Prognostic Factors in Adult Patients with Dengue: Developing Risk Scoring Models and Emphasizing Factors Associated with Death ≤7 Days after Illness Onset and ≤3 Days after Presentation

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Design, Patients, and Severity of Dengue
2.3. Definitions
2.4. Statistical Analysis
3. Results
3.1. Dengue Epidemic and Patient Characteristics
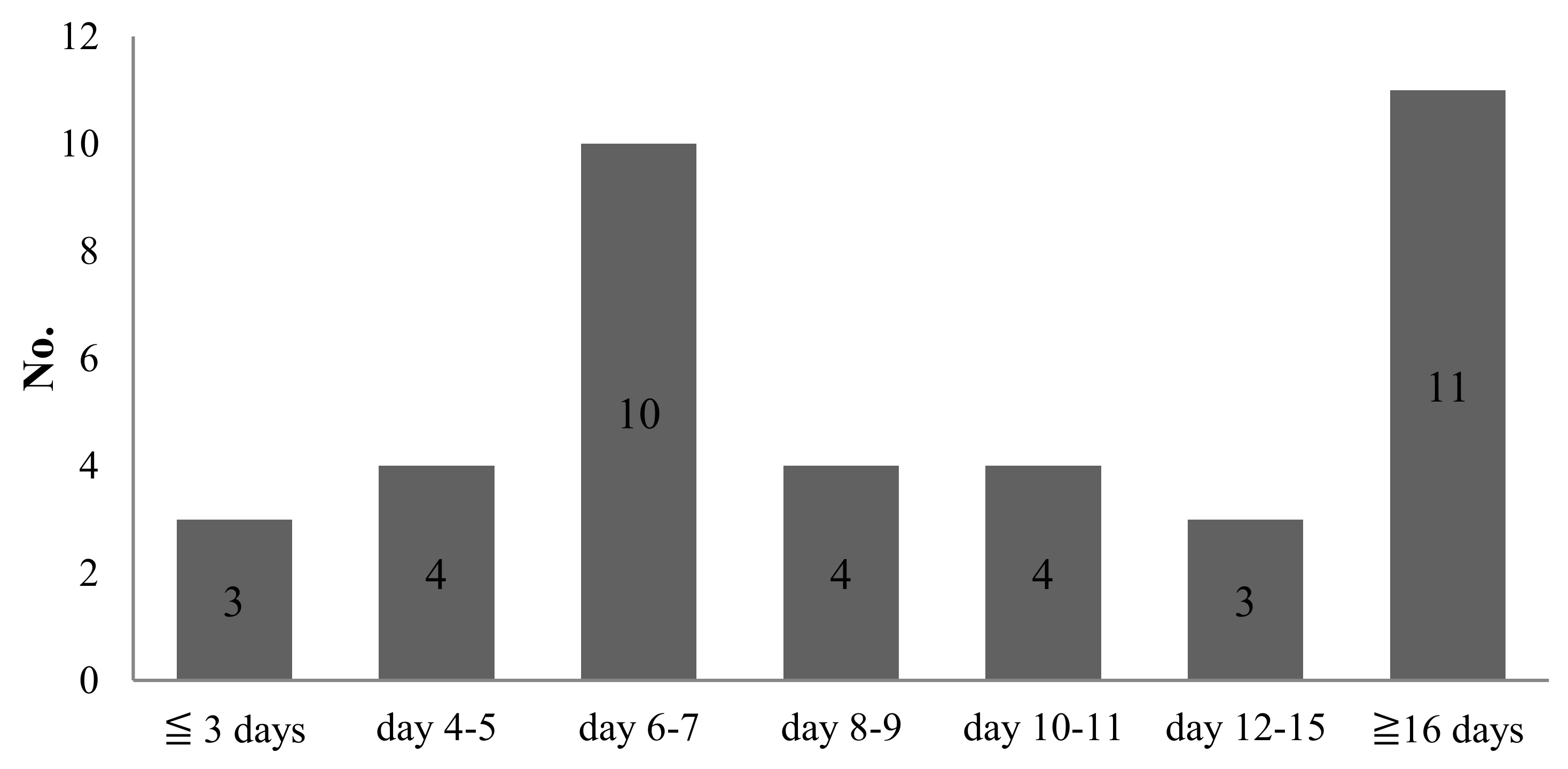
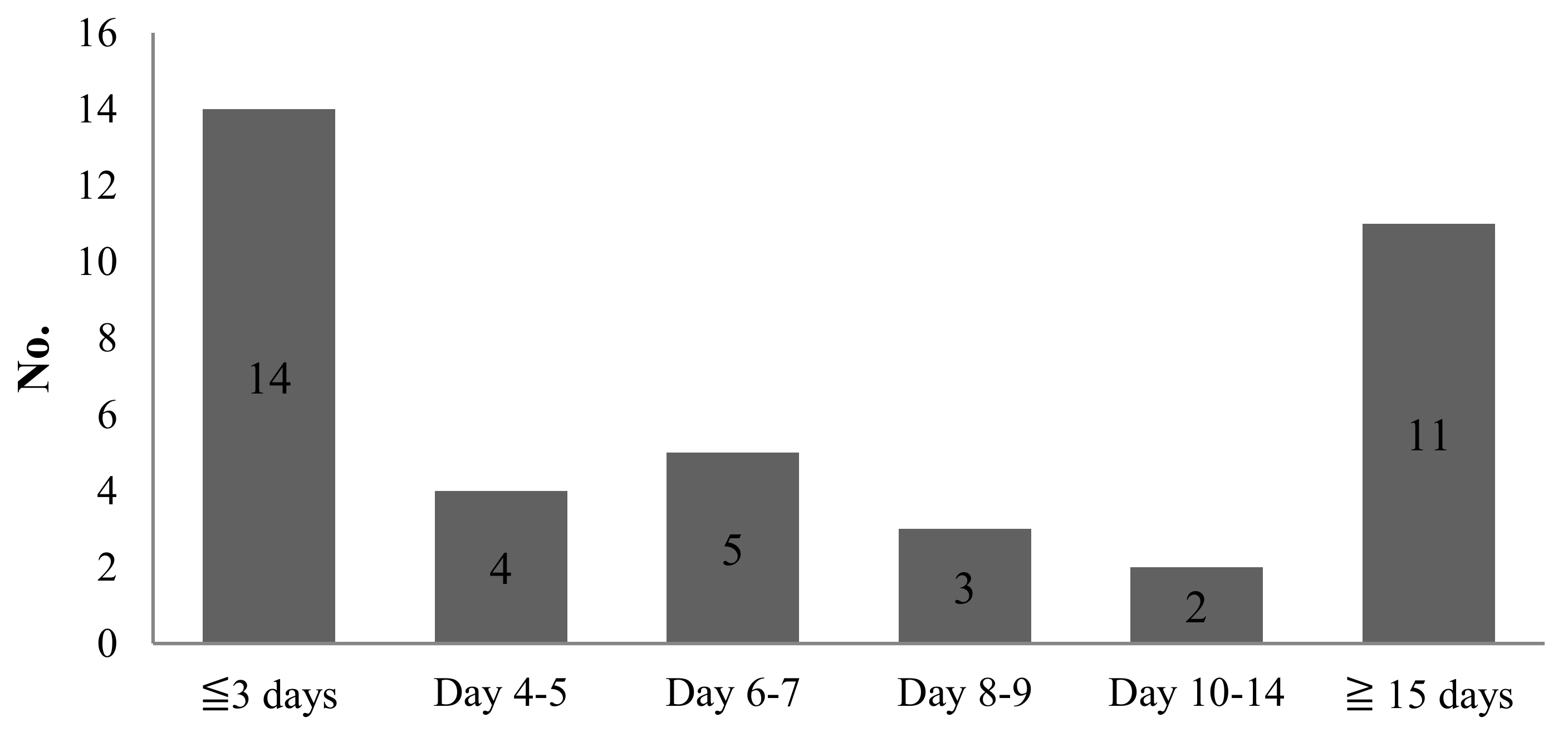
3.2. Clinical Features of Fatal Patients
3.3. Comparison between Survivors (N = 1047) and Non-Survivors (N = 39) (Table 2 and Table 3)
3.4. Comparison between Survivors (N = 1047) and Individuals Who Died ≤7 Days after Illness Onset (N = 17) (Table 2 and Table 3)
3.5. Comparison between Survivors (N = 1047) and Individuals Who Died ≤3 Days after Presentation (N = 14) (Table 2 and Table 3)
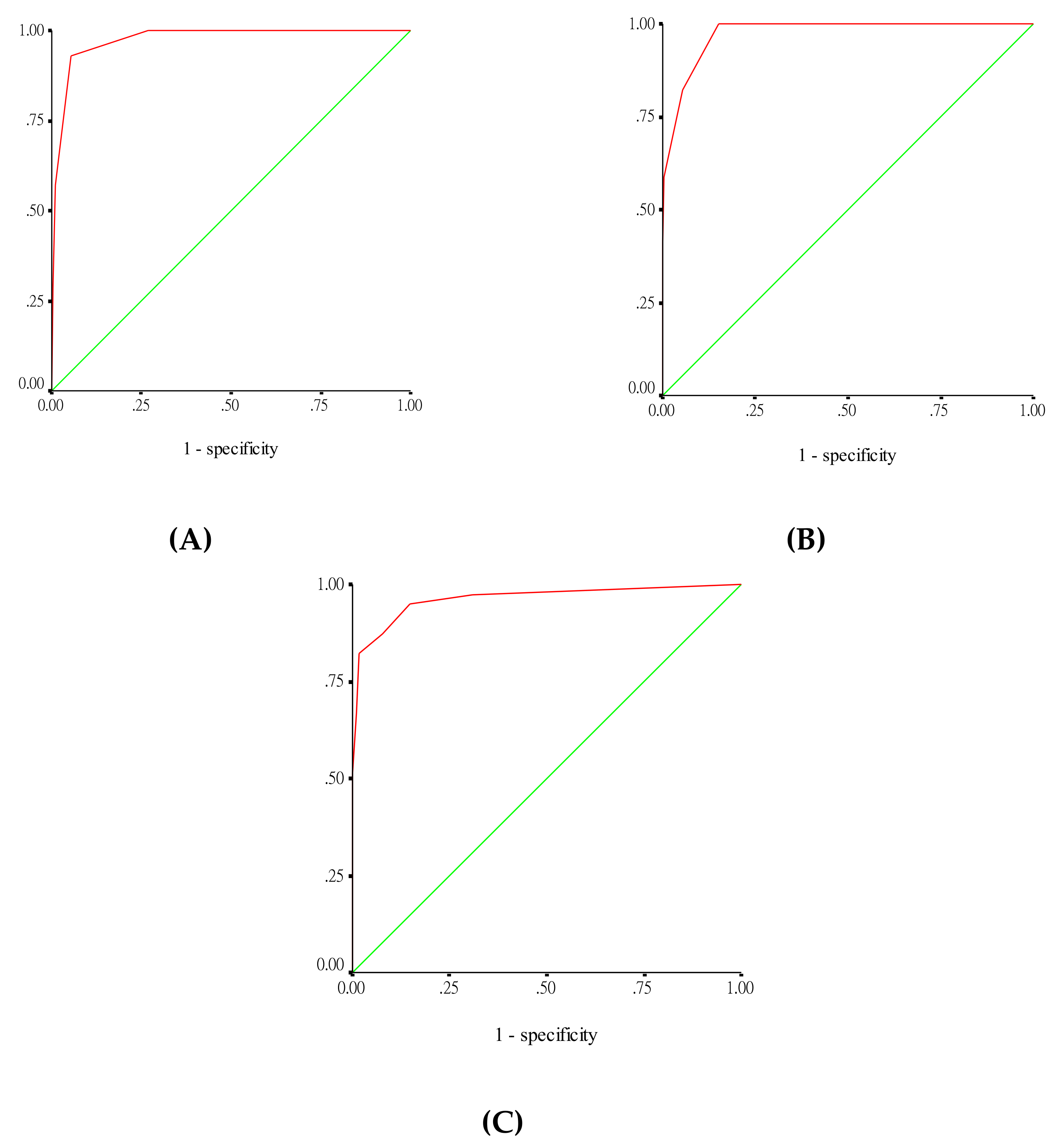
3.6. Risk Scoring Models (Table 3)
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Simmons, C.P.; Farrar, J.J.; Nguyen, V.V.; Will, B. Dengue. N. Engl. J. Med. 2012, 366, 1423–1432. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The global distribution and burden of dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control, New ed.; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Wilder-Smith, A.; Quam, M.; Sessions, O.; Rocklov, J.; Liu-Helmersson, J.; Franco, L.; Khan, K. The 2012 dengue outbreak in Madeira: exploring the origins. Euro. Surveill. 2014, 9, 19. [Google Scholar] [CrossRef]
- San Martín, J.L.; Brathwaite, O.; Zambrano, B.; Solórzano, J.O.; Bouckenooghe, A.; Dayan, G.H.; Guzmán, M.G. The epidemiology of dengue in the Americas over the last three decades: A worrisome reality. Am. J. Trop. Med. Hyg. 2010, 82, 128–135. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Dengue Haemorrhagic Fever: Diagnosis, Treatment, Prevention and Control, 2nd ed.; World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Deen, J.L.; Harris, E.; Wills, B.; Balmaseda, A.; Hammond, S.N.; Rocha, C.; Dung, N.M.; Hung, N.T.; Hien, T.T.; Farrar, J.J. The WHO dengue classification and case definitions: Time for a reassessment? Lancet 2006, 368, 170–173. [Google Scholar] [CrossRef]
- Kalayanarooj, S.; Vaughn, D.W.; Nimmannitya, S.; Green, S.; Suntayakorn, S.; Kunentrasai, N.; Viramitrachai, W.; Ratanachu-eke, S.; Kiatpolpoj, S.; Innis, B.L.; et al. Early clinical and laboratory indicators of acute dengue illness. J. Inf. Dis. 1997, 176, 313–321. [Google Scholar] [CrossRef]
- Lan, N.T.P.; Hirayama, K. Host genetic susceptibility to severe dengue infection. Trop. Med. Health 2011, 39, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Pang, J.; Salim, A.; Lee, V.J.; Hibberd, M.L.; Chia, K.S.; Leo, Y.S.; Lye, D.C. Diabetes with hypertension as risk factors for adult dengue hemorrhagic fever in a predominantly dengue serotype 2 epidemic: A case control study. PLoS Negl. Trop. Dis. 2012, 6, e1641. [Google Scholar] [CrossRef] [PubMed]
- Vu, T.T.; Holmes, E.C.; Duong, V.; Nguyen, T.Q.; Tran, T.H.; Quail, M.; Churcher, C.; Parkhill, J.; Cardosa, J.; Farrar, J.; et al. Emergence of the Asian 1 genotype of dengue virus serotype 2 in Viet Nam: In vitro fitness advantage and lineage replacement in South East Asia. PLoS Negl. Trop. Dis. 2010, 4, 1–11. [Google Scholar]
- Rigau-Perez, J.G.; Laufer, M.K. Dengue-related deaths in Puerto Rico, 1992–1996: Diagnosis and clinical alarm signals. Clin. Infect. Dis. 2006, 42, 1241–1246. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.K.; Liu, J.W.; Yang, K.D. Clinical and laboratory characteristics and risk factors for fatality in elderly patients with dengue hemorrhagic fever. Am. J. Trop. Med. Hyg. 2008, 79, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.J.; Lee, T.H.; Leo, Y.S. Dengue in the elderly: A review. Expert. Rev. Anti. Infect. Ther. 2017, 15, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Yeh, C.Y.; Chen, P.L.; Chuang, K.T.; Shu, Y.C.; Chien, Y.W.; Perng, G.C.; Ko, W.C.; Ko, N.Y. Symptoms associated with adverse dengue fever prognoses at the time of reporting in the 2015 dengue outbreak in Taiwan. PLoS. Negl. Trop. Dis. 2017, 11, e0006091. [Google Scholar] [CrossRef] [PubMed]
- Pinto, R.C.; Castro, D.B.; Albuquerque, B.C.; de Souza Sampaio, V.; Passos, R.A.; Costa, C.F.; Sadahiro, M.; Braga, J.U. Mortality predictors in patients with severe dengue in the state of amazonas, Brazil. PLoS One 2016, 11, e0161884. [Google Scholar] [CrossRef] [PubMed]
- Moraes, G.H.; Duarte, E.D.; Duarte, E.C. Determinants of mortality from severe dengue in Brazil: A population-based case-control study. Am. J. Trop. Med. Hyg. 2013, 88, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Leo, Y.S.; Thein, T.L.; Fisher, D.A.; Low, J.G.; Oh, H.M.; Narayanan, R.L.; Gan, V.C.; Lee, V.J.; Lye, D.C. Confirmed adult dengue deaths in Singapore: 5-Year multi-center retrospective study. BMC. Infect. Dis. 2011, 11, 123. [Google Scholar] [CrossRef] [PubMed]
- Tomashek, K.M.; Gregory, C.J.; Rivera, Sánchez, A.; Bartek, M.A.; Garcia Rivera, E.J.; Hunsperger, E.; Muñoz-Jordán, J.L.; Sun, W. Dengue deaths in Puerto Rico: Lessons learned from the 2007 epidemic. PLoS Negl. Trop. Dis. 2012, 6, e1614. [Google Scholar] [CrossRef] [PubMed]
- Shu, P.Y.; Chang, S.F.; Kuo, Y.C.; Yueh, Y.Y.; Chien, L.J.; Sue, C.L.; Lin, T.H.; Huang, J.H. Development of group and serotype-specific one-step SYBR Green I-based real-time reverse transcription-PCR assay for dengue virus. J. Clin. Microbiol. 2003, 41, 2408–2416. [Google Scholar] [CrossRef] [PubMed]
- Rockey, D.C. Gastrointestinal bleeding. Gastroenterol. Clin. North. Am. 2005, 34, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO Clinical practice guideline for the care of kidney transplant recipients. Am. J. Transplant 2009, 9 (Suppl 3), S1–S157. [Google Scholar] [CrossRef] [PubMed]
- Bagley, W.H.; Yang, H.; Shah, K.H. Rhabdomyolysis. Intern. Emerg. Med. 2007, 2, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Jackson, P.G. Cardiac troponins. J. Clin. Pathol. 2004, 57, 1025–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, L.M.; Massaro, J.M.; D’Agostino, R.B. Sr. Presentation of multivariate data for clinical use: The Framingham Study risk score functions. Stat. Med. 2004, 23, 1631–1660. [Google Scholar] [CrossRef] [PubMed]
- Zweig, M.H.; Campbell, G. Receiver-operating characteristic (ROC) plots: A fundamental evaluation tool in clinical medicine. Clin. Chem. 1993, 39, 561–577. [Google Scholar] [PubMed]
- Chang, K.; Huang, C.H.; Lee, I.K.; Lu, P.L.; Lin, C.Y.; Chen, T.C.; Lai, P.C.; Hsieh, H.C.; Yu, H.L.; Hung, C.H.; et al. Differences in mortality and clinical manifestations of dengue hemorrhagic fever in Taiwan in different years: A comparison for cases in 2014 and 2015 epidemics. Am. J. Trop. Med. Hyg. 2017, 97, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.C.; Lee, I.K.; Su, M.C.; Lin, H.I.; Huang, Y.C.; Liu, S.F.; Wu, C.C.; Lin, M.C. Differences in clinical and laboratory characteristics and disease severity between children and adults with dengue virus infection in Taiwan, 2002. Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 871–877. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.C.; Hsu, C.C.; Guo, H.R.; Su, S.B.; Lin, H.J. Dengue fever mortality score: A novel decision rule to predict death from dengue fever. J. Infect. 2017, 75, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Ong, A.; Sandar, M.; Chen, M.I.; Sin, L.Y. Fatal dengue hemorrhagic fever in adults during a dengue epidemic in Singapore. Int. J. Infect. Dis. 2007, 11, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Sam, S.S.; Omar, S.F.; Teoh, B.T.; Abd-Jamil, J.; AbuBakar, S. Review of Dengue hemorrhagic fever fatal cases seen among adults: a retrospective study. PLoS Negl. Trop. Dis. 2013, 7, e2194. [Google Scholar] [CrossRef] [PubMed]
- Thu, T.L.T.; Minh, D.N.; Van, N.T.; Tinh, H.T.; Van Vinh, C.N.; Wolbers, M.; Thi Hoai, T.D.; Farrar, J.; Simmons, C.; Wills, B. Clinical features of dengue in a large vietnamese cohort: Intrinsically lower platelet counts and greater risk for bleeding in adults than children. PLoS Negl. Trop. Dis. 2012, 6, e1679. [Google Scholar]
- Huang, W.C.; Lee, I.K.; Chen, Y.C.; Tsai, C.Y.; Liu, J.W. Characteristics and predictors for gastrointestinal hemorrhage among adult patients with dengue virus infection: Emphasizing the impact of existing comorbid disease(s). PLoS One. 2018, 13, e0192919. [Google Scholar] [CrossRef] [PubMed]
- Lam, P.K.; Tam, D.T.; Diet, T.V.; Tam, C.T.; Tien, N.T.; Kieu, N.T.; Simmons, C.; Farrar, J.; Nga, N.T.; Qui, P.T.; et al. Clinical characteristics of dengue shock syndrome in Vietnamese children: A 10-year prospective study in a single hospital. Clin. Infect. Dis. 2013, 57, 1577–1586. [Google Scholar] [CrossRef] [PubMed]
- Thein, T.L.; Lye, D.C.; Leo, Y.S.; Wong, J.G.; Hao, Y.; Wilder-Smith, A. Severe neutropenia in dengue patients: Prevalence and significance. Am. J. Trop. Med. Hyg. 2014, 90, 984–987. [Google Scholar] [CrossRef] [PubMed]
- Thein, T.L.; Ng, E.L.; Yeang, M.S.; Leo, Y.S.; Lye, D.C. Risk factors for concurrent bacteremia in adult patients with dengue. J. Microbiol. Immunol. Infect. 2017, 50, 314–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- See, K.C.; Phua, J.; Yip, H.S.; Yeo, L.L.; Lim, T.K. Identification of concurrent bacterial infection in adult patients with dengue. Am. J. Trop. Med. Hyg. 2013, 89, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Ruokonen, E.; Takala, J.; Kari, A.; Alhava, E. Septic shock and multiple organ failure. Crit. Care. Med. 1991, 19, 1146–1151. [Google Scholar] [CrossRef] [PubMed]
- Mallhi, T.H.; Khan, A.H.; Adnan, A.S.; Sarriff, A.; Khan, Y.H.; Jummaat, F. Incidence, characteristics and risk factors of acute kidney injury among dengue patients: A retrospective analysis. PLoS One. 2015, 10, e0138465. [Google Scholar]
- Khalil, M.A.; Tan, J.; Khalil, M.A.; Awan, S.; Rangasami, M. Predictors of hospital stay and mortality in dengue virus infection-experience from Aga Khan University Hospital Pakistan. BMC. Res. Notes. 2014, 7, 473. [Google Scholar] [CrossRef] [PubMed]
- Halstead, S.B. Neutralization and antibody-dependent enhancement of dengue viruses. Adv. Virus. Res. 2003, 60, 421–467. [Google Scholar]
- Anderson, K.B.; Gibbons, R.V.; Cummings, D.A.T.; Nisalak, A.; Green, S.; Libraty, D.H.; Jarman, R.G.; Srikiatkhachorn, A.; Mammen, M.P.; Darunee, B.; et al. A shorter time interval between first and second dengue infections is associated with protection from clinical illness in a school-based cohort in Thailand. J. Infect. Dis. 2014, 209, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Changal, K.H.; Raina, A.H.; Raina, A.; Raina, M.; Bashir, R.; Latief, M.; Mir, T.; Changal, Q.H. Differentiating secondary from primary dengue using IgG to IgM ratio in early dengue: An observational hospital based clinico-serological study from North India. BMC. Infect. Dis. 2016, 16, 715. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Included Cases (N = 1086) | |
|---|---|
| Demographic and clinical features | |
| Median age (range), years | 52 (18–91) |
| Age > 65 years | 191 (17.5) |
| Male | 513 (47.2) |
| Comorbid condition | |
| Diabetes alone | 58 (5.3) |
| Hypertension alone | 123 (11.3) |
| Diabetes and hypertension | 92 (8.4) |
| Diabetes, hypertension, and other comorbidity | 12 a (1.1) |
| End-stage renal disease alone | 3 (0.3) |
| Median time from illness onset to hospital presentation (range), days | 3 (1–10) |
| Severe dengue (2009 WHO) | 82 (7.4) |
| Fatal | 39 (3.6) |
| Symptoms and signs at presentation | |
| Fever | 1028 (94.6) |
| Myalgia | 393 (36.2) |
| Bone pain | 463 (42.6) |
| Rash | 386 (35.5) |
| Headache | 445 (41) |
| Cough | 285 (26.2) |
| Retro-orbital pain | 123 (11.3) |
| Diarrhea | 158 (14.5) |
| Abdomen pain | 236 (21.7) |
| Vomiting | 322 (29.6) |
| Drowsiness | 106 (9.7) |
| Petechiae | 251 (23.1) |
| Variable | Patients Who Survived (N = 1047) | Patients Who Died | Pa | Pb | Pc | ||
|---|---|---|---|---|---|---|---|
| ≤3 Days after Presentation (N = 14) | ≤7 Days after Onset of Dengue Illness (N = 17) | Overall (N = 39) | |||||
| Demographic and clinical features | |||||||
| Median age (range), years | 51 (18–91) | 66 (41–83) | 69 (45–86) | 66 (33–86) | <0.001 | <0.001 | <0.001 |
| Age > 65 years | 171 (16.3) | 7 (50) | 9 (52.9) | 20 (51.2) | 0.004 | 0.001 | <0.001 |
| Male | 488 (46.6) | 9 (64.3) | 11 (64.7) | 25 (64.1) | 0.281 | 0.150 | 0.034 |
| Comorbid condition | |||||||
| Diabetes alone | 54 (5.5) | 1 (7.1) | 2 (11.7) | 4 (10.2) | >0.99 | >0.99 | >0.99 |
| Hypertension alone | 115 (10.9) | 3 (21.4) | 4 (23.5) | 8 (20.5) | >0.99 | >0.99 | >0.99 |
| Diabetes and hypertension | 83 (7.9) | 2 (14.3) | 3 (17.6) | 9 (23) | >0.99 | >0.99 | >0.99 |
| Diabetes, hypertension, and other comorbidity | 5 d (0.5) | 3 e (21.4) | 5 f (29.4) | 7 g (17.9) | >0.99 | <0.001 | <0.001 |
| End-stage renal disease alone | 1 (0.1) | 0 (0) | 0 (0) | 2 (5.1) | >0.99 | >0.99 | 0.004 |
| Median time from illness onset to hospital presentation (range), days | 3 (1–10) | 3 (1–8) | 1 (1–4) | 3 (1–8) | 0.803 | 0.062 | 0.035 |
| Median time from hospital presentation to fatality (range), days | - | 3 (2–3) | 3 (2–7) | 6 (2–39) | - | - | - |
| Median time from illness onset to fatality (range), days | - | 6 (3–10) | 6 (3–7) | 9 (3–47) | - | - | - |
| Severe dengue (2009 WHO) | 43 (4.1) | 14 (100) | 17 (100) | 39 (100) | <0.001 | <0.001 | <0.001 |
| Symptoms on the day of presentation | |||||||
| Fever | 996 (95.1) | 12 (85.7) | 14 (82.4) | 32 (82) | >0.99 | 0.051 | 0.003 |
| Myalgia | 382 (36.4) | 4 (28.6) | 3 (17.6) | 11 (28.2) | 0.781 | 0.131 | 0.314 |
| Bone pain | 452 (43.1) | 5 (35.7) | 3 (17.6) | 11 (28.2) | 0.787 | 0.046 | 0.070 |
| Rash | 383 (36.5) | 2 (14.3) | 1 (5.9) | 3 (7.7) | 0.099 | 0.009 | <0.001 |
| Headache | 436 (41.6) | 3 (21.4) | 3 (17.6) | 9 (23) | 0.173 | 0.050 | 0.021 |
| Cough | 268 (25.5) | 3 (21.4) | 5 (29.4) | 17 (43.5) | >0.99 | 0.780 | 0.016 |
| Retro-orbital pain | 122 (11.6) | 1 (7.1) | 0 | 1 (2.5) | >0.99 | 0.244 | 0.116 |
| Diarrhea | 150 (14.3) | 4 (28.6) | 4 (23.5) | 8 (20.5) | >0.99 | 0.292 | 0.255 |
| Petechiae | 245 (23.4) | 2 (14.3) | 1 (5.8) | 6 (15.3) | 0.541 | 0.142 | 0.333 |
| Warning signs ≤72 hours after presentation | |||||||
| Abdomen pain | 224 (21.3) | 4 (28.6) | 6 (35.3) | 12 (30.7) | >0.99 | 0.229 | 0.168 |
| Vomiting | 314 (3) | 3 (21.4) | 6 (35.3) | 8 (20.5) | 0.573 | 0.603 | 0.283 |
| Drowsiness | 86 (8.2) | 10 (71.4) | 8 (47.1) | 20 (51.2) | <0.001 | >0.99 | <0.001 |
| Mucosal bleed | |||||||
| Gastrointestinal bleed | 79 (7.5) | 8 (57.1) | 10 (58.8) | 27 (69.2) | <0.001 | <0.001 | <0.001 |
| Hemoptysis | 19 (1.8) | 0 | 0 | 0 | >0.99 | >0.99 | >0.99 |
| Gum bleed | 90 (8.6) | 0 | 0 | 0 | 0.623 | 0.388 | 0.068 |
| Clinical fluid accumulation, no./total no. (%) | |||||||
| Pleural effusion | 65/632 (10) | 5/14 (35.7) | 5/17 (29.4) | 11/39 (28.2) | >0.99 | 0.028 | 0.002 |
| Ascites | 39/411 (9.5) | 2/14 (14.3) | 2/17 (11.8) | 6/39 (15.3) | >0.99 | >0.99 | 0.260 |
| Increase in hematocrit > 20% concurrent decrease platelet count, no./total no. (%) | 37/547(6.8) | 4/14 (28.6) | 4/14 (28.6) | 6/36 (16.6) | >0.99 | >0.99 | >0.99 |
| Laboratory data on the day of presentation | |||||||
| Leukopenia (WBC < 3 × 109 cells/L) | 341 (32.5) | 2 (14.3) | 0 (0) | 3 (7.7) | 0.248 | 0.001 | <0.001 |
| Leukocytosis (WBC > 10 × 109 cells/L) | 10 (0.9) | 4 (28.6) | 6 (35.3) | 14 (35.9) | >0.99 | <0.001 | <0.001 |
| Median hemoglobin (range) (g/dL) | 13.5 (6.4–18) (n = 965) | 12 (8.6–18.1) (n = 12) | 13 (8.3–18.1) (n = 13) | 12.9 (7.5–33.9) (n = 37) | 0.216 | 0.442 | 0.018 |
| Median hematocrit (range) (%) | 39.4 (21.4–57.2) | 36.6 (25.5–51.9) | 38.1 (24.8–51.9) | 38.1 (21.8–75) | 0.339 | 0.422 | 0.052 |
| Median platelet count (range) (×109 cells/L) | 100 (1–413) (n = 1025) | 12.5 (0.3–258) | 36 (3.6–258) | 44.1 (0.3–258) | <0.001 | 0.023 | 0.001 |
| Platelet count < 100 × 109 cells/L, no./total no. (%) | 517/1025 (50.4) | 12/14 (85.7) | 12/17 (70.5) | 27/39 (69.2) | >0.99 | >0.99 | 0.856 |
| Platelet count < 50 × 109 cells/L, no./total no. (%) | 247/1025 (24) | 10/14 (71.4) | 9/17 (52.9) | 20/39 (51.2) | <0.001 | 0.010 | <0.001 |
| Median AST (range) (IU/L) | 70.5 (11–4299) (n = 684) | 420.5 (66–2884) (n = 6) | 100 (30–4040) (n = 10) | 86.5 (20–4040) (n= 28) | 0.015 | 0.117 | 0.250 |
| Median ALT (range) (IU/L) | 48 (5–1555) (n = 597) | 177.5 (27–2491) (n = 8) | 71.5 (18–2491) (n = 12) | 67.5 (13–2491) (n = 28) | 0.037 | 0.085 | 0.301 |
| Laboratory data during hospitalization | |||||||
| Leukopenia (WBC < 3 × 109 cells/L)) | 472 (45) | 0 | 1 (5.9) | 6 (15.4) | <0.001 | 0.001 | <0.001 |
| Leukocytosis (WBC > 10 × 109 cells/L) | 62 (5.9) | 8 (57.1) | 13 (76.5) | 32 (82) | <0.001 | <0.001 | <0.001 |
| Median peak hematocrit (range) (%) | 40.4 (23.7–57.2) | 38.2 (25.5–51.9) | 41 (25.5–51.9) | 40.8 (23.1–59) | 0.300 | 0.659 | 0.584 |
| Median nadir platelet count (range) (×109 cells/L) | 58 (0.7–307) (n = 1033) | 13 (3–52) (n =13) | 15 (5–135) | 15.5 (3–303) (n = 38) | <0.001 | <0.001 | <0.001 |
| Platelet count < 100 × 109 cells/L, no./total no. (%) | 751/1033 (72.7) | 13/13 (100) | 17/17 (100) | 37/38 (97.3) | 0.025 | 0.010 | <0.001 |
| Platelet count < 50 × 109 cells/L, no./total no. (%) | 469/1033 (45.4) | 12/13 (92.3) | 13/17 (76.4) | 32/38 (84.2) | 0.001 | 0.013 | <0.001 |
| Median peak AST (range) (U/L) | 93 (10.5–3392) (n = 398) | 6577 (966–19,347) (n = 5) | 5495 (148–19,347) (n = 7) | 601 (17–19,347) (n = 12) | <0.001 | 0.001 | 0.006 |
| Median peak ALT (range) (U/L) | 73 (7–1729) (n = 407) | 1637 (758–61,620) (n = 6) | 928.5 (89–6162) (n = 8) | 446 (4–6162) (n = 13) | <0.001 | 0.001 | 0.018 |
| Complications during the entire clinical course | |||||||
| Hemoconcentration (increase hematocrit >20%) | 41 (3.9) | 7 (50) | 13 (76.5) | 30 (76.9) | <0.001 | <0.001 | <0.001 |
| Acute kidney injury | 14 (1.3) | 10 (71.4) | 12 (70.6) | 27 (69.2) | <0.001 | <0.001 | <0.001 |
| Severe hepatitis (AST or ALT >1000 IUL), no./total no. (%) | 8/784 (1) | 5/10 (50) | 6/12 (50) | 6/28 (21.4) | >0.99 | >0.99 | >0.99 |
| Bacteremia | 0 (0) | 2 (14.3) | 3 (17.6) | 11 (28.2) | <0.001 | <0.001 | <0.001 |
| Candidemia | 0 (0) | 0 (0) | 0 | 2 (5.1) | - | - | 0.036 |
| Pneumonia | 9 (0.9) | 2 (14.3) | 1 (5.9) | 7 (17.9) | >0.99 | >0.99 | >0.99 |
| Rhabdomyolysis | 6 (0.6) | 2 (14.3) | 3 (17.6) | 4 (10.2) | >0.99 | >0.99 | >0.99 |
| Myocardial injury | 2 (0.2) | 5 (35.7) | 8 (47.1) | 11 (28.2) | <0.001 | <0.001 | <0.001 |
| Variable | Adjusted Odds Ratio | 95% Confidence Interval | P | Coefficient | Risk Score Weight |
|---|---|---|---|---|---|
| Survivors (N = 1047) versus individuals who died ≤3 days after presentation (N = 14) | |||||
| Gastrointestinal bleeding ≤72 h after presentation | 15.854 | 2.911–86.356 | 0.001 | 2.763 | 1 |
| Platelet count < 50 × 109 cells/L at presentation | 18.562 | 2.521–136.668 | 0.004 | 2.921 | 1 |
| Acute kidney injury during hospitalization | 318.987 | 47.053–2162.495 | <0.001 | 5.765 | 2 |
| Survivor (N = 1047) versus individuals who died ≤7 days after illness onset (N = 17) | |||||
| Gastrointestinal bleeding ≤72 h after presentation | 8.879 | 2.024–38.961 | 0.004 | 2.184 | 1 |
| Leukocytosis during hospitalization | 19.925 | 4.875–81.443 | <0.001 | 2.992 | 1 |
| Hemoconcentration during hospitalization | 71.667 | 16.375-313.661 | <0.001 | 4.272 | 2 |
| Survivor (N = 1047) versus non-survivors (N = 39) | |||||
| Gastrointestinal bleeding ≤72 h after presentation | 20.728 | 5.089–84.426 | <0.001 | 3.031 | 2 |
| Platelet count < 50 × 109 cells/L at presentation | 5.422 | 1.398–21.025 | 0.015 | 1.690 | 1 |
| Leukocytosis during hospitalization | 12.763 | 3.788–43.003 | <0.001 | 2.547 | 2 |
| Hemoconcentration during hospitalization | 55.674 | 13.110–236.422 | <0.001 | 4.020 | 2 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, I.-K.; Huang, C.-H.; Huang, W.-C.; Chen, Y.-C.; Tsai, C.-Y.; Chang, K.; Chen, Y.-H. Prognostic Factors in Adult Patients with Dengue: Developing Risk Scoring Models and Emphasizing Factors Associated with Death ≤7 Days after Illness Onset and ≤3 Days after Presentation. J. Clin. Med. 2018, 7, 396. https://doi.org/10.3390/jcm7110396
Lee I-K, Huang C-H, Huang W-C, Chen Y-C, Tsai C-Y, Chang K, Chen Y-H. Prognostic Factors in Adult Patients with Dengue: Developing Risk Scoring Models and Emphasizing Factors Associated with Death ≤7 Days after Illness Onset and ≤3 Days after Presentation. Journal of Clinical Medicine. 2018; 7(11):396. https://doi.org/10.3390/jcm7110396
Chicago/Turabian StyleLee, Ing-Kit, Chung-Hao Huang, Wen-Chi Huang, Yi-Chun Chen, Ching-Yen Tsai, Ko Chang, and Yen-Hsu Chen. 2018. "Prognostic Factors in Adult Patients with Dengue: Developing Risk Scoring Models and Emphasizing Factors Associated with Death ≤7 Days after Illness Onset and ≤3 Days after Presentation" Journal of Clinical Medicine 7, no. 11: 396. https://doi.org/10.3390/jcm7110396