Association of Pre-Eclampsia with Carotid Artery Intima–Media Thickness and Non-Alcoholic Fatty Liver Disease

Abstract
:1. Introduction
2. Experimental Section
2.1. Ethics Approval
2.2. Study Population
2.3. Statistical Analysis
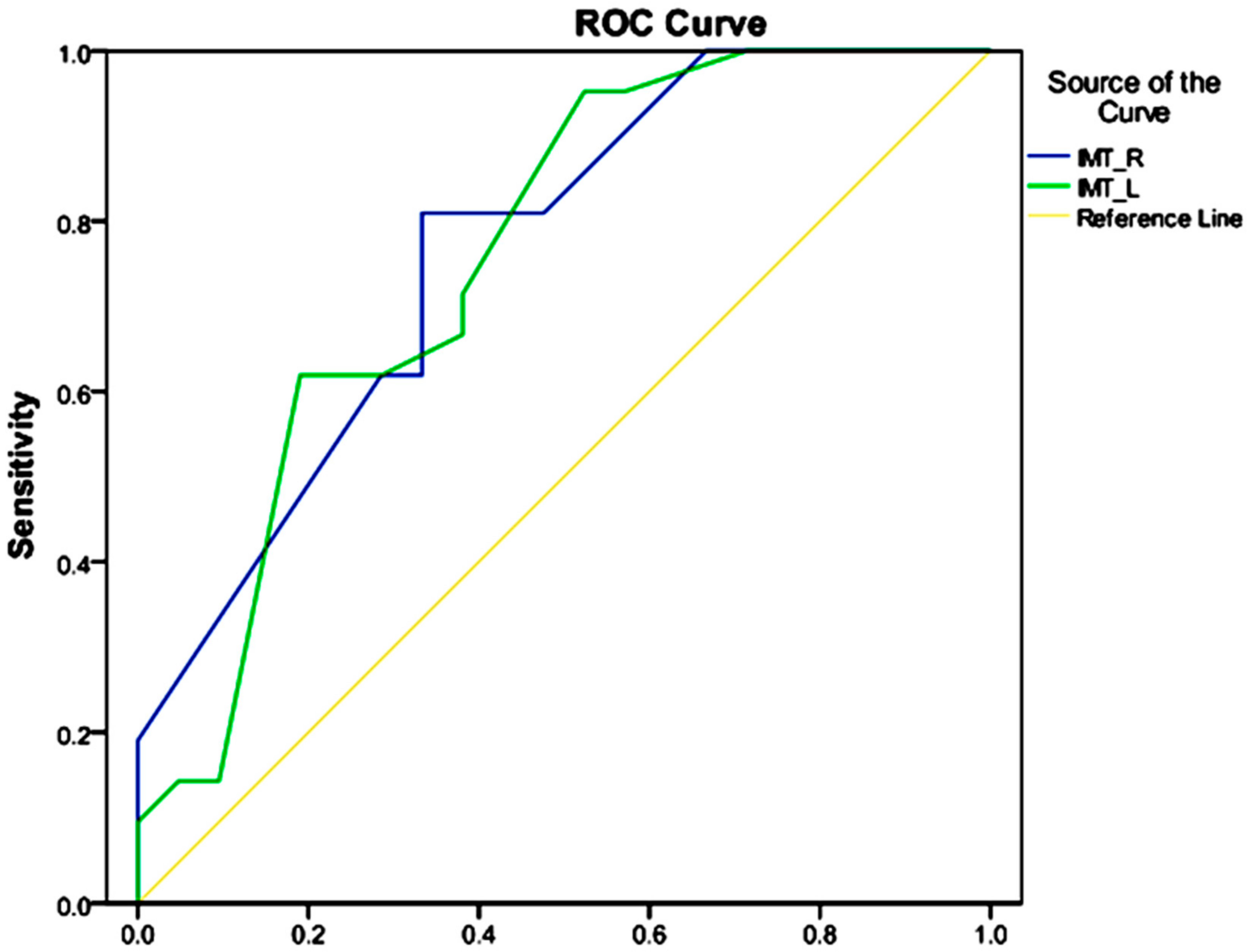
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cai, J.; Zhang, S.; Huang, W. Association between nonalcoholic fatty liver disease and carotid atherosclerosis: A meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 7673–7678. [Google Scholar] [PubMed]
- Lee, Y.J.; Jang, Y.N.; Han, Y.M.; Kim, H.M.; Jeong, J.M.; Son, M.J.; Jin, C.B.; Kim, H.J.; Seo, H.S. Caffeoylquinic Acid-Rich Extract of Aster glehni F. Schmidt Ameliorates Nonalcoholic Fatty Liver through the Regulation of PPARδ and Adiponectin in ApoE KO Mice. PPAR Res. 2017, 2017, 3912567. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Jang, Y.N.; Han, Y.M.; Kim, H.M.; Jeong, J.M.; Seo, H.S. Fimasartan Ameliorates Nonalcoholic Fatty Liver Disease through PPARδ Regulation in Hyperlipidemic and Hypertensive Conditions. PPAR Res. 2017, 2017, 8048720. [Google Scholar] [CrossRef] [PubMed]
- Petrakos, G.; Andriopoulos, P.; Tsironi, M. Pregnancy in women with thalassemia: Challenges and solutions. Int. J. Womens Health 2016, 8, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Powe, C.E.; Levine, R.J.; Karumanchi, S.A. Preeclampsia, a disease of the maternal endothelium: The role of antiangiogenic factors and implications for later cardiovascular disease. Circulation 2011, 123, 2856. [Google Scholar] [CrossRef] [PubMed]
- Uzan, J.; Carbonnel, M.; Piconne, O.; Asmar, R.; Ayoubi, J.M. Pre-eclampsia: Pathophysiology, diagnosis, and management. Vasc. Health Risk Manag. 2011, 7, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Kattah, A.G.; Garovic, V.D. The management of hypertension in pregnancy. Adv. Chronic Kidney Dis. 2013, 20, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Burchakov, D.I.; Kuznetsova, I.V.; Uspenskaya, Y.B. Omega-3 Long-Chain Polyunsaturated Fatty Acids and Preeclampsia: Trials Say “No,” but Is It the Final Word? Nutrients 2017, 9, 1364. [Google Scholar] [CrossRef] [PubMed]
- Amirabi, A.; Danaii, S. A comparison of 4- and 24-hour urine samples for the diagnosis of proteinuria in pregnancy. Iran. J. Med. Sci. 2011, 36, 167–171. [Google Scholar] [PubMed]
- Nischintha, S.; Pallavee, P.; Ghose, S. Correlation between 24-h urine protein, spot urine protein/creatinine ratio, and serum uric acid and their association with fetomaternal outcomes in preeclamptic women. J. Nat. Sci. Biol. Med. 2014, 5, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Duhig, K.; Vandermolen, B.; Shennan, A. Recent advances in the diagnosis and management of pre-eclampsia. F1000Prime Rep. 2018, 7, 242. [Google Scholar] [CrossRef] [Green Version]
- Burwick, R.M.; Pilliod, R.A.; Dukhovny, S.E.; Caughey, A.B. Fetal hydrops and the risk of severe preeclampsia. J. Matern. Fetal. Neonatal. Med. 2017, 8, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Berry, C.; Atta, M.G. Hypertensive disorders in pregnancy. World J. Nephrol. 2016, 5, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Ye, C.; Ruan, Y.; Zou, L.; Li, G.; Li, C. The 2011 survey on hypertensive disorders of pregnancy (HDP) in China: Prevalence, risk factors, complications, pregnancy and perinatal outcomes. PloS ONE 2014, 9, e100180. [Google Scholar] [CrossRef] [PubMed]
- Qu, B.; Qu, T. Causes of changes in carotid intima-media thickness: A literature review. Cardio. Ultra. 2015, 13, 46. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.H.; Youn, H.J. Is Carotid Artery Ultrasound Still Useful Method for Evaluation of Atherosclerosis? Korean Circ. J. 2017, 47, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ring, M.; Eriksson, M.J.; Jogestrand, T.; Caidahl, K. Ultrasound measurements of carotid intima-media thickness by two semi-automated analysis systems. Clin. Physiol. Funct. Imaging 2016, 36, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Blaauw, J.; van Pampus, M.G.; Van Doormaal, J.J.; Fokkema, M.R.; Fidler, V.; Smit, A.J. Increased intima-media thickness after early-onset preeclampsia. Obstet. Gynecol. 2006, 107, 1345–1351. [Google Scholar] [CrossRef] [PubMed]
- Blaauw, J.; Souwer, E.T.D.; Coffeng, S.M.; Smit, A.J.; van Doormaal, J.J.; Faas, M.M. Follow up of intima–media thickness after severe early-onset preeclampsia. Acta Obstet. Gynecol. Scand. 2014, 93, 1309–1316. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L.J.; Xue, D.; Duan, Y.Y.; Cao, T.S.; Yang, H.G.; Zhou, N. Carotid arterial intima–media thickness and arterial stiffness in pre-eclampsia: Analysis with a radiofrequency ultrasound technique. Ultrasound. Obstet. Gynecol. 2013, 42, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.W.; Dueker, N.; Jamieson, D.J.; Cole, J.W.; Wozniak, M.A.; Stern, B.J. Preeclampsia and the Risk of Ischemic Stroke among Young Women Results from the Stroke Prevention in Young Women Study. Stroke 2006, 37, 1055–1059. [Google Scholar] [CrossRef] [PubMed]
- Leonard, D.; Akhter, T.; Nordmark, G.; Ronnblom, L.; Naessen, T. Increased carotid intima thickness and decreased media thickness in premenopausal women with systemic lupus erythematosus: An investigation by non-invasive high-frequency ultrasound. Scand. J. Rheumatol. 2011, 40, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Hammoud, G.M.; Ibdah, J.A. Preeclampsia-induced liver dysfunction, HELLP syndrome and acute fatty liver of pregnancy. Clin. Liver Dis. 2014, 4, 69–73. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Mean ± SD (n = 42) |
|---|---|
| Mother’s age (years) | 31.43 ± 5.58 |
| Gestational age (week) | 33.67 ± 2.88 |
| BMI, kg/m3 | 31.47 ± 3.63 |
| Systolic blood pressure (mmHg) | 114.28 ± 16.03 |
| Diastolic blood pressure (mmHg) | 74.28 ± 14.51 |
| Hb, g/dL | 12.3 ± 1.7 |
| PLT × 103/mL | 192.5 ± 54.4 |
| TG, mg/dL | 319.8 ± 108.6 |
| CHOL, mg/dL | 217.5 ± 58.5 |
| LDL, mg/dL | 127.8 ± 37.9 |
| HDL, mg/dL | 54.1 ± 6.5 |
| AST, U/L | 26.2 ± 12.6 |
| ALT, U/L | 24.4 ± 21.5 |
| LDH, mg/dL | 383.6 ± 146.3 |
| 24-h urine creatinine, g/mmol | 917.2 ± 238.3 |
| 24-h urine protein, g/mmol | 723.8 ± 356.5 |
| 24-h urine volume, g/mmol | 1745.8 ± 501.9 |
| Intima–media thickness of the right carotid artery, mm | 0.55 ± 0.09 |
| Intima–media thickness of the left carotid artery, mm | 0.54 ± 0.10 |
| Variable | Status | Frequency (%) |
|---|---|---|
| Gravid | One | 11 (26.2) |
| Two | 13 (31) | |
| Three | 10 (23.8) | |
| Four | 5 (11.9) | |
| Five | 3 (7.1) | |
| Parity | Zero | 15 (35.7) |
| One | 12 (28.6) | |
| Two | 13 (31) | |
| Three | 2 (4.8) | |
| History of hypertension | Yes | 4 (9.5) |
| No | 38 (90.5) | |
| History of pre-eclampsia | Yes | 7 (16.7) |
| No | 35 (83.3) | |
| Non-alcoholic fatty liver | Yes | 19 (45.2) |
| No | 23 (54.8) |
| Variable | Mean ± SD | Significance Level | |
|---|---|---|---|
| Healthy Pregnant Women | Pregnant Women with Pre-Eclampsia | ||
| Mother’s age (years) | 30.00 ± 5.92 | 32.86 ± 4.95 | 0.098 |
| Gestational age (weeks) | 33.57 ± 3.22 | 33.76 ± 2.57 | 0.833 |
| BMI (kilograms per square meter) | 30.65 ± 3.41 | 32.30 ± 3.75 | 0.144 |
| Systolic blood pressure (mmHg) | 102.86 ± 8.30 | 125.71 ± 13.53 | >0.001 |
| Diastolic blood pressure (mmHg) | 64.76 ± 7.50 | 83.81±13.59 | >0.001 |
| Hb | 12.53 ± 1.14 | 12.33 ± 1.14 | 0.624 |
| PLT | 18,361.05 ± 4187.80 | 202,142.8 ± 665,051.74 | 0.279 |
| TG | 322.14 ± 91.15 | 316.62 ± 125.49 | 0.871 |
| CHOL | 191.24 ± 36.69 | 243.67 ± 64.91 | 0.003 |
| LDL | 121.24 ± 21.72 | 134.33 ± 48.6 | 0.267 |
| HDL | 54.38 ± 7.83 | 54.24 ± 5.90 | 0.947 |
| AST | 20.76 ± 5.00 | 31.48 ± 15.60 | 0.005 |
| ALT | 13.90 ± 7.08 | 29.19 ± 32.59 | 0.042 |
| LDH | 370.49 ± 158.92 | 397.42 ± 136.00 | 0.558 |
| 24-h urine protein | 85.59 ± 113.19 | 599.90 ± 972.2 | 0.027 |
| 24-h urine creatinine | 908.86 ± 175.50 | 925.38 ± 292.73 | 0.826 |
| 24-h urine volume | 1942.65 ± 396.99 | 1548.90 ± 526.88 | 0.009 |
| Intima–media thickness of the right carotid artery | 0.51 ± 0.08 | 0.60 ± 0.07 | 0.001 |
| Intima–media thickness of the left carotid artery | 0.10 ± 0.50 | 0.59 ± 0.09 | 0.003 |
| Variable | Frequency (%) | Significance Level | ||
|---|---|---|---|---|
| Status | Healthy Pregnant Women | Pregnant Women with Pre-eclampsia | ||
| Gravid | One | 5 (23.8) | 28.6 (6) | 0.859 |
| Two | 8 (38.1) | 23.8 (5) | ||
| Three | 5 (23.8) | 23.8 (5) | ||
| Four | 2 (9.5) | 14.3 (3) | ||
| Five | 1 (4.8) | 9.5 (2) | ||
| Parity | Zero | 8 (38.1) | 33.3 (7) | 0.479 |
| One | 7 (33.3) | 23.8 (5) | ||
| Two | 6 (28.6) | 33.3 (7) | ||
| Three | 0.0 (0) | 9.5 (2) | ||
| History of hypertension | Yes | 0.0 (0) | 19.0 (4) | 0.053 |
| No | 100 (21) | 81.0 (17) | ||
| History of pre-eclampsia | Yes | 0.0 (0) | 33.3 (7) | 0.004 |
| No | 100 (21) | 66.7 (14) | ||
| Non-alcoholic fatty liver | Yes | 23.8 (5) | 66.7 (14) | 0.006 |
| Variable | Beta Coefficient | Student’s t | Significance Level |
|---|---|---|---|
| Mother’s age (years) | 0.146 | 0.922 | 0.328 |
| BMI (kilograms per square meter) | 0.023 | 0.171 | 0.865 |
| CHOL | 0.172 | 0.978 | 0.335 |
| AST | −0.383 | −1.240 | 0.223 |
| ALT | 0.340 | 1.113 | 0.273 |
| Group (healthy or with pre-eclampsia) | 0.434 | 2.582 | 0.014 |
| Variable | Beta Coefficient | Student’s t | Significance Level |
|---|---|---|---|
| Mother’s age (years) | −0.064 | −0.410 | 0.685 |
| BMI (kilograms per square meter) | 0.008 | 0.054 | 0.957 |
| CHOL | −0.121 | −0.649 | 0.521 |
| AST | −0.105 | −0.322 | 0.750 |
| ALT | 0.372 | 1.145 | 0.260 |
| Group (healthy or with pre-eclampsia) | 0.439 | 2.463 | 0.019 |
| Variable | Test Wald | The Significance Level | Odds Ratio (Confidence Interval) |
|---|---|---|---|
| Mother’s age (years) | 1.933 | 0.164 | 1.107 (1.278-0.959) |
| BMI (kilograms per square meter) | 0.456 | 0.500 | 1.076 (1.330-0.870) |
| History of preeclampsia | 0.512 | 0.474 | 0.462 (3.824-0.056) |
| CHOL | 1.337 | 0.248 | 1.010 (1.028-0.993) |
| AST | 0.441 | 0.507 | 1.048 (1.205-0.912) |
| ALT | 1.440 | 0.230 | 0.959 (1.027-0.895) |
| Group (healthy or with pre-eclampsia) | 2.677 | 0.102 | 4.754 (30.771-0.735) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Memari, B.; Moghiseh, N.; Mohammadian, F.; Ghajarzadeh, M.; Ghoreishian, H. Association of Pre-Eclampsia with Carotid Artery Intima–Media Thickness and Non-Alcoholic Fatty Liver Disease. J. Clin. Med. 2018, 7, 275. https://doi.org/10.3390/jcm7090275
Memari B, Moghiseh N, Mohammadian F, Ghajarzadeh M, Ghoreishian H. Association of Pre-Eclampsia with Carotid Artery Intima–Media Thickness and Non-Alcoholic Fatty Liver Disease. Journal of Clinical Medicine. 2018; 7(9):275. https://doi.org/10.3390/jcm7090275
Chicago/Turabian StyleMemari, Behzad, Niloofar Moghiseh, Farnaz Mohammadian, Mahsa Ghajarzadeh, and Hadi Ghoreishian. 2018. "Association of Pre-Eclampsia with Carotid Artery Intima–Media Thickness and Non-Alcoholic Fatty Liver Disease" Journal of Clinical Medicine 7, no. 9: 275. https://doi.org/10.3390/jcm7090275