Radiotherapy for Elderly Patients Aged ≥75 Years with Clinically Localized Prostate Cancer—Is There a Role of Brachytherapy?

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Treatment Planning
2.2.1. Brachytherapy (BT)
Low-Dose-Rate Interstitial BT (LDR-BT) with or without External Beam Radiotherapy (EBRT)
High-Dose-Rate Interstitial Brachytherapy (HDR-BT) Monotherapy
2.2.2. Image-Guided Intensity-Modulated Radiotherapy (IG-IMRT)
2.3. Statistical Analysis
3. Results
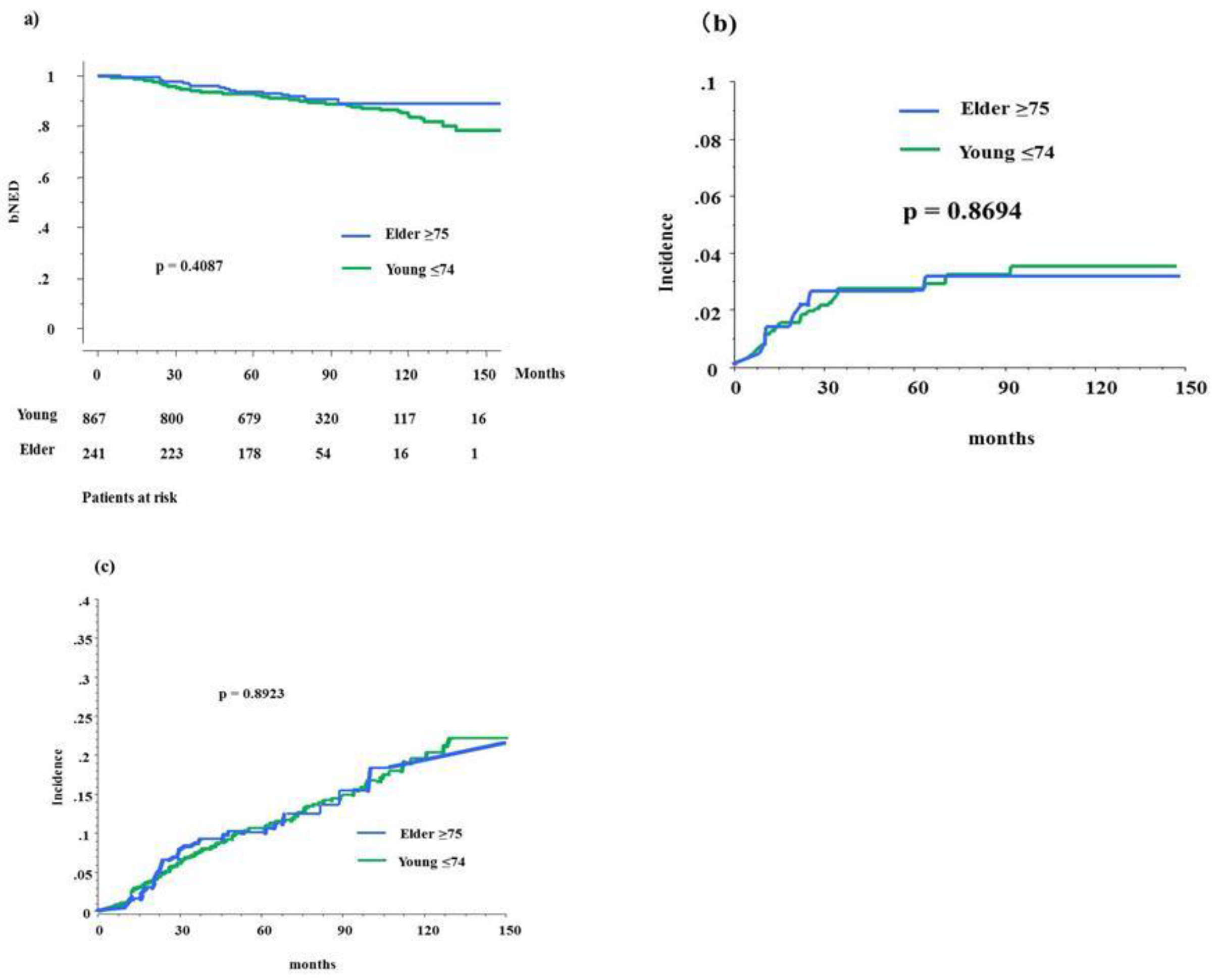
3.1. Biochemical Control, Survival, and Toxicity between Elderly Patients and Younger Controls
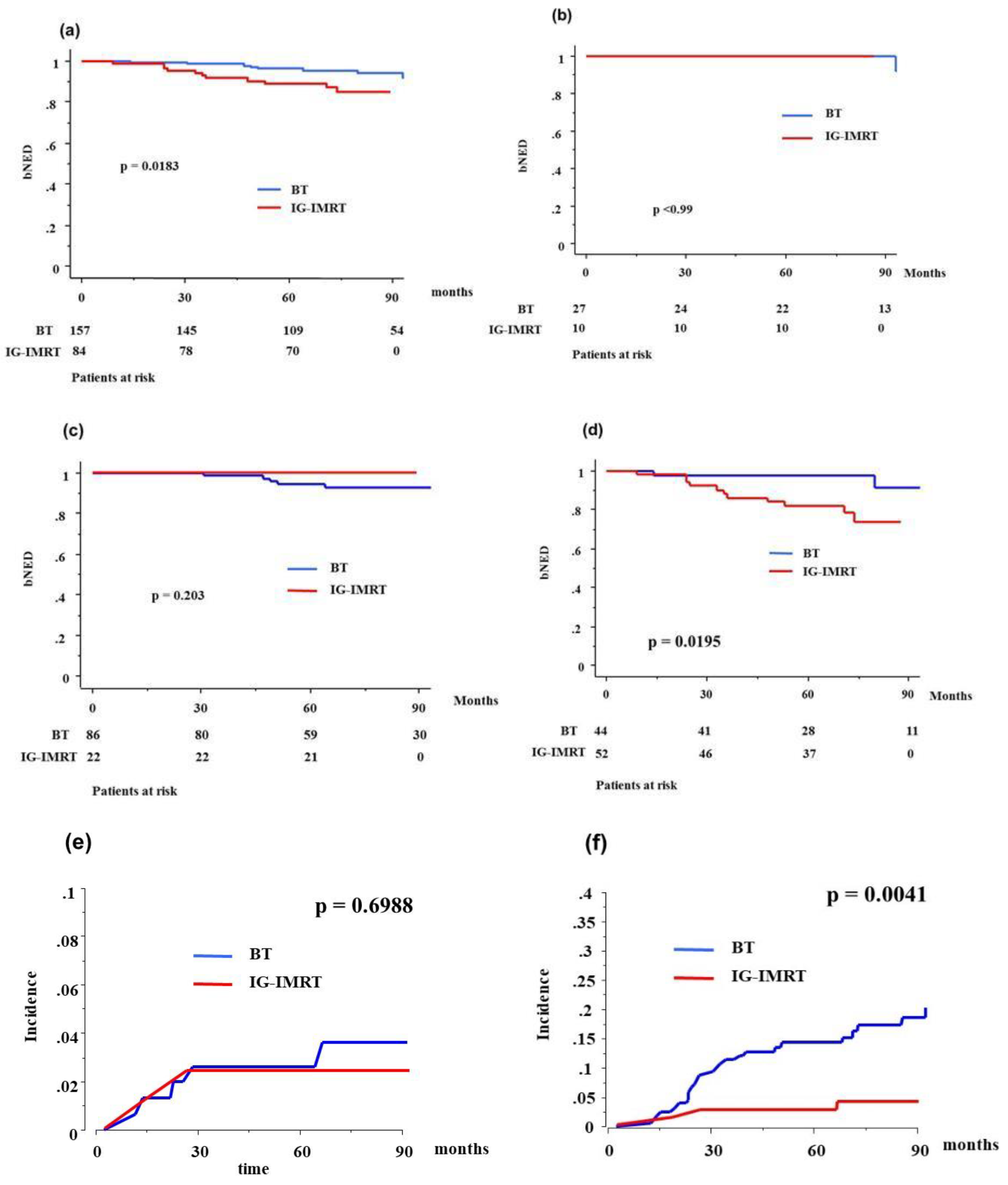
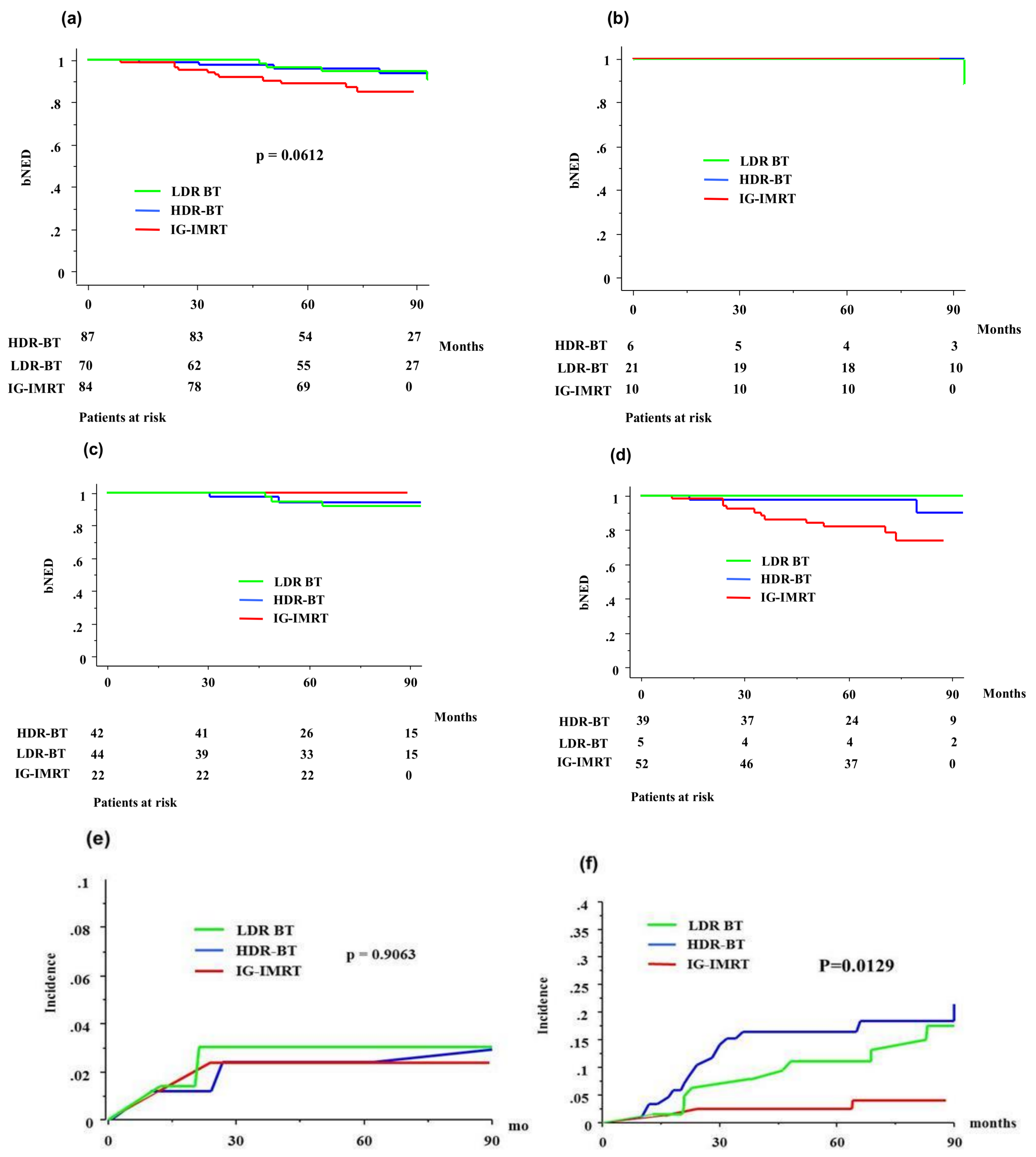
3.2. Biochemical Control and Survival in Elderly Patients after BT or IG-IMRT
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Wang, H.K.; Qu, Y.Y.; Ye, D.W. Prostate cancer in East Asia: Evolving trend over the last decade. Asian J. Androl. 2015, 17, 48–57. [Google Scholar] [PubMed]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®)—Prostate Cancer 2016, version 4; National Comprehensive Cancer Network: Fort Washington, PA, USA, 2016. [Google Scholar]
- Droz, J.P.; Albrand, G.; Gillessen, S.; Hughes, S.; Mottet, N.; Oudard, S.; Payne, H.; Puts, M.; Zulian, G.; Balducci, L.; et al. Management of prostate cancer in elderly patients: Recommendations of a task force of the international society of geriatric oncology. Eur. Urol. 2017, 72, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Hamdy, F.C.; Donovan, J.L.; Lane, J.A.; Mason, M.; Metcalfe, C.; Holding, P.; Davis, M.; Peters, T.J.; Turner, E.L.; Martin, R.M. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N. Engl. J. Med. 2016, 375, 1415–1424. [Google Scholar] [CrossRef] [PubMed]
- Lu-Yao, G.L.; Albertsen, P.C.; Moore, D.F.; Lin, Y.; DiPaola, R.S.; Yao, S.L. Fifteen-year outcomes following conservative management among men aged 65 years or older with localized prostate cancer. Eur. Urol. 2015, 68, 805–811. [Google Scholar] [CrossRef] [PubMed]
- Wilt, T.J.; Jones, K.M.; Barry, M.J.; Andriole, G.L.; Culkin, D.; Wheeler, T.; Aronson, W.J.; Brawer, M.K. Follow-up of prostatectomy versus observation for early prostate cancer. N. Engl. J. Med. 2017, 377, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Bill-Axelson, A.; Holmberg, L.; Ruutu, M.; Garmo, H.; Stark, J.R.; Busch, C.; Nordling, S.; Häggman, M.; Andersson, S.-O.; Bratell, S.; et al. Radical prostatectomy versus watchful waiting in early prostate cancer. N. Engl. J. Med. 2011, 364, 1708–1717. [Google Scholar] [CrossRef] [PubMed]
- Lu-Yao, G.L.; Kim, S.; Moore, D.F.; Shih, W.; Lin, Y.; DiPaola, R.S.; Shen, S.; Zietman, A.; Yao, S.-L. Primary radiotherapy vs. conservative management for localized prostate cancer—A population-based study. Prostate Cancer Prostatic Dis. 2015, 18, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Dell’Oglio, P.; Boehm, K.; Trudeau, V.; Tian, Z.; Larcher, A.; Leyh-Bannurah, S.R.; Moschini, M.; Capitanio, U.; Shariat, S.F.; Briganti, A.; et al. Survival after conservative management versus external beam radiation therapy in elderly patients with localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 1037–1045. [Google Scholar] [CrossRef] [PubMed]
- Wong, Y.N.; Mitra, N.; Hudes, G.; Localio, R.; Schwartz, J.S.; Wan, F.; Montagnet, C.; Armstrong, K. Survival associated with treatment vs. observation of localized prostate cancer in elderly men. JAMA 2006, 296, 2683–2693. [Google Scholar] [CrossRef] [PubMed]
- Potosky, A.L.; Haque, R.; Cassidy-Bushrow, A.E.; Ulcickas-Yood, M.; Jiang, M.; Tsai, H.T.; Luta, G.; Keating, N.L.; Smith, M.R.; Van Den Eeden, S.K. Effectiveness of primary androgen-deprivation therapy for clinically localized prostate cancer. J. Clin. Oncol. 2014, 32, 1324–1330. [Google Scholar] [CrossRef] [PubMed]
- Chin, J.; Rumble, R.B.; Kollmeier, M.; Heath, E.; Efstathiou, J.; Dorff, T.; Berman, B.; Feifer, A.; Jacques, A.; Loblaw, D.A. Brachytherapy for patients with prostate cancer: American Society of Clinical Oncology/Cancer Care Ontario Joint guideline update. J. Clin. Oncol. 2017, 35, 1737–1743. [Google Scholar] [CrossRef] [PubMed]
- Morris, W.J.; Tyldesley, S.; Rodda, S.; Halperin, R.; Pai, H.; McKenzie, M.; Duncan, G.; Morton, G.; Hamm, J.; Murray, N. Androgen suppression combined with elective nodal and dose escalated radiation therapy (the ASCENDE-RT Trial): An analysis of survival endpoints for a randomized trial comparing a low-dose-rate brachytherapy boost to a dose-escalated external beam boost for high- and intermediate-risk prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 275–285. [Google Scholar] [PubMed]
- Yamada, Y.; Masui, K.; Iwata, T.; Naitoh, Y.; Yamada, K.; Miki, T.; Okihara, K. Permanent prostate brachytherapy and short-term androgen deprivation for intermediate-risk prostate cancer in Japanese men: Outcome and toxicity. Brachytherapy 2015, 14, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Okihara, K.; Kobayashi, K.; Iwata, T.; Naitoh, Y.; Kamoim, K.; Kawauchim, A.; Yamadam, K.; Mikim, T. Assessment of permanent brachytherapy combined with androgen deprivation therapy in an intermediate-risk prostate cancer group without a Gleason score of 4 + 3: A single Japanese institutional experience. Int. J. Urol. 2014, 21, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, Y.; Nose, T.; Yoshida, K.; Inoue, T.; Yamazaki, H.; Tanaka, E.; Shiomi, H.; Imai, A.; Nakamura, S.; Shimamoto, S.; et al. High-dose-rate interstitial brachytherapy as a monotherapy for localized prostate cancer: Treatment description and preliminary results of a phase I/II clinical trial. Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, 675–681. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, K.; Yamazaki, H.; Takenaka, T.; Kotsuma, T.; Yoshida, M.; Masui, K.; Yoshioka, Y.; Narumi, Y.; Oka, T.; Tanaka, E. High-dose-rate interstitial brachytherapy in combination with androgen deprivation therapy for prostate cancer: Are high-risk patients good candidates? Strahlenther Onkol. 2014, 190, 1015–1020. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, D.; Yamazaki, H.; Nishimura, T.; Aibe, N.; Okabe, H. Long-term tumor control and late toxicity in patients with prostate cancer receiving hypofractionated (2.2 Gy) soft-tissue-matched image-guided intensity-modulated radiotherapy. Anticancer Res. 2017, 37, 5829–5835. [Google Scholar] [PubMed]
- Yamazaki, H.; Masui, K.; Suzuki, G.; Nakamura, S.; Shimizu, D.; Nishikawa, T.; Okabe, H.; Yoshida, K.; Kotsuma, T.; Tanaka, E.; et al. High-dose-rate brachytherapy monotherapy versus image-guided intensity-modulated radiotherapy with helical tomotherapy for patients with localized prostate cancer. Cancers 2018, 10, 322. [Google Scholar] [CrossRef] [PubMed]
- Tsubokura, T.; Yamazaki, H.; Masui, K.; Sasaki, N.; Shimizu, D.; Suzuki, G.; Nakamura, S.; Yamada, K.; Okihara, K.; Shiraishi, T.; et al. Comparison of image-guided intensity-modulated radiotherapy and low-dose rate brachytherapy with or without external beam radiotherapy in patients with localized prostate cancer. Sci. Rep. 2018, 8, 10538. [Google Scholar] [CrossRef] [PubMed]
- Bittner, N.H.; Orio, P.F., 3rd; Merrick, G.S.; Prestidge, B.R.; Hartford, A.C.; Rosenthal, S.A. The American College of Radiology and the American Brachytherapy Society practice parameter for transperineal permanent brachytherapy of prostate cancer. Brachytherapy 2017, 16, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Cooperberg, M.R.; Broering, J.M.; Carroll, P.R. Time trends and local variation in primary treatment of localized prostate cancer. J. Clin. Oncol. 2010, 28, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Lunardi, P.; Ploussard, G.; Grosclaude, P.; Roumiguié, M.; Soulié, M.; Beauval, J.B.; Malavaud, B. Current impact of age and comorbidity assessment on prostate cancer treatment choice and over/undertreatment risk. World J. Urol. 2017, 35, 587–593. [Google Scholar] [CrossRef] [PubMed]
- Zamboglou, N.; Tselis, N.; Baltas, D.; Buhleier, T.; Martin, T.; Milickovic, N.; Papaioannou, S.; Ackermann, H.; Tunn, U.W. High-dose-rate interstitial brachytherapy as monotherapy for clinically localized prostate cancer: Treatment evolution and mature results. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Hoskin, P.; Rojas, A.; Lowe, G.; Bryant, L.; Ostler, P.; Hughes, R.; Milner, J.; Cladd, H. High-dose-rate brachytherapy alone for localized prostate cancer in patients at moderate or high risk of biochemical recurrence. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 1376–1384. [Google Scholar] [CrossRef] [PubMed]
- Prada, P.J.; Cardenal, J.; Blanco, A.G.; Anchuelo, J.; Ferri, M.; Fernández, G.; Arrojo, E.; Vázquez, A.; Pacheco, M.; Fernández, J. High-dose-rate interstitial brachytherapy as monotherapy in one fraction for the treatment of favorable stage prostate cancer: Toxicity and long-term biochemical results. Radiother. Oncol. 2016, 119, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, A.S.; Stanford, J.L.; Gilliland, F.D.; Albertsen, P.C.; Stephenson, R.A.; Hoffman, R.M.; Eley, J.W.; Harlan, L.C.; Potosky, A.L. Health outcomes after external-beam radiation therapy for clinically localized prostate cancer: Results from the Prostate Cancer Outcomes Study. J. Clin. Oncol. 2001, 19, 2517–2526. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, A.V.; Chen, M.H.; Renshaw, A.A.; Loffredo, M.; Kantoff, P.W. Androgen suppression and radiation vs radiation alone for prostate cancer: A randomized trial. JAMA 2008, 299, 289–295. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Strata | Elder (Age ≥75) n = 241 | Control (Age ≤74) n = 867 | p-Value | ||
|---|---|---|---|---|---|---|
| N or Median (Range) | (%) | N or Median (Range) | (%) | |||
| Age | 77 (75–86) | 68 (45–74) | NA | |||
| T category | 1 | 73 | (30%) | 350 | (40%) | 0.008 |
| 2 | 124 | (51%) | 381 | (44%) | ||
| 3 | 44 | (18%) | 126 | (15%) | ||
| 4 | 0 | (0%) | 10 | (1%) | ||
| Pretreatment PSA | ng/mL | 9.70 (1.971–245) | 8.26 (1.4–658) | 0.0312 | ||
| Gleason score | ≤6 | 82 | (34%) | 399 | (46%) | 0.0005 |
| 7 | 93 | (39%) | 314 | (36%) | ||
| ≥8 | 66 | (27%) | 154 | (18%) | ||
| NCCN risk classification | Low | 37 | (15%) | 232 | (27%) | 0.0008 |
| Intermediate | 108 | (45%) | 341 | (39%) | ||
| High | 96 | (40%) | 274 | (32%) | ||
| Treatment modality | IG-IMRT | 84 | (35%) | 186 | (21%) | <0.0001 |
| Brachytherapy | 157 | (65%) | 681 | (79%) | ||
| HDR-BT | 87 | (36%) | 265 | (31%) | ||
| LDR-BT | 70 | (29%) | 416 | (48%) | ||
| Hormonal therapy | Yes | 159 | (66%) | 447 | (52%) | <0.0001 |
| No | 82 | (34%) | 420 | (48%) | ||
| Follow-up | Months | 74 (14.5–161) | 83.4 (12–216) | <0.0001 | ||
| Variable | Strata | Biochemical Control | |||||
|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | ||||||
| HR | 95% CIs | p | HR | 95% CIs | p | ||
| Age (years) | <75 | 1 | (referent) | - | 1 | (referent) | - |
| ≥75 | 1.232 | 0.752–2.020 | 0.407 | 1.309 | 0.793–2.162 | 0.2923 | |
| T classification | T1–2 | 1 | (referent) | - | 1 | (referent) | - |
| T3–4 | 2.313 | 1.551–3.449 | <0.0001 | 1.676 | 0.989–2.840 | 0.0548 | |
| Gleason score | <7 | 1 | (referent) | - | 1 | (referent) | - |
| ≥8 | 0.605 | 0.398–0.919 | 0.0186 | 0.838 | 0.526–1.336 | 0.4584 | |
| Pretreatment PSA (ng/mL) | <20 | 1 | (referent) | - | 1 | (referent) | - |
| ≥20 | 0.399 | 0.270–0.590 | <0.0001 | 0.481 | 0.293–0.791 | 0.0039 | |
| NCCN risk classification | Low | 1 | (referent) | - | NA | ||
| Intermediate | 1.642 | 0.907–2.973 | 0.1018 | ||||
| High | 3.211 | 1.820–2.973 | <0.0001 | ||||
| Hormonal therapy | No | 1 | (referent) | - | 1 | (referent) | - |
| Yes | 0.832 | 0.574–1.205 | 0.3302 | 1.426 | 0.903–2.252 | 0.128 | |
| Treatment modalities | IG-IMRT | 1 | (referent) | - | 1 | (referent) | - |
| BT | 0.555 | 0.366–0.841 | 0.0055 | 0.603 | 0.391–0.929 | 0.0219 | |
| Toxicities | Strata | Control (Age ≤74) | Elder (Age ≥75) | p-Value | ||
|---|---|---|---|---|---|---|
| n = 867 | n = 241 | |||||
| Gastrointestinal | 0 | 759 | (88%) | 216 | (90%) | 0.4722 |
| 1 | 80 | (9%) | 18 | (7%) | ||
| 2 | 22 | (3%) | 7 | (3%) | ||
| 3 | 6 | (0.7%) | 0 | (0%) | ||
| Genitourinary | 0 | 480 | (55%) | 139 | (58%) | 0.7958 |
| 1 | 260 | (30%) | 71 | (29%) | ||
| 2 | 114 | (13%) | 29 | (12%) | ||
| 3 | 13 | (1.5%) | 2 | (1%) | ||
| Variables | Strata | IG-IMRT n = 84 | Brachytherapy n = 157 | p-Value | ||
|---|---|---|---|---|---|---|
| N or Median (Range) | (%) | N or Median (Range) | (%) | |||
| Age | 77 (75–86) | 76 (75–86) | 0.0127 | |||
| T category | 1 | 23 | (27%) | 50 | (32%) | 0.0727 |
| 2 | 39 | (46%) | 85 | (54%) | ||
| 3 | 22 | (26%) | 22 | (14%) | ||
| 4 | 0 | (0%) | 0 | (0%) | ||
| Pretreatment PSA | ng/mL | 10.0 (4.3–245) | 9.4 (1.9–98.6) | 0.1644 | ||
| Gleason score | ≤6 | 23 | (27%) | 59 | (38%) | <0.0001 |
| 7 | 23 | (27%) | 70 | (45%) | ||
| ≥8 | 38 | (45%) | 28 | (18%) | ||
| NCCN risk classification | Low | 10 | (12%) | 27 | (17%) | <0.0001 |
| Intermediate | 22 | (26%) | 86 | (55%) | ||
| High | 52 | (62%) | 44 | (28%) | ||
| Treatment modality | HDR-BT | 87 | (61%) | NA | ||
| LDR-BT | 70 | (39%) | ||||
| Hormonal therapy | Yes | 64 | (76%) | 95 | (61%) | 0.0211 |
| No | 20 | (24%) | 62 | (39%) | ||
| Follow-up | Months | 73.4 (24–90) | 77.3 (14.5–161) | 0.0312 | ||
| Variables | Strata | HDR-BT n = 87 | LDR-BT n = 70 | p-Value | ||
|---|---|---|---|---|---|---|
| N or Median (Range) | (%) | N or Median (Range) | (%) | |||
| Age | 76 (75–86) | 77 (75–83) | 0.4342 | |||
| T category | 1 | 21 | (24%) | 29 | (41%) | <0.0001 |
| 2 | 45 | (52%) | 40 | (57%) | ||
| 3 | 21 | (24%) | 1 | (1%) | ||
| 4 | 0 | (0%) | 0 | (0%) | ||
| Pretreatment PSA | ng/mL | 10.8 (1.97–98.6) | 7.45 (3.56–26) | 0.0002 | ||
| Gleason score | ≤6 | 26 | (30%) | 33 | (47%) | 0.0024 |
| 7 | 38 | (44%) | 32 | (46%) | ||
| ≥8 | 23 | (26%) | 5 | (7%) | ||
| NCCN risk classification | Low | 6 | (45%) | 21 | (7%) | <0.0001 |
| Intermediate | 42 | (48%) | 44 | (63%) | ||
| High | 39 | (7%) | 5 | (30%) | ||
| Hormonal therapy | Yes | 72 | (83%) | 47 | (67%) | <0.0001 |
| No | 15 | (17%) | 23 | (33%) | ||
| Follow-up | Months | 72.2 (20–161) | 83.7 (14.5–143) | 0.2622 | ||
| Toxicities | Strata | BT n = 157 | IG-IMRT n = 84 | p-Value | ||
|---|---|---|---|---|---|---|
| N (%) | N (%) | |||||
| Gastrointestinal | 0 | 140 | (89%) | 76 | (90%) | 0.9257 |
| 1 | 12 | (8%) | 6 | (7%) | ||
| 2 | 5 | (3%) | 2 | (2%) | ||
| 3 | 0 | (0%) | 0 | (0%) | ||
| Genitourinary | 0 | 70 | (45%) | 69 | (82%) | <0.0001 |
| 1 | 59 | (38%) | 12 | (14%) | ||
| 2 | 27 | (17%) | 2 | (2%) | ||
| 3 | 1 | (1%) | 1 | (0.4%) | ||
| Toxicities | Strata | HDR-BT n = 87 | LDR-BT n = 70 | p-Value | ||
|---|---|---|---|---|---|---|
| N (%) | N (%) | |||||
| Gastrointestinal | 0 | 76 | (87%) | 64 | (91%) | 0.6943 |
| 1 | 8 | (9%) | 4 | (6%) | ||
| 2 | 3 | (3%) | 2 | (3%) | ||
| 3 | 0 | (0%) | 0 | (0%) | ||
| Genitourinary | 0 | 42 | (48%) | 28 | (40%) | 0.3804 |
| 1 | 28 | (32%) | 31 | (44%) | ||
| 2 | 16 | (18%) | 11 | (16%) | ||
| 3 | 1 | (1%) | 0 | (0%) | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamazaki, H.; Masui, K.; Suzuki, G.; Nakamura, S.; Aibe, N.; Shimizu, D.; Nishikawa, T.; Okabe, H.; Yoshida, K.; Kotsuma, T.; et al. Radiotherapy for Elderly Patients Aged ≥75 Years with Clinically Localized Prostate Cancer—Is There a Role of Brachytherapy? J. Clin. Med. 2018, 7, 424. https://doi.org/10.3390/jcm7110424
Yamazaki H, Masui K, Suzuki G, Nakamura S, Aibe N, Shimizu D, Nishikawa T, Okabe H, Yoshida K, Kotsuma T, et al. Radiotherapy for Elderly Patients Aged ≥75 Years with Clinically Localized Prostate Cancer—Is There a Role of Brachytherapy? Journal of Clinical Medicine. 2018; 7(11):424. https://doi.org/10.3390/jcm7110424
Chicago/Turabian StyleYamazaki, Hideya, Koji Masui, Gen Suzuki, Satoaki Nakamura, Norihiro Aibe, Daisuke Shimizu, Tatsuyuki Nishikawa, Haruumi Okabe, Ken Yoshida, Tadayuki Kotsuma, and et al. 2018. "Radiotherapy for Elderly Patients Aged ≥75 Years with Clinically Localized Prostate Cancer—Is There a Role of Brachytherapy?" Journal of Clinical Medicine 7, no. 11: 424. https://doi.org/10.3390/jcm7110424