Finite Element Modeling of an Elderly Person’s Cornea and Rigid Gas Permeable Contact Lenses for Presbyopic Patients


1
National Applied Research Laboratories, Hsin Chu City 300, Taiwan
2
National Synchrotron Radiation Research Center, Hsin Chu City 300, Taiwan
3
New Taipei Eye Clinic, New Taipei City 221, Taiwan
*
Author to whom correspondence should be addressed.
Appl. Sci. 2018, 8(6), 855; https://doi.org/10.3390/app8060855
Submission received: 2 May 2018
/
Revised: 19 May 2018
/
Accepted: 22 May 2018
/
Published: 23 May 2018
(This article belongs to the Special Issue Selected Papers from IEEE ICASI 2018)
Abstract
:Featured Application
Applying on Rigid Gas Permeable Contact Lenses for Presbyopic Patients.
Abstract
Rigid gas permeable (RGP) contact lenses are a common presbyopic correction tool. However, many patients clinically need a long period of adaptation after wearing. This study adopted finite element modeling to analyze the contact stress between RGP contact lens and an elderly person’s cornea. The RGP-lens-produced stress concentration at the corneal edge and maximum pressure on the cornea of elderly subjects aged >64 years was 104.140 kPa, but only 86.889 kPa for the 15–64 group. Therefore, how to decrease the stress concentration on the cornea is important to increasing elderly user comfort while wearing lenses. This study found that when the contact angle is designed on the basis of patient’s actual radian of corneal edge, the contact stress dropped sharply to 60.966 kPa, thus increasing user’s wearing comfort.
1. Introduction
Due to the rapid aging of population and the prolonged daily use of computer, communication, and consumer electronics by people in the 21st century, the number of presbyopic patients is increasing. Moreover, the young population tends to be increasingly affected by presbyopia. Holden [1] accessed estimates from the International Data Base by the United States Census Bureau. According to these estimates, more than 1 billion people in the world are presbyopic; among these people, 571 million are not aware that they are presbyopic or are reluctant to wear presbyopic glasses. By 2020, the global presbyopic population will increase to 1.4 billion. Moreover, by 2050, this number will further increase to 1.8 billion. Taiwan has the highest myopic population in the world. The average age at which people become presbyopic has continued to decline. Moreover, people aged more than 40 years tend to have both myopia and presbyopia. People with myopia and presbyopia have to use two types of glasses—glasses for myopia and reading—to have a clear far and near vision, which causes considerable inconvenience to them.
In addition to glasses, rigid gas permeable (RGP) contact lenses are a common visual acuity correction tool; RGP lenses have a concentric multicircle design. In clinical use, many patients complain that RGP lenses easily slide out of position after wearing and require a long period of adaptation [2]. In addition, a research team from Israel [3] reported that the resolution of these lenses is relatively poor and that the glasses easily display a halo phenomenon when worn. After extensive research, many scholars have found that as an individual’s age increases, the intraocular pressure (IOP) increases [4,5,6,7,8,9,10]. This increase in IOP causes stress and discomfort in the cornea while wearing RGP contact lenses. In this study, we used finite element modeling to analyze the contact stress distribution among the corneas of people in three age groups by using Boston XO2 RGP contact lenses. Moreover, we utilized HFSS® software (ANSYS, Canonsburg, PA, USA) to simulate an appropriate RGP lens contact angle that is suitable for elderly people. In this study, we aim to improve the existing RGP lens design defects by reducing the waiting time for lens modification due to incorrect positioning of the lens after wearing and relaxing or tightening of the lens curvature so that patients with degenerative visual focus are more willing to wear RGP contact lenses.
2. History of the RGP Lens Development
In 1948, Kevin Tuohy, an optician in California, launched the first generation of RGP contact lenses. These plastic lenses made of nonporous plastic material PMMA (poly(methyl methacrylate)) are known as corneal contact lenses because they are smaller in diameter than the previous soft contact lenses and only cover the front portion of a cornea. Subsequent advances in lens manufacturing processes and ophthalmologists’ expertise led to the rapid development of hard plastic contact lenses.
From 1965 to 1991, RGP lenses were emphasized as alternatives to the traditional soft contact lenses with approximately 100% patient usage in 1965 and approximately 40% usage in 1991 [2]. Polycon® lenses were the superior RGP lenses at that time [11]. Irving Fatt, an American chemist, conducted a breakthrough experiment on oxygen and air permeability and invented an oxygen-permeable plastic material. He provided a method for measuring the oxygen transmission rate (Dk) of RGP contact lenses [12]. Subsequently, Nissel et al. developed the second generation of Excel O2, a more hygroscopic and more comfortable gas permeable lens. In 1977, the first RGP lens compression molded from cellulose acetate butyrate was produced in the United Kingdom [13]. The most common RGP lens prescription diameter of 9–9.5 mm was also set during this period. For superior wearing comfort, RGP lenses larger than 9.5 mm in diameter were also used.
A few years later, Dr. Michael Freeman in London developed the first bifocal diffractive RGP lens that differed from the typical bifocal lens designs. This lens, also known as synchronous vision bifocal contact lens, provides hyperopic and myopic images of the central diffraction region on the back of the lens. Because the design of diffractive optics involves two visions for both focuses, an individual’s pupil size and the lighting conditions do not affect imaging performance. Toshida et al. [14] found that bifocal RGP lenses are effective. However, they also suggested that the lenses cannot enable a clear vision for presbyopic people older than 40 years. Moreover, the glare caused by the lenses and the partial bifocal myopia vision still needs improvement.
Synchronous vision bifocal contact lenses are also known as segmented lenses [14]. Bifocal lenses enable clear far and near vision by using the upper and lower portion of the lens, respectively. Therefore, to see a nearby object, it is necessary to move the boresight downward, and the image can be clearly seen at the junction where the upper part meets the lower part. The aspheric design of the RGP lens is an ophthalmic clinical prescription for correcting senile presbyopia, astigmatism [15], and keratoconus in children [11,16].
3. Factors Causing RGP Discomfort
On the topic of contact lens discomfort (CLD), Alipour et al. [17] reviewed 139 articles that had been published between 1982 and 2015 and concluded that CLD can be either caused by the contact lens worn or an environmental factor. The contact-lens-related factors were as follows: (1) material (lubricity and water content), (2) design (edge, base curve, and asphericity), (3) fit, (4) wearing schedule, and (5) maintenance system (chemical composition and regimen). The environmental factors were as follows: (1) aging (age, gender, systemic diseases, and psychiatric and psychological conditions), (2) ocular surface condition, (3) external environment (humidity, wind, and temperature), (4) occupational parameters (computer, light, and altitude), and (5) medications. Efron et al. [18] found a considerable reduction in the overall percentage of contact lens wearers above 55 years old. Moreover, contact lenses with well-rounded anterior edge profiles were found to be significantly more comfortable than lenses with square anterior edge profiles [19]. The rounded edge profile created a smaller impression on the conjunctiva than did the other edge profiles [20]. A high contact stress might be a factor that causes RGP contact lens discomfort when RGP contact lenses are used by elderly people [21].
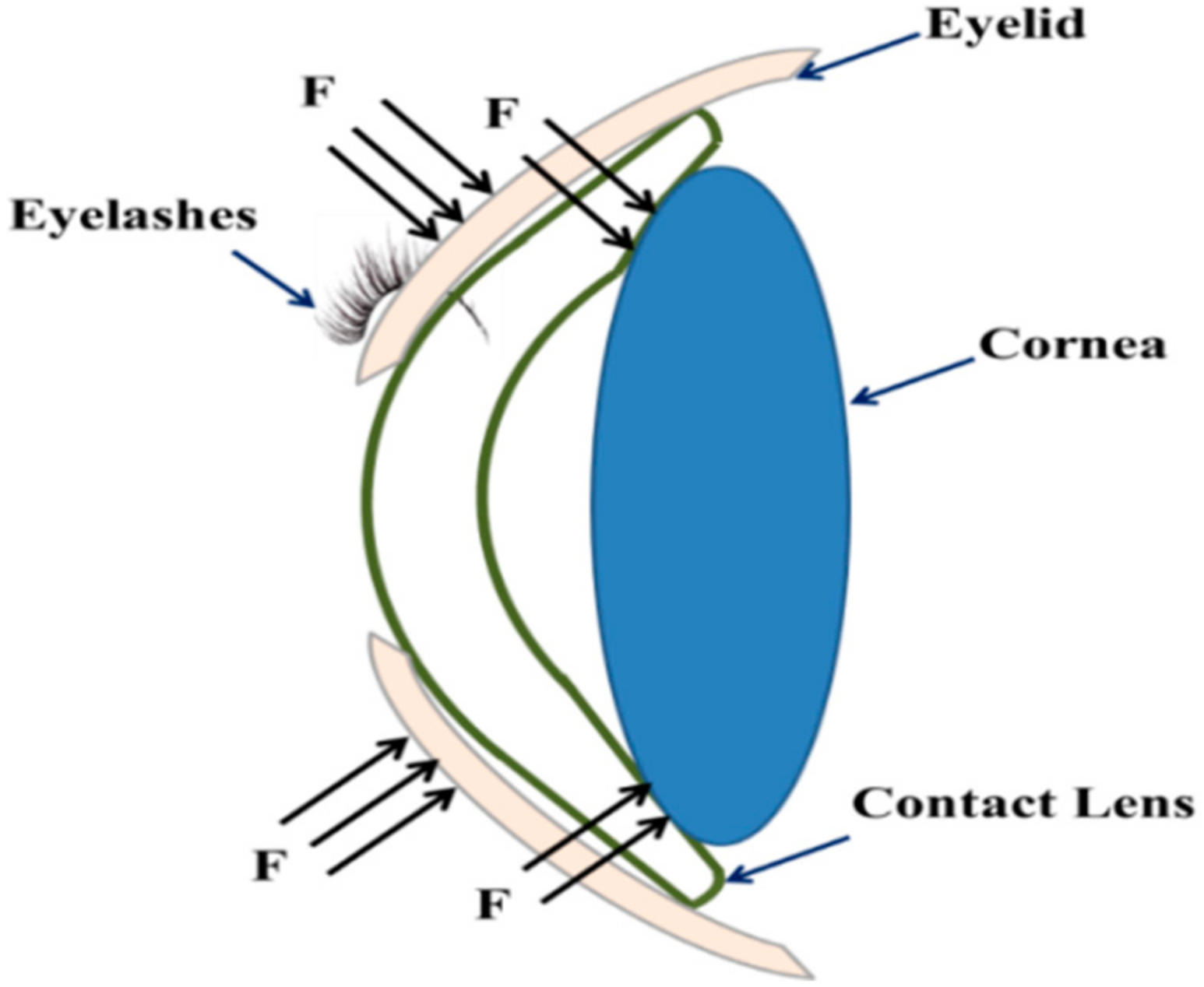
The RGP lens production process is presented in Figure 1. A normal corneal surface is not completely spherical; thus, manufacturers employ three curvatures to form an arc design and allow patients to select the optimal fit (Figure 1). On the basis of the author’s clinical experience in ophthalmology, the contact lens-related and environmental factors that cause RGP discomfort are closely related. In particular, the aging [22] and RGP lens design factors are closely associated. When an individual wears RGP lenses and blinks (Figure 2), the upper and lower eyelids exert pressure on the outer surfaces of the RGP lenses. This pressure forces the RGP lenses to attach to the corneas (Figure 3). Anatomically speaking, the peripheral area of the arc of the RGP lens and cornea come in contact with each other. The area of contact between the peripheral arc of an RGP lens and a cornea affects the pressure distribution on the cornea (Figure 3). Therefore, the shape of the peripheral arc of the RGP lens is a crucial factor that affects lens wearing comfort.
4. Research Method
In this study, the IOP value (Table 1), Young’s modulus, and Poisson’s ratio of the cornea was adopted from a study by Shin et al. [8]. They collected IOP samples from 536 healthy individuals from 2012 to 2016, and confidence interval (CI) for each age group was 95%. Thus, the IOP data for different age groups from the reference paper are reliable. They divided the samples on the basis of three age groups—0–14, 15–64, and more than 64 years. They used Corvis® ST (OCULUS Optikgeräte GmbH, Wetzlar, Germany) to measure the corneal Young’s modulus and then converted the IOP values by using a modified Taber’s model to correct the error that occurred because of direct measurement of the IOP values.
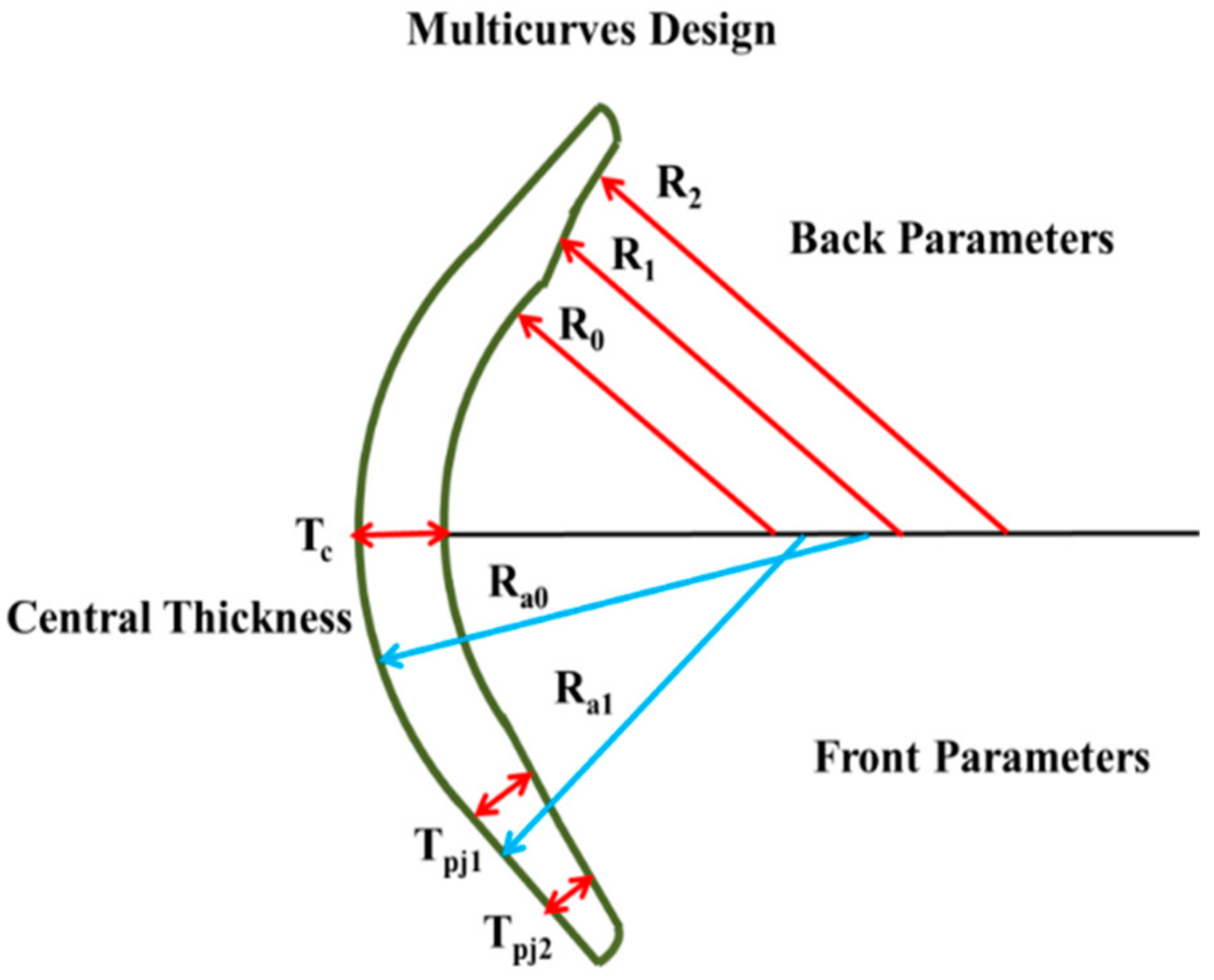
Moreover, Boston XO2 (Bausch & Lomb Incorporated, Rochester, NY, USA) and ANSYS® workbench 15 software were used to simulate the stress distribution between the cornea and RGP lens in the three age groups on the basis of the three edge-of-arc curvatures (R0, R1, and R2) of the lens (Figure 4) and the thickness of the lens center (Te).The FEM simulation flow is shown in Figure 5, the contact lens and corneal model after design, it can load ANSYS software to calculate the corneal stress distribution. The IOP boundary condition is citied from Shin et al. [8], and the RGP lens design is shown in Figure 4.
5. Results
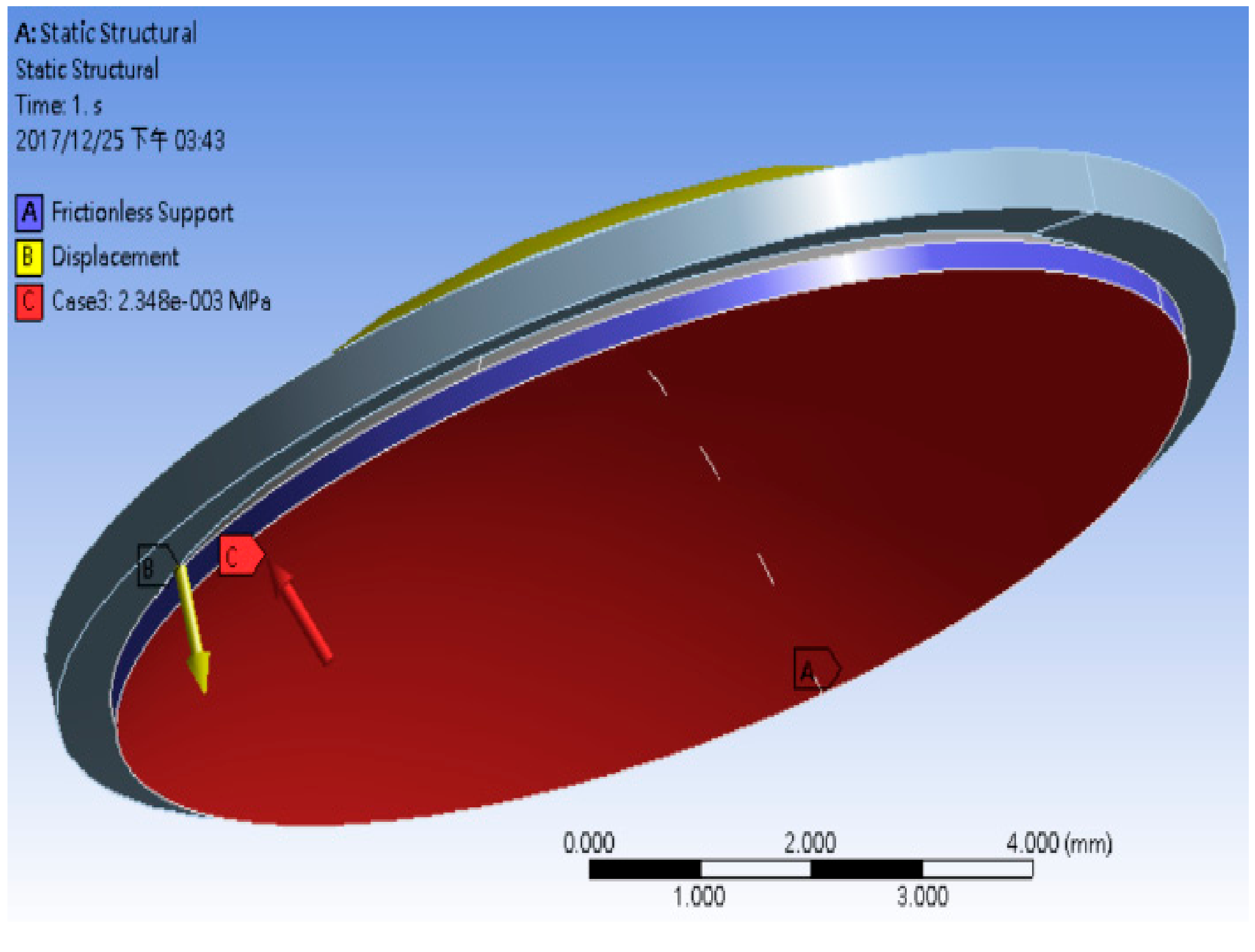
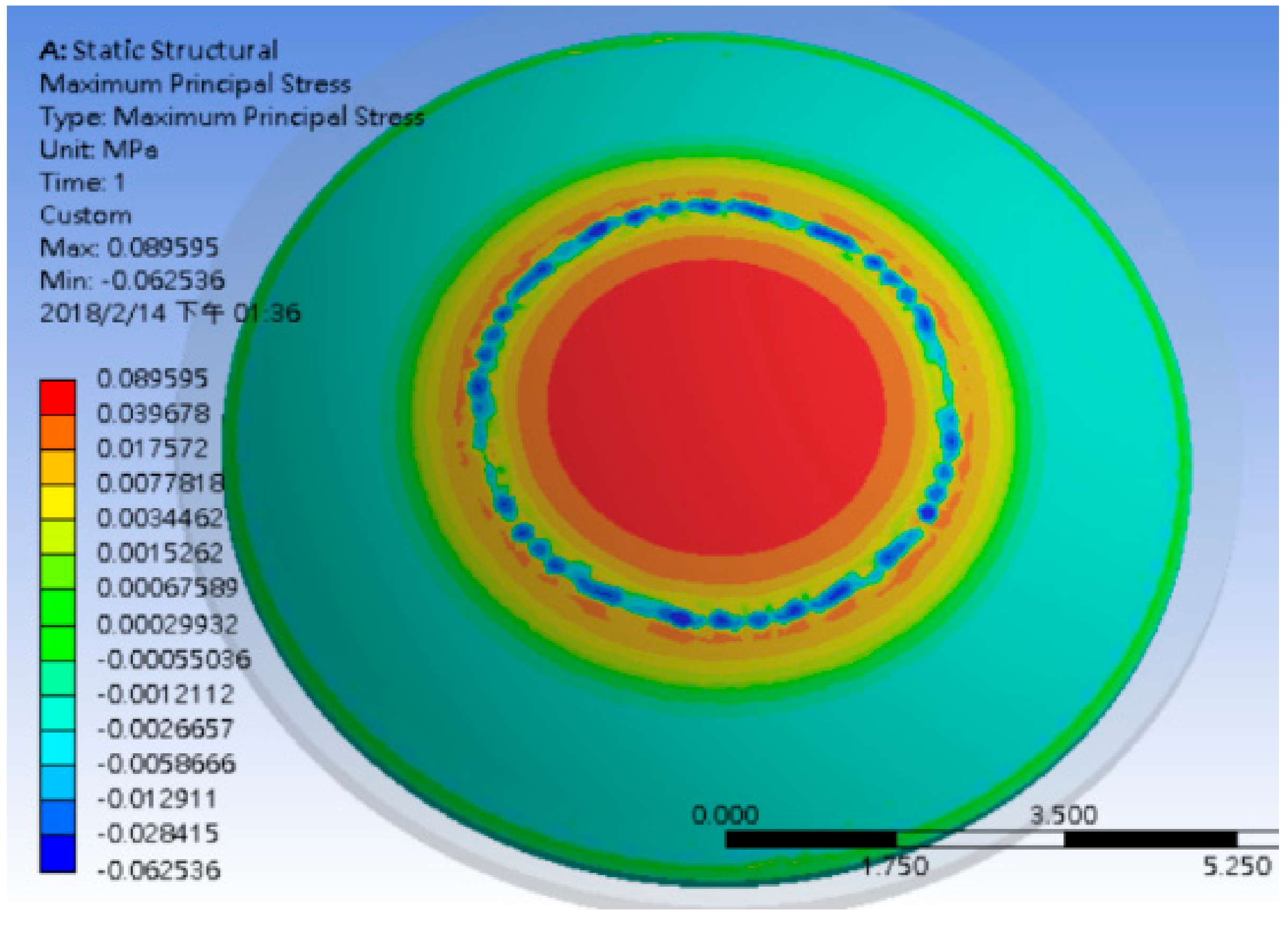
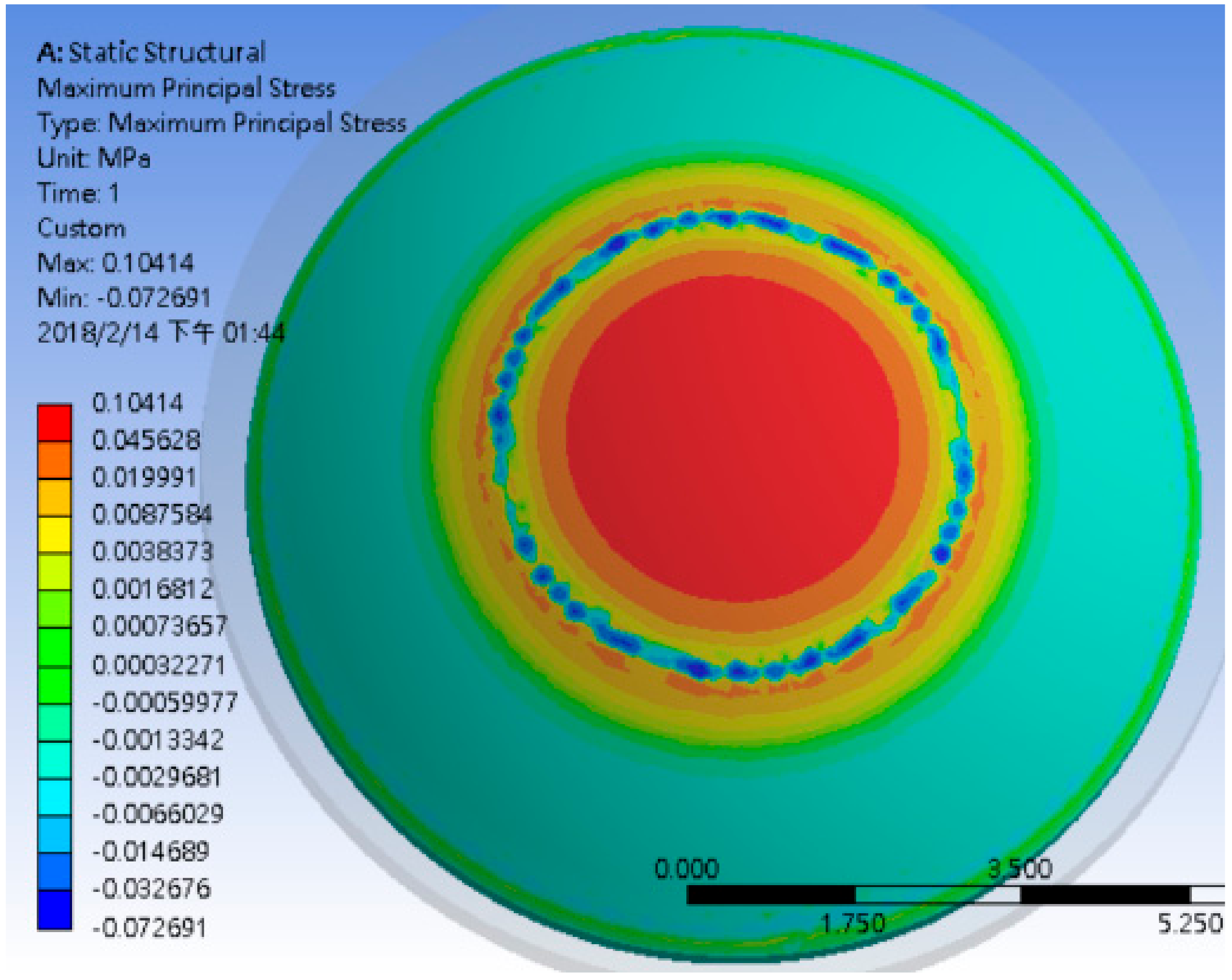
In this study, an ANSYS® finite element model was employed to analyze the stress distribution and stress–strain relationships between the IOP and RGP lens for three age groups. Figure 6 displays a finite element grid diagram of the force direction of the RGP lens on a cornea. However, the structures of the cornea and RGP lens are complex. Therefore, a nonstructural grid is used and the number of grids is increased to enhance the calculation accuracy. Before the finite element calculation, the boundary conditions should be set. The corneal boundary conditions in this study were IOP and frictionless support [9], as shown in Figure 7. After the simulation, we observed that the IOP experienced by different subjects of varying ages differed, although all subjects wore the same material of the RGP lens. These results also confirmed our statement that RGP discomfort might occur due to the relationship between aging and RGP lens design (Figure 8, Figure 9 and Figure 10). This implied that the RGP lens and cornea have varying contact stresses. When the IOP value is higher, the stress value is higher. The stress values for the different age groups are shown in Table 2.
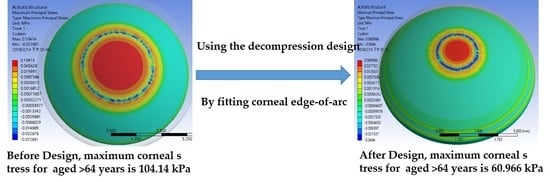
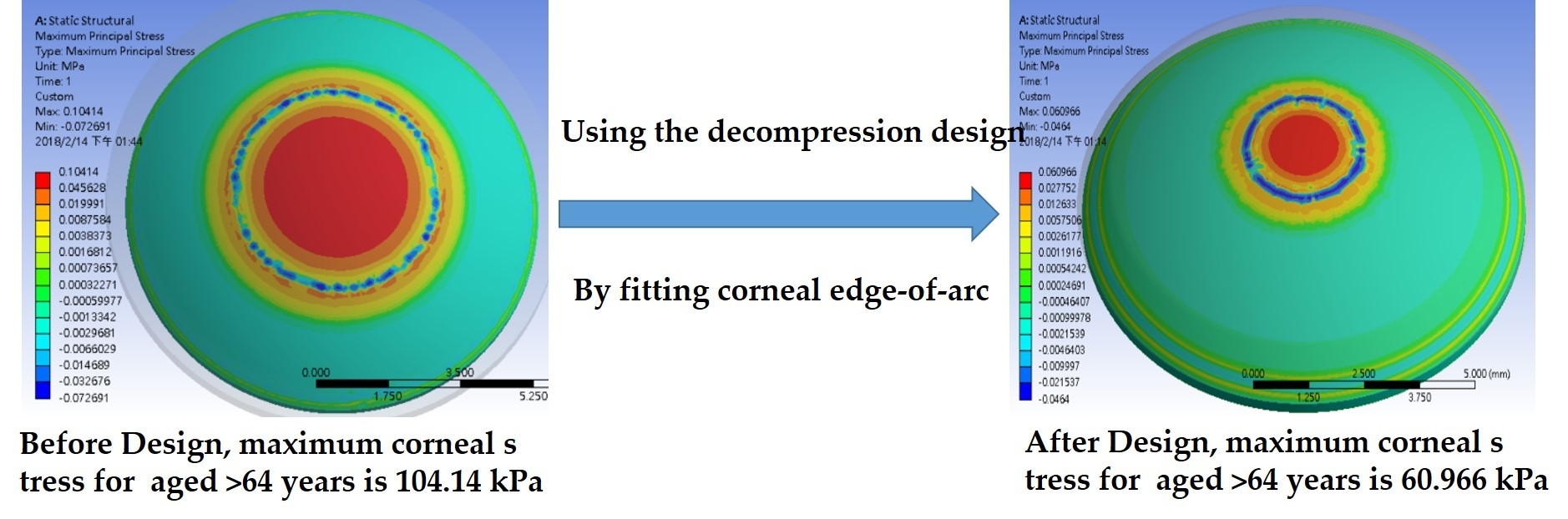
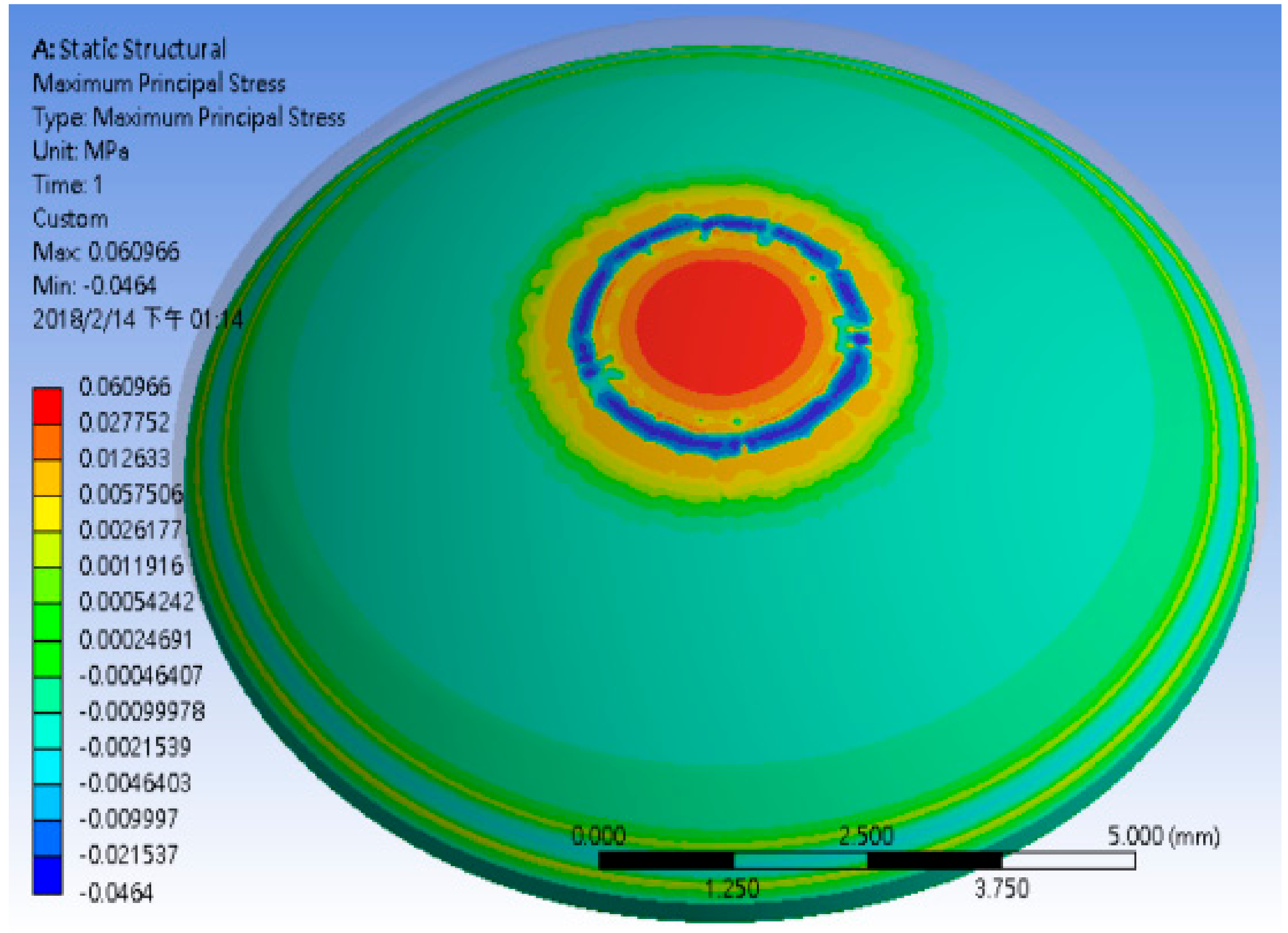
Subsequently, on the basis of the corneal pressure distribution results and average size of >64 group’s corneal edge-of-arc (r = 6.432 mm, RAD = 0.423 mm) [8,9], this study simulated the contact surface of RGP lenses for individuals older than 64 years by using ANSYS HFSS® to improve the contact stress. By comparing Figure 10 and Figure 11, we found that the stress concentration area before using the decompression design was higher than that after using the decompression design. Simultaneously, the maximum pressure declined considerably from 104.140 to 60.966 kPa, which was 58.5% of the original pressure value. The technical comparison table in the 510(k) premarket notification of K171404 by FDA only displays that the accurate wetting angle for Boston XO2 is 38°, which is not specifically designed for the elderly with their IOP and corneal edge-of-arc. Therefore, if the wetting angle of the RGP lens can be designed according to the actual eye structure of the elderly patients, the comfort after wearing can be greatly improved.
6. Conclusions
Due to the aging society and increase in the number of senior citizens, elderly health and care are gradually being taken seriously. When aging, presbyopia is the most common disease in middle-aged people. Wearing presbyopic glasses and RGP contact lenses are the most common treatments used for correcting presbyopia in senior citizens. Although the optical properties of RGP contact lens are good and corrective astigmatism is excellent, the image from the center of the field of view to the edge is clear and consistent. There is no image distortion caused by the divergence of the image refraction or the shrinkage of the image. However, users wearing the lenses encounter the following problems: (1) a longer adaptation period is required and (2) the users experience heaviness and discomfort in their eyes. Finite element modeling demonstrated that the stress concentration at the corneal edge might be the reason for discomfort after wearing RGP contact lenses. This study also found that if the contact angle of the RGP lens is designed on the basis of the actual radius of the patient’s corneal edge, then the wearing comfort for the elderly person is improved. In the future, we intend to work with vendors for developing a corneal-edge-radius measuring equipment. Moreover, we aim to design an RGP lens satisfaction survey by involving a parameter for evaluating the comfort level percentage for senior citizens to analyze the stress force reduction percentage.
Author Contributions
Conceptualization, H.-C.C. and W.-T.H.; Methodology, M.-Y.H.; Software, M.-Y.H.; Validation, P.J.-T.S.; Formal Analysis, M.-Y.H.; Investigation, P.J.-T.S.; Resources, P.J.-T.S.; Data Curation, W.-T.H.; Writing-Original Draft Preparation, H.-C.C.; Writing-Review & Editing, M.-Y.H.; Project Administration, H.-C.C. and W.-T.H.; Funding Acquisition, H.-C.C. and M.-Y.H.
Funding
This research was funded by the Ministry of Science and Technology of Taiwan (grant numbers MOST 106-2221-E-492-021 and MOST 106-2622-E-492-014-CC3).
Conflicts of Interest
The authors declare no conflict of interest. The founding sponsors had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, and in the decision to publish the results.
References
- Holden, B.A.; Fricke, T.R.; Ho, S.M.; Wong, R.; Schlenther, G.; Cronjé, S.; Burnett, A.; Papas, E.; Naidoo, K.S.; Frick, K.D. Global vision impairment due to uncorrected presbyopia. Arch. Ophthalmol. 2008, 126, 1731–1739. [Google Scholar] [CrossRef] [PubMed]
- Efron, N. Obituary—Rigid contact lenses. Contact Lens Anterior Eye 2010, 33, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Yaish, S.B.; Zkitnik, A.; Limon, O.; Yacouel, K.L.; Doron, R.; Zalevsky, Z. Multifocal rigid gas permeable contact lenses with reduced halo. Opt. Commun. 2014, 319, 113–116. [Google Scholar] [CrossRef]
- Carvalho, L.A.; Prado, M.; Cunha, R.H.; Costa Neto, A.; Paranhos, A., Jr.; Schor, P.; Chamon, W. Keratoconus prediction using a finite element model of the cornea with local biomechanical properties. Arq. Bras. Oftalmol. 2009, 72, 139–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kling, S.; Marcos, S. Finite-element modeling of intrastromal ring segment implantation into a hyperelastic cornea. Investig. Ophthalmol. Vis. Sci. 2013, 54, 881–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nejad, T.M.; Foster, C.; Gongal, D. Finite element modelling of cornea mechanics: A review. Arq. Bras. Oftalmol. 2014, 77, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.D.; Ramesh, K.T.; Schein, O. A Computational Model of the Eye for Primary and Secondary Blast Injury; Johns Hopkins University: Baltimore, MD, USA, 2012. [Google Scholar]
- Shin, P.J.; Huang, C.J.; Huang, T.-H.; Lin, H.-C.; Yen, J.-Y.; Wang, I.-J.; Cao, H.-J.; Shih, W.-P.; Dai, C.-A. Estimation of the corneal young’s modulus in vivo based on a fluid-filled spherical-shell model with scheimpflug imaging. J. Ophthalmol. 2017, 2017, 11. [Google Scholar] [CrossRef]
- Thompson, K.A.; Bhardwai, R.; Nguyen, T.D. Development of an Anatomically Accurate Finite Element Human Ocular Globe Model for Blast-Related Fluid-Structure Interaction Studies; US Army Research Laboratory Aberdeen Proving Ground United States: Harford County, MD, USA, 2013. [Google Scholar]
- Whitford, C.; Studer, H.; Boote, C.; Meek, K.M.; Elsheikh, A. Biomechanical model of the human cornea: Considering shear stiffness and regional variation of collagen anisotropy and density. J. Mech. Behav. Biomed. Mater. 2015, 42, 76–87. [Google Scholar] [CrossRef] [PubMed]
- Romero-Jiménez, M.; Santodomingo-Rubido, J.; González-Meijóme, J.M.; Flores-Rodriguez, P.; Villa-Collar, C. Which soft lens power is better for piggyback in keratoconus? Part II. Contact Lens Anterior Eye 2015, 38, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Brennan, N.A.; Efron, N.; Holden, B.A. Oxygen permeability of hard gas permeable contact lens materials. Clin. Exp. Optom. 1986, 69, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, B.A.; Trimber, C.J. Corneal response to extended wear of cab contact lenses in aphakia. Ophthalmology 1980, 87, 292–297. [Google Scholar] [CrossRef]
- Toshida, H.; Takahashi, K.; Sado, K.; Kanai, A.; Murakami, A. Bifocal contact lenses: History, types, characteristics, and actual state and problems. Clin. Ophthalmol. 2008, 2, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Mandathara, P.S.; Fatima, M.; Taureen, S.; Dumpati, S.; Ali, M.H.; Rathi, V. RGP contact lens fitting in keratoconus using fitscan technology. Contact Lens Anterior Eye 2013, 36, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Michaud, L.; Barriault, C.; Dionne, A.; Karwatsky, P. Empirical fitting of soft or rigid gas-permeable contact lenses for the correction of moderate to severe refractive astigmatism: A comparative study. Optometry 2009, 80, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Alipour, F.; Khaheshi, S.; Soleimanzadeh, M.; Heidarzadeh, S.; Heydarzadeh, S. Contact lens-related complications: A review. J. Ophthalmic Vis. Res. 2017, 12, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Efron, N.; Nichols, J.J.; Woods, C.A.; Morgan, P.B. Trends in us contact lens prescribing 2002 to 2014. Optom. Vis. Sci. 2015, 92, 758–767. [Google Scholar] [CrossRef] [PubMed]
- Hood, D. Edge shape and comfort of rigid lenses. Am. J. Optom. Physiol. Opt. 1988, 65, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Wolffsohn, J.S.; Drew, T.; Dhallu, S.; Sheppard, A.; Hofmann, G.J.; Prince, M. Impact of soft contact lens edge design and midperipheral lens shape on the epithelium and its indentation with lens mobility. Investig. Ophthalmol. Vis. Sci. 2013, 54, 6190–6197. [Google Scholar] [CrossRef] [PubMed]
- Wöhlk. Edge Profiles of Hydrogel Contact Lenses and Their Effect on Fitting and Wearing Characteristics. Wöhlk Contactlisen: Schönkirchen, Germany. 2010. Available online: http://www.vargellini.it/zaccagnini/download/approfondimenti/contattologia/woehlk-wissen%20edge%20profiles,%20effect&fitting.pdf (accessed on 15 January 2017).
- Chalmers, R.L.; Hunt, C.; Hickson-Curran, S.; Young, G. Struggle with hydrogel cl wear increases with age in young adults. Contact Lens Anterior Eye 2009, 32, 2009. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Production process of an RGP lens. Source: Antasee Inc.

Figure 2.
Force direction of RGP lens on cornea. Source: Antasee Inc.

Figure 3.
Force direction (F) of RGP lens on cornea.

Figure 4.
Optical design parameters of the RGP lens.

Figure 5.
The FEM simulation flowchart.

Figure 6.
Finite element grid model.

Figure 7.
Boundary conditions for the finite elements, the IOP is 2.34 kPa.

Figure 8.
Maximum corneal stress for 0–14 years.

Figure 9.
Maximum corneal stress for 15–64 years.

Figure 10.
Maximum corneal stress for aged >64 years.

Figure 11.
Decreasing contract stress by fitting corneal edge-of-arc (>64 years).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Intraocular pressure for all age groups [8].
Table 1.
Intraocular pressure for all age groups [8].
| Age Group | 0–14 | 15–64 | >64 |
|---|---|---|---|
| IOP (mmHg) | 15.19 | 14.73 | 17.66 |
Table 2.
Corneal stress value for all age groups.
| Age Group | 0–14 | 15–64 | >64 |
|---|---|---|---|
| Stress (kPa) | 89.595 | 86.889 | 104.140 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chang, H.-C.; Hsu, M.-Y.; Hsiao, W.-T.; Shum, P.J.-T. Finite Element Modeling of an Elderly Person’s Cornea and Rigid Gas Permeable Contact Lenses for Presbyopic Patients. Appl. Sci. 2018, 8, 855. https://doi.org/10.3390/app8060855
AMA Style
Chang H-C, Hsu M-Y, Hsiao W-T, Shum PJ-T. Finite Element Modeling of an Elderly Person’s Cornea and Rigid Gas Permeable Contact Lenses for Presbyopic Patients. Applied Sciences. 2018; 8(6):855. https://doi.org/10.3390/app8060855
Chicago/Turabian StyleChang, Han-Chao, Ming-Ying Hsu, Wen-Tse Hsiao, and Patrick Joi-Tsang Shum. 2018. "Finite Element Modeling of an Elderly Person’s Cornea and Rigid Gas Permeable Contact Lenses for Presbyopic Patients" Applied Sciences 8, no. 6: 855. https://doi.org/10.3390/app8060855
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.