Pulmonary Vessel Obstruction Does Not Correlate with Severity of Pulmonary Embolism
by
 , and
, and
Marianne Lerche
1 ,
,
Nikolaos Bailis
2,
Mideia Akritidou
2,
Hans Jonas Meyer
2 and
Alexey Surov
2,* 1
Department of Respiratory Medicine, University of Leipzig, Liebigstr. 20, 04103 Leipzig, Germany
2
Department of Radiology, University of Leipzig, Liebigstr. 20, 04103 Leipzig, Germany
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2019, 8(5), 584; https://doi.org/10.3390/jcm8050584
Submission received: 9 March 2019
/
Revised: 13 April 2019
/
Accepted: 23 April 2019
/
Published: 28 April 2019
(This article belongs to the Section Pulmonology)
Abstract
:The aim of the present study was to analyze possible relationships between pulmonary vessel obstruction and clinically relevant parameters and scores in patients with pulmonary embolism (PE). Overall, 246 patients (48.8% women and 51.2% men) with a mean age of 64.0 ± 17.1 years were involved in the retrospective study. The following clinical scores were calculated in the patients: Wells score, Geneva score, and pulmonary embolism severity index (PESI) score. Levels of D-dimer (µg/mL), lactate, pH, troponin, and N-terminal natriuretic peptide (BNP, pg/mL) were acquired. Thrombotic obstruction of the pulmonary arteries was quantified according to Mastora score. The data collected were evaluated by means of descriptive statistics. Spearman’s correlation coefficient was used to analyze associations between the investigated parameters. P values < 0.05 were taken to indicate statistical significance. Mastora score correlated weakly with lactate level and tended to correlate with D-dimer and BNP levels. No other clinical or serological parameters correlated significantly with clot burden. Thrombotic obstruction of pulmonary vessels did not correlate with clinical severity of PE.
1. Introduction
Acute pulmonary embolism (PE) is a common disease with a high mortality. According to the literature, the short-term mortality after an episode of acute PE can reach up to 65% [1,2]. Therefore, an immediate risk stratification of patients with acute PE at the time of presentation is very important. The use of pulmonary vessel obstruction quantified by several scores as a possible clinical predictor in PE has been widely discussed in the literature. However, the role of obstruction grade in PE for the prediction of possible complications is still unknown. The reported data regarding associations between pulmonary vessel obstruction and morbidity/mortality in PE are very contradictory. For example, Wu et al. [3] found that clot burden quantified on CT pulmonary angiography was an important predictor of death in patients with PE. Similar results were also reported by Van der Meer et al. [4]. However, other authors did not find any associations between clot burden and mortality in PE [5,6].
According to the literature, there are several clinical and serological parameters which have been established as predictors for morbidity and mortality in PE. These include pulmonary embolism severity index (PESI) [7,8], and different serological parameters, such as lactate [9], troponin [10,11] and N-terminal natriuretic peptide (BNP) [12]. Presumably, pulmonary vessel obstruction may correlate strongly with severity of PE. Therefore, the aim of the present study was to analyze possible relationships between pulmonary vessel obstruction and clinically relevant parameters and scores in patients with PE.
2. Materials and Methods
This retrospective study was approved by the institutional review board (Nr.: 118/19-ck, Ethics Committee, University of Leipzig, Leipzig, Germany).
Overall, 246 cases with PE were acquired for this retrospective study. There were 120 (48.8%) female patients and 126 (51.2%) male patients with a mean age of 64.0 ± 17.1 years, a median age of 65 years, and a range of 15–97 years.
The following clinical scores were calculated in the patients: Wells score, Geneva score, and PESI score. Furthermore, D-dimer level (µg/mL), lactate (venous blood, mmol/L), pH (venous blood), troponin (pg/mL), and N-terminal natriuretic peptide (BNP, pg/mL) were acquired for the study.
Additionally, a risk stratification of PE was performed according to the American Heart Association (AHA) as follows: low risk PE, submassive PE and massive PE [13].
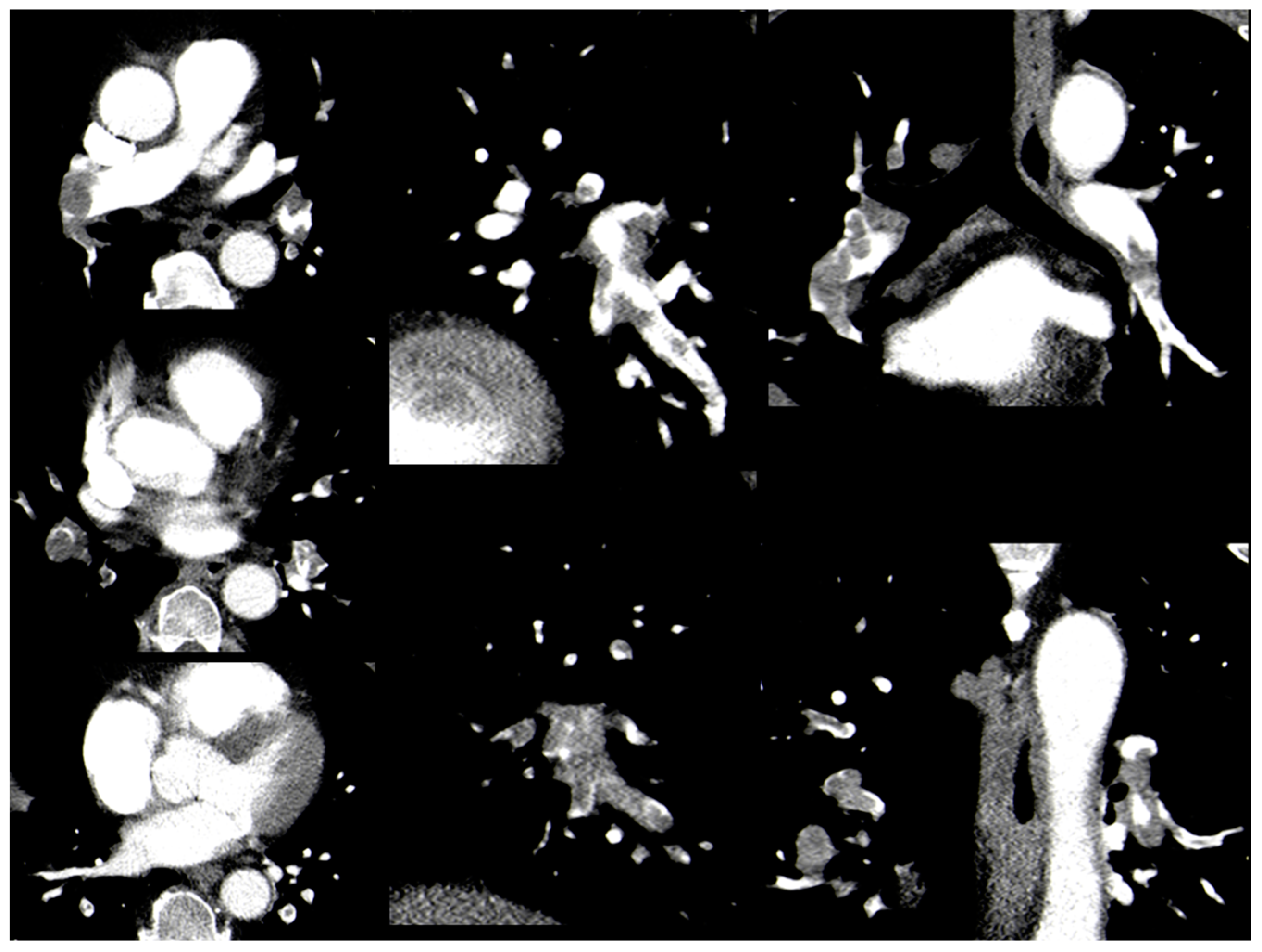
Thrombotic obstruction of the pulmonary arteries was calculated according to Mastora et al. [14] (Mastora score), as reported previously. For this score, the obstruction of the mediastinal, lobar, and segmental arteries was quantified by a percentage, i.e., (thrombus divided by the vessel lumen) multiplied by 100%. The analysis of thrombotic obstruction was performed in three-dimensional images (Figure 1). Thereafter, the sum of the percentages of all arteries was calculated as the global obstruction score with a maximum of 300%.
The statistical analysis and graphics creation were performed using GraphPad Prism (GraphPad Software, La Jolla, CA, USA). Collected data were evaluated by means of descriptive statistics (absolute and relative frequencies). Spearman’s correlation coefficient (p) was used to analyze associations between investigated parameters. In all instances, p values <0.05 were taken to indicate statistical significance.
3. Results
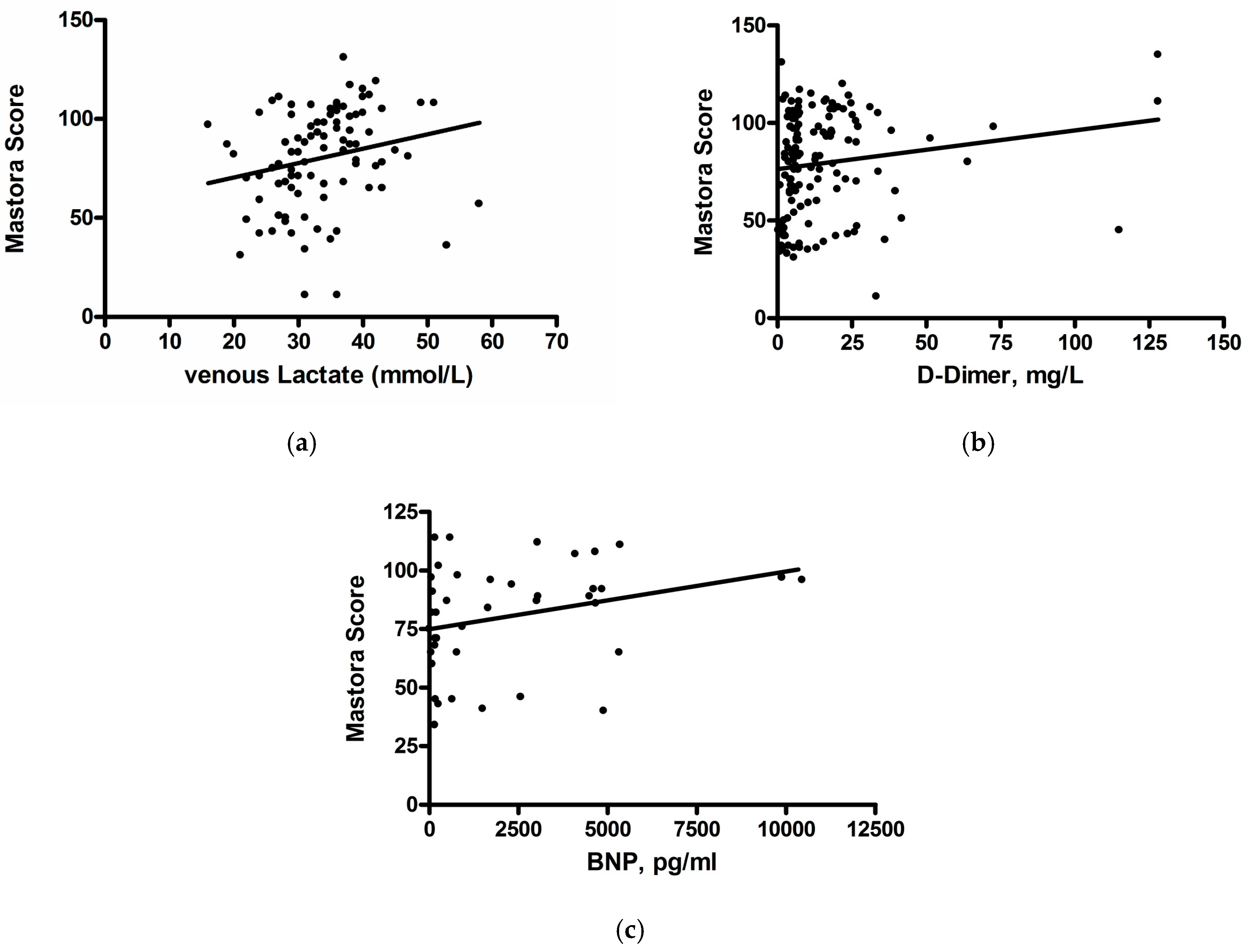
A complete overview of the results including mean values, standard deviation and ranges is shown in Table 1. The results of correlation analysis are given in Table 2. Mastora score correlated weakly with lactate level (ρ = 0.17, p = 0.01) and tended to correlate weakly with D-dimer level and BNP (ρ = 0.15, p = 0.09 and ρ = 0.29, p = 0.063, respectively) (Figure 2a–c). No other clinical or serological parameters correlated statistically significantly with clot burden.
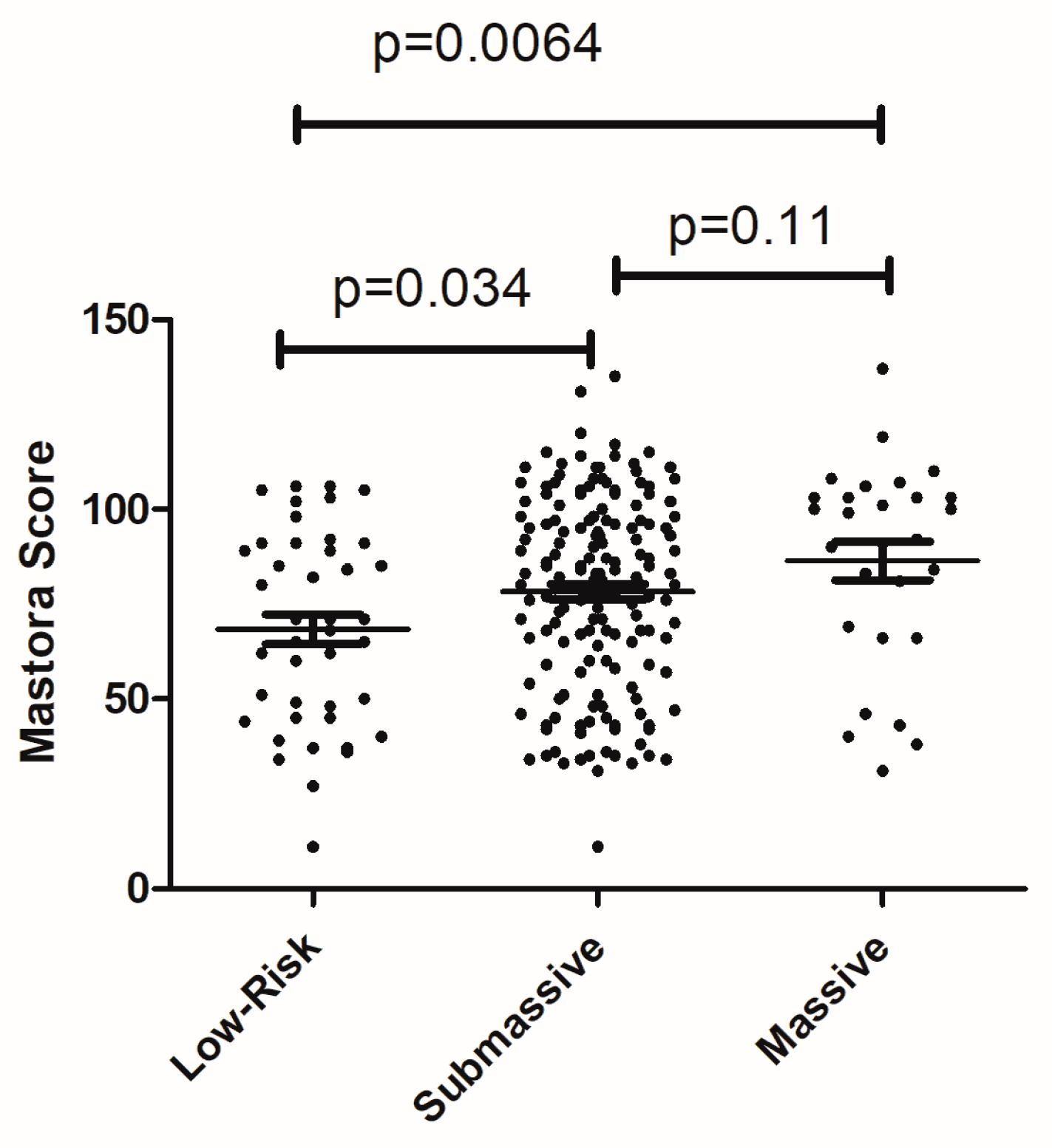
Furthermore, clot burden between the subgroups of PE according to the AHA was compared. Low risk PE was found in 42 patients, submassive PE in 160 cases, and massive PE in 29 patients. Mastora score values overlapped between the three groups (Figure 3). Patients with massive PE had a higher clot burden in comparison to the patients with low risk PE (p = 0.0064). Additionally, in patients with submassive PE, Mastora score values were also higher than in patients with low risk PE (p = 0.034).
4. Discussion
This is the first study to analyze direct associations between quantified thrombotic vessel obstruction and clinically relevant parameters in PE. Our results showed that clot burden did not correlate with important clinical and/or serological parameters in PE. This finding is very unusual. In fact, presumably, the severity of pulmonary vessel obstruction may be associated with the severity of clinical manifestation of PE. Interestingly, vessel obstruction also did not correlate with scores predicting probability of PE like Wells and Geneva scores. Previous studies analyzed only the values of the scores in relation to presence/absence of PE but not their associations with the severity of pulmonary vessel obstruction. Furthermore, our study showed that D-dimer level only tended to correlate weakly with Mastora score. Although this finding is also surprising, similar results were reported by other authors [15].
Our study also showed that thrombotic vessel obstruction did not correlate with clinically established scores for the prediction of PE severity, such as PESI score. This finding is very important. According to the literature, PESI can accurately stratify risks in PE [16,17]. Furthermore, PESI can predict mortality rate in patients with PE [16]. Our results suggest that thrombotic vessel obstruction may not significantly influence severity and mortality in PE. This is in agreement with some previous reports, which also did not find any associations between clot burden and outcome in PE. To date, Ghuysen et al. [18] have shown that neither the pulmonary obstruction index nor the pulmonary artery pressure in PE could predict patient outcome. According to Apfaltrer et al. [19], clot burden did not correlate with clinical outcome in PE. Similar results were also observed by Furlan et al. [20]. Overall, the data indicated that thrombus burden cannot be used as a clinical marker in PE. However, Attina et al. [21] found that vessel obstruction can be used for a risk stratification of pulmonary heart disease or death in patients with acute PE. Also, in the study of Martinez et al. [22] survivors had lower thrombotic burden in comparison to the deceased patients.
We found that Mastora score values were different in patients with low risk, submassive and massive PEs according to the AHA risk stratification. However, the values of clot burden overlapped significantly between the subgroups. Therefore, clot burden cannot be used as a certain factor for risk stratification in PE.
Another important question is the possible relationship between thrombotic vessel obstruction and right ventricular dysfunction (RVD) in PE. Previously, numerous reports found significant associations between RVD and mortality in PE [4,18,19,23]. PE results in a rapid increase in pulmonary vascular resistance that may lead to RVD and eventually to heart failure and death [19]. Presumably, thrombotic vessel obstruction provokes pulmonary arterial hypertension and dilation and/or failure of the right ventricle. The latter yields a release of troponin and BNP. According to the literature, serum troponin is one of the significant predictors in PE [10,24]. Previous investigations showed that an elevated troponin level was associated with right ventricular dysfunction in PE [24,25]. Furthermore, numerous reports suggested that troponin level was an independent predictor of short-term outcome in patients with PE [10,24,25]. In addition, troponin can predict long-term outcome in PE [10,24,25]. These results were confirmed by a meta-analysis, which found that elevated troponin levels were associated with a five-fold increased risk for all causes of short-term mortality and about a four-fold increased risk for serious adverse events [10]. Previously, only three studies with relatively small numbers of patients analyzed associations between troponin level and pulmonary obstruction in pulmonary embolism patients [26,27,28]. Furthermore, the reported correlation coefficients were weak. Thieme et al. [26], in their study with 63 patients, found a statistically significant correlation between Mastora score and troponin level (r = 0.37, p = 0.016). Furthermore, in the study of Gül et al. [27] which investigated 28 patients with PE, vessel obstruction index (Qanadli score) correlated slightly with troponin level (r = 0.32, p = 0.01). Similarly, Jeebun et al. [28] showed a higher statistically significant correlation between clot burden and troponin level in patients (r = 0.41, p = 0.048). In the present study, no significant correlation between troponin level and Mastora score was observed. Therefore, it may be postulated that thrombotic vessel obstruction cannot be considered a main cause of cardiac damage in PE.
Additionally, BNP was reported as a significant predictor of clinical outcome in patients with PE [29]. Surprisingly, there were no studies investigating associations between clot burden and BNP. As shown, clot burden tended to correlate with BNP level. However, the correlation coefficient was weak. This finding suggests that vessel obstruction also does not appear to be a major factor of cardiac dilatation in PE.
According to the literature, there are also other parameters that can predict the severity and prognosis of PE. For instance, serum lactate has been reported as a powerful predictor of short-term PE-related complications [30]. Moreover, patients with high lactate values had a higher mortality rate [8,30]. No previous investigations analyzed associations between lactate and clot burden in PE. As shown in the present study, Mastora score only correlated weakly with serum lactate value, i.e., the relationship between the parameters is not linear. Therefore, it can be postulated that, paradoxically, vessel obstruction does not play a central role in tissue hypoxia.
Overall, the present study showed that the mechanisms of heart dysfunction and/or failure in PE are more complex than was assumed and cannot be explained by only mechanical vessel obstruction.
The present study is limited to its retrospective design. In order to reduce possible bias, the CTs were evaluated in a blinded manner in relation to the clinical features. However, as mentioned above, this is the first study to investigate direct associations between thrombus burden and the established clinically relevant parameters in PE. Furthermore, this study investigated a large number of patients. Clearly, further prospective studies are needed to confirm our results.
In conclusion, our study showed that thrombotic obstruction of pulmonary vessels did not correlate with clinical severity of PE.
Author Contributions
M.L., N.B., M.A., H.J.M., A.S. made substantial contributions to conception and design, acquisition of data, and analysis and interpretation of data; M.L., N.B., M.A., H.J.M., A.S. were involved in drafting the manuscript or revising it critically for important intellectual content; M.L., N.B., M.A., H.J.M., A.S. gave final approval of the version to be published. Each author participated sufficiently in the work to take public responsibility for appropriate portions of the content; and M.L., N.B., A.S. agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
The Authors thank the Universitätsbibliothek Leipzig, Leipzig, Germany, for the supports.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Goldhaber, S.Z.; Visani, L.; De Rosa, M. Acute pulmonary embolism: Clinical outcomes in the international cooperative pulmonary embolism registry (ICOPER). Lancet 1999, 353, 1386–1389. [Google Scholar] [CrossRef]
- Ng, A.C.; Chung, T.; Yong, A.S.; Wong, H.S.; Chow, V.; Celermajer, D.S.; Kritharides, L. Long-term cardiovascular and noncardiovascular mortality of 1023 patients with confirmed acute pulmonary embolism. Circulation 2011, 4, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.S.; Pezzullo, J.A.; Cronan, J.J.; Hou, D.D.; Mayo-Smith, W.W. CT pulmonary angiography: Quantification of pulmonary embolus as a predictor of patient outcome-initial experience. Radiology 2004, 230, 831–835. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, R.W.; Pattynama, P.M.; van Strijen, M.J.; van den Berg-Huijsmans, A.A.; Hartmann, I.J.; Putter, H.; de Roos, A.; Huisman, M.V. Right ventricular dysfunction and pulmonary obstruction index at helical CT: Prediction of clinical outcome during 3-month follow-up in patients with acute pulmonary embolism. Radiology 2005, 235, 798–803. [Google Scholar] [CrossRef]
- Ghaye, B.; Ghuysen, A.; Bruyere, P.J.; D’Orio, V.; Dondelinger, R.F. Can CT pulmonary angiography allow assessment of severity and prognosis in patients presenting with pulmonary embolism? What the radiologist needs to know. Radiographics 2006, 26, 23–39. [Google Scholar] [CrossRef] [PubMed]
- Collomb, D.; Paramelle, P.J.; Calaque, O.; Bosson, J.L.; Vanzetto, G.; Barnoud, D.; Pison, C.; Coulomb, M.; Ferretti, G. Severity assessment of acute pulmonary embolism: Evaluation using helical CT. Eur. Radiol. 2003, 13, 1508–1514. [Google Scholar] [CrossRef]
- Dentali, F.; Riva, N.; Turato, S.; Grazioli, S.; Squizzato, A.; Steidl, L.; Guasti, L.; Grandi, A.M.; Ageno, W. Pulmonary embolism severity index accurately predicts long-term mortality rate in patients hospitalized for acute pulmonary embolism. J. Thromb. Haemost. 2013, 11, 2103–2110. [Google Scholar] [CrossRef] [Green Version]
- Barra, S.N.; Paiva, L.; Providência, R.; Fernandes, A.; Marques, A.L. A review on state-of-the-art data regarding safe early discharge following admission for pulmonary embolism: What do we know? Clin. Cardiol. 2013, 36, 507–515. [Google Scholar] [CrossRef]
- Urbina, T.; Bigé, N.; Nguyen, Y.; Boelle, P.; Dubée, V.; Joffre, J.; Baudel, I.A.J.; Maury, E.; Guidet, B.; Ait-Oufella, H. Tissue perfusion alterations correlate with mortality in patients admitted to the intensive care unit for acute pulmonary embolism: An observational study. Medicine 2018, 97, e11993. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, A.; Saleeb, M.; Rathor, P.; Sehgal, V.; Kabak, B.; Hosur, S. Prognostic value of troponins in acute nonmassive pulmonary embolism: A meta-analysis. Heart Lung 2015, 44, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Lee Chuy, K.; Hakemi, E.U.; Alyousef, T.; Dang, G.; Doukky, R. The long-term prognostic value of highly sensitive cardiac troponin I in patients with acute pulmonary embolism. Clin. Cardiol. 2017, 40, 1271–1278. [Google Scholar] [CrossRef] [Green Version]
- Henzler, T.; Roeger, S.; Meyer, M.; Schoepf, U.J.; Nance, J.W., Jr.; Haghi, D.; Kaminski, W.E.; Neumaier, M.; Schoenberg, S.O.; Fink, C. Pulmonary embolism: CT signs and cardiac biomarkers for predicting right ventricular dysfunction. Eur. Respir. J. 2012, 39, 919–926. [Google Scholar] [CrossRef]
- Jaff, M.R.; McMurtry, M.S.; Archer, S.L.; Cushman, M.; Goldenberg, N.; Goldhaber, S.Z.; Jenkins, J.S.; Kline, J.A.; Michaels, A.D.; Thistlethwaite, P.; et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: A scientific statement from the American Heart Association. Circulation 2011, 123, 1788–1830. [Google Scholar] [CrossRef]
- Mastora, I.; Remy-Jardin, M.; Masson, P.; Galland, E.; Delannoy, V.; Bauchart, J.J.; Remy, J. Severity of acute pulmonary embolism: Evaluation of a new spiral CT angiographic score in correlation with echocardiographic data. Eur. Radiol. 2003, 13, 29–35. [Google Scholar]
- Ji, Y.; Sun, B.; Juggessur-Mungur, K.S.; Li, Z.; Zhang, Z. Correlation of D-dimer level with the radiological severity indexes of pulmonary embolism on computed tomography pulmonary angiography. Chin. Med. J. 2014, 127, 2025–2029. [Google Scholar]
- Tamizifar, B.; Fereyduni, F.; Esfahani, M.A.; Kheyri, S. Comparing three clinical prediction rules for primarily predicting the 30-day mortality of patients with pulmonary embolism: The "Simplified Revised Geneva Score," the "Original PESI," and the "Simplified PESI". Adv. Biomed. Res. 2016, 5, 137. [Google Scholar] [CrossRef]
- Elias, A.; Mallett, S.; Daoud-Elias, M.; Poggi, J.N.; Clarke, M. Prognostic models in acute pulmonary embolism: A systematic review and meta-analysis. BMJ Open 2016, 6, e010324. [Google Scholar] [CrossRef]
- Ghuysen, A.; Ghaye, B.; Willems, V.; Lambermont, B.; Gerard, P.; Dondelinger, R.; D’Orio, V. Computed tomographic pulmonary angiography and prognostic significance in patients with acute pulmonary embolism. Thorax 2005, 60, 956–961. [Google Scholar] [CrossRef] [Green Version]
- Apfaltrer, P.; Henzler, T.; Meyer, M.; Roeger, S.; Haghi, D.; Gruettner, J.; Süselbeck, T.; Wilson, R.B.; Schoepf, U.J.; Schoenberg, S.O.; et al. Correlation of CT angiographic pulmonary artery obstruction scores with right ventricular dysfunction and clinical outcome in patients with acute pulmonary embolism. Eur. J. Radiol. 2012, 81, 2867–2871. [Google Scholar] [CrossRef]
- Furlan, A.; Aghayev, A.; Chang, C.C.; Patil, A.; Jeon, K.N.; Park, B.; Fetzer, D.T.; Saul, M.; Roberts, M.S.; Bae, K.T. Short-term mortality in acute pulmonary embolism: Clot burden and signs of right heart dysfunction at CT pulmonary angiography. Radiology 2012, 265, 283–293. [Google Scholar] [CrossRef]
- Attinà, D.; Valentino, M.; Galiè, N.; Modolon, C.; Buia, F.; de Luca, F.; Bacchi-Reggiani, M.L.; Zompatori, M. Application of a new pulmonary artery obstruction score in the prognostic evaluation of acute pulmonary embolism: Comparison with clinical and haemodynamic parameters. Radiol. Med. 2011, 116, 230–245. [Google Scholar] [CrossRef]
- Alonso Martinez, J.L.; Anniccherico Sánchez, F.J.; Urbieta Echezarreta, M.A.; García, I.V.; Álvaro, J.R. Central Versus Peripheral Pulmonary Embolism: Analysis of the Impact on the Physiological Parameters and Long-term Survival. N. Am. J. Med. Sci. 2016, 8, 134–142. [Google Scholar] [CrossRef] [Green Version]
- Bach, A.G.; Nansalmaa, B.; Kranz, J.; Taute, B.M.; Wienke, A.; Schramm, D.; Surov, A. CT pulmonary angiography findings that predict 30-day mortality in patients with acute pulmonary embolism. Eur. J. Radiol. 2015, 84, 332–337. [Google Scholar] [CrossRef]
- Keller, K.; Beule, J.; Schulz, A.; Coldewey, M.; Dippold, W.; Balzer, J.O. Cardiac troponin I for predicting right ventricular dysfunction and intermediate risk in patients with normotensive pulmonary embolism. Neth. Heart J. 2015, 23, 55–61. [Google Scholar] [CrossRef]
- Keller, K.; Beule, J.; Schulz, A.; Coldewey, M.; Dippold, W.; Balzer, J.O. Right ventricular dysfunction in hemodynamically stable patients with acute pulmonary embolism. Thromb. Res. 2014, 133, 555–559. [Google Scholar] [CrossRef]
- Thieme, S.F.; Ashoori, N.; Bamberg, F.; Sommer, W.H.; Johnson, T.R.; Leuchte, H.; Becker, A.; Maxien, D.; Helck, A.D.; Behr, J.; et al. Severity assessment of pulmonary embolism using dual energy CT—Correlation of a pulmonary perfusion defect score with clinical and morphological parameters of blood oxygenation and right ventricular failure. Eur. Radiol. 2012, 22, 269–278. [Google Scholar] [CrossRef]
- Gul, E.E.; Can, I.; Guler, I.; Yesildag, A.; Abdulhalikov, T.; Kayrak, M.; Ozdemir, K.; Gok, H. Association of pulmonary artery obstruction index with elevated heart-type fatty acid binding protein and short-term mortality in patients with pulmonary embolism at intermediate risk. Diagn. Interv. Radiol. 2012, 18, 531–536. [Google Scholar]
- Jeebun, V.; Doe, S.J.; Singh, L.; Worthy, S.A.; Forrest, I.A. Are clinical parameters and biomarkers predictive of severity of acute pulmonary emboli on CTPA? QJM 2010, 103, 91–97. [Google Scholar] [CrossRef]
- Klok, F.A.; Mos, I.C.; Huisman, M.V. Brain-type natriuretic peptide levels in the prediction of adverse outcome in patients with pulmonary embolism: A systematic review and meta-analysis. Am. J. Respir. Crit. Care Med. 2008, 178, 425–430. [Google Scholar] [CrossRef]
- Vanni, S.; Nazerian, P.; Bova, C.; Bondi, E.; Morello, F.; Pepe, G.; Paladini, B.; Liedl, G.; Cangioli, E.; Grifoni, S.; Jiménez, D. Comparison of clinical scores for identification of patients with pulmonary embolism at intermediate-high risk of adverse clinical outcome: The prognostic role of plasma lactate. Intern. Emerg. Med. 2017, 12, 657–665. [Google Scholar] [CrossRef]
Figure 1.
Case with bilateral pulmonary embolism. Total Mastora score is 65%.

Figure 2.
Associations between Mastora score and lactate level (a), D-dimer (b), and BNP (c).

Figure 3.
Comparison of Mastora score values between patients with low risk pulmonary embolism (PE), submassive and massive PE.
Figure 3.
Comparison of Mastora score values between patients with low risk pulmonary embolism (PE), submassive and massive PE.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Analysis of clinical and radiological parameters.
| Parameters | Mean ± Standard Deviation | Median | Range |
|---|---|---|---|
| Wells score | 6.06 ± 1.79 | 6 | 3–10.5 |
| Geneva score | 13.61 ± 3.57 | 7 | 0–17 |
| D-dimer | 13.10 ± 14.84 | 7.21 | 0.26–128 |
| PESI score | 2 ± 1 | 2 | 0–6 |
| Troponin | 90.69 ± 141.98 | 55.18 | 3–128 |
| BNP | 2112.25 ± 2622.85 | 776.7 | 0–10,445 |
| Lactate | 3.48 ± 3.56 | 2.3 | 0.6–23 |
| pH | 7.34 ± 0.15 | 7.39 | 6.59–7.53 |
| Mastora score | 77.49 ± 26.04 | 82 | 11–137 |
PESI: pulmonary embolism severity index; BNP: N-terminal natriuretic peptide.
Table 2.
Correlations between Mastora score and clinical/serological parameters in patients with pulmonary embolism.
Table 2.
Correlations between Mastora score and clinical/serological parameters in patients with pulmonary embolism.
| Wells Score | Geneva Score | D-Dimer | PESI Score | BNP | Troponin | Lactate | pH | |
|---|---|---|---|---|---|---|---|---|
| Mastora Score | ρ = 0.07 | ρ = 0.06 | ρ = 0.15 | ρ = -0.03 | ρ = 0.29 | ρ = 0.08 | ρ = 0.17 | ρ = 0.02 |
| p = 0.27 | p = 0.40 | p = 0.09 | p = 0.39 | p = 0.063 | p = 0.29 | p = 0.01 | p = 0.77 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lerche, M.; Bailis, N.; Akritidou, M.; Meyer, H.J.; Surov, A. Pulmonary Vessel Obstruction Does Not Correlate with Severity of Pulmonary Embolism. J. Clin. Med. 2019, 8, 584. https://doi.org/10.3390/jcm8050584
AMA Style
Lerche M, Bailis N, Akritidou M, Meyer HJ, Surov A. Pulmonary Vessel Obstruction Does Not Correlate with Severity of Pulmonary Embolism. Journal of Clinical Medicine. 2019; 8(5):584. https://doi.org/10.3390/jcm8050584
Chicago/Turabian StyleLerche, Marianne, Nikolaos Bailis, Mideia Akritidou, Hans Jonas Meyer, and Alexey Surov. 2019. "Pulmonary Vessel Obstruction Does Not Correlate with Severity of Pulmonary Embolism" Journal of Clinical Medicine 8, no. 5: 584. https://doi.org/10.3390/jcm8050584
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.