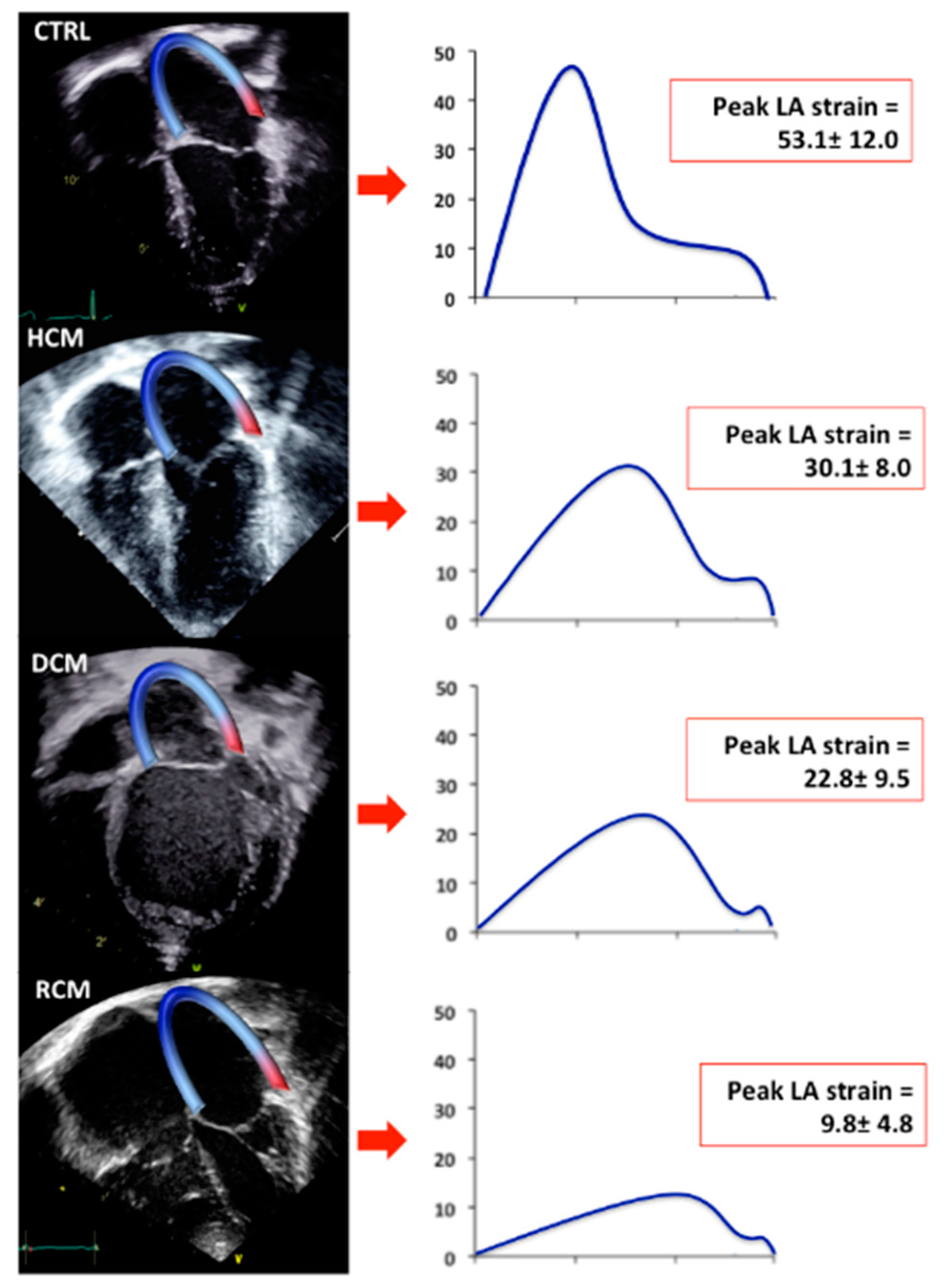
3.2. Longitudinal Strain Analyses
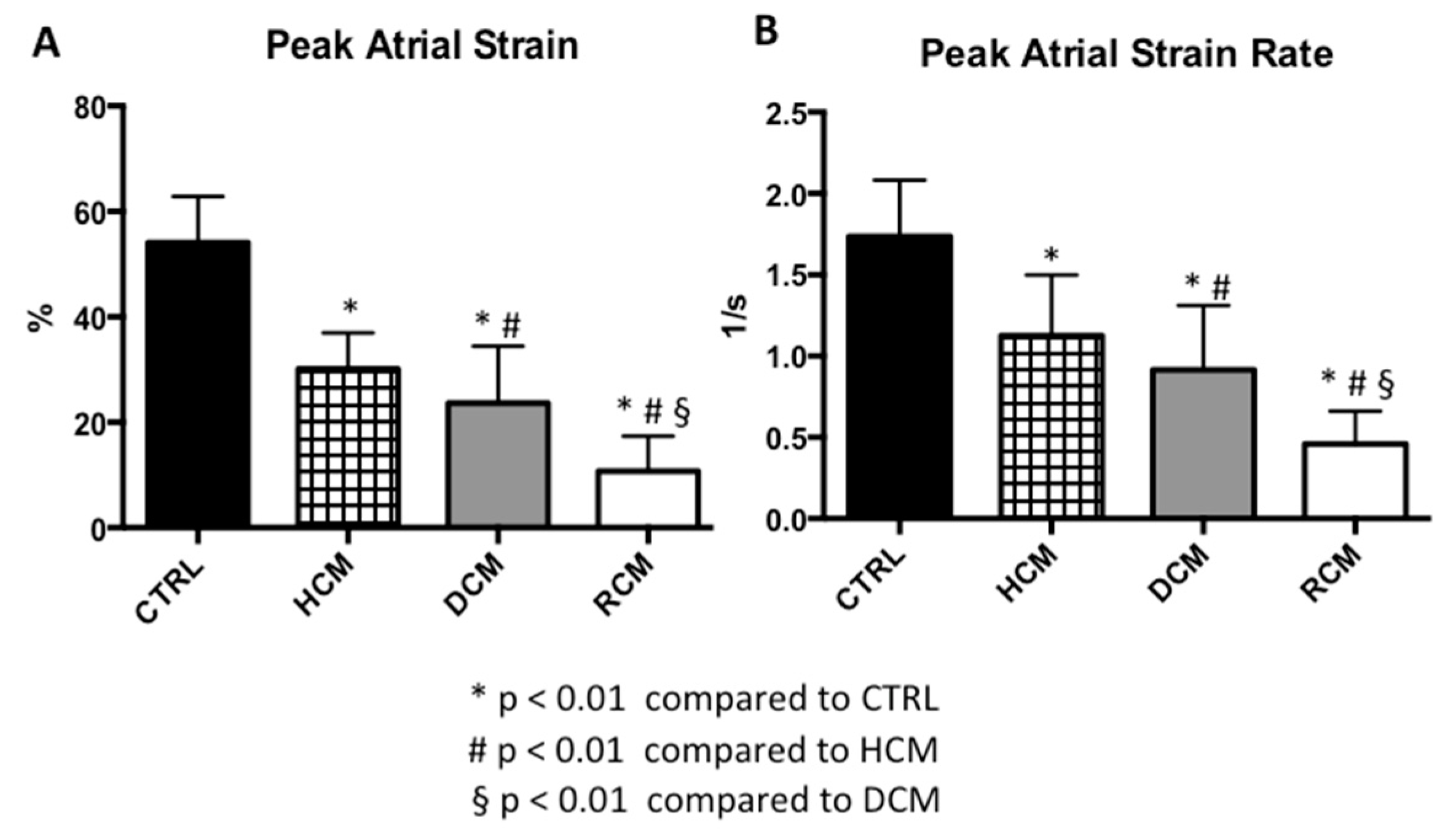
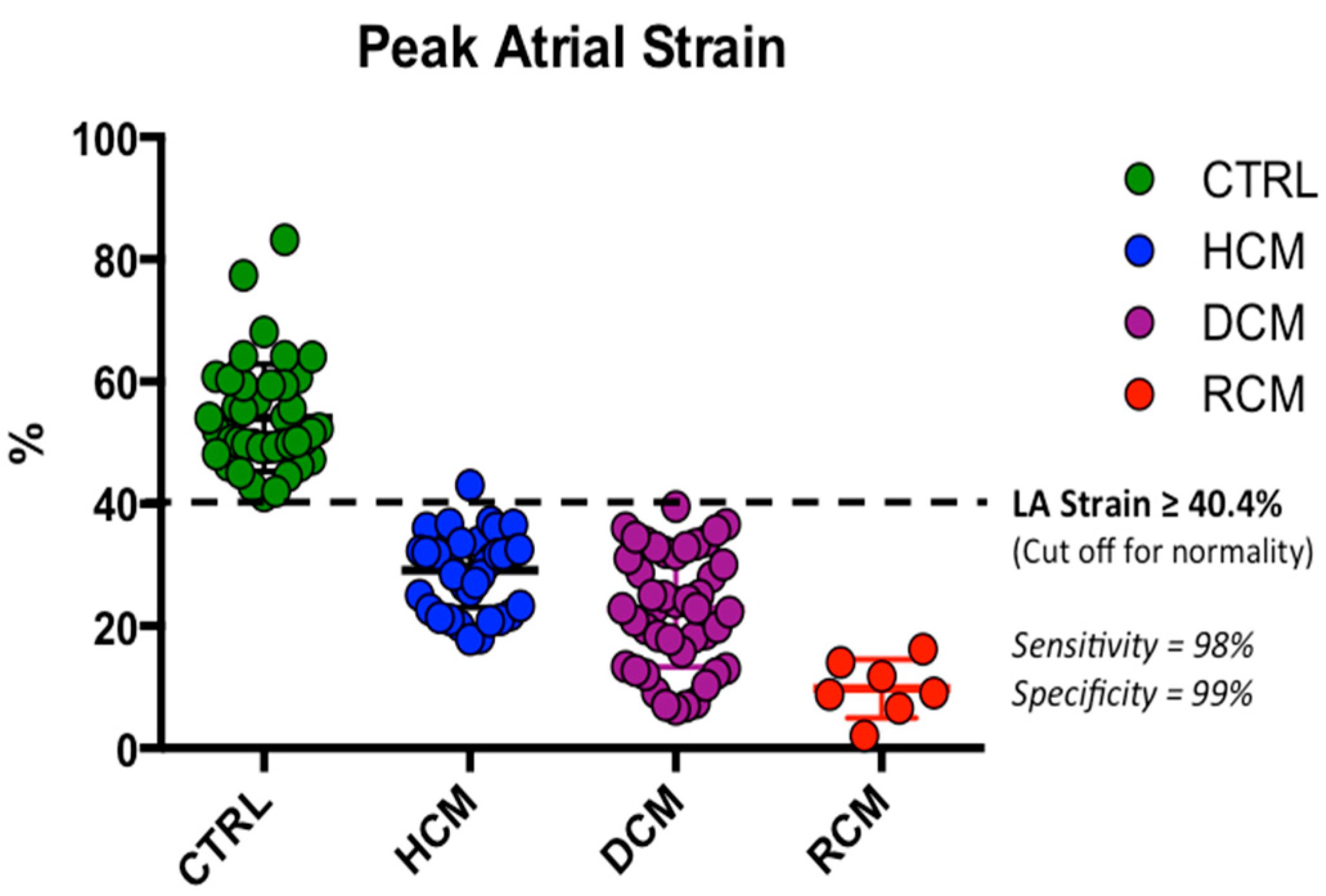
3.3. Atrial Strain Parameters
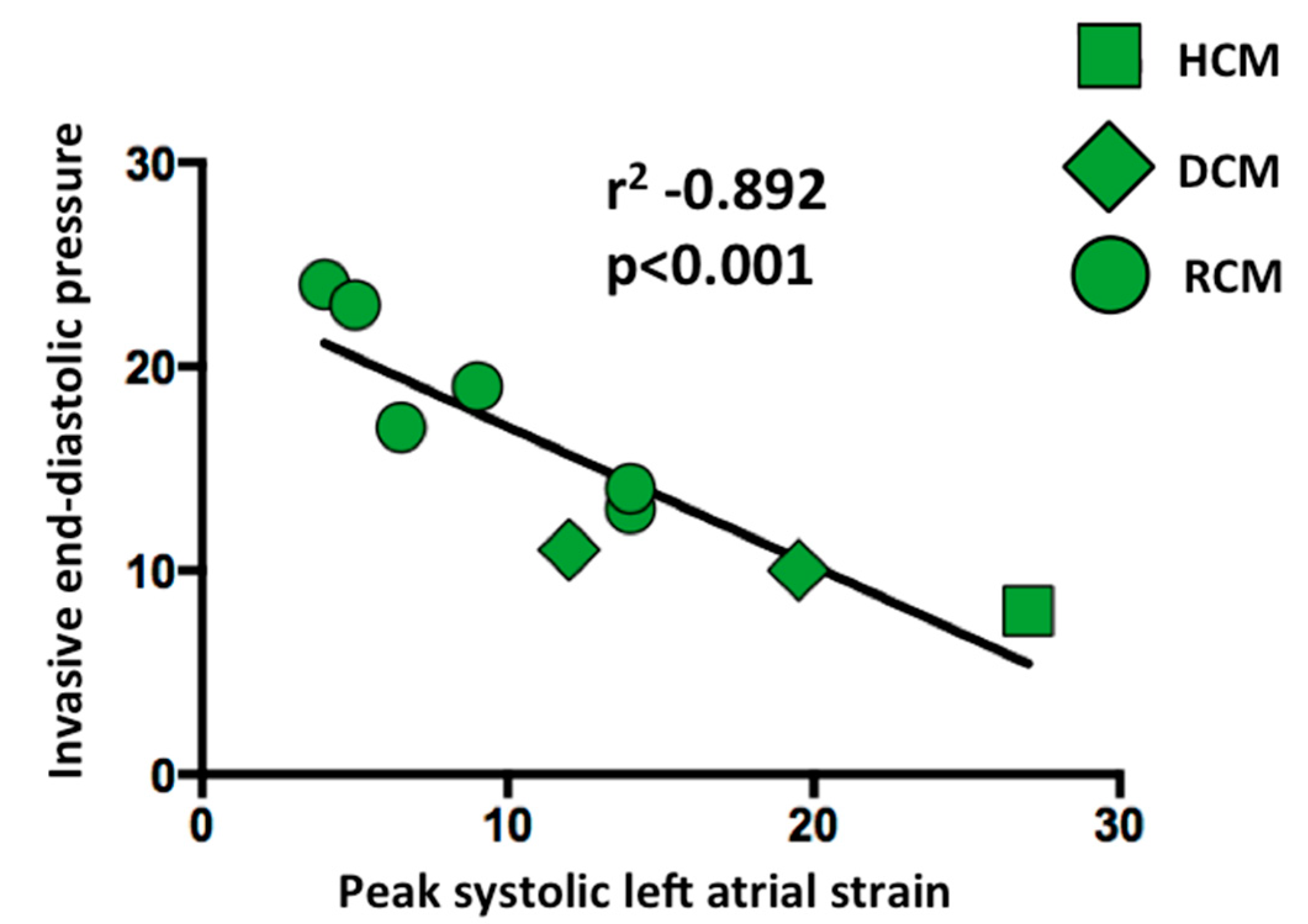
3.4. Left Atrial Strain Correlation with Invasive End-Diastolic Pressures
3.5. Reproducibility Analyses
4. Discussion
4.1. Left Atrial Strain and Standard Echo Doppler
4.2. Left Atrial Strain and Progressive Diastolic Dysfunction
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Alexander, P.M.; Daubeney, P.E.; Nugent, A.W.; Lee, K.J.; Turner, C.; Colan, S.D.; Robertson, T.; Davis, A.M.; Ramsay, J.; Justo, R.; et al. National Australian Childhood Cardiomyopathy Study. Long-term outcomes of dilated cardiomyopathy diagnosed during childhood: Results from a national population-based study of childhood cardiomyopathy. Circulation 2013, 128, 2039–2046. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, J.A.; Orav, E.J.; Wilkinson, J.D.; Fleming, L.E.; Lee, D.J.; Sleeper, L.A.; Rusconi, P.G.; Colan, S.D.; Hsu, D.T.; Canter, C.E.; et al. Pediatric Cardiomyopathy Registry Investigators. Competing risks for death and cardiac transplantation in children with dilated cardiomyopathy: Results from the pediatric cardiomyopathy registry. Circulation 2011, 124, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Friedberg, M.K.; Roche, S.L.; Mohammed, A.F.; Balasingam, M.; Atenafu, E.G.; Kantor, P.F. Left ventricular diastolic mechanical dyssynchrony and associated clinical outcomes in children with dilated cardiomyopathy. Circ. Cardiovasc. Imaging 2008, 1, 50–57. [Google Scholar] [CrossRef] [PubMed]
- McMahon, C.J.; Nagueh, S.F.; Pignatelli, R.H.; Denfield, S.W.; Dreyer, W.J.; Price, J.F.; Clunie, S.; Bezold, L.I.; Hays, A.L.; Towbin, J.A.; et al. Characterization of left ventricular diastolic function by tissue Doppler imaging and clinical status in children with hypertrophic cardiomyopathy. Circulation 2004, 109, 1756–1762. [Google Scholar] [CrossRef] [PubMed]
- McMahon, C.J.; Nagueh, S.F.; Eapen, R.S.; Dreyer, W.J.; Finkelshtyn, I.; Cao, X.; Eidem, B.W.; Bezold, L.I.; Denfield, S.W.; Towbin, J.A.; et al. Echocardiographic predictors of adverse clinical events in children with dilated cardiomyopathy: A prospective clinical study. Heart 2004, 90, 908–915. [Google Scholar] [CrossRef] [PubMed]
- McMahon, C.J.; Pignatelli, R.H.; Nagueh, S.F.; Lee, V.V.; Vaughn, W.; Valdes, S.O.; Kovalchin, J.P.; Jefferies, J.L.; Dreyer, W.J.; Denfield, S.W.; et al. Left ventricular non-compaction cardiomyopathy in children: Characterisation of clinical status using tissue Doppler-derived indices of left ventricular diastolic relaxation. Heart 2007, 93, 676–681. [Google Scholar] [CrossRef]
- Ouzounian, M.; Lee, D.S.; Liu, P.P. Diastolic heart failure: Mechanisms and controversies. Nat. Clin. Pr. Cardiovasc. Med. 2008, 5, 375–386. [Google Scholar] [CrossRef]
- Dragulescu, A.; Mertens, L.; Friedberg, M.K. Interpretation of left ventricular diastolic dysfunction in children with cardiomyopathy by echocardiography. Circ. Cardiovasc. Imaging 2013, 6, 254–261. [Google Scholar] [CrossRef]
- Russo, C.; Jin, Z.; Homma, S.; Rundek, T.; Elkind, M.S.; Sacco, R.L.; Di Tullio, M.R. Left atrial minimum volume and reservoir function as correlates of left ventricular diastolic function: Impact of left ventricular systolic function. Heart 2012, 98, 813–820. [Google Scholar] [CrossRef]
- Cameli, M.; Caputo, M.; Mondillo, S.; Ballo, P.; Palmerini, E.; Lisi, M.; Marino, E.; Galderisi, M. Feasibility and reference values of left atrial longitudinal strain imaging by two-dimensional speckle tracking. Cardiovasc. Ultrasound 2009, 7, 6. [Google Scholar] [CrossRef]
- Saraiva, R.M.; Demirkol, S.; Buakhamsri, A.; Greenberg, N.; Popović, Z.B.; Thomas, J.D.; Klein, A.L. Left atrial strain measured by two-dimensional speckle tracking represents a new tool to evaluate left atrial function. J. Am. Soc. Echocardiogr. 2010, 23, 172–180. [Google Scholar] [CrossRef] [PubMed]
- D’Alto, M.; D’Andrea, A.; Di Salvo, G.; Scognamiglio, G.; Argiento, P.; Romeo, E.; Di Marco, G.M.; Mattera Iacono, A.; Bossone, E.; Sarubbi, B.; et al. Right atrial function and prognosis in idiopathic pulmonary arterial hypertension. Int. J. Cardiol. 2017, 248, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Di Salvo, G.; Pacileo, G.; Castaldi, B.; Gala, S.; Morelli, C.; D’Andrea, A.; Limongelli, G.; Del Gaizo, F.; Merlino, E.; Russo, M.G.; et al. Two-dimensional strain and atrial function: A study on patients after percutaneous closure of atrial septal defect. Eur. J. Echocardiogr. 2009, 10, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Di Salvo, G.; Pacileo, G.; Del Giudice, E.M.; Natale, F.; Limongelli, G.; Verrengia, M.; Rea, A.; Fratta, F.; Castaldi, B.; Gala, S.; et al. Atrial myocardial deformation properties in obese nonhypertensive children. J. Am. Soc. Echocardiogr. 2008, 21, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Vianna-Pinton, R.; Moreno, C.A.; Baxter, C.M.; Lee, K.S.; Tsang, T.S.; Appleton, C.P. Two-dimensional speckle-tracking echocardiography of the left atrium: Feasibility and regional contraction and relaxation differences in normal subjects. J. Am. Soc. Echocardiogr. 2009, 22, 299–305. [Google Scholar] [CrossRef]
- Mondillo, S.; Cameli, M.; Caputo, M.L.; Lisi, M.; Palmerini, E.; Padeletti, M.; Ballo, P. Early detection of left atrial strain abnormalities by speckle-tracking in hypertensive and diabetic patients with normal left atrial size. J. Am. Soc. Echocardiogr. 2011, 24, 898–908. [Google Scholar] [CrossRef]
- Singh, A.; Addetia, K.; Maffessanti, F.; Mor-Avi, V.; Lang, R.M. LA Strain Categorization of LV diastolic dysfunction. JACC Cardiovasc. Imaging 2017, 10, 735–743. [Google Scholar] [CrossRef]
- Telagh, R.; Hui, W.; Abd El Rahman, M.; Berger, F.; Lange, P.E.; Abdul-Khaliq, H. Assessment of regional atrial function in patients with hypertrophic cardiomyopathies using tissue Doppler imaging. Pediatr. Cardiol. 2008, 29, 301–308. [Google Scholar] [CrossRef]
- Gersh, B.J.; Maron, B.J.; Bonow, R.O.; Dearani, J.A.; Fifer, M.A.; Link, M.S.; Naidu, S.S.; Nishimura, R.A.; Ommen, S.R.; Rakowski, H.; et al. accf/aha guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: A report of the american college of cardiology foundation/american heart association task force on practice guidelines. J. Thorac. Cardiovasc. Surg. 2011, 142, e153–e203. [Google Scholar] [CrossRef]
- Matitiau, A.; Perez-Atayde, A.; Sanders, S.P.; Sluysmans, T.; Parness, I.A.; Spevak, P.J.; Colan, S.D. Infantile dilated cardiomyopathy. Relation of outcome to left ventricular mechanics, hemodynamics, and histology at the time of presentation. Circulation 1994, 90, 1310–1318. [Google Scholar] [CrossRef]
- Ammash, N.M.; Seward, J.B.; Bailey, K.R.; Edwards, W.D.; Tajik, A.J. Clinical profile and outcome of idiopathic restrictive cardiomyopathy. Circulation 2000, 101, 2490–2496. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Lai, W.W.; Cohen, M.S.; Geva, T.; Mertens, L. Echocardiography in Pediatric and Congenital Heart Disease; Wiley-Blackwell: West Sussex, UK, 2009; Appendix 1; pp. 765–785. [Google Scholar]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., III; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [PubMed]
- Ancona, R.; Comenale Pinto, S.; Caso, P.; Di Salvo, G.; Severino, S.; D’Andrea, A.; Calabrò, R. Two-dimensional atrial systolic strain imaging predicts atrial fibrillation at 4-year follow-up in asymptomatic rheumatic mitral stenosis. J. Am. Soc. Echocardiogr. 2013, 26, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Di Salvo, G.; D’Aiello, A.F.; Castaldi, B.; Fadel, B.; Limongelli, G.; D’Andrea, A.; Pergola, V.; Pacileo, G.; Del Giudice, E.M.; Perrone, L.; et al. Early left ventricular abnormalities in children with heterozygous familial hypercholesterolemia. J. Am. Soc. Echocardiogr. 2012, 25, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- McNeil, B.J.; Hanley, J.A. Statistical approaches to the analysis of receiver operating characteristic (ROC) curves. Med. Decis. Mak. 1984, 4, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Iida, M.; Yamamoto, M.; Ishiguro, Y.; Honjo, H.; Kamiya, K. Association of tricuspid regurgitation within normal range on the development of left ventricular diastolic dysfunction in patients with uncomplicated hypertension. Blood Press 2018, 27, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Kurt, M.; Wang, J.; Torre-Amione, G.; Nagueh, S.F. Left atrial function in diastolic heart failure. Circ. Cardiovasc. Imaging 2009, 2, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Cameli, M.; Sparla, S.; Losito, M.; Righini, F.M.; Menci, D.; Lisi, M.; D’Ascenzi, F.; Focardi, M.; Favilli, R.; Pierli, C.; et al. Correlation of left atrial strain and doppler measurements with invasive measurement of left ventricular end-diastolic pressure in patients stratified for different values of ejection fraction. Echocardiography 2016, 33, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Wakami, K.; Ohte, N.; Asada, K.; Fukuta, H.; Goto, T.; Mukai, S.; Narita, H.; Kimura, G. Correlation between left ventricular end-diastolic pressure and peak left atrial wall strain during left ventricular systole. J. Am. Soc. Echocardiogr. 2009, 22, 847–851. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | ||||
|---|---|---|---|---|
| General and Echocardiographic Variables | CTRL (N = 45) | HCM (N = 40) | DCM (N = 44) | RCM (N = 7) |
| Age (years) | 10.4 (4.7) | 10.9 (5.5) | 5.0 (5.2) | 10.0 (7.0) |
| Male, n (%) | 18 (40) | 24 (61) | 21 (48) | 3 (43) |
| Body Surface Area (BSA) (m2) | 1.2 (0.5) | 1.3 (0.5) | 0.8 (0.5) | 1.1 (0.6) |
| Mean Heart Rate (bpm) | 85 (15) | 71 (22) | 115 (18) | 95 (18) |
| LVEDD (mm) | 39.6 (7) | 34.5 (8) * | 44.5 (10) # | 35.3 (9) |
| LVEDD Z score | −0.5 (0.8) | −1.7 (0.5) * | 3.5 (0.2) *,# | −1.1 (0.4) § |
| IVS (mm) | 6.1 (1) | 13.5 (5) * | 5.1 (2) *,# | 7.1 (2) # |
| IVS Z score | −0.4 (0.7) | 3.1 (0.2) * | -0.9 (0.9) # | 1.2 (0.7) § |
| LVEF (%) | 60 (4) | 68 (7) * | 39 (12) *,# | 59 (8) #,§ |
| Groups | ||||
|---|---|---|---|---|
| Diastolic Parameters | CTRL (N = 45) | HCM (N = 40) | DCM (N = 44) | RCM (N = 7) |
| MV E vel (cm/sec) | 90.2 (13.8) | 95.6 (19.9) | 98.4 (25.8) | 80.0 (33.0) |
| MV A vel (cm/sec) | 53.2 (14.7) | 59.2 (20.3) | 58.0 (20.1) | 34.8 (20.3) |
| MV E/A (ratio) | 1.8 (0.5) | 1.8 (0.9) | 1.8 (0.8) | 2.5 (1.5) |
| MV DT (msec) | 162 (45.8) | 219 (175.7) | 125 (123) # | 87 (40) * |
| MV E’ sep (cm/sec) | 13.6 (2.0) | 8.3 (3.0) * | 9.3 (2.8) * | 6.2 (1.8) *,§ |
| MV E’ lat (cm/sec) | 16.8 (3.4) | 11.2 (4.1) * | 11.3 (4.1) * | 8.0 (4.1) * |
| MV E/E’ avg | 6.2 (1.2) | 11.5 (5.5) * | 10.7 (4.2) * | 12.4 (3.4) * |
| LAVi (mL/m2) | 17.7 (4.9) | 24.6 (9.0) * | 29.6 (16.8) * | 59.6 (40.3) *,#,§ |
| PTRG (mmHg) | 16.1 (2.0) | 21.9 (6.1) * | 24.3 (12.8) * | 43.8 (21.5) *,#,§ |
| PV S/D | 1.0 (0.3) | 1.3 (0.3) | 1.0 (0.3) | 1.4 (0.7) |
| Atrial and ventricular strain parameters | ||||
| LV LS (%) | −21.5 (2.1) | −16.7 (3.0) * | −13.3 (5.3) *,# | −16.6 (2.3) * |
| LA peak systolic strain (%) | 53.1 (12.0) | 30.1 (8.0) * | 22.8 (9.5) *,# | 9.8 (4.8) *,#,§ |
| LA peak systolic strain rate (1/s) | 1.7 (0.3) | 1.1 (0.3) * | 0.9 (0.4) *,# | 0.4 (0.2) *,#,§ |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sabatino, J.; Di Salvo, G.; Prota, C.; Bucciarelli, V.; Josen, M.; Paredes, J.; Borrelli, N.; Sirico, D.; Prasad, S.; Indolfi, C.; et al. Left Atrial Strain to Identify Diastolic Dysfunction in Children with Cardiomyopathies. J. Clin. Med. 2019, 8, 1243. https://doi.org/10.3390/jcm8081243
Sabatino J, Di Salvo G, Prota C, Bucciarelli V, Josen M, Paredes J, Borrelli N, Sirico D, Prasad S, Indolfi C, et al. Left Atrial Strain to Identify Diastolic Dysfunction in Children with Cardiomyopathies. Journal of Clinical Medicine. 2019; 8(8):1243. https://doi.org/10.3390/jcm8081243
Chicago/Turabian StyleSabatino, Jolanda, Giovanni Di Salvo, Costantina Prota, Valentina Bucciarelli, Manjit Josen, Josefa Paredes, Nunzia Borrelli, Domenico Sirico, Sanjay Prasad, Ciro Indolfi, and et al. 2019. "Left Atrial Strain to Identify Diastolic Dysfunction in Children with Cardiomyopathies" Journal of Clinical Medicine 8, no. 8: 1243. https://doi.org/10.3390/jcm8081243