
Interventions to Increase Treatment Adherence in Pediatric Atopic Dermatitis: A Systematic Review

Abstract
:
1. Introduction
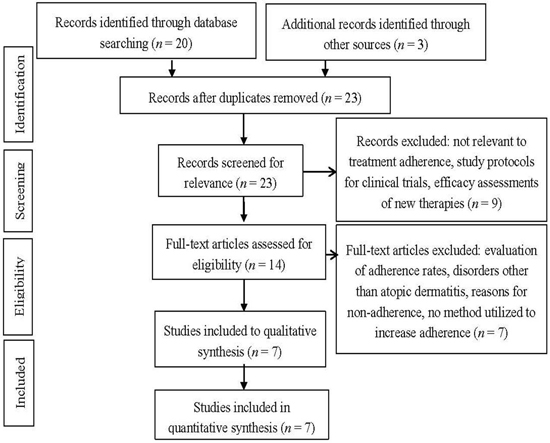
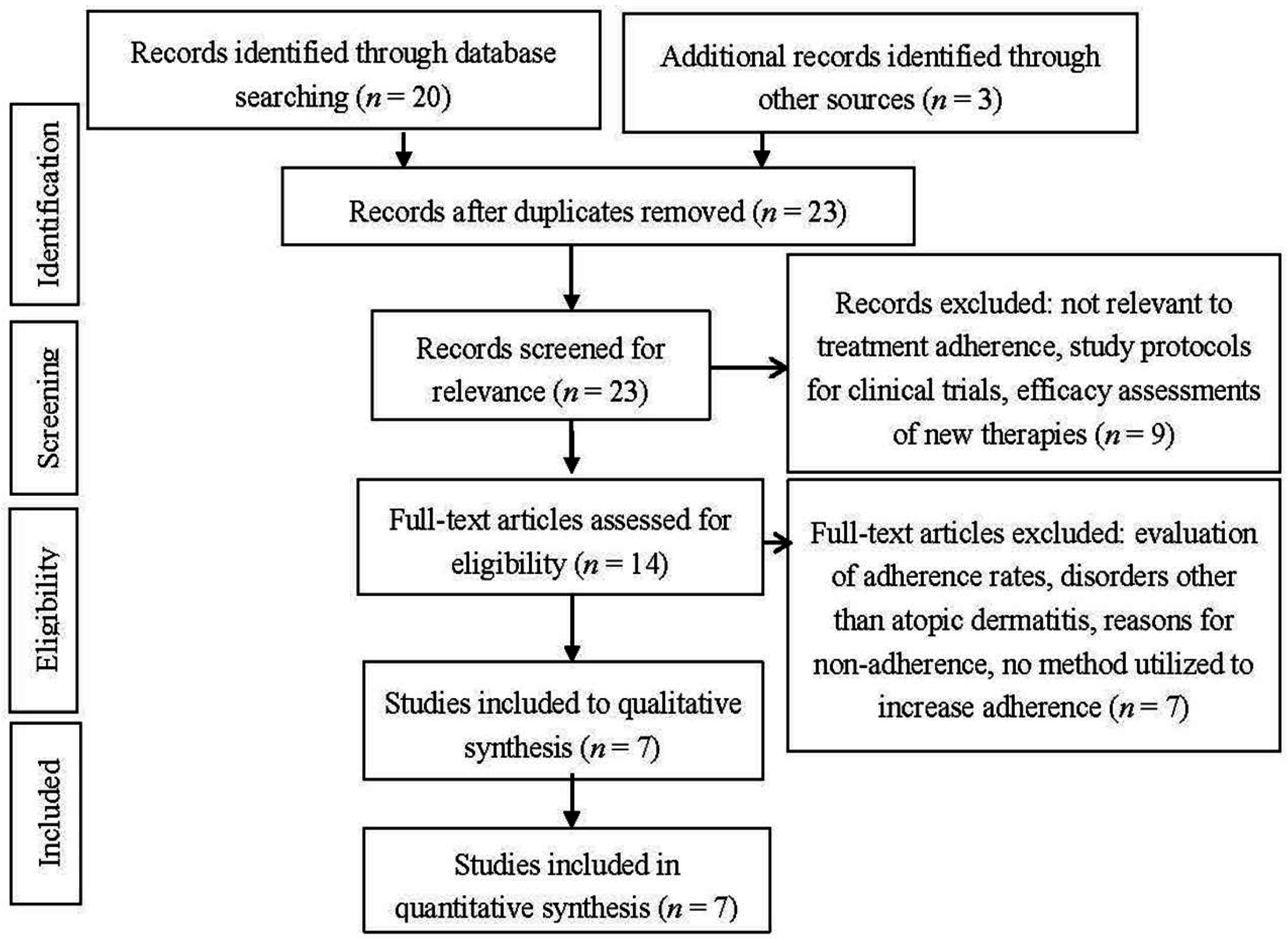
2. Methods
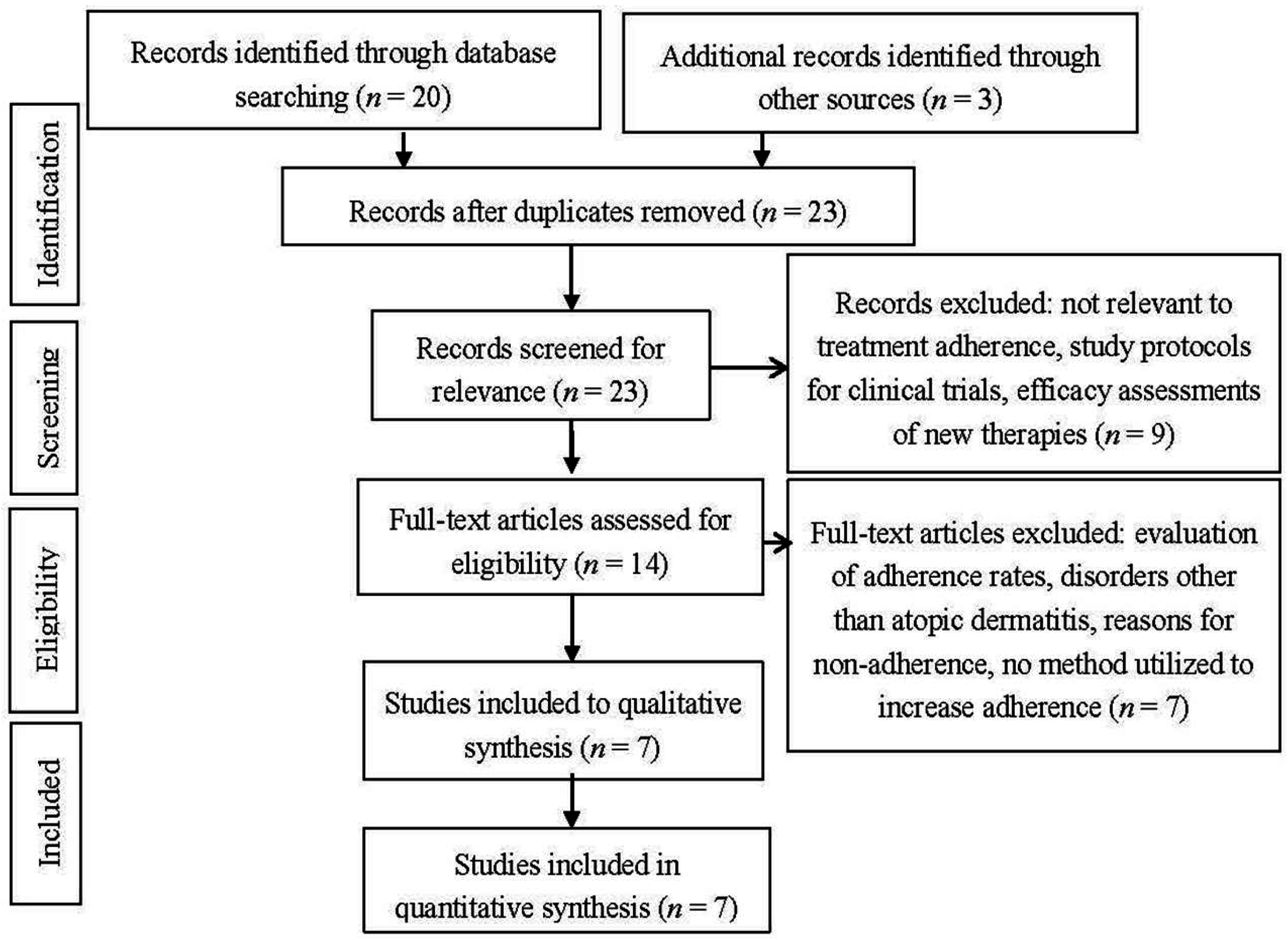
3. Results

{kind=link}
{kind=link}
| Study; Year (From most Effective to Least Effective Intervention) | Adherence Intervention | Sample Size | Measures Used to Assess Adherence and/or Severity | Was Adherence Directly Measured? If So, What Was the Result? | Improvement in Severity | Other Outcomes |
|---|---|---|---|---|---|---|
| Rork et al. [14]; 2012 | Written eczema action plan (EAP) | 35 | Parental survey at baseline and at follow up between 3–12 months later addressing severity, treatment comfort level, and if they had received a previous action plan | Not directly measured | 80% of the parents rated their child’s eczema lower on the severity scale, 68% attributed improved severity due to the EAP | Parental comfort increased to 86% from 57% at baseline in the intervention group, 86% of parents found the EAP helpful |
| Moore et al. [12]; 2009 | Nurse-led eczema workshops | 99 | SCORAD index | Not directly measured | 73% improvement to mild severity in the intervention group versus 40% in the control group | N/A |
| Sagransky et al. [18]; 2010 | Extra office visit at one week | 20 | MEMS cap measured adherence, EASI and VAS measured clinical efficacy | Yes by MEMS cap. Mean adherence was 69% in the intervention group versus 54% in the control group | Mean improvement between the two groups was not statistically significant. (Improvement in the VAS and EASI scores in the intervention group respectively were 65% and 76% versus 36% and 45% in the control group) | N/A |
| Grillo et al. [15]; 2006 | Education workshop (2 h session) | 61 | Severity measured by the SCORAD index, family impact using DFI, and quality of life using the IDQOL and CDLQI | Not directly measured | SCORAD showed mean improvement of 45% at week 4 and 54% at week 12 in the intervention group compared to 7% at week 4 and 16% at week 12 in the control group | DFI, IDQOL, and CDLQI scores showed no significant difference between the groups |
| Staab, [16]; 2002 | Educational program consisting of 6 group sessions of 2 h each | 204 | Severity measured by the SCORAD index; treatment behavior, dietary restriction, indoor allergen reduction, quality of life, coping, and treatment costs measured by a questionnaire | Yes by survey. After 1 year, 82% of the intervention group versus 67% of the control group stated regular use of their skin care products versus 88% of the intervention group and 89% of the control group at baseline | Results were not statistically significant. Average decrease in the SCORAD index intervention group was 20 points, compared to 16 points in the control group | Increased dietary restriction, reduction in indoor allergens, increased quality of life, decrease in rumination, and decrease in treatment costs were all seen in the intervention group compared to the control group at 1 year follow up |
| Shaw et al. [13]; 2008 | Atopic dermatitis educator (15 min session) | 106 | Severity measured by the SCORAD index, quality of life using the IDQOL and the CDLQI indices | Not directly measured | Severity decreased 31% in the test group versus 21% in the control group but the results were found to be not statistically significant (p > 0.05) | No significant difference was noted in the infant’s or children’s quality of life as measured by the IDQOL and CDLQI, respectively |
| Chinn et al. [17]; 2002 | Nurse consultation (30 min session) | 235 | Family impact using the FDI and quality of life using the IDQOL and CDLQI at 4 and 12 weeks | Not directly measured | Not directly measured | Marginal suggestion of benefit in the intervention group using the FDI only at 4 weeks, no significant difference seen between the groups in quality of life |
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Kubota, Y.; Yoneda, K.; Nakai, K.; Katsuura, J.; Moriue, T.; Matsuoka, Y.; Miyamoto, I.; Ohya, Y. Effect of sequential applications of topical tacrolimus and topical corticosteroids in the treatment of pediatric atopic dermatitis: An open-label pilot study. J. Am. Acad. Dermatol. 2009, 60, 212–217. [Google Scholar] [PubMed]
- Ou, H.T.; Feldman, S.R.; Balkrishnan, R. Understanding and improving treatment adherence in pediatric patients. Semin. Cutan. Med. Surg. 2010, 29, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Storm, A.; Andersen, S.E.; Benfeldt, E.; Serup, J. One in 3 prescriptions are never redeemed: Primary nonadherence in an outpatient clinic. J. Am. Acad. Dermatol. 2008, 59, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Krejci-Manwaring, J.; Tusa, M.G.; Carroll, C.; Camacho, F.; Kaur, M.; Carr, D.; Fleischer, A.B., Jr.; Rajesh Balkrishnan, R.; Feldman, S.R. Stealth monitoring of adherence to topical medication: adherence is very poor in children with atopic dermatitis. J. Am. Acad. Dermatol. 2007, 56, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Hix, E.; Gustafson, C.J.; O’Neill, J.L.; Huang, K.; Sandoval, L.F.; Harrison, J.; Clark, A.; Feldman, S.R. Adherence to a five day treatment course of topical fluocinonide 0.1% cream in atopic dermatitis. Available online: https://escholarship.org/uc/item/7644f317 (accessed on 9 September 2014).
- Ellis, R.M.; Koch, L.H.; McGuire, E.; Williams, J.V. Potential barriers to adherence in pediatric dermatology. Pediatr. Dermatol. 2011, 28, 242–244. [Google Scholar] [CrossRef] [PubMed]
- Carroll, C.L.; Balkrishnan, R.; Feldman, S.R.; Fleischer, A.B., Jr.; Manuel, J.C. The burden of atopic dermatitis: Impact on the patient, family, and society. Pediatr. Dermatol. 2005, 22, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Mancini, A.J.; Kaulback, K.; Chamlin, S.L. The socioeconomic impact of atopic dermatitis in the United States: A systematic review. Pediatr. Dermatol. 2008, 25, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Balato, N.; Megna, M.; Di, C.L.; Balato, A.; Ayala, F. Educational and motivational support service: A pilot study for mobile-phone-based interventions in patients with psoriasis. Br. J. Dermatol. 2013, 168, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Cardenas, V.; Sabater-Hernandez, D.; Kenny, P.; Martinez-Martinez, F.; Faus, M.J.; Benrimoj, S.I. Effect of a pharmacist intervention on asthma control. A cluster randomised trial. Respir. Med. 2013, 107, 1346–1355. [Google Scholar] [CrossRef] [PubMed]
- Luersen, K.; Davis, S.A.; Kaplan, S.G.; Abel, T.D.; Winchester, W.W.; Feldman, S.R. Sticker charts: A method for improving adherence to treatment of chronic diseases in children. Pediatr. Dermatol. 2012, 29, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.J.; Williams, A.; Manias, E.; Varigos, G.; Donath, S. Eczema workshops reduce severity of childhood atopic eczema. Australas. J. Dermatol. 2009, 50, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Shaw, M.; Morrell, D.S.; Goldsmith, L.A. A study of targeted enhanced patient care for pediatric atopic dermatitis (STEP PAD). Pediatr. Dermatol. 2008, 25, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Rork, J.F.; Sheehan, W.J.; Gaffin, J.M.; Timmons, K.G.; Sidbury, R.; Schneider, L.C.; Phipatanakul, W. Parental response to written eczema action plans in children with eczema. Arch. Dermatol. 2012, 148, 391–392. [Google Scholar] [CrossRef] [PubMed]
- Grillo, M.; Gassner, L.; Marshman, G.; Dunn, S.; Hudson, P. Pediatric atopic eczema: The impact of an educational intervention. Pediatr. Dermatol. 2006, 23, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Staab, D.; von Rueden, U.; Kehrt, R.; Erhart, M.; Wenninger, K.; Kamtsiuris, P.; Wahn, U. Evaluation of a parental training program for the management of childhood atopic dermatitis. Pediatr. Allergy. Immunol. 2002, 13, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Chinn, D.J.; Poyner, T.; Sibley, G. Randomized controlled trial of a single dermatology nurse consultation in primary care on the quality of life of children with atopic eczema. Br. J. Dermatol. 2002, 146, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Sagransky, M.J.; Yentzer, B.A.; Williams, L.L.; Clark, A.R.; Taylor, S.L.; Feldman, S.R. A randomized controlled pilot study of the effects of an extra office visit on adherence and outcomes in atopic dermatitis. Arch. Dermatol. 2010, 146, 1428–1430. [Google Scholar] [CrossRef] [PubMed]
- Ricci, G.; Bendandi, B.; Aiazzi, R.; Patrizi, A.; Masi, M. Three years of Italian experience of an educational program for parents of young children affected by atopic dermatitis: Improving knowledge produces lower anxiety levels in parents of children with atopic dermatitis. Pediatr. Dermatol. 2009, 26, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Feldman, S.R.; Camacho, F.T.; Krejci-Manwaring, J.; Carroll, C.L.; Balkrishnan, R. Adherence to topical therapy increases around the time of office visits. J. Am. Acad. Dermatol. 2007, 57, 81–83. [Google Scholar] [CrossRef] [PubMed]
- Snyder, S.; Crandell, I.; Davis, S.A.; Feldman, S.R. Medical adherence to acne therapy: A systematic review. Am. J. Clin. Dermatol. 2014, 15, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Santer, M.; Burgess, H.; Yardley, L.; Ersser, S.J.; Lewis-Jones, S.; Muller, I.; Hugh, C.; Little, P. Managing childhood eczema: Qualitative study exploring carers’ experiences of barriers and facilitators to treatment adherence. J. Adv. Nurs. 2013, 69, 2493–2501. [Google Scholar] [PubMed]
- Fenerty, S.D.; O’Neill, J.L.; Gustafson, C.J.; Feldman, S.R. Maternal adherence factors in the treatment of pediatric atopic dermatitis. JAMA Dermatol. 2013, 149, 229–231. [Google Scholar] [CrossRef] [PubMed]
- Evangelista, M.T.; Abad-Casintahan, F.; Lopez-Villafuerte, L. The effect of topical virgin coconut oil on SCORAD index, transepidermal water loss, and skin capacitance in mild to moderate pediatric atopic dermatitis: A randomized, double-blind, clinical trial. Int. J. Dermatol. 2014, 53, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Canpolat, F.; Erkocoglu, M.; Tezer, H.; Kocabas, C.N.; Kandi, B. Hydrocortisone acetate alone or combined with mupirocin for atopic dermatitis in infants under two years of age—A randomized double blind pilot trial. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 1989–1993. [Google Scholar] [PubMed]
- Eisen, D.; Ellis, C.N.; Duell, E.A.; Griffiths, C.E.; Voorhees, J.J. Effect of topical cyclosporine rinse on oral lichen planus. A double-blind analysis. N. Engl. J. Med. 1990, 323, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Happonen, H.P.; Lassus, A.; Santalahti, J.; Forsstrom, S.; Lassus, J. Topical idoxuridine for treatment of genital warts in males. A double-blind comparative study of 0.25% and 0.5% cream. Genitourin. Med. 1990, 66, 254–256. [Google Scholar] [PubMed]
- Carroll, C.L.; Feldman, S.R.; Camacho, F.T.; Manuel, J.C.; Balkrishnan, R. Adherence to topical therapy decreases during the course of an 8-week psoriasis clinical trial: Commonly used methods of measuring adherence to topical therapy overestimate actual use. J. Am. Acad. Dermatol. 2004, 51, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Balkrishnan, R.; Carroll, C.L.; Camacho, F.T.; Feldman, S.R. Electronic monitoring of medication adherence in skin disease: Results of a pilot study. J. Am. Acad. Dermatol. 2003, 49, 651–654. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bass, A.M.; Anderson, K.L.; Feldman, S.R. Interventions to Increase Treatment Adherence in Pediatric Atopic Dermatitis: A Systematic Review. J. Clin. Med. 2015, 4, 231-242. https://doi.org/10.3390/jcm4020231
Bass AM, Anderson KL, Feldman SR. Interventions to Increase Treatment Adherence in Pediatric Atopic Dermatitis: A Systematic Review. Journal of Clinical Medicine. 2015; 4(2):231-242. https://doi.org/10.3390/jcm4020231
Chicago/Turabian StyleBass, Alexandria M., Kathryn L. Anderson, and Steven R. Feldman. 2015. "Interventions to Increase Treatment Adherence in Pediatric Atopic Dermatitis: A Systematic Review" Journal of Clinical Medicine 4, no. 2: 231-242. https://doi.org/10.3390/jcm4020231