Multidisciplinary Management of Neuroendocrine Neoplasia: A Real-World Experience from a Referral Center

 , , and
, , and 
Abstract
:1. Introduction
2. Patients and Methods
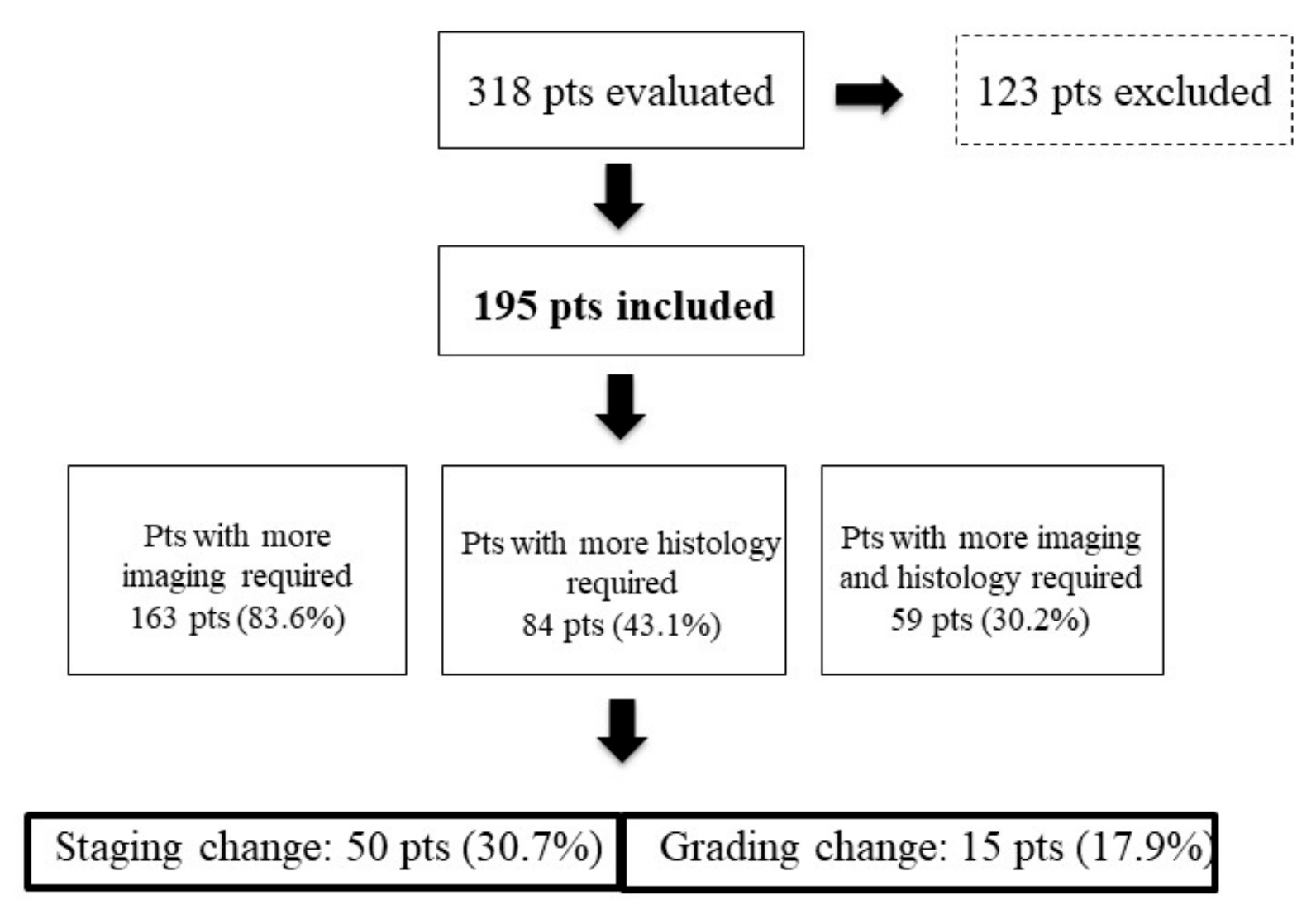
3. Results
Patients’ Management
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Caplin, M.E.; Baudin, E.; Ferolla, P.; Filosso, P.; Garcia-Yuste, M.; Lim, E.; Oberg, K.; Pelosi, G.; Perren, A.; Rossi, R.E.; et al. Pulmonary neuroendocrine (carcinoid) tumors: European Neuroendocrine Tumor Society expert consensus and recommendations for best practice for typical and atypical pulmonary carcinoids. Ann. Oncol. 2015, 26, 1604–1620. [Google Scholar] [CrossRef] [PubMed]
- Panzuto, F.; Merola, E.; Pavel, M.E.; Rinke, A.; Kump, P.; Partelli, S.; Rinzivillo, M.; Rodriguez-Laval, V.; Pape, U.F.; Lipp, R.; et al. Stage IV Gastro-Entero-Pancreatic Neuroendocrine Neoplasms: A Risk Score to Predict Clinical Outcome. Oncologist 2017, 22, 409–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rindi, G.; Klersy, C.; Albarello, L.; Baudin, E.; Bianchi, A.; Buchler, M.W.; Caplin, M.; Couvelard, A.; Cros, J.; de Herder, W.W.; et al. Competitive Testing of the WHO 2010 versus the WHO 2017 Grading of Pancreatic Neuroendocrine Neoplasms: Data from a Large International Cohort Study. Neuroendocrinology 2018, 107, 375–386. [Google Scholar] [CrossRef]
- Strosberg, J. Gastroenteropancreatic Neuroendocrine Tumors. CA Cancer J. Clin. 2018, 68, 552–570. [Google Scholar]
- Bulens, P.; Thomas, M.; Deroose, C.M.; Haustermans, K. PET imaging in adaptive radiotherapy of gastrointestinal tumors. Q. J. Nucl. Med. Mol. Imaging 2018, 62, 385–403. [Google Scholar] [CrossRef] [PubMed]
- Opalinska, M.; Hubalewska-Dydejczyk, A.; Sowa-Staszczak, A. Radiolabeled peptides: Current and new perspectives. Q. J. Nucl. Med. Mol. Imaging 2017, 61, 153–167. [Google Scholar] [PubMed]
- Zeelen, C.; Paus, C.; Draper, D.; Heskamp, S.; Signore, A.; Galli, F.; Griessinger, C.M.; Aarntzen., E.H. In-vivo imaging of tumor-infiltrating immune cells: Implications for cancer immunotherapy. Q. J. Nucl. Med. Mol. Imaging 2018, 62, 56–77. [Google Scholar] [PubMed]
- Kunz, P.L.; Reidy-Lagunes, D.; Anthony, L.B.; Bertino, E.M.; Brendtro, K.; Chan, J.A.; Chen, H.; Jensen, R.T.; Kim, M.K.; Klimstra, D.S.; et al. Consensus Guidelines for the Management and Treatment of Neuroendocrine Tumors. Pancreas 2013, 42, 557–577. [Google Scholar] [CrossRef] [Green Version]
- De Herder, W.W.; Capdevila, J. Unmet Needs in the Field of Neuroendocrine Neoplasms of the Gastrointestinal Tract, Pancreas, and Respiratory System: Reports by the ENETS Group. Neuroendocrinology 2019, 108, 5–6. [Google Scholar] [CrossRef]
- Forrest, L.M.; McMillan, D.C.; McArdle, C.S.; Dunlop, D.J. An evaluation of the impact of a multidisciplinary team, in a single centre, on treatment and survival in patients with inoperable non-small-cell lung cancer. Br. J. Cancer 2005, 93, 977–978. [Google Scholar] [CrossRef] [Green Version]
- Wright, F.; De Vito, C.; Langer, B.; Hunter, A. Multidisciplinary cancer conferences: A systematic review and development of practice standards. Eur. J. Cancer 2007, 43, 1002–1010. [Google Scholar] [CrossRef] [PubMed]
- Keating, N.L.; Landrum, M.B.; Lamont, E.B.; Bozeman, S.R.; Shulman, L.N.; McNeil, B.J. Tumor Boards and the Quality of Cancer Care. J. Natl. Cancer Inst. 2013, 105, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Bosman, F.T.; Carneiro, F.; Hruban, R.H.; Theise, N.D. WHO Classification of Tumours of the Digestive System, 4th ed.; WHO Press: Geneva, Switzerland, 2010. [Google Scholar]
- Lloyd, R.V.; Osamura, R.; Kloppel, G.; Rosai, J. WHO Classification of Tumours of Endocrine Organs, 4th ed.; IARC Press: Lyon, France, 2017. [Google Scholar]
- Travis, W.D.; Brambilla, E.; Muller-Hermelink, H.; Harris, C.C. Tumours of the Lung, Pleura, Thymus and Heart; IARC Press: Lyon, France, 2004. [Google Scholar]
- Rindi, G.; Klöppel, G.; Alhman, H.; Caplin, M.; Couvelard, A.; De Herder, W.W.; Erikssson, B.; Falchetti, A.; Falconi, M.; Komminoth, P.; et al. TNM staging of foregut (neuro)endocrine tumors: A consensus proposal including a grading system. Virchows Archiv 2006, 449, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Rindi, G.; Klöppel, G.; Couvelard, A.; Komminoth, P.; Körner, M.; Lopes, J.M.; McNicol, A.-M.; Nilsson, O.; Perren, A.; Scarpa, A.; et al. TNM staging of midgut and hindgut (neuro) endocrine tumors: A consensus proposal including a grading system. Virchows Archiv 2007, 451, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Perren, A.; Couvelard, A.; Scoazec, J.-Y.; Costa, F.; Borbath, I.; Fave, G.D.; Gorbounova, V.; Gross, D.; Grossman, A.; Jensen, R.T.; et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors: Pathology - Diagnosis and Prognostic Stratification. Neuroendocrinology 2017, 105, 196–200. [Google Scholar] [CrossRef]
- Knigge, U.; Capdevila, J.; Bartsch, D.K.; Baudin, E.; Falkerby, J.; Kianmanesh, R.; Kos-Kudla, B.; Niederle, B.; Nieveen van Dijkum, E.; O’Toole, D.; et al. ENETS Consensus Recommendations for the Standards of Care in Neuroendocrine Neoplasms: Follow-Up and Documentation. Neuroendocrinology 2017, 105, 310–319. [Google Scholar] [CrossRef] [Green Version]
- Metz, D.C.; Choi, J.; Strosberg, J.; Heaney, A.P.; Howden, C.W.; Klimstra, D.; Yao, J.C. A rationale for multidisciplinary care in treating neuroendocrine tumours. Curr. Opin. Endocrinol. Diabetes Obes. 2012, 19, 306–313. [Google Scholar] [CrossRef]
- Singh, S.; Law, C. Multidisciplinary Reference Centers: The Care of Neuroendocrine Tumors. J. Oncol. Pr. 2010, 6, e11–e16. [Google Scholar] [CrossRef] [Green Version]
- Fazio, N.; Ungaro, A.; Spada, F.; Cella, C.A.; Pisa, E.; Barberis, M.; Grana, C.; Zerini, D.; Bertani, E.; Ribero, D.; et al. The role of multimodal treatment in patients with advanced lung neuroendocrine tumors. J. Thorac. Dis. 2017, 9, S1501–S1510. [Google Scholar] [CrossRef] [Green Version]
- Pape, U.F.; Böhmig, M.; Berndt, U.; Tiling, N.; Wiedenmann, B.; Plöckinger, U. Survival and clinical outcome of patients with neuroendocrine tumors of the gastroenteropancreatic tract in a german referral center. Ann. N. Y. Acad. Sci. 2004, 1014, 222–233. [Google Scholar] [CrossRef]
- Panzuto, F.; Nasoni, S.; Falconi, M.; Corleto, V.D.; Capurso, G.; Cassetta, S.; Di Fonzo, M.; Tornatore, V.; Milione, M.; Angeletti, S.; et al. Prognostic factors and survival in endocrine tumor patients: Comparison between gastrointestinal and pancreatic localization. Endocr. Relat. Cancer 2005, 12, 1083–1092. [Google Scholar] [CrossRef] [PubMed]
- Basuroy, R.; Bouvier, C.; Ramage, J.K.; Sissons, M.; Kent, A.; Srirajaskanthan, R. Presenting Symptoms and Delay in Diagnosis of Gastrointestinal and Pancreatic Neuroendocrine Tumours. Neuroendocrinology 2018, 107, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Pezzilli, R.; Partelli, S.; Cannizzaro, R.; Pagano, N.; Crippa, S.; Pagnanelli, M.; Falconi, M. Ki-67 prognostic and therapeutic decision driven marker for pancreatic neuroendocrine neoplasms (PNENs): A systematic review. Adv. Med. Sci. 2016, 61, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Lin, E.; Chen, T.; Little, A.; Holliday, L.; Roach, P.; Butler, P.; Hosking, E.; Bailey, E.; Elison, B.; Currow, D. Safety and outcomes of 177 Lu-DOTATATE for neuroendocrine tumours: Experience in New South Wales, Australia. Intern. Med. J. 2019. [Google Scholar] [CrossRef] [PubMed]
- Parghane, R.V.; Talole, S.; Basu, S. Prevalence of hitherto unknown brain meningioma detected on 68Ga-DOTATATE positron-emission tomography/computed tomography in patients with metastatic neuroendocrine tumor and exploring potential of 177Lu-DOTATATE peptide receptor radionuclide therapy as single-shot treatment approach targeting both tumors. World J. Nucl. Med. 2019, 18, 160–170. [Google Scholar] [PubMed]
- Rindi, G.; Bordi, C.; La Rosa, S.; Solcia, E.; Fave, G.D. Gastroenteropancreatic (neuro)endocrine neoplasms: The histology report. Dig. Liver Dis. 2011, 43, S356–S360. [Google Scholar] [CrossRef]
- Singh, S.; Hallet, J.; Rowsell, C.; Law, C. Variability of Ki67 labeling index in multiple neuroendocrine tumors specimens over the course of the disease. Eur. J. Surg. Oncol. (EJSO) 2014, 40, 1517–1522. [Google Scholar] [CrossRef]
- Panzuto, F.; Cicchese, N.; Partelli, S.; Rinzivillo, M.; Capurso, G.; Merola, E.; Manzoni, M.; Pucci, E.; Iannicelli, E.; Pilozzi, E.; et al. Impact of Ki67 re-assessment at time of disease progression in patients with pancreatic neuroendocrine neoplasms. PLoS ONE 2017, 12, e0179445. [Google Scholar] [CrossRef]
- Singh, S.; Poon, R.; Wong, R.; Metser, U. 68Ga PET Imaging in Patients With Neuroendocrine Tumors: A Systematic Review and Meta-analysis. Clin. Nucl. Med. 2018, 43, 802–810. [Google Scholar] [CrossRef]
- Merola, E.; Pavel, M.E.; Panzuto, F.; Capurso, G.; Cicchese, N.; Rinke, A.; Gress, T.M.; Iannicelli, E.; Prosperi, D.; Pizzichini, P.; et al. Functional Imaging in the Follow-Up of Enteropancreatic Neuroendocrine Tumors: Clinical Usefulness and Indications. J. Clin. Endocrinol. Metab. 2017, 102, 1486–1494. [Google Scholar] [CrossRef]
- Panzuto, F.; Merola, E.; Rinzivillo, M.; Partelli, S.; Campana, D.; Iannicelli, E.; Pilozzi, E.; Mercantini, P.; Rossi, M.; Capurso, G.; et al. Advanced digestive neuroendocrine tumors: Metastatic pattern is an independent factor affecting clinical outcome. Pancreas 2014, 43, 212–218. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Overall n = 195 | Newly Diagnosed n = 48 | Referred n = 147 | p-Value | |
|---|---|---|---|---|
| Primary site | ||||
| Pancreas | 75 (38.5%) | 22 (45.8%) | 53 (36%) | 0.642 |
| Small bowel | 43 (22.1%) | 10 (20.8%) | 33 (22.4%) | |
| Rectum | 10 (5.1%) | 2 (4.2%) | 8 (5.4%) | |
| Appendix | 9 (4.6%) | 2 (4.2%) | 7 (4.7%) | |
| Lung | 19 (9.7%) | 6 (12.5%) | 13 (8.8%) | |
| Other | 39 (20%) | 6 (12.5%) | 33 (22.4%) | |
| Grading | ||||
| G1 | 88 (45.1%) | 22 (45.8%) | 66 (44.9%) | 0.053 |
| G2 | 80 (41%) | 18 (37.5%) | 62 (42.2%) | |
| G3 | 27 (13.9%) | 8 (16.7%) | 19 (12.9%) | |
| Median Ki67 (IQR, range) | 3% (2–9, 1–90) | 2% (2–5, 1–40) | 3% (2–10, 1–90) | 0.212 |
| Staging | ||||
| Stage 1 | 42 (21.5%) | 13 (27.1%) | 29 (19.7%) | 0.080 |
| Stage 2 | 27 (13.9%) | 6 (12.5%) | 21 (14.3%) | |
| Stage 3 | 38 (19.5%) | 8 (16.7% | 30 (20.4%) | |
| Stage 4 | 88 (45.1%) | 21 (43.7%) | 67 (45.6%) |
| Before MDT * | After MDT | |
|---|---|---|
| Somatostatin analogs | 23 (11.8%) | 37 (19%) |
| Targeted therapies | 3 (1.5%) | 20 (10.3%) |
| Peptide receptor radionuclide therapy | 1 (0.5%) | 4 (2%) |
| Systemic chemotherapy | 26 (13.3%) | 6 (3%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magi, L.; Mazzuca, F.; Rinzivillo, M.; Arrivi, G.; Pilozzi, E.; Prosperi, D.; Iannicelli, E.; Mercantini, P.; Rossi, M.; Pizzichini, P.; et al. Multidisciplinary Management of Neuroendocrine Neoplasia: A Real-World Experience from a Referral Center. J. Clin. Med. 2019, 8, 910. https://doi.org/10.3390/jcm8060910
Magi L, Mazzuca F, Rinzivillo M, Arrivi G, Pilozzi E, Prosperi D, Iannicelli E, Mercantini P, Rossi M, Pizzichini P, et al. Multidisciplinary Management of Neuroendocrine Neoplasia: A Real-World Experience from a Referral Center. Journal of Clinical Medicine. 2019; 8(6):910. https://doi.org/10.3390/jcm8060910
Chicago/Turabian StyleMagi, Ludovica, Federica Mazzuca, Maria Rinzivillo, Giulia Arrivi, Emanuela Pilozzi, Daniela Prosperi, Elsa Iannicelli, Paolo Mercantini, Michele Rossi, Patrizia Pizzichini, and et al. 2019. "Multidisciplinary Management of Neuroendocrine Neoplasia: A Real-World Experience from a Referral Center" Journal of Clinical Medicine 8, no. 6: 910. https://doi.org/10.3390/jcm8060910