
The Human Factors and Ergonomics of P300-Based Brain-Computer Interfaces

Abstract
:1. Introduction
2. Review Objectives
3. Review Method
- What signal evocation methods yield improved performance or satisfaction in subjects?
- What environmental interventions can yield improved performance or satisfaction in subjects?
- How can user acceptance be measured in currently available BCI technologies? Which concepts from HFE may increase user acceptance rates of P300-based BCI systems applied in assistive technology?
3.1. Eligibility Criteria
3.2. Information Sources
- Compendex, to provide an engineering perspective;
- IEEExplore, to provide a targeted electrical/electronics engineering perspective;
- MEDLINE, to provide a medical perspective; and
- Web of Science, to provide a broad-spectrum perspective.
3.3. Search
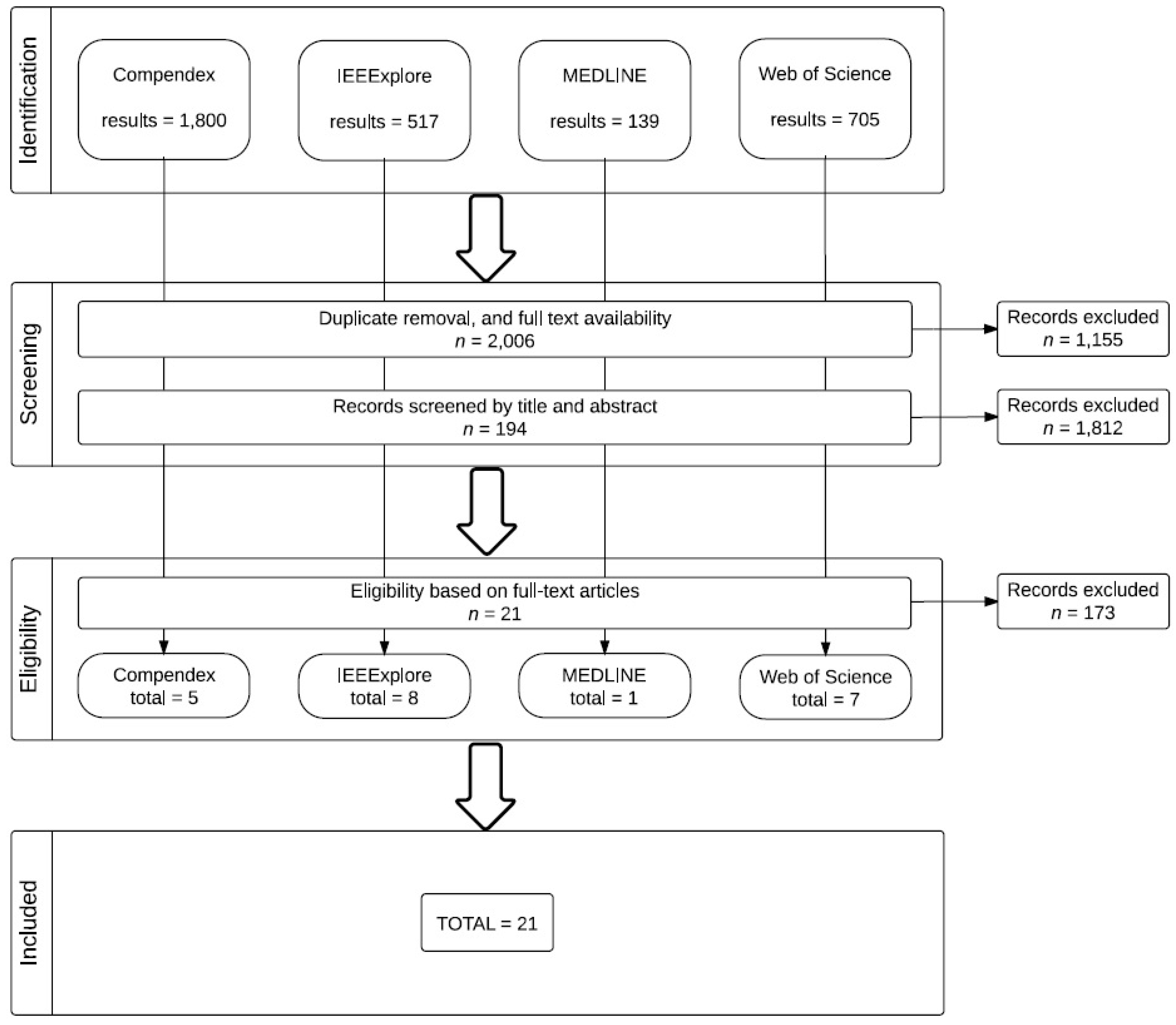
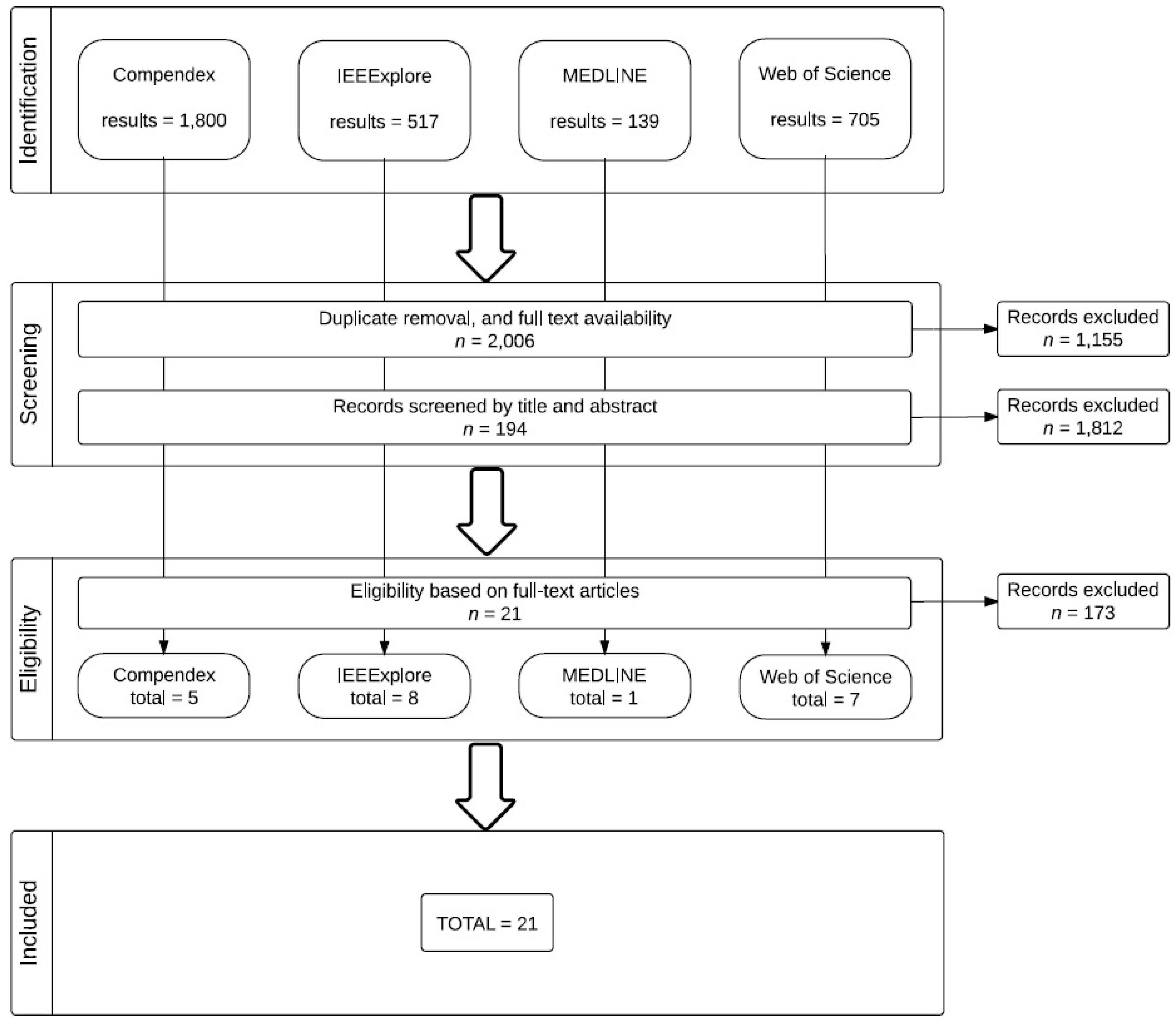
3.4. Study Selection
3.5. Data Items
- Population: Initially, we screened for studies with representative subjects (i.e., subjects with neuromuscular disabilities and assistive needs), but, due to the small-n problem, we decided not to exclude useful studies if they included only healthy participants. We excluded no study on the basis of subject age, gender, or specific neuromuscular disability.
- Interventions: For RQ1, we screened for studies that demonstrated or compared alternative implementations of the oddball paradigm to evoke the P300 wave. For RQ2, we screened for studies that demonstrated or compared alternative BCI implementation environments. For RQ3, we screened for studies that measured usability and/or user acceptance of assistive technologies using BCI.
- Comparators: We screened for studies with a design that included a control group or that managed treatments so as to provide a functional control comparison. Given the nature of BCI research on assistive technologies, there were rarely true controls. Most often, we selected studies that compared treatments or levels of a given treatment, or both. However, we did not exclude studies that sought to demonstrate a new assistive application, if such study informed our research questions.
- Outcomes: We screened for studies that accounted for user satisfaction or acceptance among its outcome metrics. For studies that did not explicitly include such a component, we screened for those studies the outcomes of which could be logically linked with user acceptance (improved performance in simulated life tasks, increased comfort, virtual or actual self-directed mobility, etc.)
- Study designs: Given the nature of BCI research on assistive technologies, there is a narrow range of study designs employed. Most frequently we encountered small-n, within-subject designs. That said, we did not screen for design type, beyond the requirement already stated that the design involve human subjects.
4. Review Results
4.1. Study Selection
4.2. Study Summaries

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Salvaris and Sepulveda (2009) [43] | Townsend et al. (2010) [44] | Acqualagna et al. (2010) [45] | Aloise et al. (2012) [46] | |
|---|---|---|---|---|
| Aim | To study the effect of changes to the visual aspects of oddball protocol, e.g., dimensions of the symbols, distance between the symbols, and colors | To compare checkerboard paradigm with the conventional row and column paradigm | To test a novel rapid serial visual presentation paradigm in an offline study, investigating two different presentation speeds and two different color conditions | To study and compare performances of gaze-independent P300-based BCI and the conventional P300 speller interface |
| Study design | Within-subject | Within-subject | Within-subject | Within-subject |
| Participants | 8 | 18 | 9 | 10 |
| Age | Mean 22.3, 19–28 | Undergraduate students | 24–31 | Mean 26.82, σ = 4.21 |
| Gender ratio (male:female) | 6:2 | 11:7 | 8:1 | 6:4 |
| Disabled participants | 0 | 3 | 0 | 0 |
| Type of non-healthy participant | N/A | ALS | N/A | N/A |
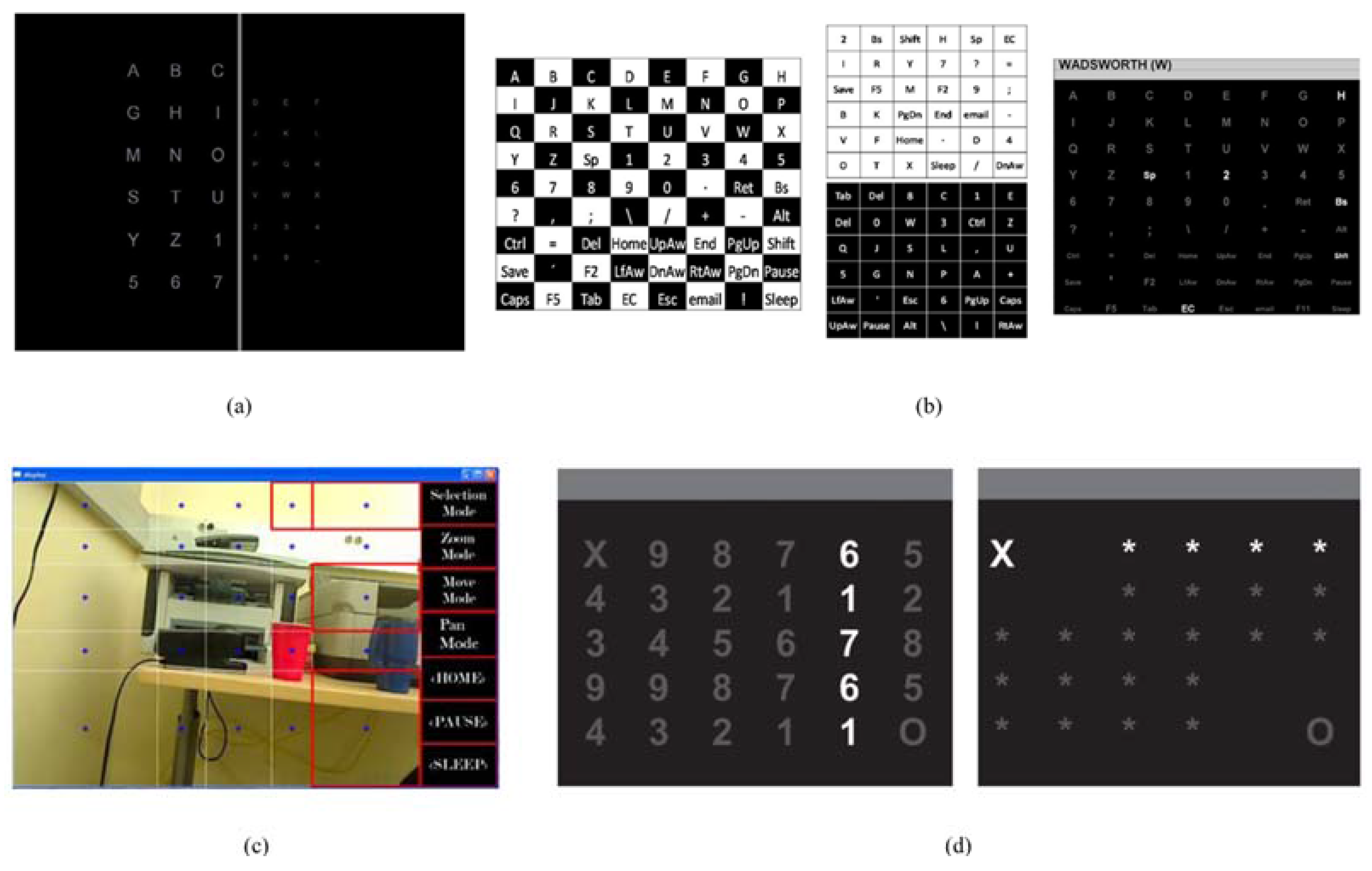
| Signal evocation method | Conventional oddball (6 × 6 matrix) | 8 × 9 matrix | Stimuli presented in the center of the screen on a gray background, with a height of 3.5 cm or 1° visual angle | Each character belonged to two sets of size n. Each set presented at the center of screen, forming a regular geometric figure, with characters displayed at the vertices |
| Interface construction | EEG with Biosemi ActiveTwo system at a sampling rate of 512 Hz; 66 channels were used, including 2 as reference; out of the 64, 8 were selected according to performance Participants sat 1 m from a 19 inch TFT screen | EGG with a standard 32-channel electrode cap; amplified and digitized by two g.tex 16-channel USB biosignal amplifiers; ALS users sat in their wheelchairs Participant sat 1 m from a computer monitor | EEG with a 64-channel actiCAP system; EEG data were sampled at a rate of 1000 Hz and subjected to off-line analysis Participants sat 80 cm from a computer monitor | Scalp EEG potentials were measured using 10–10 standard on an elastic cap; the EEG was acquired using a g.USBamp amplifier, sampled at 256 Hz Eye movements were monitored on an eye tracker system |
| Environment | Laboratory | Laboratory | Laboratory | Laboratory |
| Acceptance measure | N/A | N/A | N/A | NASA workload metrics; User acceptance score (subjective) |
| Akram et al. (2013) [47] | Pathirage et al. (2013) [48] | Alcaide-Aguirre and Huggins et al. (2014) [49] | Ma et al. (2014) [50] | |
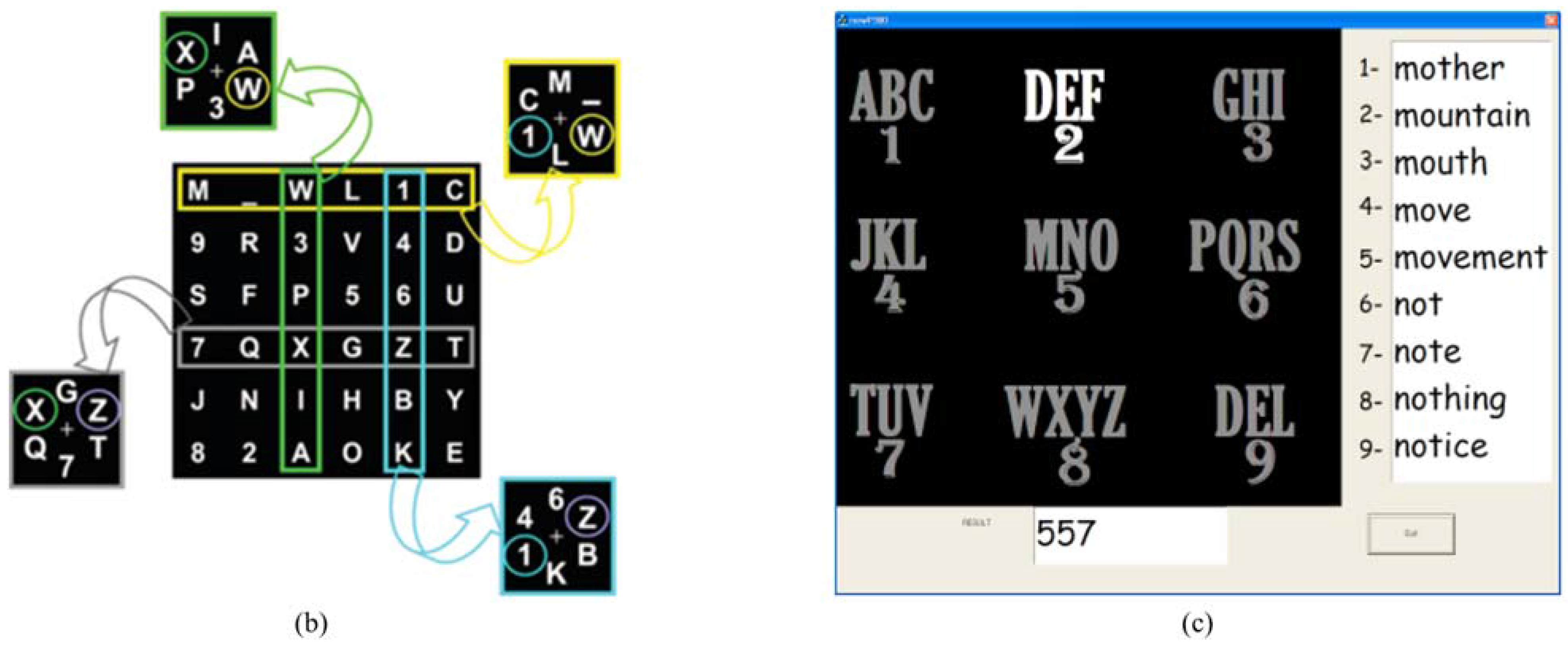
| Aim | To study a modified T9 (text on 9 keys) interface with word suggestions | To test an oddball-based paradigm with a visual interface to conduct daily living tasks; subjects could control a robotic arm mounted on wheelchair to grasp items under commands through the BCI | To evaluate a new P300 interface with reduced amount of information through series of experiments on performing hold-release and deactivation tasks | To study a hybrid P300-based EEG interface integrated with eye movement recognition, using both EEG and electrooculography (EOG), in performing two tasks of controlling robots |
| Study design | Within-subject | Proof of concept | Within-subject | Within-subject |
| Participants | 10 | 6 | 7 | 13 |
| Age | N/A | 24–40 | 14–40 | 22–30 |
| Gender ratio (male:female) | 10:0 | 5:1 | 5:2 | 11:2 |
| Disabled participants | 0 | 0 | 0 | 0 |
| Type of non-healthy participant | N/A | N/A | N/A | N/A |
| Signal evocation method | T9 interface | 5 × 5 non-uniform grid was constructed with algorithms, thus the oddball paradigm could be applied onto 25 points | 5 × 6 matrix for a P300 speller; two layouts were used, in one of which numbers were replaced with asterisks to reduce perceptual errors | Conventional oddball matrix interface for EEG evocation |
| Interface construction | EEG data was acquired through a 32-channel BrainAMP MR amplifier with a sampling frequency of 250 Hz; EEG potentials were measured using 10–20 standard | 8-channel electrode cap, a g-tec USBAmp-8 biological signal amplifier, the input signal was sampled at 256 Hz | 16-channel EEG electrode cap; subjects sat in front of a computer screen with BCI layout | EEG signal was recorded with 8 electrodes with a sampling rate of 256 Hz and was downsampled to 64 Hz Three event-related potential components were exploited: VPP, N170, and P300; P300 was evoked by oddball event, while the other two were evoked by the configural processing of facial image |
| Environment | Laboratory | Laboratory | Laboratory | Laboratory |
| Acceptance measure | N/A | N/A | N/A | N/A |
| Klobassa et al. (2009) [51] | Escolano et al. (2010) [52] | Castermans et al. (2011) [53] | Li et al. (2011) [34] | |
|---|---|---|---|---|
| Aim | To investigate auditory operation of P300 speller | To report a BCI telepresence system and to study its applicability to ALS patients | To investigate the use of P300-based BCI in an ambulatory condition | To evaluate contributing factors to user performance in BCI applications |
| Study design | Two-group, with partial control (mixed design: one group had constant treatment, while other group had treatment gradually reduced) | Proof of concept | Within-subject (each subject performing at three treatment levels) | Within-subject (two treatments at three levels of treatment) |
| Participants | 10 | 1 | 7 | 20 |
| Age | Mean 47, 22–68 | 54 | 25–33 | Healthy (mean 27.9, σ = 3.6) Disabled (mean 43.7, σ = 14.8) |
| Gender ratio (male:female) | 6:4 | Unknown | Unknown | 14:6 |
| Disabled participants | 0 | 1 | 0 | 10 |
| Type of disability | N/A | ALS | N/A | Various neuromuscular disabilities |
| Signal evocation method | Auditory and auditory/visual oddball Standard speller | Visual (iconic) oddball | Quasi-oddball (target not rare) Standard speller | ABC and Frequency oddball Standard speller |
| Interface construction | EEG cap, reclining chair | EEG, audio-visual interface over Internet | EEG cap, accelerometer strapped to head, lower limb kinematics, recorded with infrared cameras | EEG cap, each method tested in 3 screen sizes (monitor, GPS, and phone) at appropriate distance |
| Environment | Laboratory | Patient at home (Germany) Telepresence robot (Spain) | Laboratory Quasi-ambulatory (subject on treadmill) | Laboratory sedentary |
| Acceptance measure | N/A | N/A | N/A | N/A |
| Duvinage et al. (2013) [54] | Tai et al. (2013) [55] | Corralejo et al. (2014) [56] | Riccio et al. (2015) [57] | |
| Aim | To compare medical-grade and consumer-grade EEG BCI by comparing performance in P300 | To propose a BCI to enable disabled individuals to utilize the Internet | To develop and assess an assistive tool for operating electronic devices at home by means of P300-based BCI | To evaluate hybrid P300-based BCI with electromyographic error correction |
| Study design | Within-subject (4 crossed treatments: consumer vs. medical, sitting vs. treadmill) | Proof of concept | Proof of concept | Proof of concept, and within-subject (2 treatments: P300 control and P300 w/correction) |
| Participants | 9 | 14 | 15 | 11 |
| Age | 24–34 | 20–25 | Mean 50.27, 35–68 | Healthy (28 ± 7) Disabled (48, 54, 49) |
| Gender ratio (male:female) | 8:1 | Unknown | 7:8 | Healthy (5:3) Disabled (2:1) |
| Disabled participants | 0 | 0 | 15 | 3 |
| Type of disability | N/A | N/A | Varied motor and cognitive disabilities | Severe motor disabilities |
| Signal evocation method | Visual oddball | Visual oddball | P3Speller-based Visual (iconic) Matrix menu based | Visual (color and shape) |
| Interface construction | Emotiv Epoc (8 channel) ANT (used at same positions) | Not explicit | EEG | EEG and EEG+EMG |
| Environment | Laboratory sedentary and ambulatory | Not explicit Laboratory | Laboratory | Laboratory |
| Acceptance measure | N/A | N/A | Questionnaire | Interview |
| Lightbody et al. (2010) [58] | Riccio et al. (2011) [59] | Holz et al. (2013) [60] | |
| Aim | To develop a BCI system that is customizable in terms of its technology and applications | To evaluate usability through subject performance, workload, and satisfaction and to compare two applications for P300-based BCI | To evaluate usability of new SMR-BCI-controlled gaming prototype based on effectiveness, efficiency, and user satisfaction |
| Study design | Proof of concept | Within-subject | Within-subject |
| Study description | Quantitative and qualitative research of user requirements in a 3-year iterative development; SSVP, ERD/ERD, and P300 paradigms; six 30-minute sessions with 4 oscillatory visual stimuli (30, 35, 40, and 45 Hz) presented simultaneously | 2 conditions: split—oddball screen to select command and application screen where commands were executed; overlaid—oddball paradigm overlaid the application; 3 tasks: Internet browsing, word processing, and software configuration | 6 sessions of BCI interactions with Connect-Four, strategic game with two competitive players; 2 types of tasks: copy task and free playing mode |
| Participants | 20 | 8 | 4 |
| Age | Unknown | 26.7 ± 1.3 years | 45–48 |
| Gender ratio (male:female) | Unknown | 6:2 | Unknown |
| Disabled participants | 5 | 0 | 4 |
| Type of non-healthy participant | Varied motor and cognitive disabilities | N/A | Severe motor disabilities; 2 out of 4 were locked-in |
| Signal evocation method | Visual (stimuli rendered through LEDs on the outer edges of the screen) | Visual | Visual |
| Interface construction | EEG; Mightex-universal LED controller; TMSi Porti amplifier at a sampling rate of 2048 Hz | EEG; g.USBamp. amplifier; BCI2000 brain transducer | EEG; 2-class SMR-BCI game; Brain Vision and g.USBamp. amplifiers; |
| Environment | Laboratory | Laboratory | Laboratory |
| Acceptance measure | Workshops, questionnaire, and focus group | NASA Task Load Index (TLX) questionnaire for subjective workload, visual analogue scale for user satisfaction, and unstructured interview | NASA TLX for subjective workload; visual analogue scale for overall satisfaction; Extended QUEST and ATD-PA for satisfaction regarding different dimensions of BCI device; semi-structured interview and focus group |
| Bonnet et al. (2013) [61] | Zickler et al. (2013) [62] | ||
| Aim | To design and implement a multi-user BCI-based gaming system and to qualify and quantify the influence of multi-user paradigm on BCI interaction | To evaluate usability of the Brain Painting prototype according to the standards of the International Organization for Standardization. | |
| Study design | Within-subject | Within-subject | |
| Study description | Brain Arena, simple football video game based on hand motor imagery (MI), evaluated based on 3 paradigms (solo, collaborative, and competitive) in 2 experiments; classification accuracy = performance metric | 3 tasks: copy spelling, copy painting, and free painting; 2 monitors for painting: BCI command screen and “canvas”; recalibration available to support accuracy of at least 80% | |
| Participants | 20 | 4 | |
| Age | 23–52 | 39–55 | |
| Gender ratio (male:female) | 15:5 | Unknown | |
| Disabled participants | Unknown | 4 | |
| Type of non-healthy participant | Unknown | Varied motor and cognitive disabilities | |
| Signal evocation method | Visual | Visual | |
| Interface construction | EEG; USBAmp amplifiers; GAMMA Caps with 16 active electrodes; OpenVibe software platform; Ogre 3D rendering engine | EEG; 6x8 matrix for P300 spelling and Brain Painting app; g.USBamp. amplifier; BCI2000 software; Brain Vision Analyzer 2 | |
| Environment | Laboratory | Laboratory and field (at home with external distractions) | |
| Acceptance measure | Questionnaire (Likert scale, open questions) | Accuracy to measure effectiveness; ITR and utility metric for efficiency; NASA TLX for subjective workload; QUEST and ATD PA for user satisfaction; semi-structured interview | |
4.3. Study Characteristics
4.3.1. Participants
4.3.2. Experimental Design
4.3.3. Study Environment
4.4. Results of Individual Studies
4.4.1. Studies Selected for RQ1
4.4.2. Studies Selected for RQ2
4.4.3. Studies Selected for RQ3
5. Discussion
5.1. Summary of Evidence
5.1.1. Evidence for RQ1
- After proof-of-concept studies, researchers need to conduct quantitative investigation on various configuration parameters, so that the prototype system can achieve better performance in terms of HFE. That is to say, having established proof-of-concept, while it is important to investigate further extensions or applications of the concept, possible improvements to its fundamental characteristics should not be ignored. Examination of approaches to yield incremental BCI improvement, and thus HFE improvement, can be incorporated into whole-system tests. For example, in a case such as Pathirage et al. (2013) [48], further investigation of the wheelchair-mounted robotic arm could incorporate testing of variations on the configuration of the non-uniform grid to see what configurations yield improved HFE, and thus overall system performance.
- Comparison with the conventional paradigm is recommended as it would convey more information on performance metrics. In a manner similar to Aloise et al. (2012) [46] and Townsend et al. (2010) [44], comparing the performance of the well-established matrix oddball paradigm with variations or departures from it, as utilized by a common set of test subjects, allows the research community to develop baselines of BCI performance, and to better gauge the implications of new approaches to the conventional paradigm. For example, while the results of Akram et al. (2013) [47] are promising, they would be made stronger had the researchers conducted actual trials of the conventional speller with the test subjects, rather than only computing expected task times, in order to allow for proper comparison with their experimental results.
- Although adequate sample size is not always possible, researchers should try to find more users that fit the specific usage of the BCI system. This is particularly important for designs that are targeting certain clinical groups. Of the eight articles reviewed for RQ1, only Townsend et al. [44] involved clinical participants, and then only three participants with ALS among 15 non-clinical undergraduates. That said, it cannot be assumed that all BCI research has in mind the development of BCIs for assistive use. If the research is simply of a general nature, then the selection of test subjects is not critical. However, if the research is intended to be of benefit to assistive technologies or to certain clinical groups, then it should be made explicit and every effort should be made to involve appropriate clinical participants in the research. If research has not been conducted with clinical participants, then it can only be considered as proof-of-concept, regardless of the degree of success or development of the underlying techniques or systems. Given that certain clinical groups have a small population in absolute terms (such as ALS patients), perhaps some studies could involve participants with more common disabilities to simulate rarer clinical groups. For example, if work extending on Aloise et al. (2012) [46] were to be directed explicitly at developing assistive technologies, for example for patients with a neurodegenerative disease, it could be conducted with participants with oculomotor impairments only. The use of such “proxy” participants might actually be preferable in some cases in order to reduce potential confounds, as some clinical groups present simultaneously a broad variety of capacities and challenges.
5.1.2. Evidence for RQ2
- Make explicit the connections that real-world and real-world-applicable systems have to HFE. That is to say, BCI research is applied research, in that BCIs are tools that have human users, and which are intended to accomplish the users’ tasks. As such, HFE are an inescapable component of such research. HFE are always at play, regardless of whether or not researchers have addressed them. Thus, researchers must necessarily address them, as otherwise they become confounds. Addressing HFE explicitly will serve to reinforce such good practice in future work.
- Acknowledge the value of attending to HFE of users who already face severe challenges in this regard. Similarly, understand that HFE might have greater importance for clinical groups than for non-clinical groups. For example, Li et al. (2011) [34] acknowledged this, and as well made an explicit connection with HFE, as they framed their work in the following manner:
- “For those with motor disabilities, a greater degree of communication and control can enhance their self-confidence and positive attitude toward life. For these reasons, BCI applications provide hope and encouragement for people suffering from neurodegenerative diseases …. The degree of communication and control afforded to people with motor disabilities by BCI helps not only to make numerous simple tasks more convenient but also to reduce the burden of their caretakers.”
- Remember to view systems also from the perspective of users, and to evaluate them in this regard. Speaking directly to the question of cost vs. quality raised by Duvinage et al. (2013) [54], it could be that researchers should attend to the needs and capacities of users beyond what is evident in experimental settings. These needs and capacities furthermore often extend beyond individual users; Corralejo et al. (2014) [56] acknowledge this when they point out that increasing an individual’s autonomy and independence decreases dependence on nurses, caregivers and relatives. Researchers must keep in mind that unmeasured social or economic pressures might be as strong as any measured factors. Thus, HFE must be attended to, but they must also be expanded to incorporate socio-economic aspects of the user-system.
- In making explicit the value of attending to HFE to improve system performance, be also sure to make explicit the value of design that avoids potential HFE deficits. For example, while Castermans et al. (2011) [53] were somewhat ambivalent about the value of their findings, stepwise improvements that avoid the potential pitfalls of sedentary or overly noisy systems are not neutral in HFE terms—they are a benefit. Similarly, Klobassa et al. (2009) [51] reported throughput rates that were not impressive compared to those possible with the visual paradigm, but they made the important point that visual mobility often is eventually impaired or even lost among certain clinical groups—thus, an otherwise excellent hypothetical system designed only according to the visual paradigm would offer nothing to such clinical groups.
- Researchers must be aware that HFE for the disabled include more than the user—they also involve the user’s support network. Corralejo et al. (2014) [65] pointed out the benefit of their system not only to users, but also to caregivers. Similarly to point 3 above, researchers must have a social perspective on HFE for disabled users, as the human–machine system necessarily comprises more humans than the single user. Escolano et al. (2010) [52] acknowledged this in that they stated that their system was designed not only with the participation of patients (itself an essential factor), but as well with patients’ caregivers and family.
- Researchers should attend more to the affective element of HFE. For example, Escolano et al. (2010) [52] were unusual in that they noted that their system was “fun”. This is not a word commonly seen in the literature. Nevertheless, researchers should not underestimate the potential value of positive affect to overall performance and acceptance. Indeed, it is important that a research agenda be targeted on the affective component of HFE, given the degree of influence of affect upon cognition (e.g., Forgas (2008) [68]). Corralejo et al. (2014) [56] and Tai et al. (2013) [55] could have given attention to the affective elements, given the potential of their systems for individual entertainment or human interaction. It is important that the research community makes a point to remember the importance of these more diffuse human needs, and not simply decompose those needs into component tasks. If we do that, then we risk decomposing users likewise into component tasks, and thus dehumanizing them (a risk which they often already face [41]).
5.1.3. Evidence for RQ3
- The researchers working on advancing P300-based BCI in assistive technologies need to engage participants with disabilities, who represent the majority of the target user group. This is consonant with recommendation 3 of Section 5.1.1. However, that previous recommendation specifies the involvement of users that match the intended usage profile of the system. This recommendation more specifically stresses the participation of clinical groups. This is of great importance in research that addresses the question of user acceptance. For example, Riccio et al. (2011) [59] explicitly framed their research in the context of improving usability for those with severe motor disability. Yet, despite a comprehensive assessment of usability, which is laudable, the data were collected only from non-clinical participants. While the study did validate the utility of the HFE methodologies used, they did so only for healthy participants. As such methodologies generally have been developed by and for use on healthy individuals, we should not assume that they are immediately valid for non-healthy individuals (cf. Anderson 2009 [70]). The only way that the research community will be able to validate similar methodologies for clinical groups is through their participation in studies using existing methodologies, and having those methodologies adapted specifically to them.
- To yield valid user acceptance data characterizing technology that is intended to become a part of day-to-day life of users with disabilities, researchers need to conduct their tests not only in the lab, but in a real life-like environment, with multiple distracting factors and complex user-system interactions. That is to say, researchers must allow for environmental confounds, which make up the fabric of life outside of the laboratory. Zickler et al. (2013) [62] is an excellent example of this: EEG signals were not cleaned of artifacts such as eye blinks (as the researchers assumed real-world use in an environment full of artifacts), and “Daily life distractions, such as family members entering the room or telephone ringing were deliberately not avoided to guarantee for highest possible external validity.”
- The P300-based technology developers should attend to HFE concepts for design improvements, as the reviewed literature suggested, for instance: improved appearance of EEG caps, more conventional and user-friendly interfaces, simplified software installation processes, clarified training systems for software use, elimination of the need for participation of a trained EEG technician, interoperable systems development, and integration with other systems and devices. Holz et al. (2013) [60] is an excellent example of how to incorporate attention to such a design approach, and likewise how to measure user response and acceptance. While the researchers collected useful system performance data in various trials, it was in using the Extended QUEST 2.0 [64] to assess participants that the researchers learned that some users felt not only physically uncomfortable, but felt that they “look[ed] strange” in the EEG cap, or that they found the cabling distracting and uncomfortable, or that they desired a different training schedule, or that the EEG looked too much like the “hospital”. Users and researchers have different goals and needs; to ensure acceptance by users (and thus to be able to provide to them utility), researchers must not forget always to attend to those goals and needs, and to ask what they are instead of making assumptions.
5.2. Review Limitations
- The literature search was conducted only in English.
- The generalizability of the findings is hampered by the specificity of the concern (i.e., assistive technologies for individuals with certain neuromuscular impairments), and the resultant small number of representative test subjects (in our reviewed studies, n ranged only from 1 to 20).
- The bulk of research on P300-based BCI still addresses fundamentally technical issues, thus studies explicitly accounting for HFE are relatively few.
- Even among those studies addressing HFE, the goal is still technical (i.e., performance-oriented), as much technical development remains to improve the functioning of P300-based BCI systems, so that focus can be given to refining HFE. Despite the fact that these issues are related, HFE remain a secondary concern.
- It is difficult to isolate evocation methods and environmental/design variables, as each category impacts the other.
- Attention to user acceptance is confounded by the fact that many target users are impaired in ways and in degrees that leave them little choice in assistive technologies. And even though most authors of the articles reviewed for RQ3 agree on the importance of applying HFE methods to assess BCI technology in terms of subjective workload (NASA TLX), user satisfaction measurement, and accuracy, user acceptance is unfortunately often neglected.
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Daly, J.J.; Wolpaw, J.R. Brain-computer interfaces in neurological rehabilitation. Lancet Neurol. 2008, 7, 1032–1043. [Google Scholar]
- Vidal, J.J. Toward direct brain-computer communication. Annu. Rev. Biophys. Bioeng. 1973, 2, 157–180. [Google Scholar] [CrossRef]
- Elbert, T.; Rockstroh, B.; Lutzenberger, W.; Birbaumer, N. Biofeedback of slow cortical potentials. Electroencephalogr. Clin. Neurophysiol. 1980, 48, 293–301. [Google Scholar] [CrossRef]
- Shih, J.J.; Krusienski, D.J.; Wolpaw, J.R. Brain-computer interfaces in medicine. Mayo Clin. Proc. 2012, 87, 268–279. [Google Scholar] [CrossRef] [PubMed]
- Allison, B.Z.; Wolpaw, E.W.; Wolpaw, A.R. Brain-computer interface systems: Progress and prospects. Expert Rev. Med. Devices 2007, 4, 463–474. [Google Scholar] [CrossRef] [PubMed]
- Birbaumer, N. Breaking the silence: Brain-computer interfaces (BCI) for communication and motor control. Psychophysiology 2006, 43, 517–532. [Google Scholar] [CrossRef] [PubMed]
- Birbaumer, N.; Murguialday, A.R.; Cohen, L. Brain-computer interface in paralysis. Curr. Opin. Neurol. 2008, 21, 634–638. [Google Scholar] [CrossRef] [PubMed]
- Kübler, A.; Kotchoubey, B.; Kaiser, J.; Wolpaw, J.R.; Birbaumer, N. Brain-computer communication: Unlocking the locked in. Psychol. Bull. 2001, 127, 358–375. [Google Scholar] [CrossRef] [PubMed]
- Murguialday, A.R.; Hill, J.; Bensch, M.; Martens, S.; Halder, S.; Nijboer, F.; Schoelkopf, B.; Birbaumer, N.; Gharabaghi, A. Transition from the locked in to the completely locked-in state: A physiological analysis. Clin. Neurophysiol. 2011, 122, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, E.V.C.; Suttie, N.; Sivanathan, A.; Lim, T.; Louchart, S.; Pineda, J.A. Brain-computer interface game applications for combined neurofeedback and biofeedback treatment for children on the autism spectrum. Front. Neuroeng. 2014, 7, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Pineda, J.A.; Friedrich, E.V.C.; LaMarca, K. Neurorehabilitation of social dysfunctions: A model-based neurofeedback approach for low and high-functioning autism. Front. Neuroeng. 2014, 7, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Sun, Y.; Zeng, J.; Sun, H. Mirror neural training induced by virtual reality in brain-computer interfaces may provide a promising approach for the autism therapy. Med. Hypotheses 2011, 76, 646–647. [Google Scholar] [CrossRef] [PubMed]
- Geuze, J.; Farquhar, J.; Desain, P. Towards a communication brain computer interface based on semantic relations. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Lebedev, M.A.; Nicolelis, M.A.L. Brain-machine interfaces: Past, present and future. Trends Neurosci. 2006, 29, 536–546. [Google Scholar] [CrossRef] [PubMed]
- Sellers, E.W.; Ryan, D.B.; Hauser, C.K. Noninvasive brain-computer interface enables communication after brainstem stroke. Sci. Transl. Med. 2014, 6. [Google Scholar] [CrossRef] [PubMed]
- Wolpaw, J.R. Brain-computer interfaces. In Handbook of Clinical Neurology; Michael, P.B., David, C.G., Eds.; Elsevier: Amsterdam, The Netherlands, 2013; Volume 110, pp. 67–74. [Google Scholar]
- Huggins, J.E.; Moinuddin, A.A.; Chiodo, A.E.; Wren, P.A. What would brain-computer interface users want: Opinions and priorities of potential users with spinal cord injury. Arch. Phys. Med. Rehabil. 2015, 96. [Google Scholar] [CrossRef] [PubMed]
- King, C.; Wang, P.; Chui, L.; Do, A.; Nenadic, Z. Operation of a brain-computer interface walking simulator for individuals with spinal cord injury. J. Neuroeng. Rehabil. 2013, 10, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Rupp, R.; Rohm, M.; Schneiders, M.; Kreilinger, A.; Muller-Putz, G.R. Functional rehabilitation of the paralyzed upper extremity after spinal cord injury by noninvasive hybrid neuroprostheses. Proc. IEEE 2015, 103, 954–968. [Google Scholar] [CrossRef]
- Han, Y.; Bin, H. Brain-computer interfaces using sensorimotor rhythms: Current state and future perspectives. IEEE Trans. Biomed. Eng. 2014, 61, 1425–1435. [Google Scholar] [CrossRef] [PubMed]
- Papadelis, C.; Braun, C.; Pantazis, D.; Soekadar, S.R.; Bamidis, P. Using brain waves to control computers and machines. Adv. Hum. Comput. Interact. 2013, 2013, 1–2. [Google Scholar] [CrossRef]
- Ribeiro, P.R.D.A.; Brasil, F.L.; Witkowski, M.; Shiman, F.; Cipriani, C.; Vitiello, N.; Carrozza, M.C.; Soekadar, S.R. Controlling assistive machines in paralysis using brain waves and other biosignals. Adv. Hum. Comp. Interact. 2013, 2013, 1–9. [Google Scholar] [CrossRef]
- Wolpaw, J.R.; Birbaumer, N.; McFarland, D.J.; Pfurtscheller, G.; Vaughan, T.M. Brain-computer interfaces for communication and control. Clin. Neurophysiol. 2002, 113, 767–791. [Google Scholar] [CrossRef] [PubMed]
- Moghimi, S.; Kushki, A.; Guerguerian, A.M.; Chau, T. A review of EEG-based brain-computer interfaces as access pathways for individuals with severe disabilities. Assist. Technol. 2013, 25, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.D.; Borasio, G.D. Amyotrophic lateral sclerosis. Lancet 2007, 369, 2031–2041. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; Antao, V.; Kaye, W.; Sanchez, M.; Williamson, D.; Bryan, L.; Muravov, O.; Horton, K. Prevalence of amyotrophic lateral sclerosis—United States, 2010–2011. Morb. Mortal. Weekly Rep. 2014, 63, 1–14. [Google Scholar]
- Hillyard, S.A.; Kutas, M. Electrophysiology of cognitive processing. Annu. Rev. Psychol. 1983, 34, 33–61. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, W.S. Psychophysiology of P300. Psychol. Bull. 1981, 89, 506–540. [Google Scholar] [CrossRef] [PubMed]
- Duncan, C.C.; Barry, R.J.; Connolly, J.F.; Fischer, C.; Michie, P.T.; Naatanen, R.; Polich, J.; Reinvang, I.; van Petten, C. Event-related potentials in clinical research: Guidelines for eliciting, recording, and quantifying mismatch negativity, P300, and N400. Clin. Neurophysiol. 2009, 120, 1883–1908. [Google Scholar] [CrossRef] [PubMed]
- Duncan-Johnson, C.C.; Donchin, E. The P300 component of the event-related brain potential as an index of information-processing. Biol. Psychol. 1982, 14, 1–52. [Google Scholar] [CrossRef]
- Nieuwenhuis, S.; Aston-Jones, G.; Cohen, J.D. Decision making, the P3, and the locus coeruleus-norepinephrine system. Psychol. Bull. 2005, 131, 510–532. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.C.; Kuo, W.J.; Hung, D.L.; Tzeng, O.J.L. Action co-representation is tuned to other humans. J. Cognit. Neurosci. 2008, 20, 2015–2024. [Google Scholar] [CrossRef] [PubMed]
- Fazel-Rezai, R.; Allison, B.Z.; Guger, C.; Sellers, E.W.; Kleih, S.C.; Kübler, A. P300 brain computer interface: Current challenges and emerging trends. Front. Neuroeng. 2012, 5, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.Q.; Nam, C.S.; Shadden, B.B.; Johnson, S.L. A P300-based brain-computer interface: Effects of interface type and screen size. Int. J. Hum. Comput. Interact. 2011, 27, 52–68. [Google Scholar] [CrossRef]
- Polich, J.; Kok, A. Cognitive and biological determinants of P300: An integrative review. Biol. Psychol. 1995, 41, 103–146. [Google Scholar] [CrossRef]
- Farwell, L.A.; Donchin, E. Talking off the top of your head: Toward a mental prosthesis utilizing event-related brain potentials. Electroencephalogr. Clin. Neurophysiol. 1988, 70, 510–523. [Google Scholar] [CrossRef]
- Dul, J.; Bruder, R.; Buckle, P.; Carayon, P.; Falzon, P.; Marras, W.S.; Wilson, J.R.; van der Doelen, B. A strategy for human factors/ergonomics: Developing the discipline and profession. Ergonomics 2012, 55, 377–395. [Google Scholar] [CrossRef] [PubMed]
- Nam, C.S. Brain-computer interface (BCI) and ergonomics. Ergonomics 2012, 55, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Nam, C.S.; Li, Y.Q.; Johnson, S. Evaluation of P300-based brain-computer interface in real-world contexts. Int. J. Hum. Comput. Interact. 2010, 26, 621–637. [Google Scholar] [CrossRef]
- Nam, C.S.; Woo, J.; Bahn, S. Severe motor disability affects functional cortical integration in the context of brain-computer interface (BCI) use. Ergonomics 2012, 55, 581–591. [Google Scholar] [CrossRef] [PubMed]
- Blain-Moraes, S.; Schaff, R.; Gruis, K.L.; Huggins, J.E.; Wren, P.A. Barriers to and mediators of brain-computer interface user acceptance: Focus group findings. Ergonomics 2012, 55, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 6. [Google Scholar] [CrossRef]
- Salvaris, M.; Sepulveda, F. Visual modifications on the P300 speller BCI paradigm. J. Neural Eng. 2009, 6, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Townsend, G.; LaPallo, B.K.; Boulay, C.B.; Krusienski, D.J.; Frye, G.E.; Hauser, C.K.; Schwartz, N.E.; Vaughan, T.M.; Wolpaw, J.R.; Sellers, E.W. A novel P300-based brain-computer interface stimulus presentation paradigm: Moving beyond rows and columns. Clin. Neurophysiol. 2010, 121, 1109–1120. [Google Scholar] [CrossRef] [PubMed]
- Acqualagna, L.; Treder, M.S.; Schreuder, M.; Blankertz, B. A novel brain-computer interface based on the rapid serial visual presentation paradigm. In Proceedings of the 32nd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Buenos Aires, Argentina, 31 August–4 September 2010; IEEE: Buenos Aires, Argentina, 2010; pp. 2686–2689. [Google Scholar]
- Aloise, F.; Arico, P.; Schettini, F.; Riccio, A.; Salinari, S.; Mattia, D.; Babiloni, F.; Cincotti, F. A covert attention P300-based brain-computer interface: Geospell. Ergonomics 2012, 55, 538–551. [Google Scholar] [CrossRef] [PubMed]
- Akram, F.; Han, H.S.; Jeon, H.J.; Park, K.; Park, S.H.; Cho, J.; Kim, T.S. An efficient words typing P300-BCI system using a modified T9 interface and random forest classifier. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Osaka, Japan, 3–7 July 2013; IEEE: Osaka, Japan, 2013; pp. 2251–2254. [Google Scholar]
- Pathirage, I.; Khokar, K.; Klay, E.; Alqasemi, R.; Dubey, R. A vision based P300 brain computer interface for grasping using a wheelchair-mounted robotic arm. In Proceedings of the 2013 IEEE/ASME International Conference on Advanced Intelligent Mechatronics, Wollongong, Australia, 9–12 July 2013; IEEE: Wollongong, Australia, 2013; pp. 188–193. [Google Scholar]
- Alcaide-Aguirre, R.E.; Huggins, J.E. Novel hold-release functionality in a P300 brain-computer interface. J. Neural Eng. 2014, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Zhang, Y.; Cichocki, A.; Matsuno, F. A novel EOG/EEG hybrid human-machine interface adopting eye movements and ERPs: Application to robot control. IEEE Trans. Biomed. Eng. 2014, 62, 876–889. [Google Scholar] [CrossRef] [PubMed]
- Klobassa, D.S.; Vaughan, T.M.; Brunner, P.; Schwartz, N.E.; Wolpaw, J.R.; Neuper, C.; Sellers, E.W. Toward a high-throughput auditory P300-based brain-computer interface. Clin. Neurophysiol. 2009, 120, 1252–1261. [Google Scholar] [CrossRef] [PubMed]
- Escolano, C.; Murguialday, A.R.; Matuz, T.; Birbaumer, N.; Minguez, J. A Telepresence robotic system operated with a P300-based brain-computer interface: Initial tests with ALS patients. In Proceedings of the 32nd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Buenos Aires, Argentina, 31 August–4 September 2010; IEEE: Buenos Aires, Argentina, 2010; pp. 4476–4480. [Google Scholar]
- Castermans, T.; Duvinage, M.; Petieau, M.; Hoellinger, T.; de Saedeleer, C.; Seetharaman, K.; Bengoetxea, A.; Cheron, G.; Dutoit, T. Optimizing the performances of a P300-based brain-computer interface in ambulatory conditions. IEEE J. Emerg. Sel. Top. Circuits Syst. 2011, 1, 566–577. [Google Scholar] [CrossRef]
- Duvinage, M.; Castermans, T.; Petieau, M.; Hoellinger, T.; Cheron, G.; Dutoit, T. Performance of the Emotiv Epoc headset for P300-based applications. Biomed. Eng. OnLine 2013, 12. [Google Scholar] [CrossRef] [PubMed]
- Tai, Y.H.; Tian, Y.J.; Huang, T.W.; Sun, K.T. Brainwave technology gives Internet access to the physically disabled. In Fourth Global Congress on Intelligent Systems; IEEE: Hong Kong, China, 2013; pp. 331–335. [Google Scholar]
- Corralejo, R.; Nicolas-Alonso, L.F.; Alvarez, D.; Hornero, R. A P300-based brain-computer interface aimed at operating electronic devices at home for severely disabled people. Med. Biol. Eng. Comput. 2014, 52, 861–872. [Google Scholar] [CrossRef] [PubMed]
- Riccio, A.; Holz, E.M.; Arico, P.; Leotta, F.; Aloise, F.; Desideri, L.; Rimondini, M.; Kubler, A.; Mattia, D.; Cincotti, F. Hybrid P300-based brain-computer interface to improve usability for people with severe motor disability: Electromyographic signals for error correction during a spelling task. Arch. Phys. Med. Rehabil. 2015, 96, S54–S61. [Google Scholar] [CrossRef] [PubMed]
- Lightbody, G.; Ware, M.; McCullagh, P.; Mulvenna, M.D.; Thomson, E.; Martin, S.; Todd, D.; Medina, V.C.; Martinez, S.C. A user centred approach for developing brain-computer interfaces. In Proceedings of the 4th International Conference on Pervasive Computing Technologies for Healthcare, Munich, Germany, 22–25 March 2010; pp. 1–8.
- Riccio, A.; Leotta, F.; Bianchi, L.; Aloise, F.; Zickler, C.; Hoogerwerf, E.J.; Kubler, A.; Mattia, D.; Cincotti, F. Workload measurement in a communication application operated through a P300-based brain-computer interface. J. Neural Eng. 2011, 8, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Holz, E.M.; Höhne, J.; Staiger-Sälzer, P.; Tangermann, M.; Kübler, A. Brain-computer interface controlled gaming: Evaluation of usability by severely motor restricted end-users. Artif. Intell. Med. 2013, 59, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, L.; Lotte, F.; Lecuyer, A. Two brains, one game: Design and evaluation of a multiuser BCI video game based on motor imagery. IEEE Trans. Computat. Intell. AIGames Impact Factor 2013, 5, 185–198. [Google Scholar] [CrossRef]
- Zickler, C.; Halder, S.; Kleih, S.C.; Herbert, C.; Kubler, A. Brain painting: Usability testing according to the user-centered design in end users with severe motor paralysis. Artif. Intell. Med. 2013, 59, 99–110. [Google Scholar] [CrossRef] [PubMed]
- NASA TLX: Task Load Index. Available online: http://humansystems.arc.nasa.gov/groups/tlx/ (accessed on 6 June 2015).
- Gelderblom, G.J.; de Witte, L.P.; Demers, L.; Weiss-Lambrou, R.; Ska, B. The Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0): An overview and recent progress. Technol. Disabil. 2002, 14, 101–105. [Google Scholar]
- Scherer, M.J. The Matching Person & Technology (MPT) Model Manual and Assessments, 5th ed.; The Institute for Matching Person & Technology, Inc.: Webster, NY, USA, 2005. [Google Scholar]
- Norman, D.A.; Draper, S.W. User Centered System Design: New Perspectives on Human–Computer Interaction; CRC Press: Hillsdale, NJ, USA, 1986; p. 540. [Google Scholar]
- International Organization for Standardization. Ergonomics of Human–System Interaction: Human-Centred Design for Interactive Systems; ISO 9241:210; International Organization for Standardization: Geneva, Switzerland, 2010. [Google Scholar]
- Forgas, J.P. Affect and cognition. Perspect. Psychol. Sci. 2008, 3, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Randolph, A.B.; Hubona, G.S. Organizational and individual acceptance of assistive interfaces and technologies. Adv. Manag. Inf. Syst. 2006, 6, 379–400. [Google Scholar]
- Anderson, K.D. Consideration of user priorities when developing neural prosthetics. J. Neural Eng. 2009, 6. [Google Scholar] [CrossRef] [PubMed]
- Huggins, J.E. BCI applications. In Brain-Computer Interfaces: Principles and Practice; Wolpaw, J.R., Wolpaw, E.W., Eds.; Oxford University Press: Oxford, UK; New York, NY, USA, 2012; pp. 197–212. [Google Scholar]
- Hochberg, L.R.; Anderson, K.D. BCI users and their needs. In Brain-Computer Interfaces: Principles and Practice; Wolpaw, J.R., Wolpaw, E.W., Eds.; Oxford University Press: Oxford, UK; New York, NY, USA, 2012; pp. 317–323. [Google Scholar]
- Allison, B. Trends in BCI research: Progress today, backlash tomorrow? XRDS 2011, 18, 18–22. [Google Scholar] [CrossRef]
- Kleih, S.C.; Kaufmann, T.; Zickler, C.; Halder, S.; Leotta, F.; Cincotti, F.; Aloise, F.; Riccio, A.; Herbert, C.; Mattia, D.; et al. Out of the frying pan into the fire—The P300-based BCI faces real-world challenges. In Progress Brain Research, Jens Schouenborg; Garwicz, M., Nils, D., Eds.; Elsevier: Amsterdam, The Netherlands, 2011; Volume 194, pp. 27–46. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Powers, J.C.; Bieliaieva, K.; Wu, S.; Nam, C.S. The Human Factors and Ergonomics of P300-Based Brain-Computer Interfaces. Brain Sci. 2015, 5, 318-356. https://doi.org/10.3390/brainsci5030318
Powers JC, Bieliaieva K, Wu S, Nam CS. The Human Factors and Ergonomics of P300-Based Brain-Computer Interfaces. Brain Sciences. 2015; 5(3):318-356. https://doi.org/10.3390/brainsci5030318
Chicago/Turabian StylePowers, J. Clark, Kateryna Bieliaieva, Shuohao Wu, and Chang S. Nam. 2015. "The Human Factors and Ergonomics of P300-Based Brain-Computer Interfaces" Brain Sciences 5, no. 3: 318-356. https://doi.org/10.3390/brainsci5030318