Angiopoietin-2: A Potential Mediator of the Glycocalyx Injury in Adult Nephrotic Patients


Abstract
:1. Introduction
2. Methods
2.1. Subjects
2.2. Laboratory Analysis
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Syndecan-1 in Nephrotic Patients
3.3. Angiopoietin-2 is Closely Associated with Syndecan-1 and LDL-Cholesterol
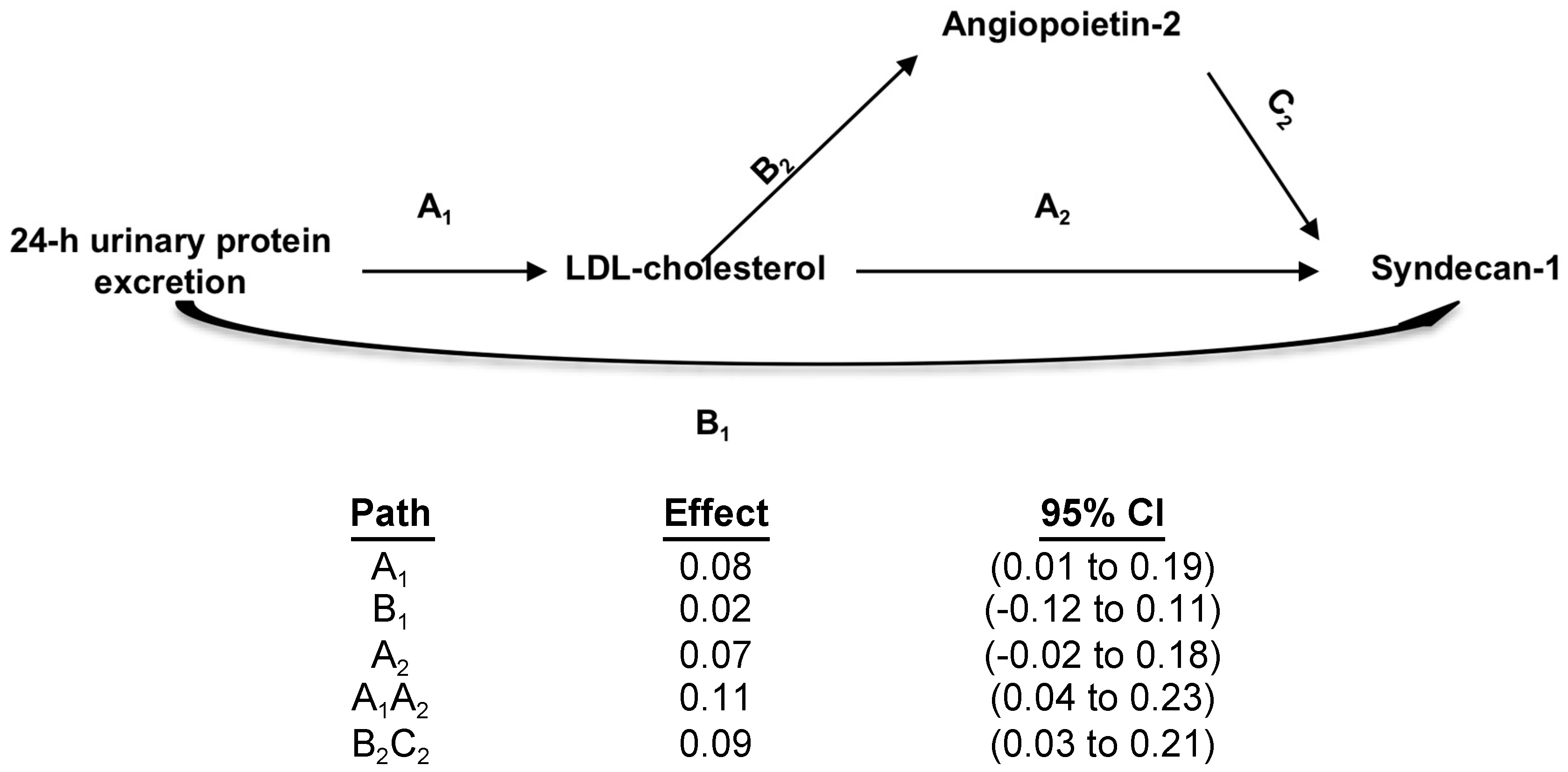
3.4. Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kidney Disease Improving Global Outcomes. KDIGO Clinical Practice Guideline for Glomerulonephritis. 2012. Available online: http://www.kdigo.org/clinical_practice_guidelines/pdf/KDIGO-GN-Guideline.pdf (accessed on 20 September 2018).
- Tian, X.; Ishibe, S. Targeting the podocyte cytoskeleton: From pathogenesis to therapy in proteinuric kidney disease. Nephrol. Dial. Transpl. 2016, 31, 1577–1583. [Google Scholar] [CrossRef] [PubMed]
- Salmito, F.T.S.; de Oliveira Neves, F.M.; Meneses, G.C.; de Almeida Leitão, R.; Martins, A.M.C.; Libório, A.B. Glycocalyx injury in adults with nephrotic syndrome: Association with endothelial function. Clin. Chim. Acta 2015, 447, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Ordoñez, J.D.; Hiatt, R.; Killebrew, E.J.; Fireman, B.H. The increased risk of coronary heart disease associated with nephrotic syndrome. Kidney Int. 1993, 44, 638–642. [Google Scholar] [CrossRef] [PubMed]
- Theodorou, K.; Boon, R. Endothelial cell metabolism in atherosclerosis. Front. Cell Dev. Biol. 2018, 6, 82. [Google Scholar] [CrossRef] [PubMed]
- Thomas, M.; Augustin, H.G. The role of the angiopoietins in vascular morphogenesis. Angiogenesis 2009, 12, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Davis, B.; Dei Cas, A.; Long, D.A.; White, K.E.; Hayward, A.; Ku, C.-H.; Woolf, A.S.; Bilous, R.; Viberti, G.; Gnudi, L. Podocyte-Specific Expression of Angiopoietin-2 Causes Proteinuria and Apoptosis of Glomerular Endothelia. J. Am. Soc. Nephrol. 2007, 18, 2320–2329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padberg, J.S.; Wiesinger, A.; di Marco, G.S.; Reuter, S.; Grabner, A.; Kentrup, D.; Lukasz, A.; Oberleithner, H.; Pavenstädt, H.; Brand, M.; et al. Damage of the endothelial glycocalyx in chronic kidney disease. Atherosclerosis 2014, 234, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Lange, T.; Hansen, K.W.; Sørensen, R.; Galatius, S. Applied mediation analyses: A review and tutorial. Epidemiol. Health 2017, 39, e2017035. [Google Scholar] [CrossRef] [PubMed]
- Woodard, T.; Sigurdsson, S.; Gotal, J.D.; Torjesen, A.A.; Inker, L.A.; Aspelund, T.; Eiriksdottir, G.; Gudnason, V.; Harris, T.B.; Launer, L.J.; et al. Mediation Analysis of Aortic Stiffness and Renal Microvascular Function. J. Am. Soc. Nephrol. 2015, 26, 1181–1187. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A. Introduction to Mediation, Moderation, and Conditional Process Analysis; The Guilford Press: New York, NY, USA, 2013; pp. 3–4. [Google Scholar]
- David, S.; Kümpers, P.; Lukasz, A.; Fliser, D.; Martens-Lobenhoffer, J.; Bode-Böger, S.M.; Kliem, V.; Haller, H.; Kielstein, J.T. Circulating angiopoietin-2 levels increase with progress of chronic kidney disease. Nephrol. Dial. Transplant. 2010, 25, 2571–2579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, F.C.; Lai, T.S.; Chiang, C.K.; Chen, Y.M.; Wu, M.S.; Chu, T.S.; Wu, K.D.; Lin, S.L. Angiopoietin-2 Is Associated with Albuminuria and Microinflammation in Chronic Kidney Disease. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Monach, P.A.; Kümpers, P.; Lukasz, A.; Tomasson, G.; Specks, U.; Stone, J.H.; Cuthbertson, D.; Krischer, J.; Carette, S.; Ding, L.; et al. Circulating angiopoietin-2 as a biomarker in ANCA-associated vasculitis. PLoS ONE 2012, 7. [Google Scholar] [CrossRef] [PubMed]
- Rasul, S.; Reiter, M.H.; Ilhan, A.; Lampichler, K.; Wagner, L.; Kautzky-Willer, A. Circulating angiopoietin-2 and soluble Tie-2 in type 2 diabetes mellitus: A cross-sectional study. Cardiovasc. Diabetol. 2011, 10, 55. [Google Scholar] [CrossRef] [PubMed]
- El-Banawy, H.S.; Gaber, E.W.; Maharem, D.A.; Matrawy, K.A. Angiopoietin-2, endothelial dysfunction and renal involvement in patients with systemic lupus erythematosus. J. Nephrol. 2012, 25, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Woolf, A.S.; Gnudi, L.; Long, D.A. Roles of Angiopoietins in Kidney Development and Disease. J. Am. Soc. Nephrol. 2009, 20, 239–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morinaga, J.; Kadomatsu, T.; Miyata, K.; Endo, M.; Terada, K.; Tian, Z.; Sugizaki, T.; Tanigawa, H.; Zhao, J.; Zhu, S.; et al. Angiopoietin-like protein 2 increases renal fibrosis by accelerating transforming growth factor-β signaling in chronic kidney disease. Kidney Int. 2016, 89, 327–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cara-Fuentes, G.; Segarra, A.; Silva-Sanchez, C.; Wang, H.; Lanaspa, M.A.; Johnson, R.J.; Garin, E.H. Angiopoietin-like-4 and minimal change disease. PLoS ONE 2017, 12. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Shah, T.; Yang, J.; Min, D.I. Association of genetic polymorphisms of angiopoietin-like 4 with severity of posttransplant proteinuria in kidney allograft recipients. Transpl. Immunol. 2017, 40, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, N.D. Disorders of lipid metabolism in nephrotic syndrome: Mechanisms and consequences. Kidney Int. 2016, 90, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, S.; Zaritsky, J.J.; Fornoni, A.; Smoyer, W.E. Dyslipidaemia in nephrotic syndrome: Mechanisms and treatment. Nat. Rev. Nephrol. 2017, 14, 57–70. [Google Scholar] [CrossRef] [PubMed]
- Lukasz, A.; Hillgruber, C.; Oberleithner, H.; Kusche-Vihrog, K.; Pavenstädt, H.; Rovas, A.; Hesse, B.; Goerge, T.; Kümpers, P. Endothelial glycocalyx breakdown is mediated by angiopoietin-2. Cardiovasc. Res. 2017, 113, 671–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clement, L.C.; Macé, C.; Avila-Casado, C.; Joles, J.A.; Kersten, S.; Chugh, S.S. Circulating angiopoietin-like 4 links proteinuria with hypertriglyceridemia in nephrotic syndrome. Nat. Med. 2014, 20, 37–46. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Glomerulopathy Patients (n = 65) | Controls (n = 25) | p | |
|---|---|---|---|
| Age (years) | 38.1 ± 12.6 | 38.5 ± 9.6 | 0.830 |
| Gender (M/F) | 28/37 | 11/14 | 1.000 |
| Renal biopsy diagnosis | |||
| FSGS/ML | 32 | ||
| MN | 18 | ||
| IgAN | 09 | ||
| MPGN | 04 | ||
| Serum creatinine (mg/dL) | 1.1 ± 0.2 | 0.82 ± 0.1 | <0.001 |
| Serum urea (mg/dL) | 43.4 ± 28.7 | 36.2 ± 11.2 | 0.227 |
| GFR (ml/min/1.73 m2) | 87.3 ± 19.6 | 107.4 ± 9.6 | <0.001 |
| Serum albumin (g/dL) | 2.6 ± 0.9 | 4.06 ± 0.32 | <0.001 |
| Total cholesterol (mg/dL) | 297.6 ± 106.3 | 183.4 ± 26.7 | <0.001 |
| LDL cholesterol (mg/dL) | 181.4 ± 71.1 | 86.0 ± 16.5 | <0.001 |
| HDL cholesterol (mg/dL) | 56.2 ± 28.1 | 50.6 ± 9.5 | <0.001 |
| Triglycerides (mg/dL) | 261.3 ± 108.1 | 134.7 ± 27.0 | <0.001 |
| 24 h urinary protein excretion (g/1.73 m2) | 5.9 ± 2.2 | 0.08 ± 0.01 | <0.001 |
| Angiopoietin-2 (pg/mL) | 7505 ± 1354 | 862 ± 101 | <0.001 |
| Syndecan-1 (ng/mL) | 102.8 ± 36.2 | 28.2 ± 9.8 | <0.001 |
| Serum Albumin | Total Cholesterol | LDL Cholesterol | HDL Cholesterol | Triglycerides | 24 h Urinary Protein Excretion | |
|---|---|---|---|---|---|---|
| Syndecan-1 | −0.039 | 0.282 | 0.388 | 0.306 | 0.261 | 0.260 |
| p = 0.828 | p = 0.005 | p < 0.001 | p = 0.014 | p = 0.037 | p = 0.038 | |
| Angiopoietin-2 | −0.256 | 0.298 | 0.408 | 0.051 | 0.111 | 0.332 |
| p = 0.047 | p = 0.016 | p = 0.003 | p = 0.690 | p = 0.382 | p = 0.007 |
| Variable | Standardized β Coefficient | p |
|---|---|---|
| Age (years) | 1.158 | 0.041 |
| GFR (mL/min/1.73 m2) | −0.126 | 0.556 |
| Serum albumin (g/dL) | −0.204 | 0.263 |
| Total cholesterol (mg/dL) | 0.139 | 0.508 |
| LDL-cholesterol (mg/dL) | 0.469 | 0.001 |
| HDL-cholesterol (mg/dL) | 0.265 | 0.167 |
| Triglycerides (mg/dL) | 0.192 | 0.321 |
| 24 h urinary protein excretion (mg/1.73 m2) | 0.193 | 0.632 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chaves, M.M.S.; Mendes, M.d.S.; Schwermann, M.P.; Queiroz, R.; Coelho, R.F.; Salmito, F.T.S.; Meneses, G.C.; Martins, A.M.C.; Moreira, A.C.d.O.M.; Libório, A.B. Angiopoietin-2: A Potential Mediator of the Glycocalyx Injury in Adult Nephrotic Patients. J. Clin. Med. 2018, 7, 401. https://doi.org/10.3390/jcm7110401
Chaves MMS, Mendes MdS, Schwermann MP, Queiroz R, Coelho RF, Salmito FTS, Meneses GC, Martins AMC, Moreira ACdOM, Libório AB. Angiopoietin-2: A Potential Mediator of the Glycocalyx Injury in Adult Nephrotic Patients. Journal of Clinical Medicine. 2018; 7(11):401. https://doi.org/10.3390/jcm7110401
Chicago/Turabian StyleChaves, Maria Moura Santana, Matheus de Souza Mendes, Maximilian Pinho Schwermann, Raquel Queiroz, Regina Freitas Coelho, Francisco Thiago Santos Salmito, Gdayllon Cavalcante Meneses, Alice Maria Costa Martins, Ana Cristina de Oliveira Monteiro Moreira, and Alexandre Braga Libório. 2018. "Angiopoietin-2: A Potential Mediator of the Glycocalyx Injury in Adult Nephrotic Patients" Journal of Clinical Medicine 7, no. 11: 401. https://doi.org/10.3390/jcm7110401