Preliminary Findings that a Targeted Intervention Leads to Altered Brain Function in Children with Fetal Alcohol Spectrum Disorder

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Design and Procedures
2.3. The Intervention
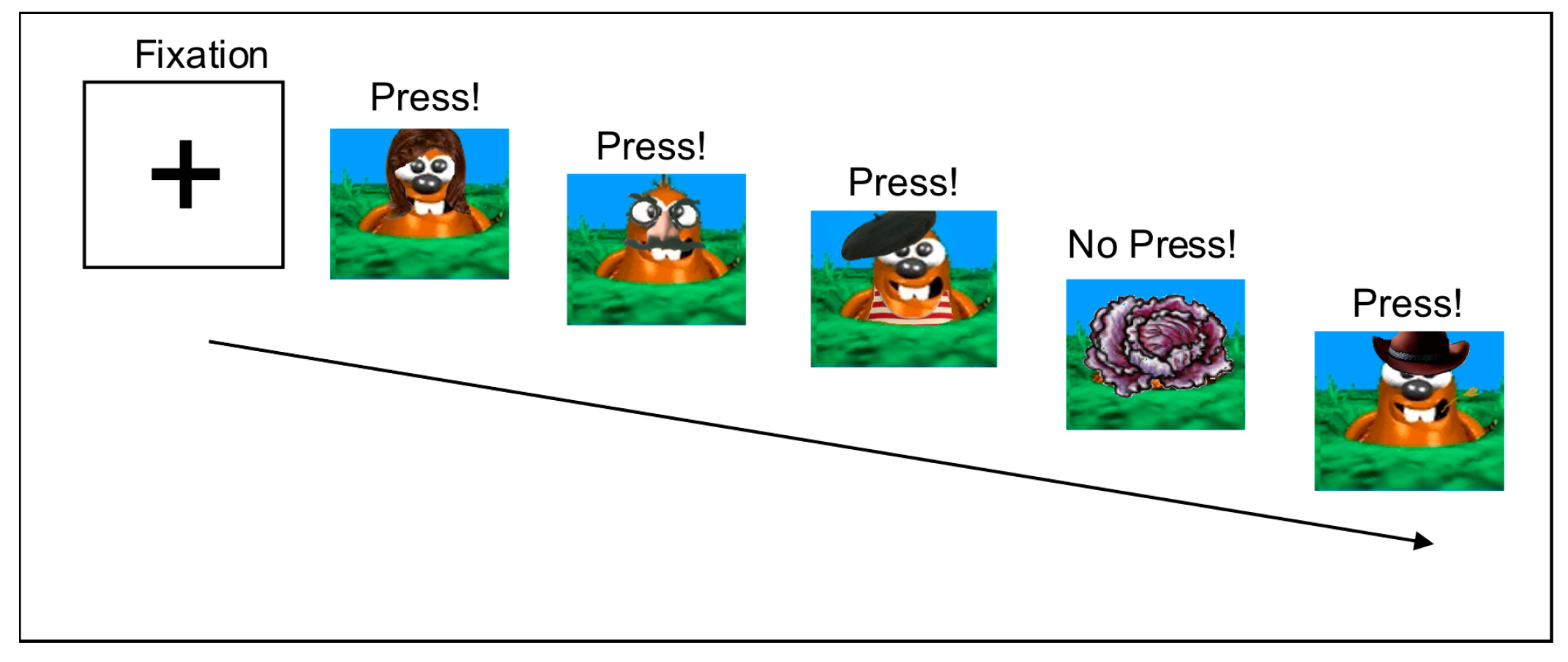
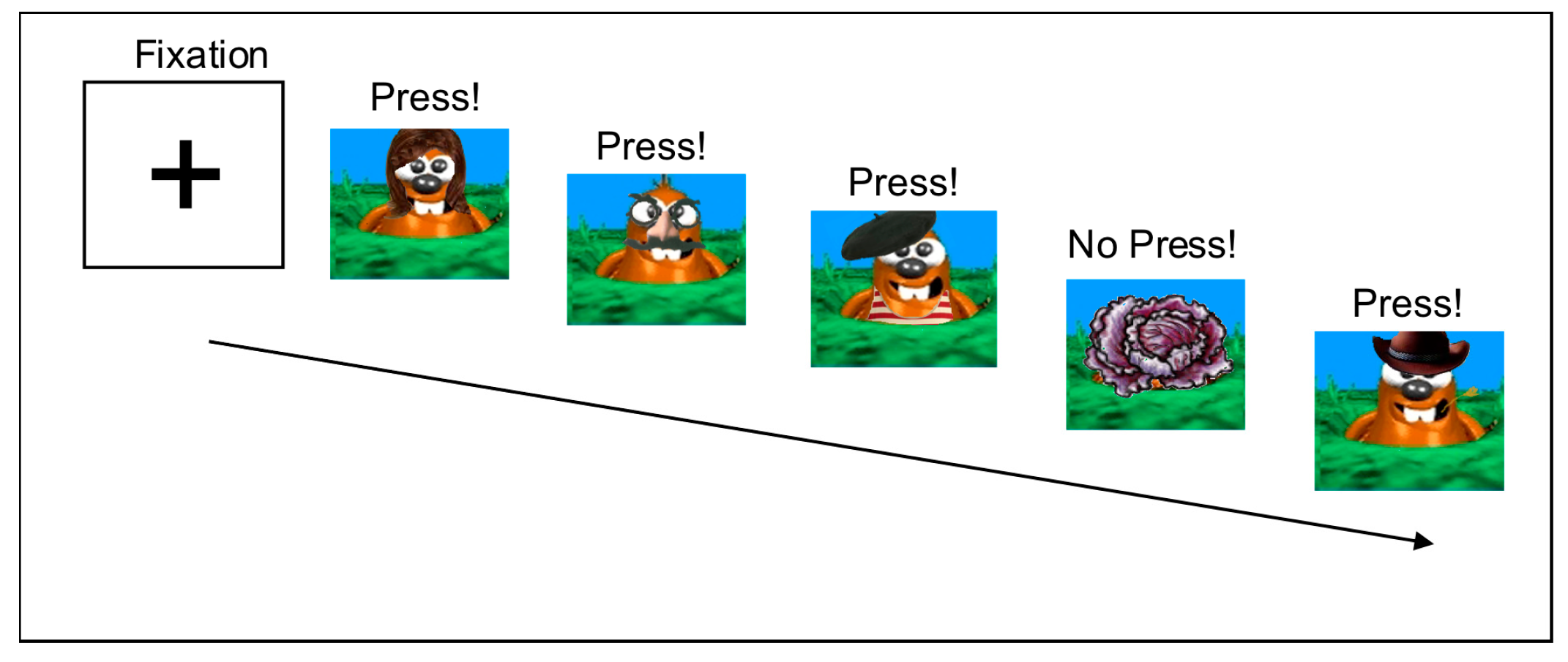
2.4. Neuroimaging Task, Procedures, and Image Analysis
2.5. Statistical Approach and Analyses
3. Results
3.1. Demographic Data
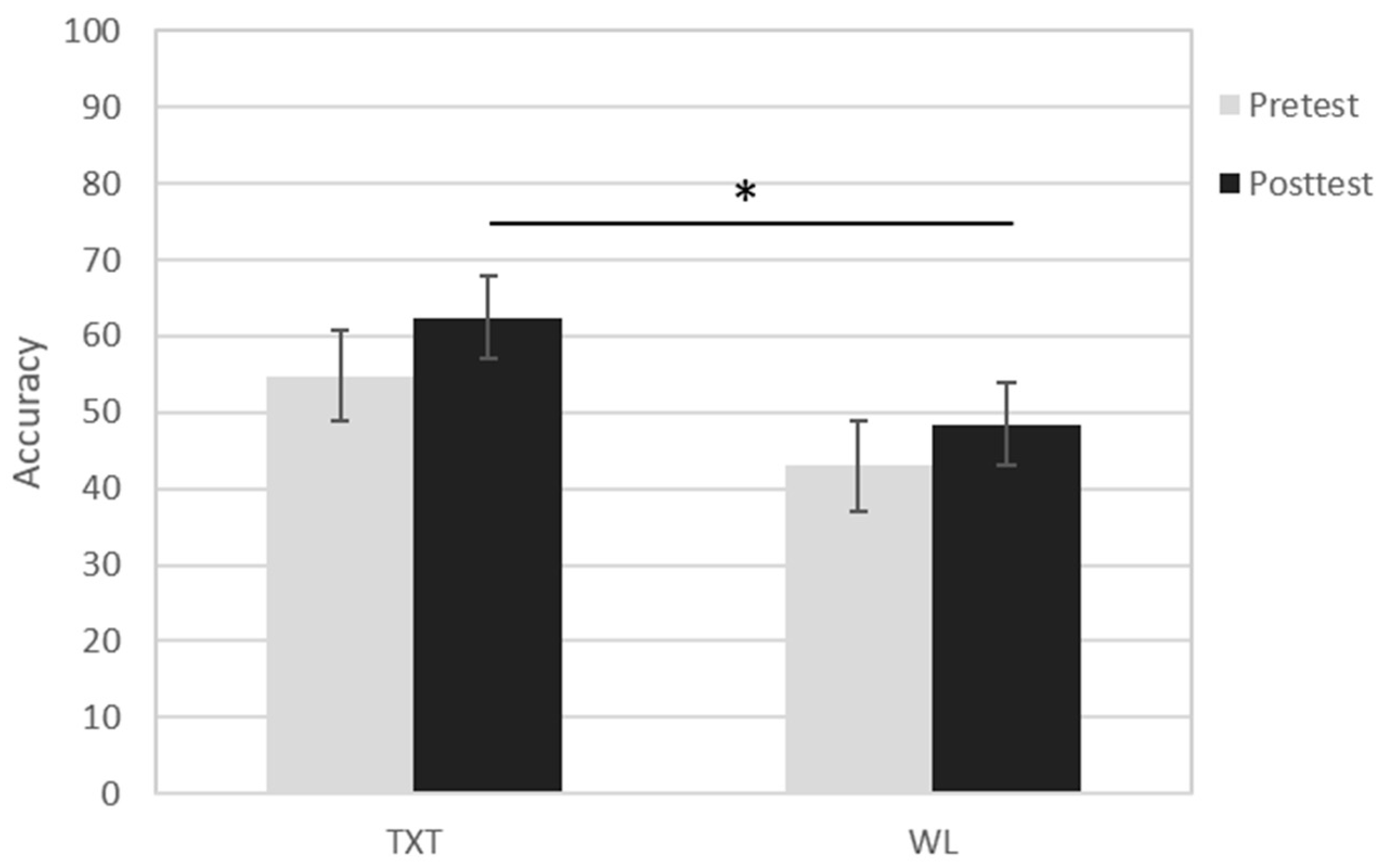
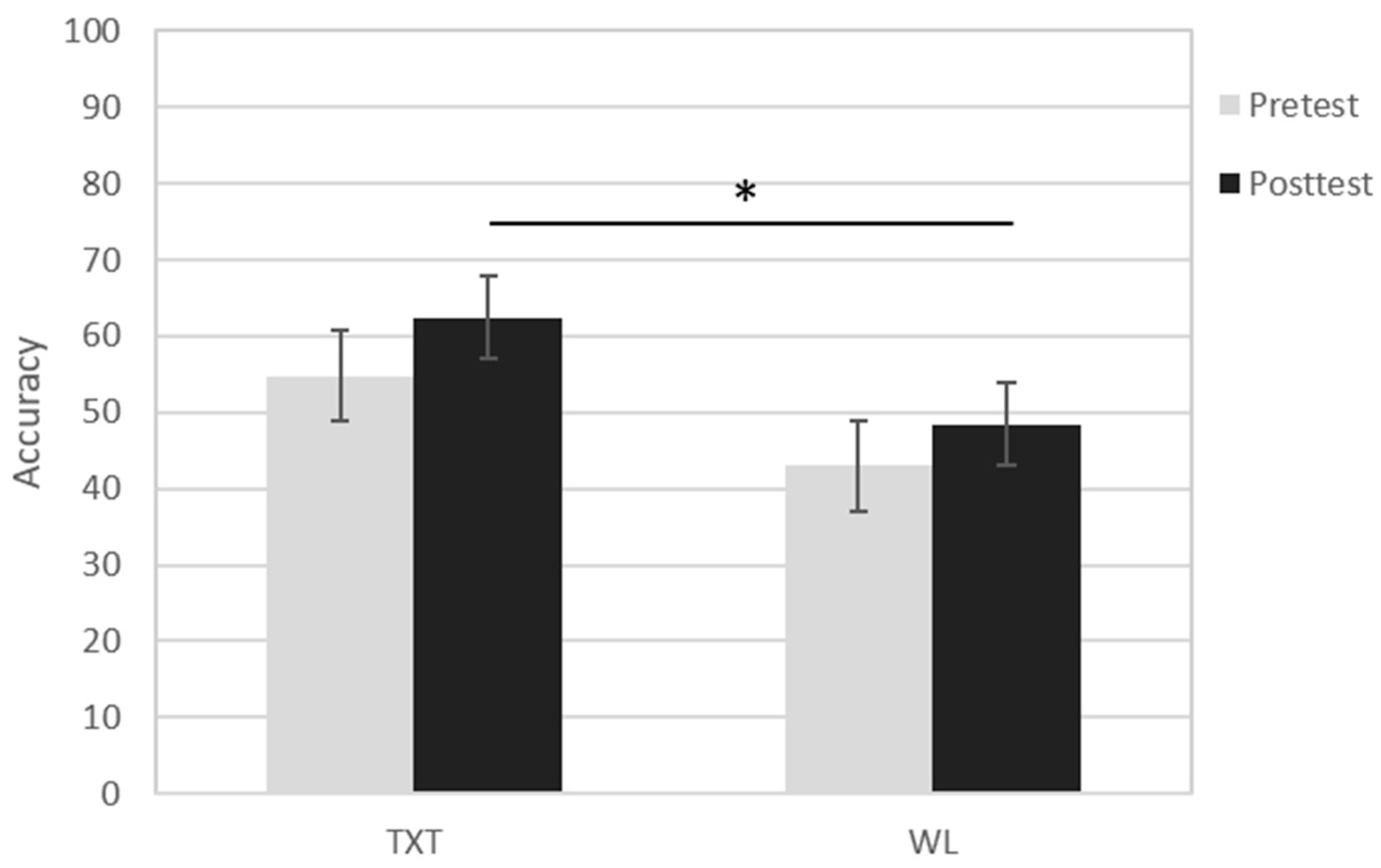
3.2. Behavioral Results
3.3. fMRI Results
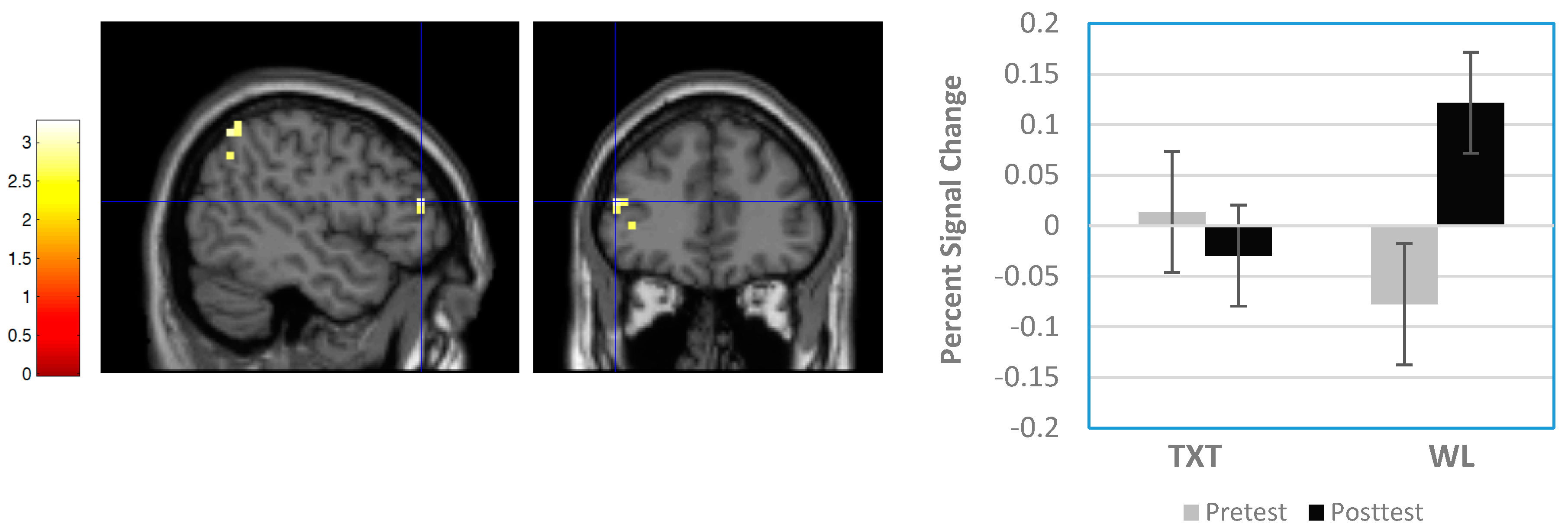
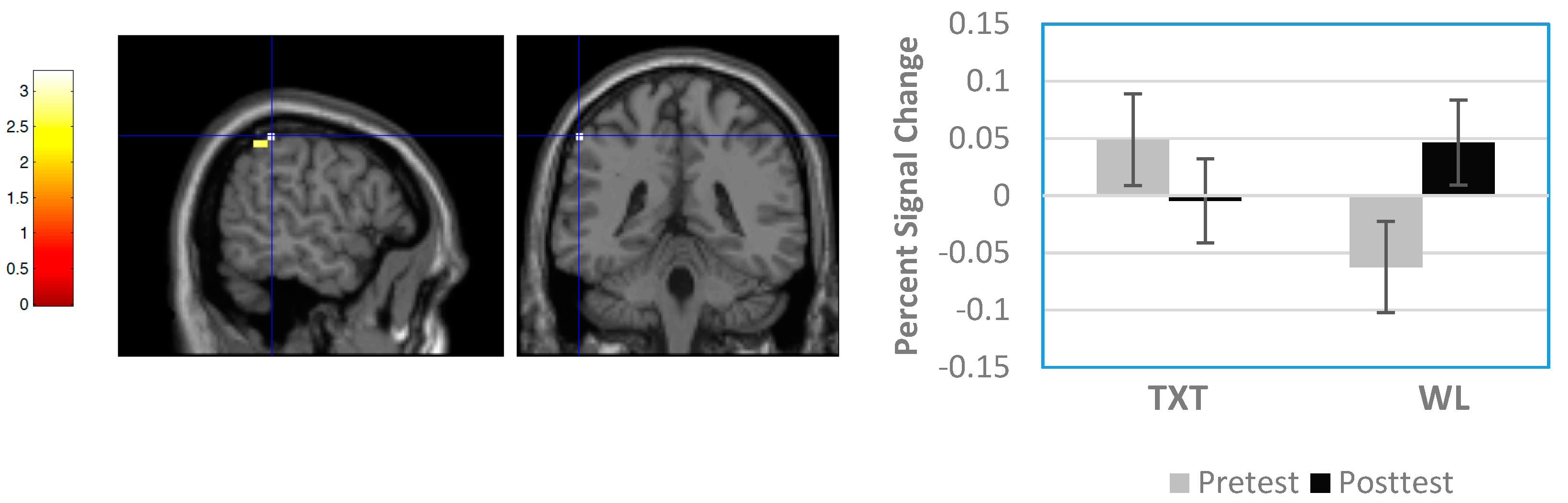
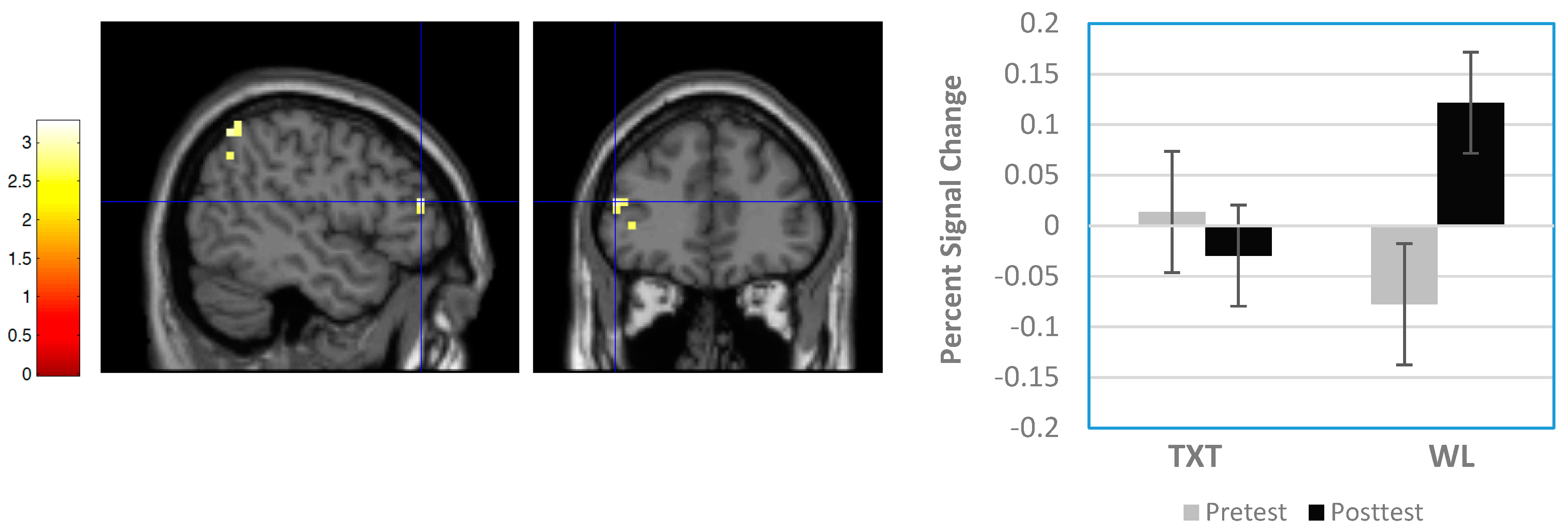
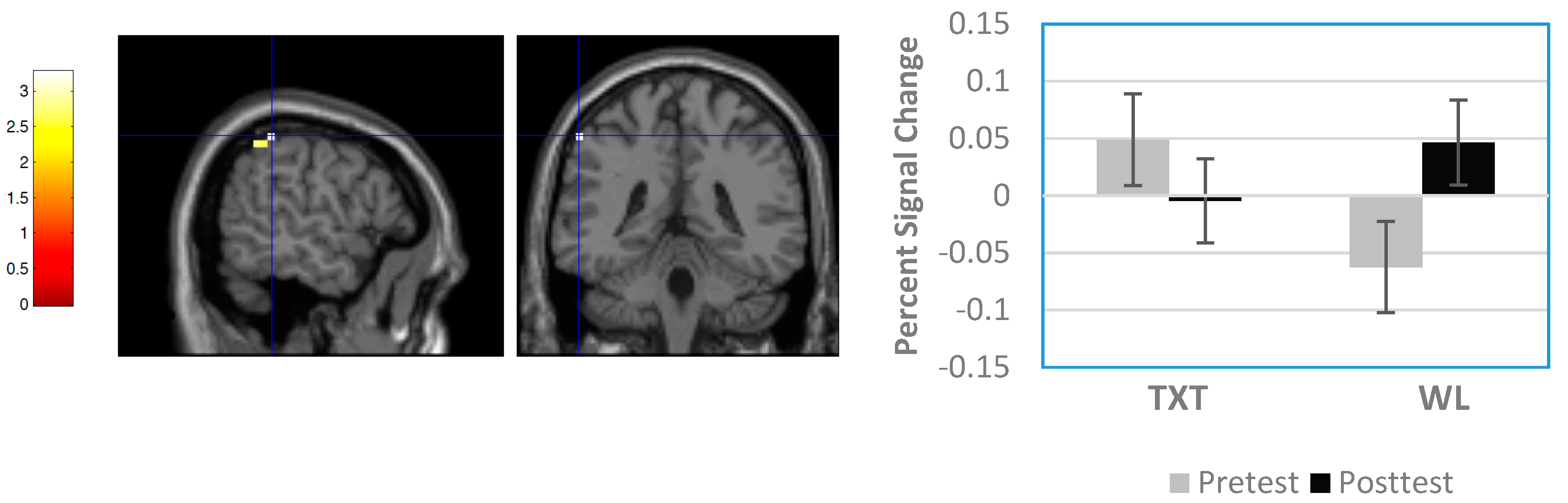
3.3.1. Whole Brain Results
3.3.2. Region-of-Interest Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Warren, K.R.; Bast, R.J. Alcohol-related birth defects: An update. Public Health Rep. 1988, 103, 638–642. [Google Scholar] [PubMed]
- May, P.A.; Baete, A.; Russo, J.; Elliott, A.J.; Blankenship, J.; Kalberg, W.O.; Buckley, D.; Brooks, M.; Hasken, J.; Abdul-Rahman, O.; et al. Prevalence and characteristics of fetal alcohol spectrum disorders. Pediatrics 2014, 134, 855–866. [Google Scholar] [CrossRef] [PubMed]
- May, P.A.; Fiorentino, D.; Coriale, G.; Kalberg, W.O.; Hoyme, H.E.; Aragon, A.S.; Buckley, D.; Stellavato, C.; Gossage, J.P.; Robinson, L.K.; et al. Prevalence of children with severe fetal alcohol spectrum disorders in communities near Rome, Italy: New estimated rates are higher than previous estimates. Int. J. Environ. Res. Public Health 2011, 8, 2331–2351. [Google Scholar] [CrossRef] [PubMed]
- May, P.A.; Blankenship, J.; Marais, A.S.; Gossage, J.P.; Kalberg, W.O.; Barnard, R.; De Vries, M.; Robinson, L.K.; Adnams, C.M.; Buckley, D.; et al. Approaching the prevalence of the full spectrum of fetal alcohol spectrum disorders in a South African population-based study. Alcohol. Clin. Exp. Res. 2013, 37, 818–830. [Google Scholar] [CrossRef] [PubMed]
- Mullally, A.; Cleary, B.J.; Barry, J.; Fahey, T.P.; Murphy, D.J. Prevalence, predictors and perinatal outcomes of peri-conceptional alcohol exposure—Retrospective cohort study in an urban obstetric population in Ireland. BMC Pregnancy Childbirth 2011, 11, 27. [Google Scholar] [CrossRef] [PubMed]
- Robinson, G.C.; Conry, J.L.; Conry, R.F. Clinical profile and prevalence of fetal alcohol syndrome in an isolated community in British Columbia. Can. Med. Assoc. J. 1987, 127, 203–307. [Google Scholar]
- Fitzpatrick, J.P.; Latimer, J.; Olson, H.C.; Carter, M.; Oscar, J.; Lucas, B.R.; Doney, R.; Salter, C.; Try, J.; Hawkes, G.; et al. Prevalence and profile of Neurodevelopment and Fetal Alcohol Spectrum Disorder (FASD) among Australian Aboriginal children living in remote communities. Res. Dev. Disabil. 2017, 65, 114–126. [Google Scholar] [CrossRef] [PubMed]
- Burd, L.; Moffatt, M.E.K. Epidemiology of Fetal Alcohol Syndrome in American Indians, Alaskan natives, and Canadian aboriginal peoples: A review of the literature. Public Health Rep. 1994, 109, 688–693. [Google Scholar] [PubMed]
- Stoler, M.; Holmes, L.B. Under recognition of prenatal alcohol effects in infants of known alcohol abusing women. J. Pediatr. 1999, 135, 430–436. [Google Scholar] [CrossRef]
- Stratton, K.R.; Howe, C.J.; Battaglia, F.C. Fetal Alcohol Syndrome: Diagnosis, Epidemiology, Prevention, and Treatment; National Academy Press: Washington, DC, USA, 1996. [Google Scholar]
- Chudley, A.E.; Conry, J.; Cook, J.L.; Loock, C.; Rosales, T.; LeBlanc, N.; Public Health Agency of Canada’s National Advisory Committee on Fetal Alcohol Spectrum Disorder. Fetal alcohol spectrum disorder: Canadian guidelines for diagnosis. Can. Med. Assoc. J. 2005, 172, S1–S21. [Google Scholar]
- Rasmussen, C.; Horne, K.; Witol, A. Neurobehavioral functioning in children with fetal alcohol spectrum disorder. Child Neuropsychol. 2006, 12, 438–468. [Google Scholar] [CrossRef] [PubMed]
- Mattson, S.N.; Riley, E.P.; Gramling, L.; Delis, D.C.; Jones, K.L. Heavy prenatal alcohol exposure with or without physical features of fetal alcohol syndrome leads to IQ deficits. J. Pediatr. 1997, 131, 718–721. [Google Scholar] [CrossRef]
- Nash, K.; Stevens, S.; Rovet, J.; Fantus, E.; Nulman, I.; Sorbara, D.; Koren, G. Towards identifying a characteristic neuropsychological profile for fetal alcohol spectrum disorders. 1. Analysis of the Motherisk FASD Clinic. J. Popul. Ther. Clin. Pharmacol. 2013, 20, e44–e52. [Google Scholar] [PubMed]
- Olson, H.C.; Sampson, P.D.; Barr, H.; Streissguth, A.P.; Bookstein, F.L. Prenatal exposure to alcohol and school problems in late childhood: A longitudinal prospective study. Dev. Psychopathol. 1992, 4, 341–359. [Google Scholar] [CrossRef]
- Howell, K.K.; Lynch, M.E.; Platzman, K.A.; Smith, G.H.; Coles, C.D. Prenatal alcohol exposure and ability, academic achievement, and school functioning in adolescence: A longitudinal follow-up. J. Pediatr. Psychol. 2006, 31, 116–126. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, C.M.; Taylor, C.; Zubrick, S.R.; Kurinczuk, J.J.; Bower, C. Prenatal alcohol exposure and educational achievement in children aged 8–9 years. Pediatrics 2013, 132, e468–e475. [Google Scholar] [CrossRef] [PubMed]
- Coles, C.D.; Kable, J.A.; Taddeo, E. Math performance and behavior problems in children affected by prenatal alcohol exposure: Intervention and follow-up. J. Dev. Behav. Pediatr. 2009, 30, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Mattson, S.N.; Riley, E.P.; Delis, D.C.; Stern, C.; Jones, K.L. Verbal learning and memory in children with fetal alcohol syndrome. Alcohol. Clin. Exp. Res. 1996, 20, 810–816. [Google Scholar] [CrossRef] [PubMed]
- Pei, J.R.; Rinaldi, C.M.; Rasmussen, C.; Massey, V.; Massey, D. Memory patterns of acquisition and retention of verbal and nonverbal information in children with fetal alcohol spectrum disorders. Can. J. Clin. Pharmacol. 2008, 15, 44–56. [Google Scholar]
- Willoughby, K.A.; Sheard, E.D.; Nash, K.; Rovet, J. Effects of prenatal alcohol exposure on hippocampal volume, verbal learning, and verbal and spatial recall in late childhood. J. Int. Neuropsychol. Soc. 2008, 14, 1022–1033. [Google Scholar] [CrossRef] [PubMed]
- Willford, J.A.; Richardson, G.A.; Leech, S.L.; Day, N.L. Verbal and visuospatial learning and memory function in children with moderate prenatal alcohol exposure. Alcohol. Clin. Exp. Res. 2004, 28, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Mattson, S.N.; Gramling, L.; Riley, E.P.; Delis, D.C.; Jones, K.L. Global-local processing in children prenatally exposed to alcohol. Child Neuropsychol. 1996, 2, 165–175. [Google Scholar] [CrossRef]
- Greenbaum, R.; Nulman, I.; Rovet, J.; Koren, G. The Toronto experience in diagnosing alcohol-related neurodevelopmental disorder: A unique profile of deficits and assets. Can. J. Clin. Pharmacol. 2002, 9, 215–225. [Google Scholar] [PubMed]
- Mattson, S.N.; Calarco, K.E.; Lang, A.R. Focused and shifting attention in children with heavy prenatal alcohol exposure. Neuropsychology 2006, 20, 361–369. [Google Scholar] [CrossRef] [PubMed]
- McGee, C.L.; Bjorkquist, O.A.; Riley, E.P.; Mattson, S.N. Impaired language performance in young children with heavy prenatal alcohol exposure. Neurotoxicol. Teratol. 2009, 31, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, C. Executive functioning and working memory in fetal alcohol spectrum disorder. Alcohol. Clin. Exp. Res. 2005, 29, 1359–1367. [Google Scholar] [CrossRef] [PubMed]
- Kodituwakku, P. Defining the behavioral phenotype in children with fetal alcohol spectrum disorders: A review. Neurosci. Biobehav. Rev. 2007, 31, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Mattson, S.N.; Crocker, N.; Nguyen, T.T. Fetal alcohol spectrum disorders: neuropsychological and behavioral features. Neuropsychol. Rev. 2011, 21, 81–101. [Google Scholar] [CrossRef] [PubMed]
- Vaurio, L.; Riley, E.P.; Mattson, S.N. Neuropsychological comparison of children with heavy prenatal alcohol exposure and an IQ-matched comparison group. J. Int. Neuropsychol. Soc. 2011, 14, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Burden, M.J.; Jacobson, S.W.; Sokol, R.J.; Jacobson, J.L. Effects of prenatal alcohol exposure on attention and working memory at 7.5 years of age. Alcohol. Clin. Exp. Res. 2005, 29, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Green, C.R.; Mihic, A.M.; Nikkel, S.M.; Stade, B.C.; Rasmussen, C.; Munoz, D.P.; Reynolds, J.N. Executive function deficits in children with fetal alcohol spectrum disorders (FASD) measured using the Cambridge Neuropsychological Tests Automated Battery (CANTAB). J. Child Psychol. Psychiatry 2009, 50, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Kully-Martens, K.; Treit, S.; Pei, J.; Rasmussen, C. Affective decision-making on the Iowa gambling task in children and adolescents with fetal alcohol spectrum disorders. J. Int. Neuropsychol. Soc. 2013, 19, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Donald, K.A.; Eastman, E.; Howells, F.M.; Adnams, C.; Riley, E.P.; Woods, R.P.; Narr, K.L.; Stein, D.J. Neuroimaging effects of prenatal alcohol exposure on the developing human brain: A magnetic resonance imaging review. Acta Neuropsychiatr. 2015, 27, 251–269. [Google Scholar] [CrossRef] [PubMed]
- Astley, S.J.; Aylward, E.H.; Olson, H.C.; Kerns, K.; Brooks, A.; Coggins, T.E.; Davies, J.; Dorn, S.; Gendler, B.; Jirikowic, T.; et al. Magnetic resonance imaging outcomes from a comprehensive magnetic resonance study of children with fetal alcohol spectrum disorders. Alcohol. Clin. Exp. Res. 2009, 33, 1671–1689. [Google Scholar] [CrossRef] [PubMed]
- Sowell, E.R.; Trauner, D.A.; Gamst, A.; Jernigan, T.L. Development of cortical and subcortical brain structures in childhood and adolescence: A structural MRI study. Dev. Med. Child Neurol. 2002, 44, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Dudek, J.; Skocic, J.; Sheard, E.; Rovet, J. Hippocampal abnormalities in youth with alcohol-related neurodevelopmental disorder. J. Int. Neuropsychol. Soc. 2014, 20, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, S.W.; Jacobson, J.L.; Molteno, C.D.; Warton, C.M.R.; Wintermark, P.; Hoyme, H.E.; De Jong, G.; Taylor, P.; Warton, F.; Lindinger, N.M.; et al. Heavy prenatal alcohol exposure is related to smaller corpus callosum in newborn MRI scans. Alcohol. Clin. Exp. Res. 2017, 41, 965–975. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Roussotte, F.; Kan, E.; Sulik, K.K.; Mattson, S.N.; Riley, E.P.; Jones, K.L.; Adnams, C.M.; May, P.A.; O’Connor, M.J.; et al. Abnormal cortical thickness alterations in Fetal Alcohol Spectrum Disorders and their relationships with facial dysmorphology. Cereb. Cortex 2012, 22, 1170–1179. [Google Scholar] [CrossRef] [PubMed]
- Sowell, E.R.; Mattson, S.N.; Kan, E.; Thompson, P.M.; Riley, E.P.; Toga, A.W. Abnormal cortical thickness and brain behavior correlation patterns in individuals with heavy prenatal alcohol exposure. Cereb. Cortex 2008, 18, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.; Lebel, C.; Lepage, C.; Rasmussen, C.; Evans, A.; Wyper, K.; Pei, J.; Andrew, G.; Massey, A.; Massey, D.; et al. Developmental cortical thinning in fetal alcohol spectrum disorders. Neuroimage 2011, 58, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Rajaprakash, M.; Chakravarty, M.M.; Lerch, J.P.; Rovet, J. Cortical morphology in children with alcohol-related neurodevelopmental disorder. Brain Behav. 2014, 4, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Infante, M.A.; Moore, E.M.; Bischoff-Grethe, A.; Migliorini, R.; Mattson, S.N.; Riley, E.P. Atypical cortical gyrification in adolescents with histories of heavy prenatal alcohol exposure. Brain Res. 2015, 1624, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Hendrickson, T.J.; Mueller, B.A.; Sowell, E.R.; Mattson, S.N.; Coles, C.D.; Kable, J.A.; Jones, K.L.; Boys, C.J.; Lim, K.O.; Riley, E.P.; et al. Cortical gyrification is abnormal in children with prenatal alcohol exposure. NeuroImage Clin. 2017, 15, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Wozniak, J.R.; Mueller, B.A.; Chang, P.N.; Muetzel, R.L.; Caros, L.; Lim, K.O. Diffusion tensor imaging in children with fetal alcohol spectrum disorders. Alcohol. Clin. Exp. Res. 2006, 30, 1799–1806. [Google Scholar] [CrossRef] [PubMed]
- Lebel, C.; Walker, L.; Leemans, A.; Phillips, L.; Beaulieu, C. Microstructural maturation of the human brain from childhood to adulthood. Neuroimage 2008, 40, 1044–1055. [Google Scholar] [CrossRef] [PubMed]
- Sowell, E.R.; Johnson, A.; Kan, E.; Lu, L.H.; Van Horn, J.D.; Toga, A.W.; O’Connor, M.J.; Bookheimer, S.Y. Mapping white matter integrity and neurobehavioral correlates in children with fetal alcohol spectrum disorders. J. Neurosci. 2008, 28, 1313–1319. [Google Scholar] [CrossRef] [PubMed]
- Malisza, K.L.; Allman, A.A.; Shiloff, D.; Jakobson, L.; Longstaffe, S.; Chudley, A.E. Evaluation of spatial working memory function in children and adults with fetal alcohol spectrum disorders: A functional magnetic resonance imaging study. Pediatr. Res. 2005, 58, 1150–1157. [Google Scholar] [CrossRef] [PubMed]
- Spadoni, A.D.; Bazinet, A.D.; Fryer, S.L.; Tapert, S.F.; Mattson, S.N.; Riley, E.P. BOLD response during spatial working memory in youth with heavy prenatal alcohol exposure. Alcohol. Clin. Exp. Res. 2009, 33, 2067–2076. [Google Scholar] [CrossRef] [PubMed]
- O’Conaill, C.R.; Malisza, K.L.; Buss, J.L.; Bolster, R.B.; Clancy, C.; de Gervai, P.D.; Chudley, A.E.; Longstaffe, S. Visual search for feature conjunctions: An fMRI study comparing alcohol-related to neurodevelopmental disorder (ARND) to ADHD. J. Neurodev. Disord. 2015, 7, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Meintjes, E.M.; Jacobson, J.L.; Molteno, C.D.; Gatenby, J.C.; Warton, C.; Cannistraci, C.J.; Hoyme, H.E.; Robinson, L.K.; Khaole, N.; Gore, J.C.; et al. An fMRI study of number processing in children with Fetal Alcohol Syndrome. Alcohol. Clin. Exp. Res. 2010, 34, 1450–1464. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Coles, C.C.; Lynch, M.E. Occipital-temporal reduction and sustained visual attention deficit in prenatal alcohol exposed adults. Brain Imaging Behav. 2008, 2, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Roussotte, F.F.; Bramen, J.E.; Nunez, S.C.; Quandt, L.C.; Smith, L.; O’Connor, M.J.; Bookheimer, S.Y.; Sowell, E.R. Abnormal brain activation during working memory in children with prenatal exposure to drugs of abuse: The effects of methamphetamine, alcohol, and polydrug exposure. Neuroimage 2011, 54, 3067–3075. [Google Scholar] [CrossRef] [PubMed]
- Fryer, S.L.; Tapert, S.F.; Mattson, S.N.; Paulus, M.P.; Spadoni, A.D.; Riley, E.P. Prenatal alcohol exposure affects frontal-striatal BOLD response during inhibitory control. Alcohol. Clin. Exp. Res. 2007, 31, 1415–1424. [Google Scholar] [CrossRef] [PubMed]
- Kodali, V.N.; Jacobson, J.L.; Lindinger, N.M.; Dodge, N.C.; Molteno, C.D.; Meintjes, E.M.; Jacobson, S.W. Differential recruitment of brain regions during response inhibition in children prenatally exposed to alcohol. Alcohol. Clin. Exp. Res. 2017, 41, 334–344. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.W.; Norman, A.L.; Fryer, S.L.; Tapert, S.F.; Paulus, M.P.; Jones, K.L.; Riley, E.P.; Mattson, S.N. Effect of predictive cuing on response inhibition in children with heavy prenatal alcohol exposure. Alcohol. Clin. Exp. Res. 2013, 37, 644–654. [Google Scholar] [CrossRef] [PubMed]
- Ware, A.L.; Infante, M.A.; O’Brien, J.W.; Tapert, S.F.; Jones, K.L.; Riley, E.P.; Mattson, S.N. An fMRI study of behavioral response inhibition in adolescents with and without histories of heavy prenatal alcohol exposure. Behav. Brain Res. 2015, 278, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Seguin, D.; Gerlai, R. Fetal alcohol spectrum disorders: Zebrafish in the analysis of the milder and more prevalent form of the disorder. Behav. Brain Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Ware, A.L.; Glass, L.; Crocker, N.; Deweese, B.N.; Coles, C.D.; Kable, J.A.; May, P.A.; Kalberg, W.O.; Sowell, E.R.; Jones, K.L.; et al. Effects of prenatal alcohol exposure and attention-deficit/hyperactivity disorder on adaptive functioning. Alcohol. Clin. Exp. Res. 2014, 38, 1439–1447. [Google Scholar] [CrossRef] [PubMed]
- Kodituwakku, P. A neurodevelopmental framework for the development of interventions for children with fetal alcohol spectrum disorders. Alcohol 2010, 44, 717–728. [Google Scholar] [CrossRef] [PubMed]
- Coles, C.D.; Smith, I.E.; Falek, A. Prenatal alcohol exposure and infant behavior: Immediate effects and implications for later development. Adv. Alcohol Subst. Abuse 1987, 6, 87–104. [Google Scholar] [CrossRef] [PubMed]
- McLachlan, K.; Pei, J.; Kully-Martens, K.; Rasmussen, C. Performance- and questionnaire-based tools for the evaluation of executive function in children and adolescents with fetal alcohol spectrum disorder. Int. J. Dev. Neurosci. 2015. [Google Scholar] [CrossRef]
- Kodituwakku, P.W.; Handmaker, N.S.; Cutler, S.K.; Weathersby, E.K.; Handmaker, S.D. Specific impairments in self-regulation in children exposed to alcohol prenatally. Alcohol. Clin. Exp. Res. 1995, 6, 1558–1564. [Google Scholar] [CrossRef]
- Khoury, J.E.; Milligan, K.; Girard, T.A. Executive functioning in children and adolescents prenatally exposed to alcohol: A meta-analytic review. Neuropsychol. Rev. 2015, 25, 149–170. [Google Scholar] [CrossRef] [PubMed]
- Lynch, M.E.; Kable, J.A.; Cole, C.D. Prenatal alcohol exposure, adaptive function, and entry into adult roles in a prospective study of young adults. Neurotoxicol. Teratol. 2015, 51, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Streissguth, A.P.; Bookstein, F.L.; Barr, H.M.; Sampson, P.D.; O’Malley, K.; Young, J.K. Risk factors for adverse life outcomes in fetal alcohol syndrome and fetal alcohol effects. J. Dev. Behav. Pediatr. 2004, 25, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Streissguth, A.P.; O’Malley, K. Neuropsychiatric implications and long-term consequences of fetal alcohol spectrum disorders. Semin. Clin. Neuropsychiatry 2000, 5, 177–190. [Google Scholar] [CrossRef] [PubMed]
- Fryer, S.L.; McGee, C.L.; Matt, G.E.; Riley, E.P.; Mattson, S.N. Evaluation of psychopathological conditions in children with heavy prenatal alcohol exposure. Pediatrics 2007, 119, e733–e741. [Google Scholar] [CrossRef] [PubMed]
- Greenbaum, R.L.; Stevens, S.A.; Nash, K.; Koren, G.; Rovet, J. Social cognitive and emotion processing abilities of children with Fetal Alchohol Spectrum Disorders: A comparison with attention Deficit Hyperactivity Disorder. Alcohol. Clin. Exp. Res. 2009, 33, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Steinhausen, H.C.; Nestler, V.; Spohr, H.L. Development of psychopathology of children with the fetal alcohol syndrome. J. Dev. Behav. Pediatr. 1982, 3, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Stevens, S.; Dudek, J.; Nash, K.; Koren, G.; Rovet, J. Social perspective taking and empathy in children with fetal alcohol spectrum disorders. J. Int. Neuropsychol. Soc. 2015, 21, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Bhatara, V.; Loudenberg, R.; Ellis, E. Association of attention deficit hyperactivity disorder and gestational alcohol axposure. J. Atten. Disord. 2006, 9, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Nash, K.; Koren, G.; Rovet, J. A differential approach for examining the behavioural phenotype of fetal alcohol spectrum disorders. J. Popul. Ther. Clin. Pharmacol. 2011, 18, 440–453. [Google Scholar]
- Streissguth, A.P.; Barr, H.M.; Kogan, J.; Bookstein, F.L. Understanding the Occurrence of Secondary Disabilities in Clients with Fetal Alcohol Syndrome (FAS) and Fetal Alcohol Effects (FAE); Final Report; University of Washington School of Medicine: Seattle, WA, USA, 1996. [Google Scholar]
- Rangmar, J.; Hjern, A.; Vinnerljung, B.; Stromland, K.; Aronson, M.; Fahlke, C. Psychosocial outcome of fetal alcohol syndrome in adulthood. Pediatrics 2015, 135, e52–e58. [Google Scholar] [CrossRef] [PubMed]
- O’Malley, K.; Huggins, J. Suicidality in adolescents and adults with fetal alcohol spectrum disorders. Can. J. Pscyhiatry 2005, 50, 125. [Google Scholar] [CrossRef] [PubMed]
- Warren, K.R.; Hewitt, B.G.; Thomas, J.D. Fetal alcohol spectrum disorders: Research challenges and opportunities. Alcohol Res. Health 2011, 34, 4–14. [Google Scholar] [PubMed]
- Mukherjee, R.; Cook, P.A.; Fleming, K.M.; Norgate, S.H. What can be done to lessen morbidity associated with fetal alcohol spectrum disorders? Arch. Dis. Child. 2017, 201, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Lupton, C.; Burd, L.; Harwood, R. Cost of fetal alcohol spectrum disorders. Am. J. Med. Genet. Part C 2004, 127, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Stade, B.; Ungar, W.J.; Stevens, B.; Beyen, J.; Koren, G. Cost of fetal alcohol spectrum disorder in Canada. Can. Fam. Phys. 2007, 53, 1303–1304. [Google Scholar]
- Popova, S.; Lange, S.; Burd, L.; Rehm, J. The economic burden of fetal alcohol spectrum disorder in Canada in 2013. Alcohol Alcohol. 2016, 51, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Peadon, E.; Rhys-Jones, B.; Bower, C.; Elliott, E.J. Systematic review of interventions for children with Fetal Alcohol Spectrum Disorders. BMC Pediatr. 2009, 9, 35. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, J. Interventions for children with fetal alcohol spectrum disorders (FASDs): Overview of findings for five innovative research projects. Res. Dev. Disabil. 2009, 30, 986–1006. [Google Scholar] [CrossRef] [PubMed]
- Reid, N.; Dawe, S.; Shelton, D.; Harnett, P.; Warner, J.; Armstrong, E.; LeGros, K.; O’Callaghan, F. Systematic review of fetal alcohol spectrum disorder interventions across the life span. Alcohol. Clin. Exp. Res. 2015, 39, 2283–2295. [Google Scholar] [CrossRef] [PubMed]
- Society, C.P. Fetal alcohol syndrome. Paediatr. Child Health 2002, 7, 161–174. [Google Scholar]
- Williams, M.S.; Schellenberger, S. “How Does Your Engine Run?” A Leader’s Guide to the Alert Program for Self Regulation; Therapy Works: Albuquerque, NM, USA, 1996. [Google Scholar]
- Barnes, K.J.; Vogel, K.A.; Beck, A.J.; Schoenfeld, H.B.; Owen, S.V. Self-regulation strategies of children with emotional disturbance. Phys. Occup. Ther. Pediatr. 2008, 28, 369–387. [Google Scholar] [CrossRef] [PubMed]
- Wells, A.M.; Chasnoff, I.J.; Schmidt, C.A.; Telford, E.; Schwartz, L.D. Neurocognitive habilitation therapy for children with fetal alcohol spectrum disorders: An adaptation of the Alert Program. Am. J. Occup. Ther. 2012, 66, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Nash, K.; Stevens, S.; Greenbaum, R.; Weiner, J.; Koren, G.; Rovet, J. Improving executive functioning in children with fetal alcohol spectrum disorders. Child Neuropsychol. 2015, 21, 191–209. [Google Scholar] [CrossRef] [PubMed]
- Soh, D.W.; Skocic, J.; Nash, K.; Stevens, S.; Turner, G.R.; Rovet, J. Self-regulation therpay increases frontal gray matter in children with fetal alcohol spectrum disorder: Evaluation by voxel-based morphometry. Front. Hum. Neurosci. 2015, 9, 108. [Google Scholar] [CrossRef] [PubMed]
- Astley, S.J.; Clarren, S.K. A fetal alcohol syndrome screening tool. Alcohol. Clin. Exp. Res. 1995, 19, 1565–1571. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, D. Wechsler Abbreviated Scale of Intelligence (WASI); The Psychological Corporation: San Antonio, TX, USA, 1999. [Google Scholar]
- Durston, S. Differential patterns of striatal activation in young children with and without ADHD. Biol. Psychiatry 2003, 53, 871–878. [Google Scholar] [CrossRef]
- Fassbender, C.; Murphy, K.; Foxe, J.J.; Wylie, G.R.; Javitt, D.C.; Robertson, I.H.; Garavan, H. A topography of executive functions and their interactions revealed by functional magnetic resonance imaging. Cognit. Brain Res. 2004, 20, 132–143. [Google Scholar] [CrossRef] [PubMed]
- Sackler Institute Website. Available online: www.sacklerinstitute.org/cornell/assays_and_tools/ (accessed on 1 July 2009).
- Tzourio-Mazoyer, N.; Landeau, B.; Papathanassiou, D.; Crivello, F.; Etard, O.; Delcroix, N.; Mazoyer, B.; Joliot, M. Automated anatomical labelling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single subject brain. NeuroImage 2002, 15, 273–289. [Google Scholar] [CrossRef] [PubMed]
- Durston, S.; Thomas, K.M.; Yang, Y.; Ulug, A.M.; Zimmerman, R.D.; Casey, B.J. A neural basis for the development of inhibitory control. Dev. Sci. 2002, 5, F9–F16. [Google Scholar] [CrossRef]
- Stevens, M.C.; Kiehl, K.A.; Pearlson, G.D.; Calhoun, V.D. Functional neural networks underlying response inhibition in adolescents and adults. Behav. Brain Res. 2007, 181, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Goldin, P.R.; McRae, K.; Ramel, W.; Gross, J.J. The neural bases of emotion regulation: Reappraisal and suppression of negative emotion. Biol. Psychiatry 2008, 63, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Janssen, T.W.P.; Heslenfeld, D.J.; van Mourik, R.; Logan, G.D.; Oosterlaan, J. Neural correlates of response inhibition in children with attention-deficit/hyperactivity disorder: A controlled version of the stop-signal task. Psychiatry Res. Neuroimaging 2015, 233, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Bertocci, M.A.; Bebko, G.; Versace, A.; Iyengar, S.; Bonar, L.; Forbes, E.E.; Almeida, J.R.C.; Perlman, S.B.; Schirda, C.; Travis, M.J.; et al. Reward-related neural activity and structure predict future substance use in dysregulated youth. Psychol. Med. 2017, 47, 1357–1369. [Google Scholar] [CrossRef] [PubMed]
- De Meo, E.; Moiola, L.; Ghezzi, A.; Veggiotti, P.; Capra, R.; Amato, M.P.; Pagani, E.; Fiorino, A.; Pippolo, L.; Pera, M.C.; et al. MRI substrates of sustained attention system and cognitive impairment in pediatric MS patients. Neurology 2017, 89, 1265–1273. [Google Scholar] [CrossRef] [PubMed]
- Bigler, E.D.; Mortensen, S.; Neeley, E.S.; Ozonoff, S.; Krasny, L.; Johnson, M.; Lu, J.; Provencal, S.L.; McMahon, W.; Lainhart, J.E. Superior temporal gyrus, language function, and autism. Dev. Neuropsychol. 2007, 31, 217–238. [Google Scholar] [CrossRef] [PubMed]
- Radua, J.; Phillips, M.L.; Russell, T.; Lawrence, N.; Marshall, N.; Kalidindi, S.; El-Hage, W.; McDonald, C.; Giampietro, V.; Brammer, M.J.; et al. Neural response to specific components of fearful faces in healthy schizophrenic adults. Neuroimage 2010, 49, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Vogan, V.M.; Morgan, B.R.; Powell, T.L.; Smith, M.L.; Taylor, M.J. The neurodevelopmental differences of increasing verbal working memory demand in children and adults. Dev. Cognit. Neurosci. 2015, 17, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Longo, C.A.; Fried, P.A.; Cameron, I.; Smith, A.M. The long-term effects of prenatal nicotine exposure on response inhibition: An fMRI study of young adults. Neurotoxicol. Teratol. 2013, 39, 9–18. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | TXT (N = 12) | WL (N = 13) | p-Value |
|---|---|---|---|
| Sex (% male) | 50 | 54 | |
| Age (mean ± SD) | 10.3 ± 1.7 | 10.4 ± 1.3 | ns |
| Birth weight (kg) | 2.9 ± 0.68 | 3.0 ± 0.74 | ns |
| Placement Status: | |||
| % Adopted | 75 | 54 | ns |
| % Fostered | 17 | 8 | ns |
| % With biological relative | 8 | 38 | ns |
| Socioeconomic Status | |||
| % Low | 42 | 69 | ns |
| % Medium | 42 | 8 | ns |
| % High | 16 | 23 | ns |
| Exposure History | |||
| % Alcohol and cigarettes | 58 | 77 | ns |
| % Alcohol and secondary drugs | 67 | 23 | 0.05 |
| Comorbidities | |||
| % Attention Deficit Hyperactivity Disorder | 75 | 85 | ns |
| % Oppositional Defiant Disorder | 25 | 15 | ns |
| % Learning Disorder diagnosis | 50 | 38 | ns |
| % Anxiety diagnosis | 0 | 15 | ns |
| % Sensory Processing Delay Diagnosis | 8 | 8 | ns |
| % Receiving stimulant medications | 67 | 54 | ns |
| Full Scale IQ (mean ± SD) | 86.3 ± 12.7 | 92.7 ± 15.3 | ns |
| Variables | TXT | WL | ||
|---|---|---|---|---|
| Pre | Post | Pre | Post | |
| Accuracy | ||||
| Go trials | 0.859 ± 0.14 | 0.881 ± 0.14 | 0.893 ± 0.08 | 0.848 ± 0.08 |
| NoGo trials | 0.548 ± 0.20 | 0.624 ± 0.16 | 0.430 ± 0.20 | 0.484 ± 0.19 |
| Go minus NoGo | 0.311 ± 0.18 | 0.257 ± 0.256 | 0.463 ± 0.16 | 0.364 ± 0.23 |
| Reaction time (ms) a | ||||
| Go trials | 0.441 ± 0.09 | 0.432 ± 0.14 | 0.400 ± 0.08 | 0.404 ± 0.11 |
| Contrast | Region BA | MNI Coordinates | Z-Score | FDR p-Value | SVC p-Value | Cluster Size | |||
|---|---|---|---|---|---|---|---|---|---|
| Between-Group Comparisons | |||||||||
| Waitlist > Treatment | Right medial frontal gyrus | 8 | 8 | 24 | 52 | 2.54 | 0.350 | 0.006 | 12 |
| Left frontal subgyral | WM | −24 | 0 | 32 | 2.64 | 0.350 | 0.004 | 15 | |
| Right cingulate gyrus | 32 | 16 | 20 | 28 | 2.85 | 0.350 | 0.002 | 30 | |
| Left cingulate gyrus | 24 | −12 | −16 | 40 | 2.78 | 0.350 | 0.003 | 12 | |
| Right putamen | 24 | 20 | −16 | 2.99 | 0.350 | 0.001 | 21 | ||
| Right superior temporal gyrus | 22 | 56 | −56 | 16 | 3.19 | 0.350 | 0.001 | 10 | |
| Group X Time Interactions | |||||||||
| Right superior frontal gyrus | 6 | 16 | 12 | 56 | 2.75 | 0.677 | 0.003 | 26 | |
| Left middle frontal gyrus | 46 | −48 | 40 | 16 | 2.58 | 0.677 | 0.005 | 14 | |
| Left inferior parietal lobule | 40 | −56 | −40 | 52 | 2.84 | 0.677 | 0.002 | 17 | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nash, K.; Stevens, S.; Clairman, H.; Rovet, J. Preliminary Findings that a Targeted Intervention Leads to Altered Brain Function in Children with Fetal Alcohol Spectrum Disorder. Brain Sci. 2018, 8, 7. https://doi.org/10.3390/brainsci8010007
Nash K, Stevens S, Clairman H, Rovet J. Preliminary Findings that a Targeted Intervention Leads to Altered Brain Function in Children with Fetal Alcohol Spectrum Disorder. Brain Sciences. 2018; 8(1):7. https://doi.org/10.3390/brainsci8010007
Chicago/Turabian StyleNash, Kelly, Sara Stevens, Hayyah Clairman, and Joanne Rovet. 2018. "Preliminary Findings that a Targeted Intervention Leads to Altered Brain Function in Children with Fetal Alcohol Spectrum Disorder" Brain Sciences 8, no. 1: 7. https://doi.org/10.3390/brainsci8010007