
Undernutrition and Overnutrition Burden for Diseases in Developing Countries: The Role of Oxidative Stress Biomarkers to Assess Disease Risk and Interventional Strategies

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Oxidative Stress Status: Measures and Possible Intervention
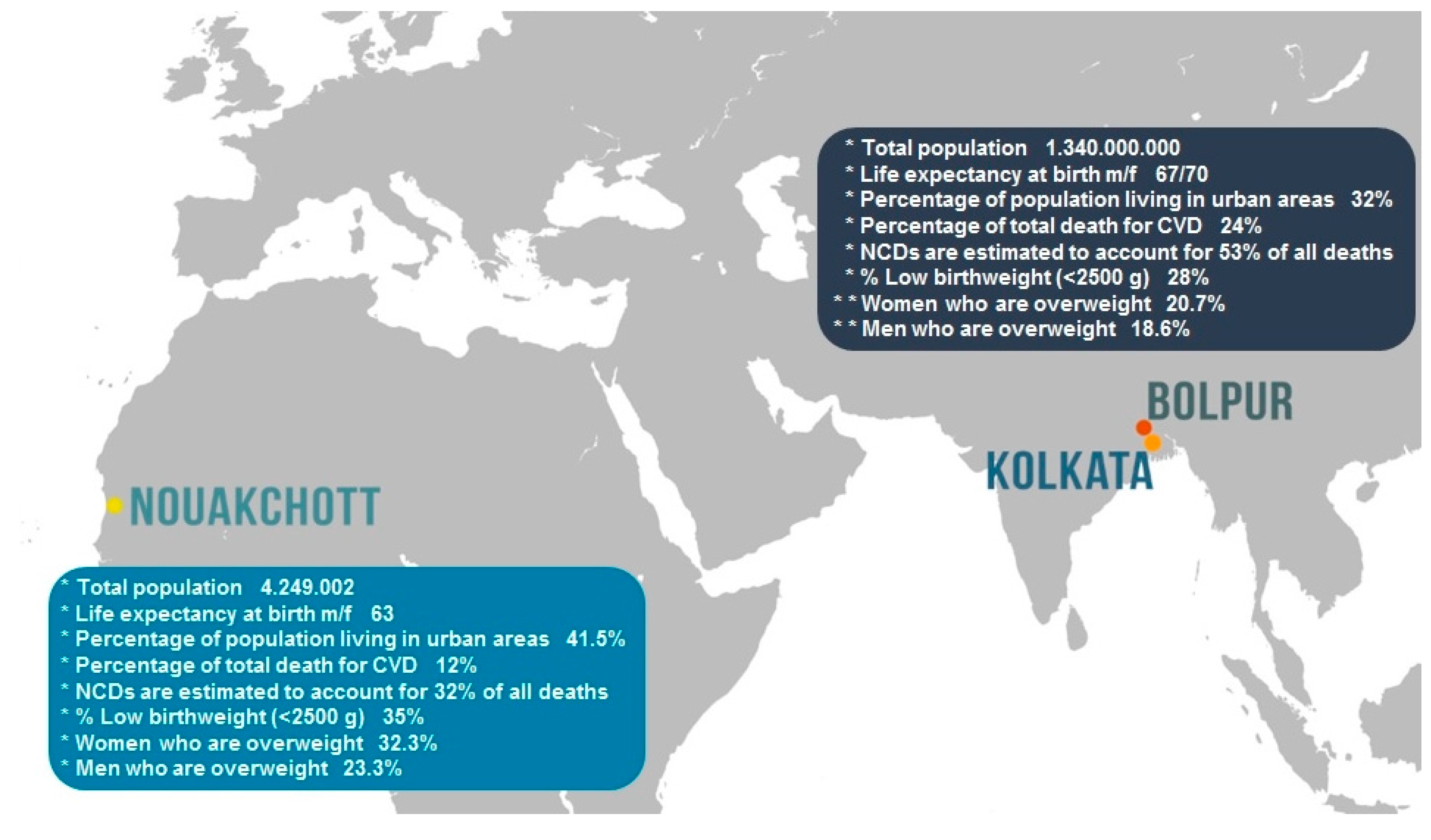
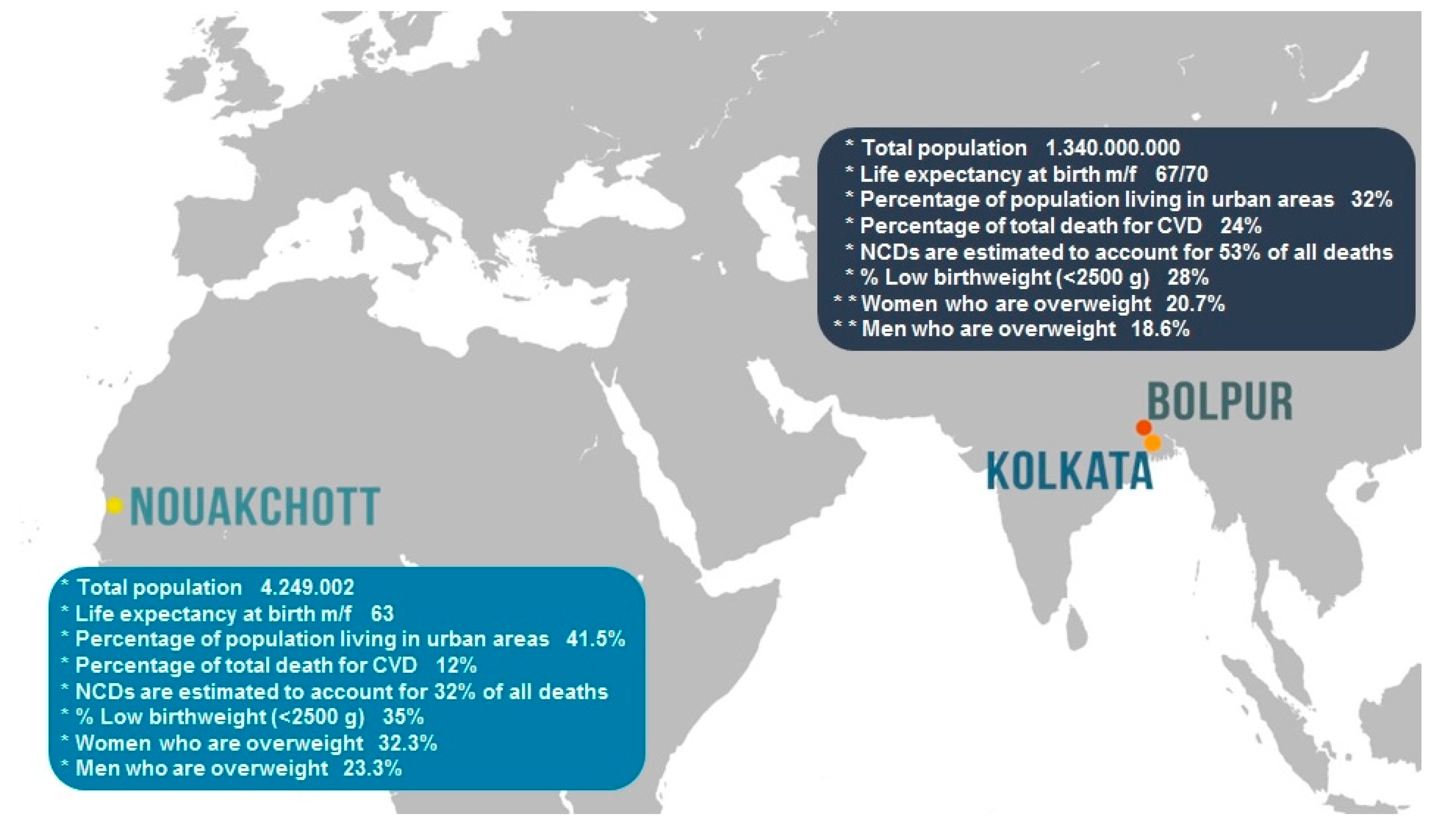
3. The Islamic Republic of Mauritania
4. India
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Belahsen, R. Nutrition transition and food sustainability. Proc. Nutr. Soc. 2014, 73, 385–388. [Google Scholar] [CrossRef] [PubMed]
- Amuna, P.; Zotor, F.B. Epidemiological and nutrition transition in developing countries: Impact on human health and development. Proc. Nutr. Soc. 2008, 67, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Global Status Report on Non-Communicable Diseases 2010. Available online: http://www.who.int/nmh/publications/ncd_report_full_en.pdf (accessed on 24 April 2017).
- Mattei, J.; Malik, V.; Wedick, N.M.; Campos, H.; Spiegelman, D.; Willett, W.; Hu, F.B. A symposium and workshop report from the Global Nutrition and Epidemiologic Transition Initiative: Nutrition transition and the global burden of type 2 diabetes. Br. J. Nutr. 2012, 108, 1325–1335. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Reddy, S.; Ounpuu, S.; Anand, S. Global burden of cardiovascular diseases: Part I: General considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation 2001, 104, 2746–2753. [Google Scholar] [CrossRef] [PubMed]
- Steyn, N.P.; McHiza, Z.J. Obesity and the nutrition transition in Sub-Saharan Africa. Ann. N. Y. Acad. Sci. 2014, 1311, 88–101. [Google Scholar] [CrossRef] [PubMed]
- Pingitore, A.; Lima, G.P.P.; Mastorci, F.; Quinones, A.; Iervasi, G.; Vassalle, C. Exercise and oxidative stress: Potential effects of antioxidant dietary strategies in sports. Nutrition 2015, 31, 916–922. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C.; Pingitore, A.; De Giuseppe, R.; Vigna, L.; Bamonti, F. Biomarkers Part II: Biomarkers to Estimate Bioefficacy of Dietary/Supplemental Antioxidants in Sport. In Antioxidants in Sport Nutrition; Lamprecht, M., Ed.; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2015; Chapter 16. [Google Scholar]
- Vassalle, C.; Lubrano, V.; L'Abbate, A.; Clerico, A. Determination of nitrite plus nitrate and malondialdehyde in human plasma: Analytical performance and the effect of smoking and exercise. Clin. Chem. Lab. Med. 2002, 40, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.; Milne, G.L.; Sandler, D.P.; Nichols, H.B. Oxidative stress in relation to diet and physical activity among premenopausal women. Br. J. Nutr. 2016, 116, 1416–1424. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C.; Pratali, L.; Boni, C.; Mercuri, A.; Ndreu, R. An oxidative stress score as a combined measure of the pro-oxidant and anti-oxidant counterparts in patients with coronary artery disease. Clin. Biochem. 2008, 41, 1162–1167. [Google Scholar] [CrossRef] [PubMed]
- Jood, S.; Gupta, M.; Yadav, S.K.; Khetarpaul, N. Effect of supplementation on haemoglobin and serum retinol levels and nutritional status of school children of northern India. Nutr. Health 2001, 15, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Ghone, R.A.; Suryakar, A.N.; Kulhalli, P.M.; Bhagat, S.S.; Padalkar, R.K.; Karnik, A.C.; Hundekar, P.S.; Sangle, D.A. A study of oxidative stress biomarkers and effect of oral antioxidant supplementation in severe acute malnutrition. J. Clin. Diagn. Res. 2013, 7, 2146–2148. [Google Scholar] [CrossRef] [PubMed]
- Mazumder, S.; Taneja, S.; Bhatia, K.; Yoshida, S.; Kaur, J.; Dube, B.; Toteja, G.S.; Bahl, R.; Fontaine, O.; Martines, J.; et al. Efficacy of early neonatal supplementation with vitamin A to reduce mortality in infancy in Haryana, India (Neovita): A randomised, double-blind, placebo-controlled trial. Lancet 2015, 385, 1333–1342. [Google Scholar] [CrossRef]
- Chatzianagnostou, K.; Del Turco, S.; Pingitore, A.; Sabatino, L.; Vassalle, C. The Mediterranean Lifestyle as a non-pharmacological and natural antioxidant for healthy aging. Antioxidants 2015, 4, 719–736. [Google Scholar] [CrossRef] [PubMed]
- The World Factbook—Central Intelligence Agency of the United States of America. Available online: https://www.cia.gov/library/publications/the-world-factbook/geos/mr.html (accessed on 24 April 2017).
- Zühlke, L.; Mirabel, M.; Marijon, E. Congenital heart disease and rheumatic heart disease in Africa: Recent advances and current priorities. Heart 2013, 99, 1554–1561. [Google Scholar] [CrossRef] [PubMed]
- Wuehler, S.E.; El Hafed Ould Dehah, C.M. Situational analysis of infant and young child nutrition policies and programmatic activities in the Islamic Republic of Mauritania. Matern. Child Nutr. 2011, 7, 113–132. [Google Scholar] [CrossRef] [PubMed]
- Environmental Health Challenges in Mauritania. Available online: http://www.who.int/features/2013/mauritania_environmental_health/en/ (accessed on 24 April 2017).
- Enquête sur l’Hypertension Artérielle; le Diabète et autres Facteurs de Risque Cardio-Vasculaires À Nouakchott Mauritanie Janvier-Juin, 2006. Available online: http://www.who.int/fctc/secretariat/annexfour.pdf (accessed on 24 April 2017).
- Vassalle, C.; Sciarrino, R.; Bianchi, S.; Battaglia, D.; Mercuri, A.; Maffei, S. Sex-related differences in association of oxidative stress status with coronary artery disease. Fertil. Steril. 2012, 97, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C.; Botto, N.; Andreassi, M.G.; Berti, S.; Biagini, A. Evidence for enhanced 8-isoprostane plasma levels, as index of oxidative stress in vivo, in patients with coronary artery disease. Coron. Artery Dis. 2003, 14, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Leopold, J.A. Antioxidants and coronary artery disease: From pathophysiology to preventive therapy. Coron. Artery Dis. 2015, 26, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C.; Maffei, S.; Ndreu, R.; Mercuri, A. Age-related oxidative stress modulation by smoking habit and obesity. Clin. Biochem. 2009, 42, 739–741. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C.; Novembrino, C.; Maffei, S.; Sciarrino, R.; De Giuseppe, R.; Vigna, L.; de Liso, F.; Mercuri, A.; Bamonti, F. Determinants of oxidative stress related to gender: Relevance of age and smoking habit. Clin. Chem. Lab. Med. 2011, 49, 1509–1513. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C.; Bianchi, S.; Battaglia, D.; Landi, P.; Bianchi, F.; Carpeggiani, C. Elevated levels of oxidative stress as a prognostic predictor of major adverse cardiovascular events in patients with coronary artery disease. J. Atheroscler. Thromb. 2012, 19, 712–717. [Google Scholar] [CrossRef] [PubMed]
- Ikonomidis, I.; Michalakeas, C.A.; Lekakis, J.; Paraskevaidis, I.; Kremastinos, D.T. Multimarker approach in cardiovascular risk prediction. Dis. Markers 2009, 26, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Lemine, M.; Mint, F.; Mohamed Ahmed, M.V.O.; Ben Mohamed Maoulainine, L.; Bouna Zel, A.; Samb, A.; Boukhary, O.; Salem, AO. Antioxidant activity of various Mauritanian date palm (Phoenix dactylifera L.) fruits at two edible ripening stages. Food Sci. Nutr. 2014, 2, 700–705. [Google Scholar] [CrossRef] [PubMed]
- World Population Ageing, 2015. Available online: http://www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2015_Report.pdf (accessed on 24 April 2017).
- Vassalle, C.; Mazzone, A.; Sabatino, L.; Carpeggiani, C. Uric Acid for Cardiovascular Risk: Dr. Jekyll or Mr. Hide? Diseases 2016, 4, 12. [Google Scholar] [CrossRef]
- Chatterjee, K.; Sinha, R.K.; Kundu, A.K.; Shankar, D.; Gope, R.; Nair, N.; Tripathy, P.K. Social determinants of inequities in under-nutrition (weight-for-age) among under-5 children: A cross sectional study in Gumla district of Jharkhand, India. Int. J. Equity Health 2016, 15, 104. [Google Scholar] [CrossRef] [PubMed]
- Reddy, V.B.; Kusuma, Y.S.; Pandav, C.S.; Goswami, A.K.; Krishnan, A. Prevalence of malnutrition, diarrhea, and acute respiratory infections among under-five children of Sugali tribe of Chittoor district, Andhra Pradesh, India. J. Nat. Sci. Biol. Med. 2016, 7, 155–160. [Google Scholar] [PubMed]
- Bentley, A.; Das, S.; Alcock, G.; Shah More, N.; Pantvaidya, S.; Osrin, D. Malnutrition and infant and young child feeding in informal settlements in Mumbai, India: Findings from a census. Food Sci. Nutr. 2015, 3, 257–271. [Google Scholar] [CrossRef] [PubMed]
- Menon, J.; Vijayakumar, N.; Joseph, J.K.; David, P.C.; Menon, M.N.; Mukundan, S.; Dorphy, P.D.; Banerjee, A. Below the poverty line and non-communicable diseases in Kerala: The Epidemiology of Non-communicable Diseases in Rural Areas (ENDIRA) study. Int. J. Cardiol. 2015, 187, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Antioxidants in the Diet and Cognitive Function: Which Role for the Mediterranean Life-style? Available online: http://www.jpreventionalzheimer.com/registration.html (accessed on 24 April 2017).
- Kinra, S.; Rameshwar Sarma, K.V.; Ghafoorunissa Mendu, V.V.; Ravikumar, R.; Mohan, V.; Wilkinson, I.B.; Cockcroft, J.R.; Davey Smith, G.; Ben-Shlomo, Y. Effect of integration of supplemental nutrition with public health programmes in pregnancy and early childhood on cardiovascular risk in rural Indian adolescents: Long term follow-up of Hyderabad nutrition trial. BMJ 2008, 337, a605. [Google Scholar] [CrossRef] [PubMed]
- Anand, P.; Awasthi, S.; Mahdi, A.; Tiwari, M.; Agarwal, G.G. Serum homocysteine in Indian adolescents. Indian J. Pediatr. 2009, 76, 705–709. [Google Scholar] [CrossRef] [PubMed]
- George, G.M.; Sharma, K.K.; Ramakrishnan, S.; Gupta, S.K. A study of cardiovascular risk factors and its knowledge among school children of Delhi. Indian Heart J. 2014, 66, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, U.; Misra, A.; Mohan, V.; Unnikrishnan, R.; Bachani, D. Obesity, Diabetes and Cardiovascular Diseases in India: Public Health Challenges. Curr. Diabetes Rev. 2017, 13, 65–80. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, K.; Dwivedi, L.K. The burden of infectious and cardiovascular diseases in India from 2004 to 2014. Epidemiol. Health 2016. [Google Scholar] [CrossRef] [PubMed]
- Misra, A.; Singha, N.; Sivakumar, B.; Bhagat, N.; Jaiswal, A.; Khurana, L. Nutrition transition in India: Secular trends in dietary intake and their relationship to diet-related non-communicable diseases. J. Diabetes 2011, 3, 278–292. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.; Arokiasamy, P. Understanding epidemiological transition in India. Glob. Health Action 2014, 7, 23248. [Google Scholar] [CrossRef] [PubMed]
- Mondal, N.K.; Roychoudhury, S.; Mukherjee, S.; Siddique, S.; Banerjee, M.; Slaughter, M.S.; Lahiri, T.; Ray, M.R. Increased risk of cardiovascular disease in premenopausal female ragpickers of Eastern India: Involvement of inflammation, oxidative stress, and platelet hyperactivity. Mol. Cell. Biochem. 2016, 419, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Dutta, A.; Ray, M.R.; Banerjee, A. Systemic inflammatory changes and increased oxidative stress in rural Indian women cooking with biomass fuels. Toxicol. Appl. Pharmacol. 2012, 261, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Hegde, A.; Yadav, C.; Ahmad, A.; Manjrekar, P.A.; Srikantiah, R.M. Assessment of oxidative stress and inflammation in prediabetes—A hospital based cross-sectional study. Diabetes Metab. Syndr. 2016, 10, S123–S126. [Google Scholar] [CrossRef] [PubMed]
- Pandey, G.; Shihabudeen, M.S.; David, H.P.; Thirumurugan, E.; Thirumurugan, K. Association between hyperleptinemia and oxidative stress in obese diabetic subjects. J. Diabetes Metab. Disord. 2015, 14, 24. [Google Scholar] [CrossRef] [PubMed]
- Indulekha, K.; Surendar, J.; Anjana, R.M.; Geetha, L.; Gokulakrishnan, K.; Pradeepa, R.; Mohan, V. Metabolic obesity, adipocytokines, and inflammatory markers in Asian Indians—CURES-124. Diabetes Technol. Ther. 2015, 17, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Niranjan, G.; Anitha, D.; Srinivasan, A.R.; Velu, V.K.; Venkatesh, C.; Babu, M.S.; Ramesh, R.; Saha, S. Association of inflammatory sialoproteins, lipid peroxides and serum magnesium levels with cardiometabolic risk factors in obese children of South Indian population. Int. J. Biomed. Sci. 2014, 10, 118–123. [Google Scholar] [PubMed]
- Jain, A.; Jadhav, A.A.; Varma, M. Relation of oxidative stress, zinc and alkaline phosphatase in protein energy malnutrition. Arch. Physiol. Biochem. 2013, 119, 15–21. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization 2015 Report. Available online: http://www.who.int/gho/publications/world_health_statistics/2015/en/ (accessed on 24 April 2017).
- National Family Health Survey—4. India Fact Sheet. Available online: http://rchiips.org/NFHS/factsheet.shtml (accessed on 24 April 2017).

© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mastorci, F.; Vassalle, C.; Chatzianagnostou, K.; Marabotti, C.; Siddiqui, K.; Eba, A.O.; Mhamed, S.A.S.; Bandopadhyay, A.; Nazzaro, M.S.; Passera, M.; et al. Undernutrition and Overnutrition Burden for Diseases in Developing Countries: The Role of Oxidative Stress Biomarkers to Assess Disease Risk and Interventional Strategies. Antioxidants 2017, 6, 41. https://doi.org/10.3390/antiox6020041
Mastorci F, Vassalle C, Chatzianagnostou K, Marabotti C, Siddiqui K, Eba AO, Mhamed SAS, Bandopadhyay A, Nazzaro MS, Passera M, et al. Undernutrition and Overnutrition Burden for Diseases in Developing Countries: The Role of Oxidative Stress Biomarkers to Assess Disease Risk and Interventional Strategies. Antioxidants. 2017; 6(2):41. https://doi.org/10.3390/antiox6020041
Chicago/Turabian StyleMastorci, Francesca, Cristina Vassalle, Kyriazoula Chatzianagnostou, Claudio Marabotti, Khawer Siddiqui, Ahmed Ould Eba, Soueid Ahmed Sidi Mhamed, Arun Bandopadhyay, Marco Stefano Nazzaro, Mirko Passera, and et al. 2017. "Undernutrition and Overnutrition Burden for Diseases in Developing Countries: The Role of Oxidative Stress Biomarkers to Assess Disease Risk and Interventional Strategies" Antioxidants 6, no. 2: 41. https://doi.org/10.3390/antiox6020041