Estimating Co-Contraction Activation of Trunk Muscles Using a Novel Musculoskeletal Model for Pregnant Women


1
School of Science for Open and Environmental Systems, Graduate School of Science and Technology, Keio University, 3-14-1 Hiyoshi, Kohoku-ku, Yokohama 223-8522, Japan
2
Department of System Design Engineering, Faculty of Science and Technology, Keio University, 3-14-1 Hiyoshi, Kohoku-ku, Yokohama 223-8522, Japan
*
Author to whom correspondence should be addressed.
Appl. Sci. 2017, 7(10), 1067; https://doi.org/10.3390/app7101067
Submission received: 8 September 2017
/
Revised: 11 October 2017
/
Accepted: 12 October 2017
/
Published: 15 October 2017
(This article belongs to the Section Mechanical Engineering)
Abstract
:Weight gain and stretched abdominal muscles from an enlarged gravid uterus are remarkable features during pregnancy. These changes elicit postural instability and place strain on body segments, contributing to lower back pain. In general, the agonist and antagonist muscles act simultaneously to increase joint stabilization; however, this can cause additional muscle stress during movement. Furthermore, this activation can be observed in pregnant women because of their unstable body joints. Hence, physical modalities based on assessments of muscle activation are useful for managing low back pain during pregnancy. Musculoskeletal models are common when investigating muscle load. However, it is difficult to apply such models to pregnant women and estimate the co-contraction of muscles using musculoskeletal models. Therefore, the purpose of this study is to construct a musculoskeletal model for pregnant women that estimates the co-contraction of trunk muscles. First, motion analysis was conducted on a pregnant woman and the muscle activations of the rectus abdominis and erector spinae were measured. Then, the musculoskeletal model was specifically modified for pregnant women. Finally, the co-contraction was estimated from the results of the musculoskeletal model and electromyography data using a genetic algorithm. With the proposed methods, weakened abdominal muscle torque and the co-contraction activation of trunk muscles were estimated successfully.
1. Introduction
Women experience specific anatomic physiologic and hormonal changes during pregnancy especially on the musculoskeletal system of the axial skeleton [1]. For example, there is weight gain in the abdomen and a shift in the center of gravity as fetal growth occurs. In addition, it is thought that an enlarged gravid uterus stretches and weakens abdominal muscles [2]. These physical and musculoskeletal changes elicit postural and movement changes and place strain on various body segments and muscles, which subsequently contribute to musculoskeletal pain, especially lower back and pelvic girdle pain during pregnancy [3,4]. Pain around the lower back and pelvis is collectively called lumbopelvic pain (LPP), and it is a common symptom during pregnancy that lowers the quality of life in many women during and after pregnancy [5,6]. LPP is thought to be strongly related to physical stress from daily basic activities, such as walking [7], and in particular, from some motions that includes flex rotations of the trunk, such as sitting, standing and bending [8,9]. Thus, physical modalities are needed to treat these musculoskeletal disorders of pregnancy, with proper exercise techniques and movement coaching, to maintain abdominal muscle function [10].
In general, the agonist and antagonist muscles of some body segment act simultaneously during human motion. For example, the rectus abdominis usually acts as an antagonist muscle to the erector spinae that acts as an agonist muscle during trunk expansion. Simultaneous contraction is called co-contraction, and is thought to be a mechanism to improve movement efficiency and increase joint stabilization [11,12]. For example, the erector spinae stretches the trunk, and at the same time, the rectus abdominis acts to increase the mechanical stiffness of the joint in the trunk segment [13]. It can be believed that the activation of these muscles is easily observed in pregnant women because of their unstable body balance. Meanwhile, one of the main risk factors of LPP is fatigue in the back muscles such as the erector spinae [4]. The activation of the rectus abdominis could increase the burden on the erector spinae as well as exacerbating mechanical stiffness. Hence, physical modalities based on assessments by both motion analysis and observations of muscle activation increase the effectiveness of remedial therapy.
Musculoskeletal models have been recently used as an effective tool for visualizing human movement, investigating muscle load, and analyzing the functional capacity of muscles. In musculoskeletal modeling simulators, skeleton and muscle models use averaged values from a human body database. By inputting motion and force data to the models, the joint torque of body segments can be calculated from inverse dynamics. The joint torque is the same value as the sum of the collective torque from muscles that act on joint motion. This assumes that all external force that is applied to the human body is inputted to the model. In addition to these procedures, muscle torque is estimated through an optimization scheme to decide the distribution ratio of joint torque to muscle torque for the joint. These models have been applied to various fields, such as sports, ergonomics, and physical modalities [14,15,16]. However, very few studies have been conducted on the construction of a musculoskeletal model of pregnant woman [17]. Moreover, it is difficult to estimate the co-contraction of agonist and antagonist muscles using a musculoskeletal model. This is because an optimization scheme for the approximate minimization of muscle stress is typically used to estimate muscle activation patterns in musculoskeletal models [18]. Antagonist muscle activation increases the metabolic cost and is not selected by such schemes. Although electromyography (EMG) is a method to measure actual muscle activation, it detects the electric potential generated by muscle cells, rather than muscle force. On the other hand, an approach to estimate muscle force based on the signal patterns of EMG was suggested [19,20]. However, measuring EMG during maximum voluntary contraction (MVC) tasks is required to use this method. In other words, this method is not suited for people who cannot perform MVC tasks, such as pregnant women. To address these issues, Oyong et al. proposed a method for estimating muscle torque and joint torque from EMG using a genetic algorithm (GA) for stroke affected patients who have difficulty in performing MVC tasks [21]. However, their method was not exclusive to stroke patients, but rather designed for anyone unable to perform MVC tasks.
This study proposes a musculoskeletal model for pregnant women in late pregnancy because they tend to experience remarkable physical changes and LPP at that time. First, sit-to-stand motion analysis was conducted on a pregnant woman using an inertial measurement unit (IMU) and surface EMG. Then, a musculoskeletal model was specifically modified to meet the size and mass of the body segments of pregnant women and their stretched abdominal muscle. Finally, the co-contraction of the rectus abdominis and erector spinae was estimated from the joint torque calculated in a musculoskeletal model of pregnant woman and EMG data using the GA.
2. Materials and Methods
Motion analysis experiments on a pregnant woman were performed while she sat down on a chair and stood up, in order to obtain the data for a musculoskeletal model. These motions were selected because they are easy to perform and related to LPP during pregnancy. Then, a musculoskeletal model specifically fitted to a pregnant woman was developed and muscle activation was estimated using a GA. The study was carried out in accordance with the guidelines of the Declaration of Helsinki, and the study protocol was reviewed and approved by the Ethics Committee of the Kishokai Medical Corporation (approval number 2015_002).
2.1. Participant
A pregnant woman was recruited and agreed to participate in the study. The participant was 36 weeks into her singleton pregnancy. She did not have serious orthopedic disorders or neurological diseases, and her pregnancy was not considered high-risk. Before the motion analysis, it was determined that she did not have external injuries that could affect the motion analysis. In addition, information pertaining to her body mass at the time of the experiment and gained body mass during pregnancy was collected from a questionnaire to construct the musculoskeletal model. This physical data is shown in Table 1.
2.2. Sitting Down and Standing Up Experiment
2.2.1. Motion Analysis
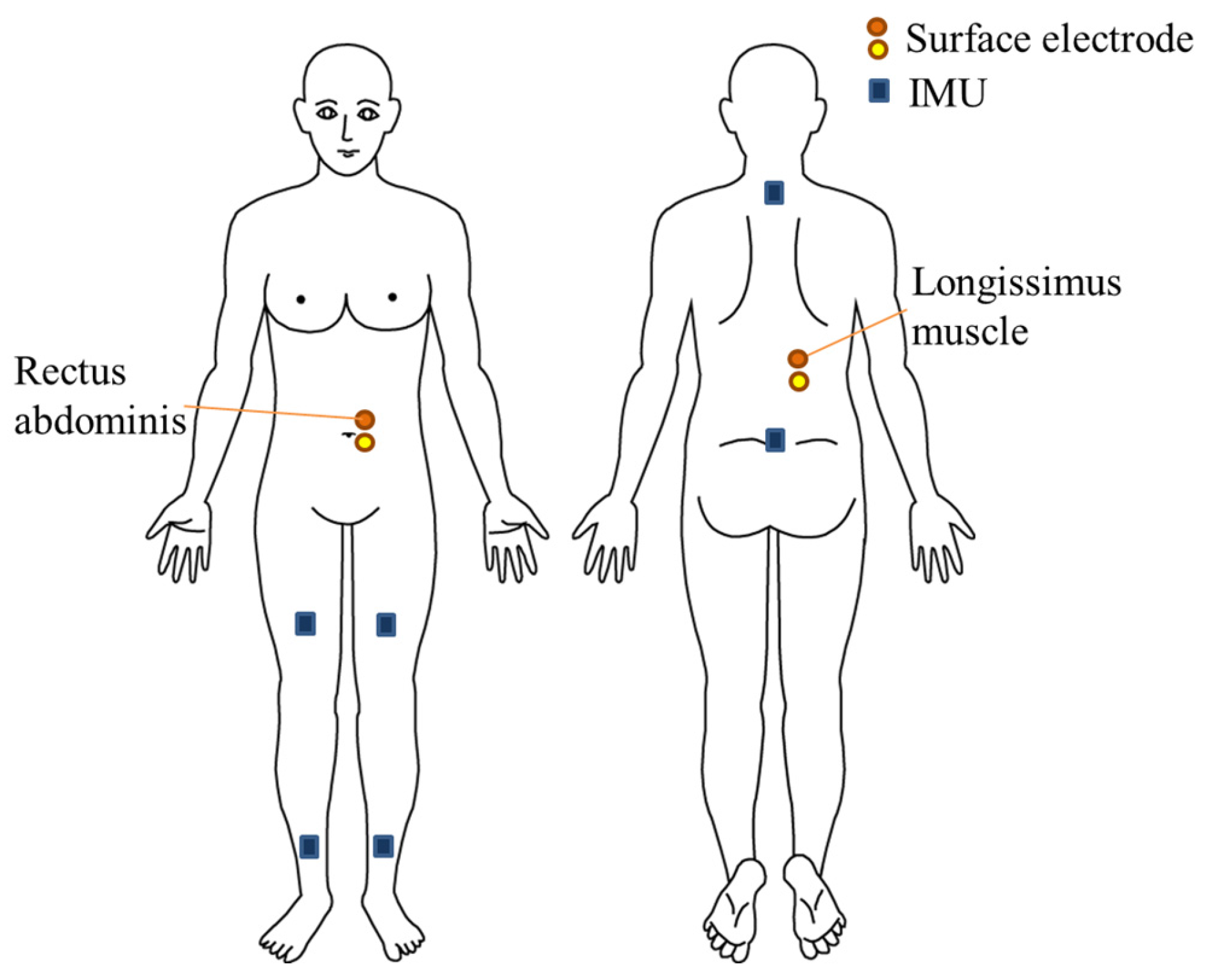
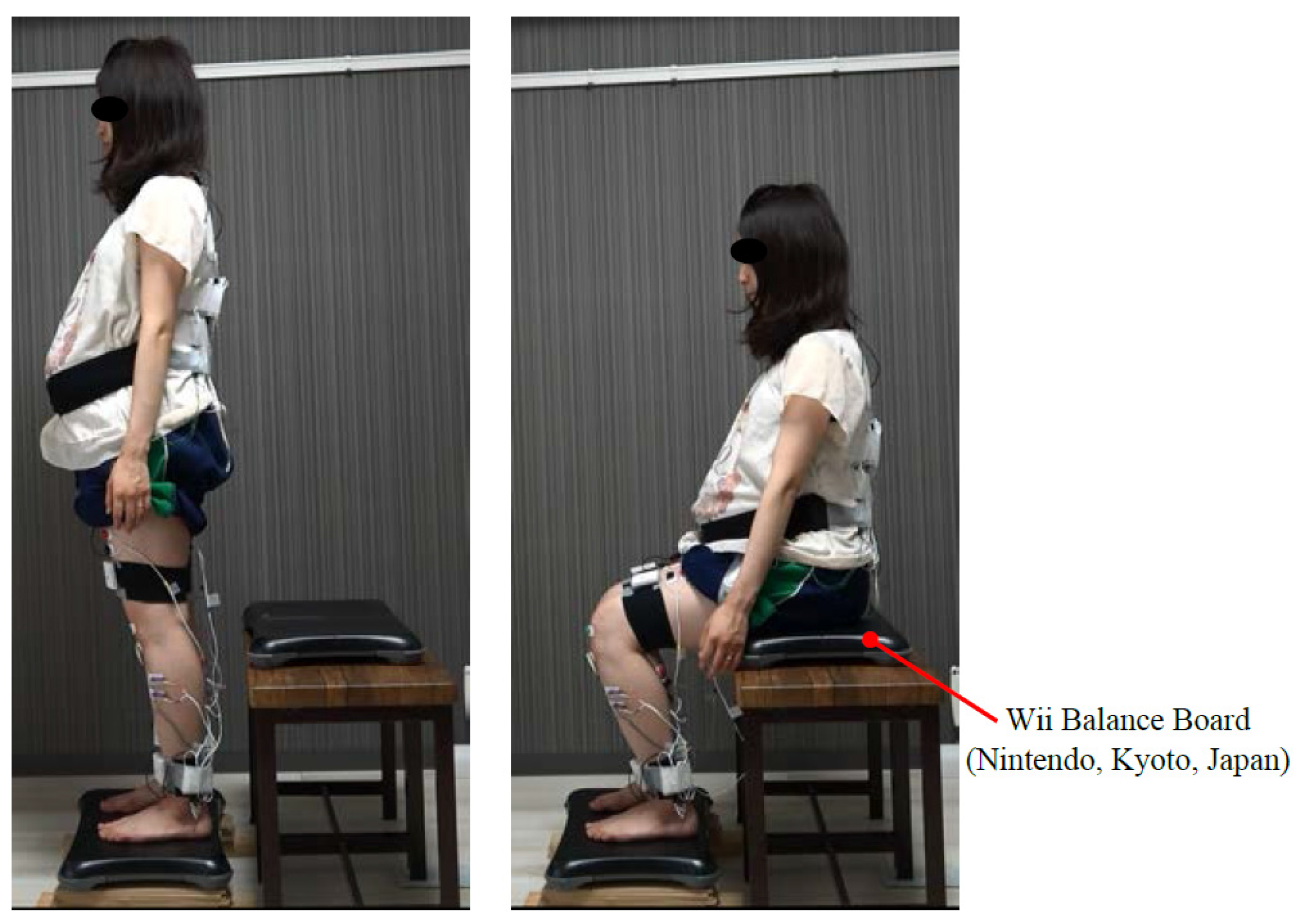
During the motion analysis of sitting down and standing up, IMUs were used to analyze the motion for the sake of clinical practice in the future. IMUs will not disturb a person’s motion or restrict the measurement environment because they are small and lightweight devices, suitable for use in clinical practice. As shown in Figure 1 and Figure 2, the participant was evaluated using six IMUs incorporating tri-axis accelerometers, gyroscopes, and magnetometers (TSND151, ATR-Promotions Co., Ltd., Kyoto, Japan). The six IMUs were attached to a fixed belt at the level of the C7 spinous process, L4 spinous process, bilateral position 10 cm above the patella, and bilateral position 10 cm above the lateral malleolus, to measure the motion of upper trunk, lower trunk (pelvis), thigh segment, and bilateral shank, respectively. Some motion, such as vibration and the rotation of each segment could be analyzed by acquiring data from the attached IMUs. The signals were sampled at a frequency of 100 Hz. Meanwhile, Nintendo’s Wii Balance Board (WBB; Nintendo, Kyoto, Japan) was used to measure vertical reaction forces. The measurement accuracy of the WBB is ± 7.84 N (0.8 kg) from 0 to 68 kg and ± 11.76 N (1.2 kg) from 68 to 100 kg. Two WBBs were placed under the participant’s feet and on the chair to measure the vertical ground reaction force and the vertical reaction force from the chair, respectively.
Figure 3 shows an overview of the measurement settings. The participant started from a standing position in front of the chair and then sat down and stood up. Sitting down and standing up were conducted eight times. A rest period of approximately 5 s was arranged between each time. An armless, backless chair was adjusted to the height of the subject’s knee (determined as the distance from the lateral knee joint line to the floor). The sit-to-stand (STS) movement was performed barefoot, and the distance between each foot was 10 cm, in accordance with previous research [22]. The participation moved at a self-selected velocity, comfortably, and performed the STS movement eight times without using her hands.
2.2.2. Electromyography
Surface electromyography (EMG) (SE-C-AMP-H100, ATR-Promotions Co., Ltd., Kyoto, Japan) can be used with IMUs (TSND151) by connecting a cable to measure the muscular activation of the abdominal and back muscles during STS movements. EMG electrodes were placed on the right and left rectus abdominis and longissimus—part of the erector spinae—as shown in Figure 2. The position was decided in accordance with previous research and SENIAM guidelines [23]. Prior to placing the electrodes, the skin at the electrode sites was shaved, cleaned with alcohol, and prepared using fine sandpaper. For optimal collection of the EMG signals, the electrodes were placed parallel to the muscle fiber orientation. EMG signals from each muscle were sampled at 1000 Hz. The acquired raw EMG signals were processed with a 50 Hz notch filter to reduce the noise associated with electrical interference. Then, the signal was full-wave rectified and filtered using a band-pass filter at 20–500 Hz.
2.3. Proposal of Musculoskeletal Models for Pregnant Women
A full-body musculoskeletal model of a pregnant woman was constructed using Biomechanics of Bodies (BoB: Marlbrook Ltd., Bromsgrove, UK). BoB consists of 36 skeletal segments and 666 locomotor muscle units. BoB’s biomechanical software is based in the MATLAB environment (The MathWorks Co., Release 2016, Tokyo, Japan) and thus inherits much of the analysis capabilities of MATLAB. It is capable of performing inverse dynamics analysis and uses optimization methods to solve for muscle torque distributions. BoB enables us to calculate the torque at the joints corresponding to the observed motion, the external force by inverse dynamics, and the muscle torque using an optimization approach [24,25]. Skeletal information (e.g., the size and mass of each body segment) and muscular information (e.g., the origin, wrapping, and insertion point of the muscle) can be modified with BoB. By using this function, the following procedures were conducted to develop a model for pregnant women.
2.3.1. Changing the Skeletal Model
First, the size and mass of each segment was modified. In BoB, these values are derived by using a database based on data for men. Thus, these values needed to be changed to render them compatible with data regarding Japanese women. The size of each segment was expressed as the fractional size of the segment relative to the total body height in BoB. This information was altered by referencing averaged data on Japanese women (between 20 and 40 years old) [26]. Similarly, the mass of each segment was expressed as the fractional mass of the segment of the total body mass. Instead of this value, statistical information pertaining to Japanese women (between 19 and 35 years old) was used [27]. When choosing these values, the range of age was as consistent as possible with the age of pregnant women in Japan.
2.3.2. Changing the Muscular Model
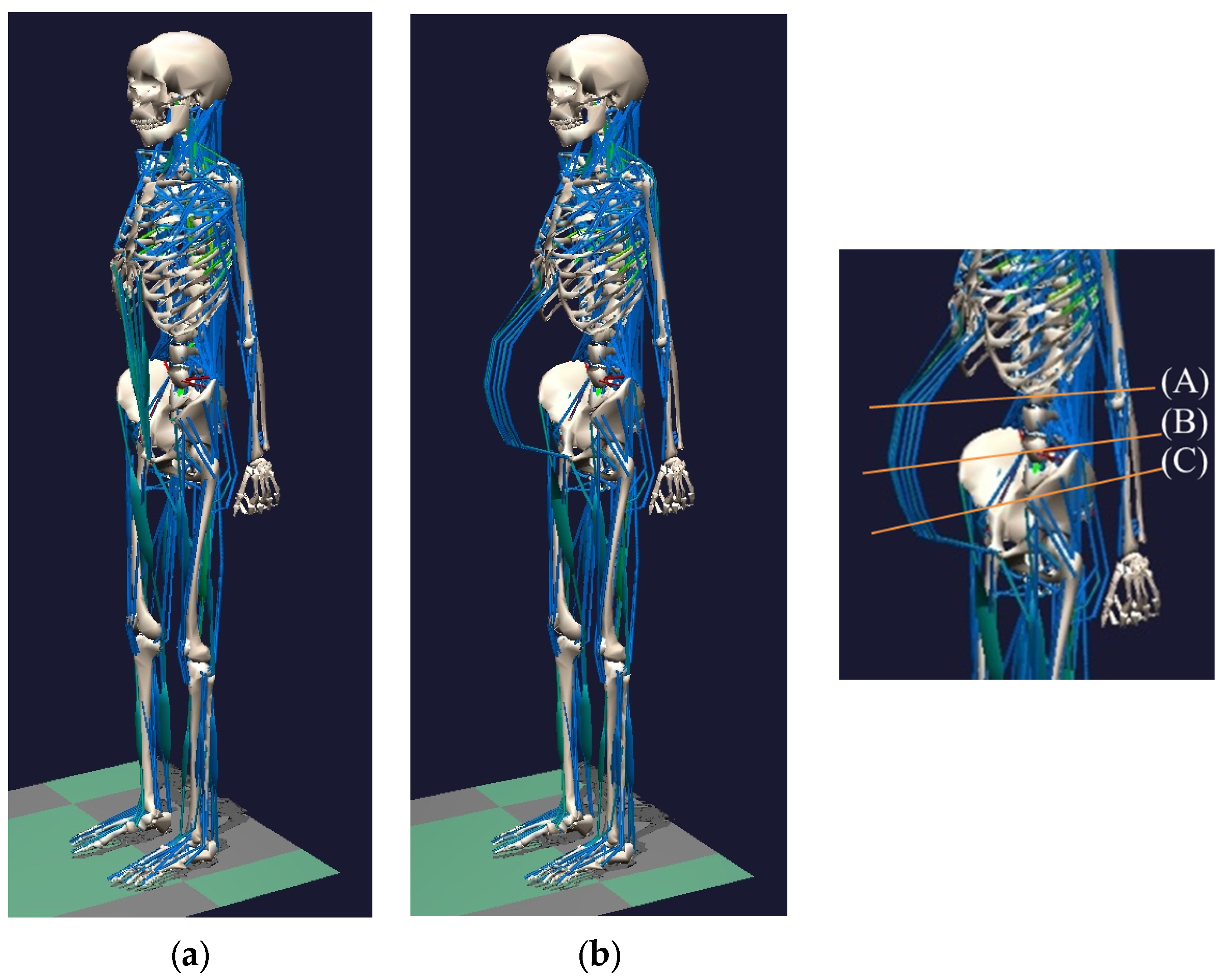
During pregnancy, the abdominal muscles are stretched and weakened by an enlarged gravid uterus. This is a remarkable change to the musculoskeletal system that occurs during pregnancy, and thus it must be considered for a musculoskeletal model peculiar to pregnant women. In previous studies, basic information with respect to the waist girth and depth of a pregnant woman was collected to design maternity wear for the later stages of pregnancy. For purpose of this, body measurements and accurate silhouette photographing were conducted every two weeks from 26 weeks to 38 weeks of pregnancy, the measured values of change to the waist of pregnant women were generalized to be correct within a certain margin of error, for all women, including Japanese women [28]. Such information was used in the present study to determine the wrapping point of the rectus abdominis. The wrapping point of a muscle can be derived as the length from a joint, such as the spinal process in BoB. Thus, we used the body length information at the spinal level with respect to the girth and depth data from the previous study. Specifically, the waist girth of the participant was measured and the depth was calculated by using the measured depth and girth at 36 weeks of pregnancy from the previous study. For example, waist girth and depth are at approximately the point of the L2 spinous process, and the values at this point (L2) increased to 0.865 m and to 0.266 m ahead of the joint (L2) for a woman who was 36 weeks pregnant [29]. In the present study, these values were used to decide the wrapping point of the rectus abdominis. When the abdominal girth with respect to the point is measured—at 0.840 m in this study—the length can be derived by reference to the ratio of depth to girth. The values used in the calculation are listed in Table 2. The girth can be measured by using a measuring tape, and this is standardly used in clinical practice. Figure 4 shows the appearance of the model for an average woman and a pregnant woman.
2.3.3. Supplementing Body Weight during Pregnancy
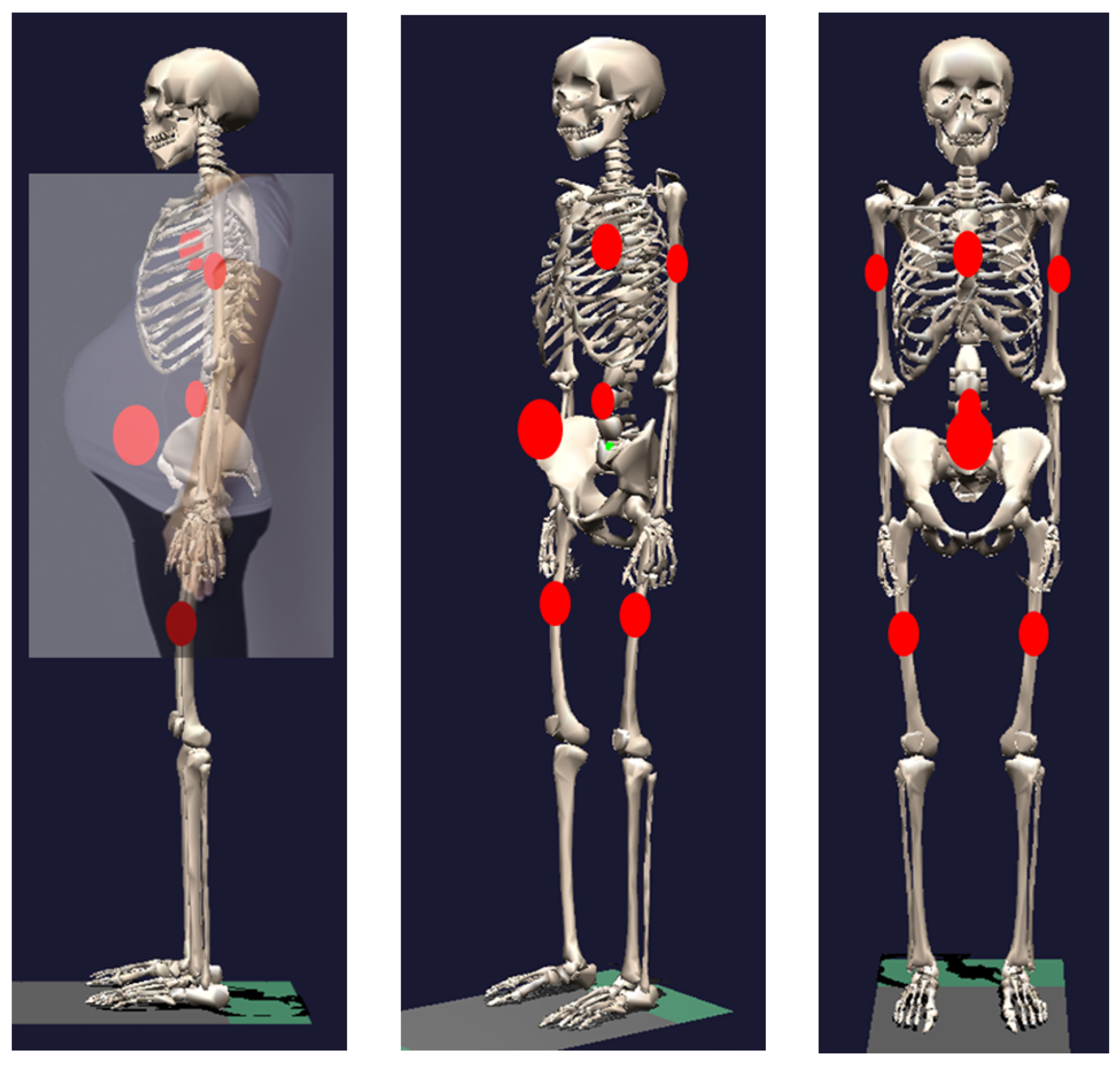
The other characteristic change during pregnancy is weight gain. This change was determined following two previous research works regarding the musculoskeletal models of pregnant woman and inertial parameters of the lower trunk of pregnant women [17,29]. This research pertained to musculoskeletal models of pregnant woman during the last trimester. Nakashima et al. added 0.95 kg to the breasts, 3.325 kg to the segments of the abdomen, arms, and legs, and 6.175 kg to the abdominal area around the uterus, for a total gain of 10.45 kg during pregnancy. A proportionate amount of weight was thus added to each segment of the participant in the current study. For example, based on the participant’s own weight gain, 0.818 kg was added to the breasts, 2.864 kg to the segments of the abdomen, arms and legs, and 5.318 kg to the abdominal area around the uterus of the participant, who had gained 9.0 kg during pregnancy. In particular, the addition of mass in the abdominal area around the uterus required meticulous care because it is strongly related to a shift in the center of gravity. However, it is extremely difficult to measure the center of the uterus mass gained in pregnancy. Hence, the addition of mass to this area was decided putatively, by reference to previous research on the inertial parameters of the lower trunks of pregnant women [29]. Thus, the location of the center of mass of the lower trunk segment was estimated at 10.5 cm below the lower edge of the tenth rib and 15.35 cm forward from the posterior end of the lower trunk segment. In this way, mass was added to specific points of the musculoskeletal model. Figure 5 shows each point of additional mass in the model for pregnant women. The red circles indicate the points where mass was added.
2.4. Measured Data Processing
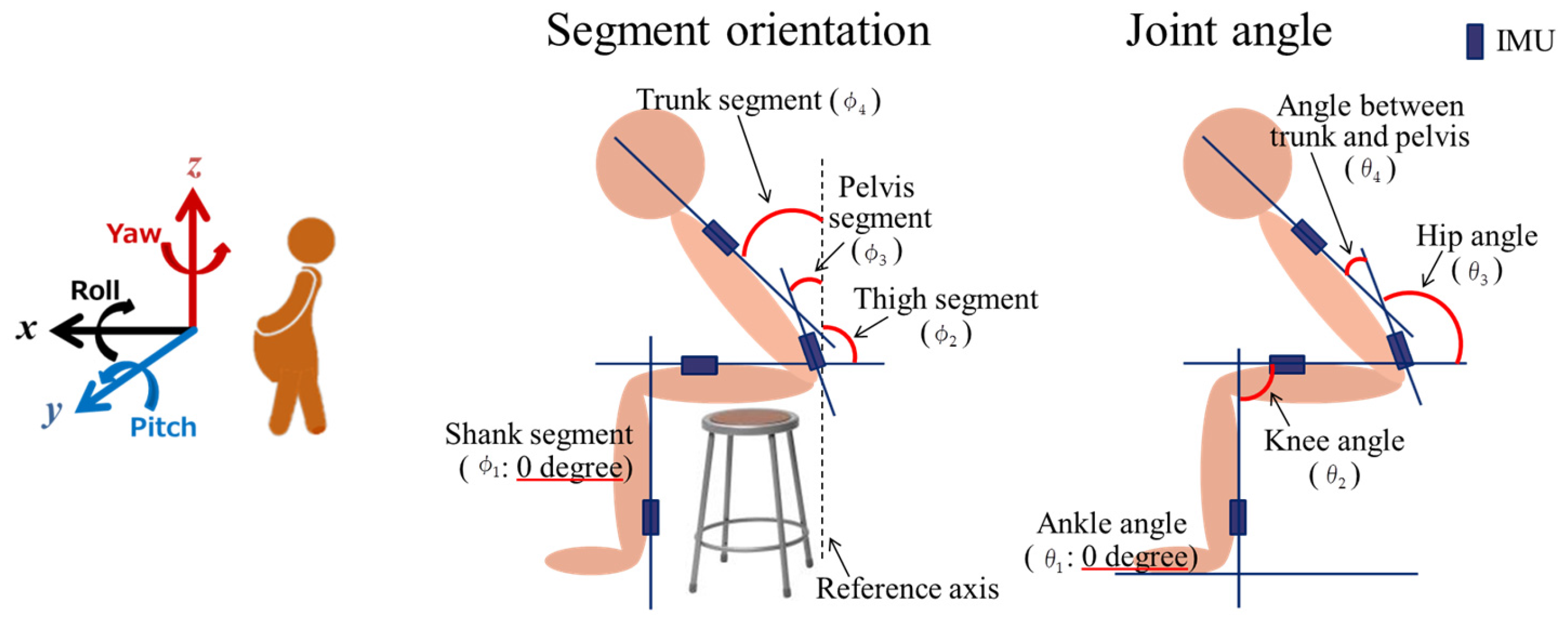
Signal processing was performed for the STS experiment using data from each IMU attached to the body segments and MATLAB (The MathWorks Co., Release 2016, Tokyo, Japan). The Madgwick algorithm is a method for accurate estimations of IMU orientations, and this method was used to obtain information regarding body segment orientation and joint angles. The algorithm calculates the attitude angle based on a fusion of measurements from an accelerometer, gyroscope, and magnetometer [30]. Figure 6 shows the coordinate system and the segment orientations and joint angles calculated in this study. The direction of the axis of the IMU, which was attached such that it matched the line along with the bone as closely as possible, was determined as the line of each segment. Pitch data was used to calculate the inclination angle for the flexion/extension of each body segment at the point of the attached IMUs: the joint angle of the ankle, knee, hip, and between the trunk and pelvis at the point between two IMUs. To calculate the inclination angle, the vertical axis in the sagittal plane was defined as 0 degrees, as a reference axis. On the other hand, the joint degree was defined as 0 degrees in the anatomically upright position. Equation (1) was used to calculate the joint angles. Before inputting the results of the motion analysis to the musculoskeletal model, skeletal and muscular information for the musculoskeletal model of a pregnant woman were modified to fit the measurements of the participant in this study, as described in Section 2.3. Then, the data from the change in the joint angle from the IMUs and the reaction forces from the ground and chair obtained from the WBBs were inputted to BoB to estimate the joint torque. Finally, the muscle torque was estimated using the joint torque through optimization in the model:
2.5. Estimating Co-Contraction Activation Using a GA
From a comparison between the results of the musculoskeletal model and EMG, it is observed that the co-contraction activation of agonist and antagonist muscles cannot be estimated with the current system. Thus, other estimation methods of the muscle torque of the rectus abdominis and erector spinae for pregnant women were needed to resolve the problem. However, most proposed methods for estimating muscle torque require measuring MVC tasks and the MVC of a rectus abdominis is risky during pregnancy. Consequently, an estimation method for the muscle torque and joint torque from EMG using a GA was selected [21]. With this method, some conversion models used to calculate torque from EMG data were proposed. From these models, the model shown in Equation (2) was used as a reference in this study:
= estimated torque, = processed EMG signal, xj = associated model parameters.
Equation (2) expresses the formula for estimating joint torque generated in the joint from the joint-bridging muscle, obtained from the EMG signal . Here, indicates the muscle torque used for the motion of the joint. The purpose of this study was to estimate two muscles torques. That is to say, the EMG signal of the rectus abdominis and erector spinae were used to estimate the joint torque generated from these muscles. Owing to this, and denote EMG data for the rectus abdominis and erector spinae, respectively, and these were substituted for in Equation (2). Therefore, Equation (3) was used in this study, where denotes the sampling time:
= processed EMG signal of rectus abdominis, = processed EMG signal of Longissimus.
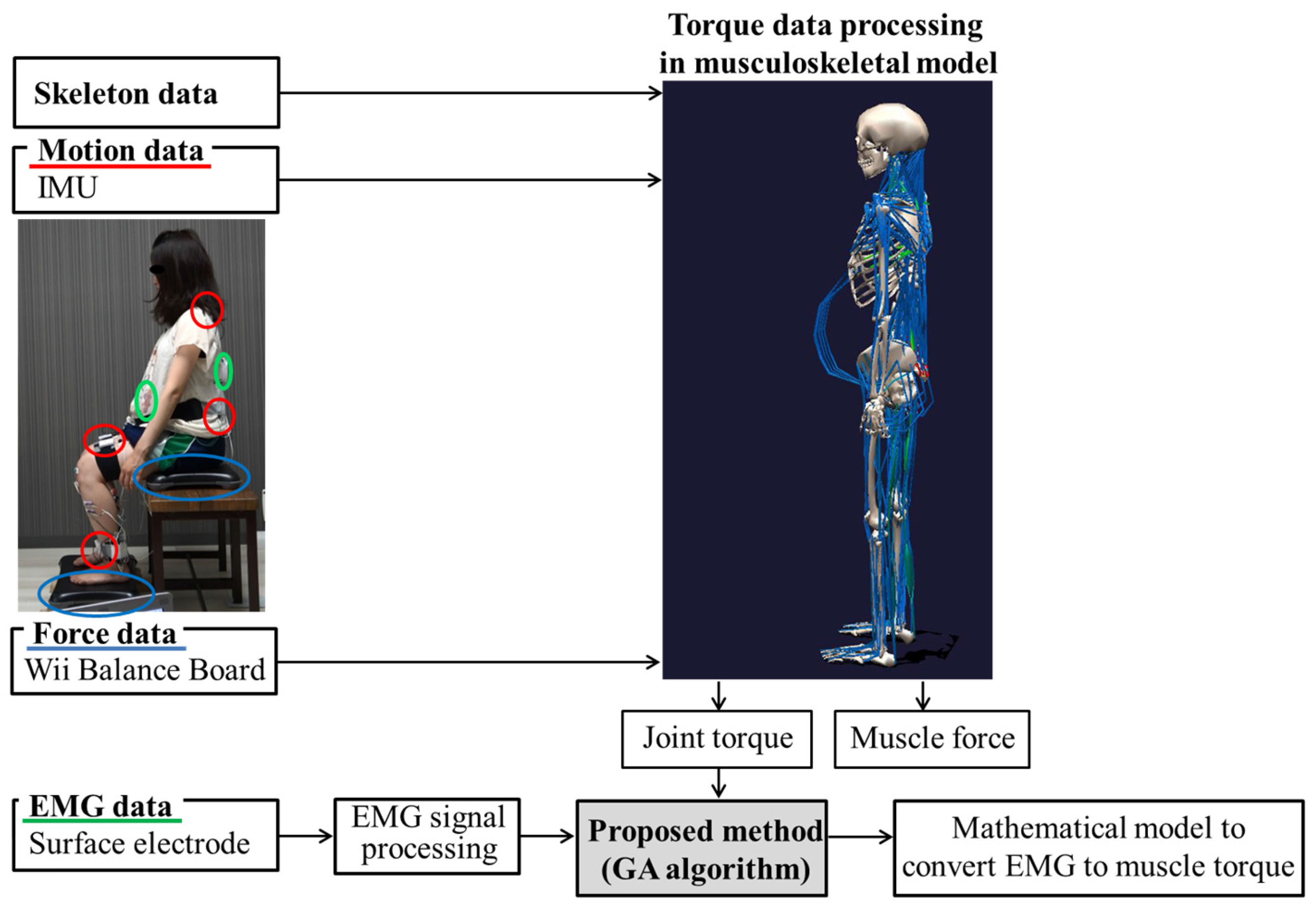
A system overview of this study is shown in Figure 7. The joint torque during STS motions was calculated for the musculoskeletal model using the skeletal data, motion data, and force data by inverse dynamics calculation. Thus, this joint torque is precise by comparison to the estimated muscle torque from the current musculoskeletal model. Meanwhile, torque expressed using Equation (3) from EMG should be equal to the joint torque, and this was used as an input value. From these values, the muscle torque was estimated using an optimized GA using Equation (4). The fitness values (FS) can only be maximized by determining a certain estimated torque () that fits the actual torque data (). In this study, the calculated joint torque from the musculoskeletal model is regarded as the actual torque. Through Equation (4), the optimal associated model parameters () were estimated using seven datasets for motion analysis from eight trials as learning data. Then, the parameters were validated using EMG data that was not used for learning.
n = Number of date of and in each trial, FS = Fitness value, = calculated joint torque from the musculoskeletal model.
Additionally, the root-mean-square error () was calculated to estimate each result from the learning sessions () and validation sessions () to evaluate the nominal performance of the learning session and the robustness of validation session, using Equation (5). Therefore, eight optimization calculations and estimations of the protocols were conducted in this study:
= The joint torque of learning session, = The estimated torque of learning session, = The joint torque of valiadation session, = The joint torque of learning session.
3. Results and Discussion
3.1. Result of Estimating Muscle Torque with the Proposed Musculoskeletal Model of a Pregnant Woman
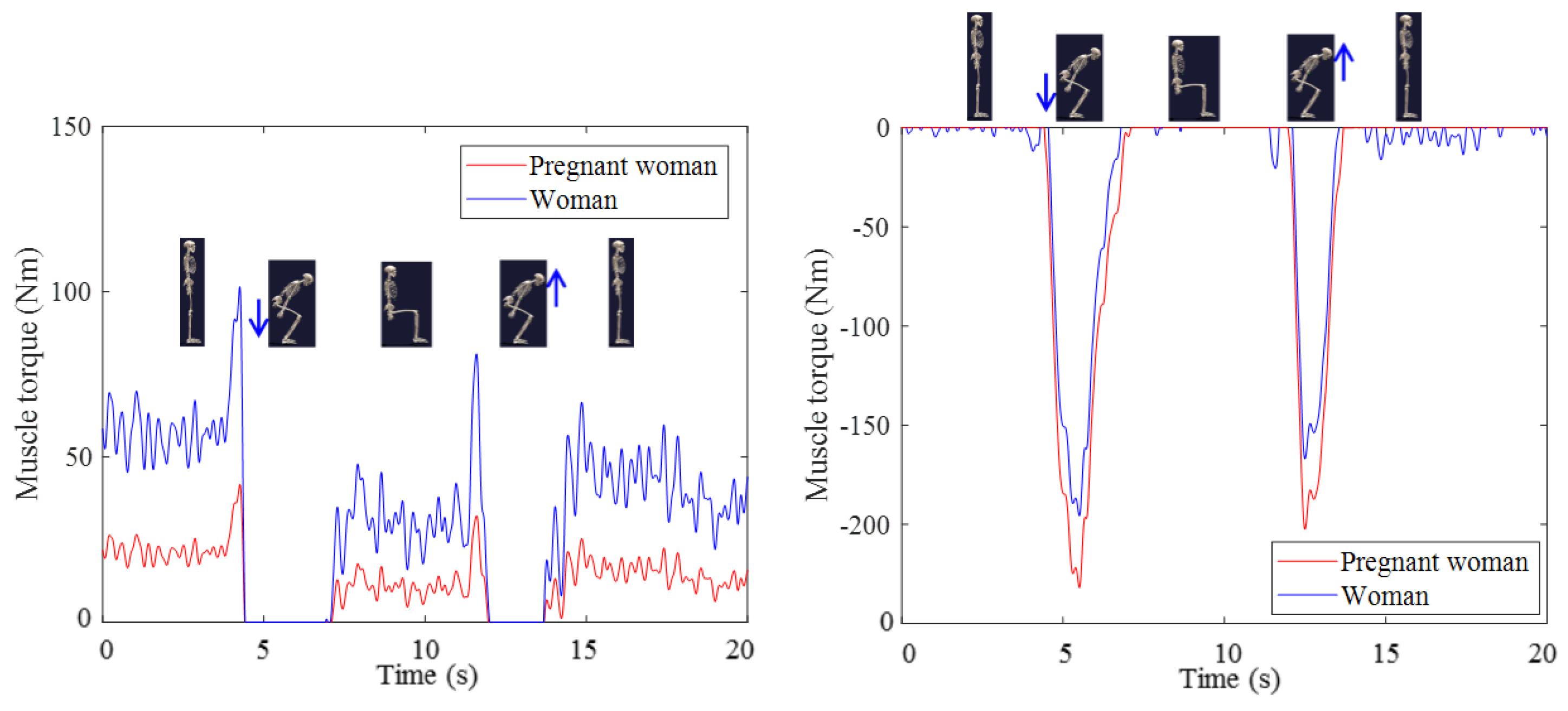
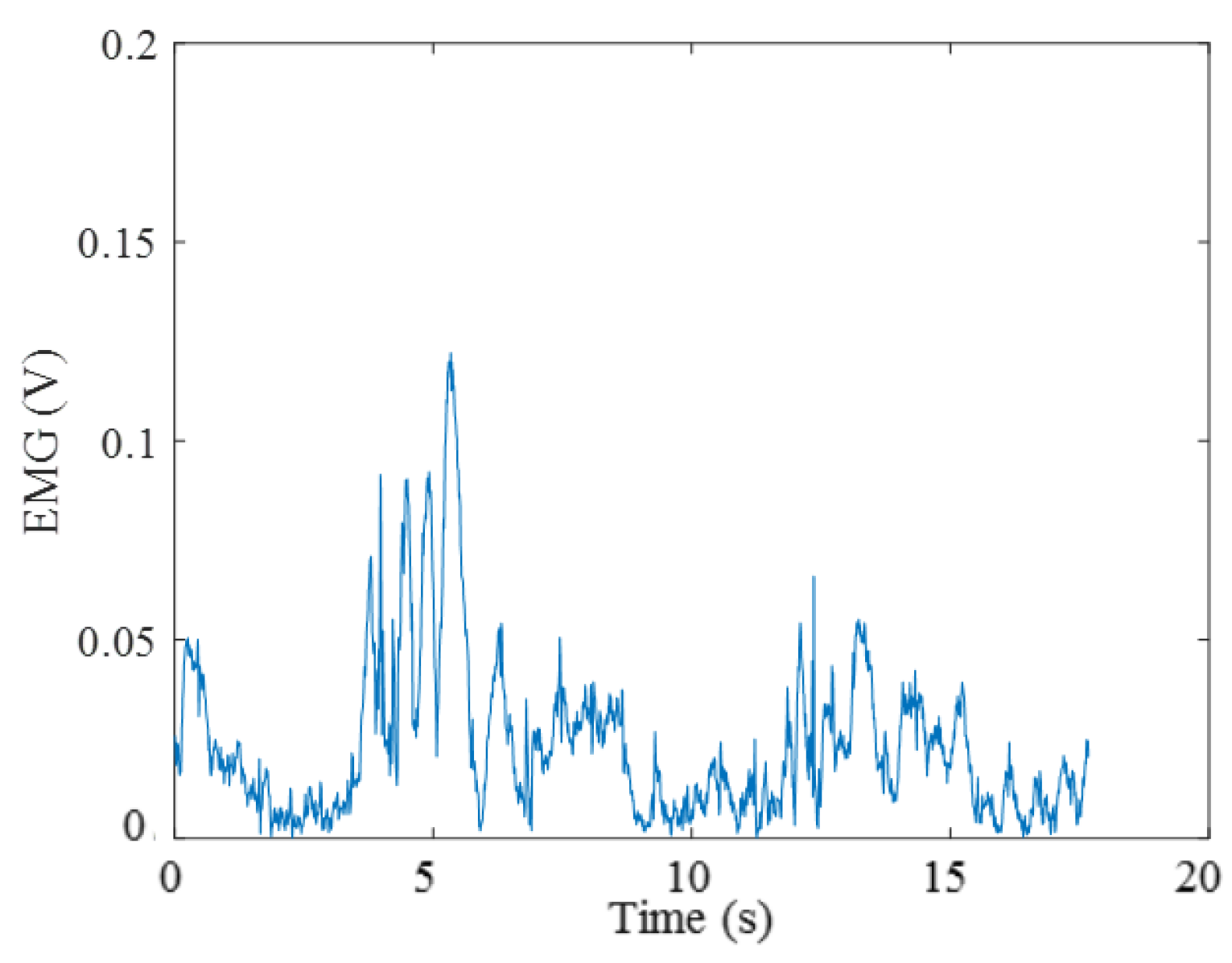
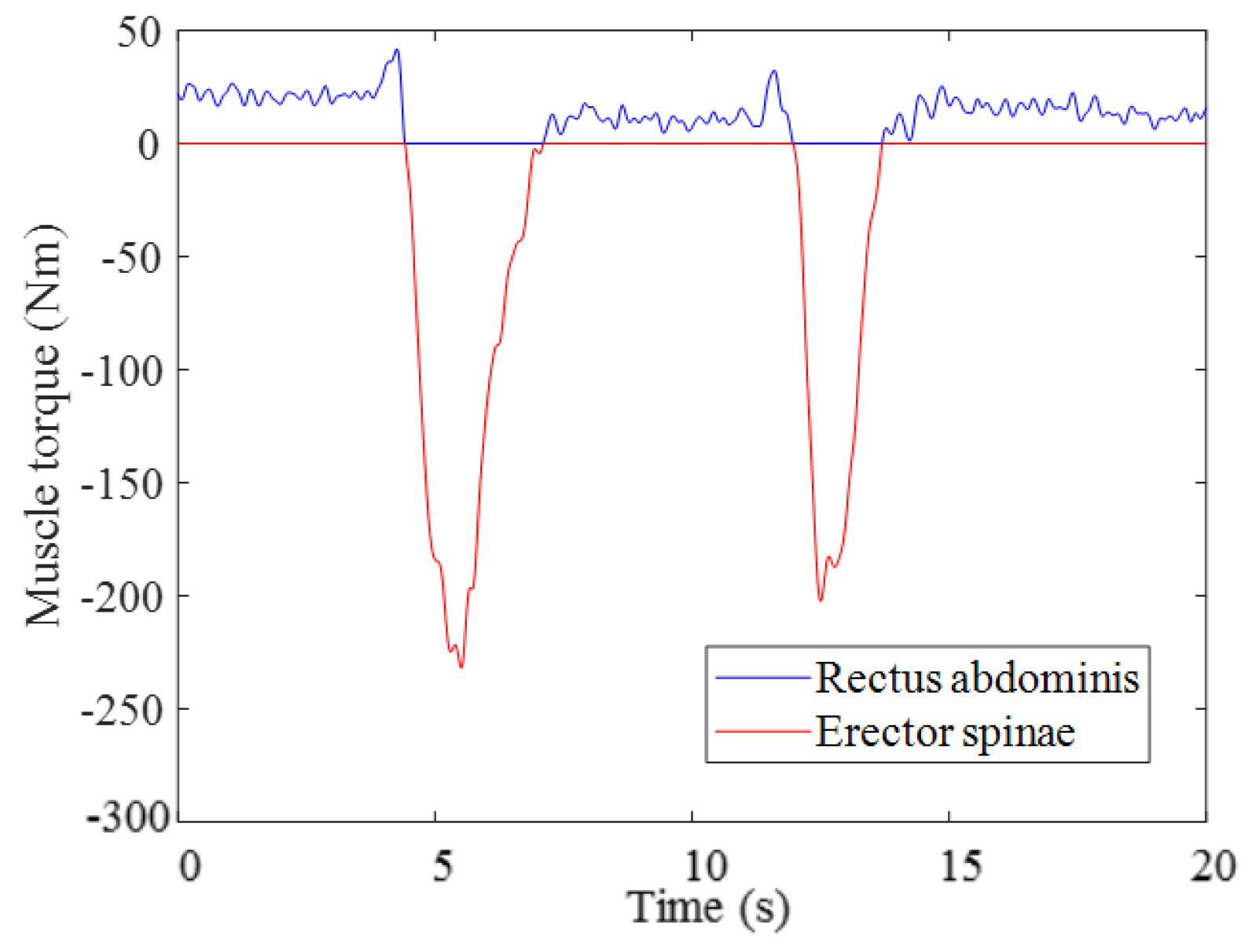
The estimated muscle torque of the rectus abdominis and erector spinae is shown in Figure 8. As shown in the figure, weakened abdominal muscle torque in the pregnant woman was observed, and this was consistent with a previous study [2]. Simultaneously, the muscle torque of the erector spinae was increased in a model for pregnant women, compared to a model for non-pregnant women. This has also been demonstrated in previous research [5]. An assessment of muscle torque, especially in the muscles around the trunk segment of pregnant women can help to assess muscle stress related to LPP, and this is useful for managing LPP [31]. Furthermore, the antagonist activation of the rectus abdominis to the erector spinae as an agonist muscle was not conspicuous from EMG, as shown in Figure 9. For example, the muscle torque of the rectus abdominis as an extension of the trunk when standing up from a chair was estimated at almost zero in the musculoskeletal model, as shown in Figure 10. By contrast, EMG data indicated that the rectus abdominis activated simultaneously with the erector spinae. It is evident from this data that an estimation of the muscle torques from co-contraction activation is needed to understand muscle activation accurately.
3.2. Results from Estimating Muscle Torque Using the GA
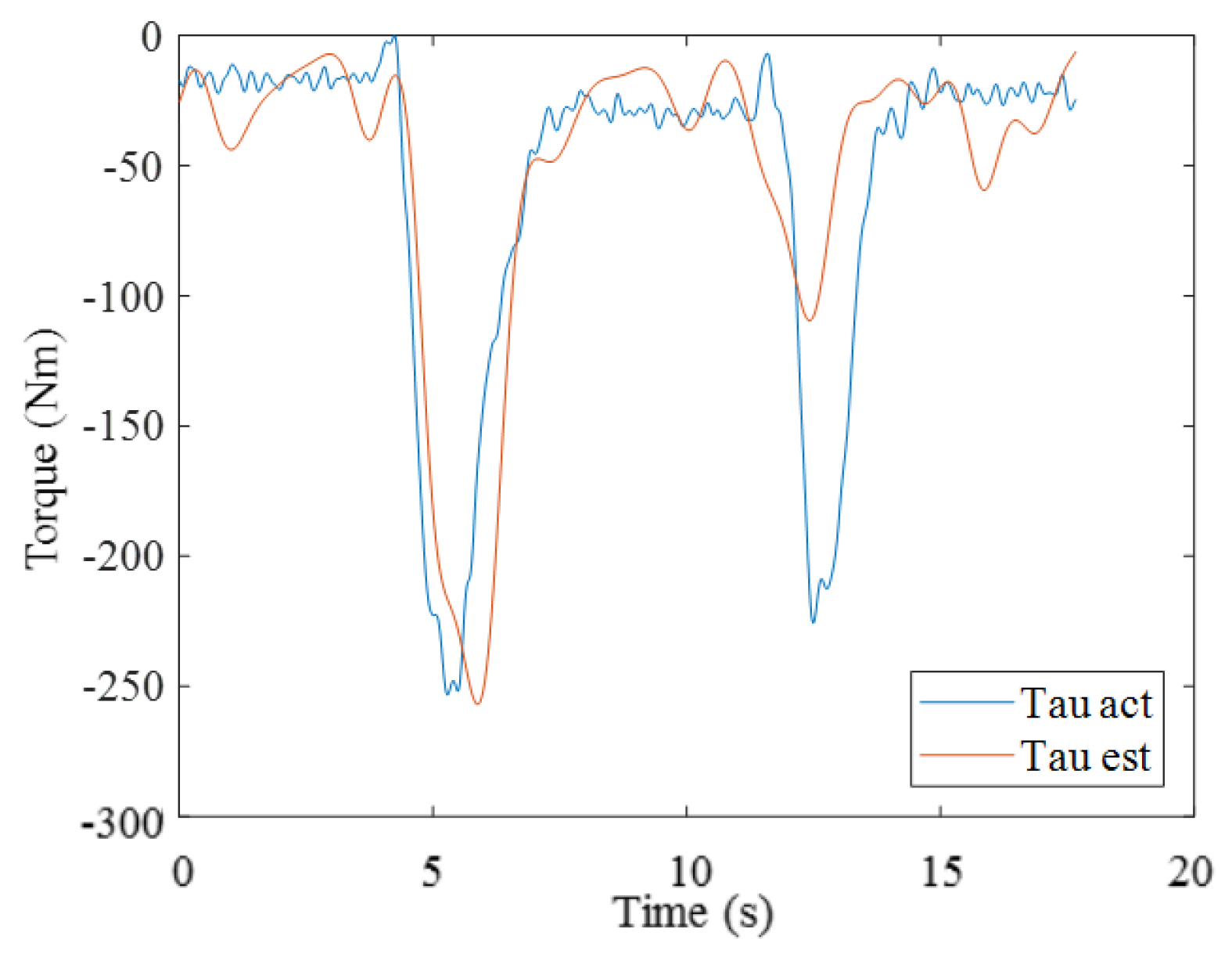
The results from validating the second trial are shown in Figure 11. Here, the values denote the calculated joint torque and estimated torque, representing the sum of muscle torque for the rectus abdominis and erector spinae using the GA. The associated model parameters and calculated for the training data and the validation session are shown in the Table 3. It is unsatisfactory that the results of muscle torque from the training session and validation session are different in each trial because this means that the results differ depending on the choice of training data. As shown in Table 2, the results for the training data and the validation session were consistently similar in every trial with the proposal method. Regarding the delay of the timing of peak in the result of estimating muscle torque using the GA in comparison to as shown in Figure 11, the similar activation of back muscles after maximum bending was observed in previous research [32]. Hence, the result might represent the actual muscle activation. From these results, the model and the parameters obtained using the GA are suitable for predicting the muscle torque in co-contracted activations of the rectus abdominis and erector spinae.
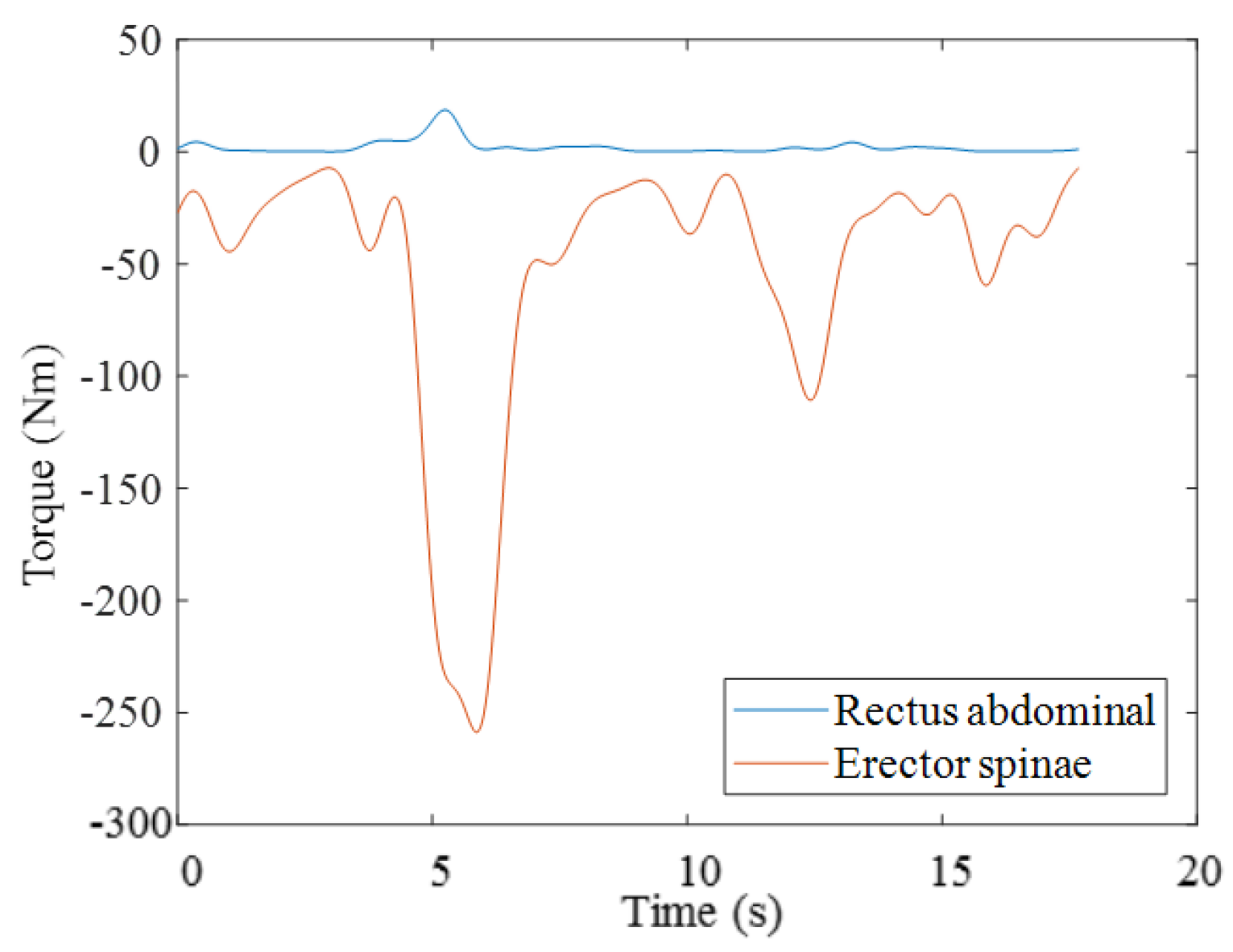
As an example of estimating muscle torque in the rectus abdominis and erector spinae using these associated model parameters as shown in Figure 12, there were 18.62 N and 233.2 N of respective torque at 5.25 s into Trial 2. From these results, the rectus abdominis was estimated to generate about 8.0% of the torque generated by the erector spinae, although this value was estimated at almost zero with the musculoskeletal model that did not consider co-contraction activation of agonist and antagonist muscles. The activation of the rectus abdominis is responsible for flexing the lumbar spine, and it is instrumental in increasing joint stabilization. In fact, the muscle torque generated by the erector spinae was 223.2 N according to the musculoskeletal model. That is, this value is lower than that from the GA-optimized model at 5.25 s into Trial 2 in this study. Therefore, the muscle stress is thought to be higher than when the antagonist muscle is not activated. This mechanism cannot be overlooked when managing LPP during pregnancy. Indeed, the GA-optimized model provides important information. It is said that the weight gain and downward shift to the center of gravity in the forward direction during pregnancy increases muscle activation especially in back muscles, accumulating muscle stress that causes LPP. Moreover, less trunk stability from changes to the body structure can lead to co-contraction activations of the abdominal and back muscles to compensate for these changes. According to the results of this study, using the GA, co-contraction activation was observed as expected. Although the activation of agonist and antagonist muscles is useful to enhance trunk stability, it concurrently increases the muscle load of the back muscles. Thus, this activation is a notable point for managing LPP during pregnancy. The muscle activation and muscle torque of the trunk muscles of pregnant women can thus be accurately estimated using the method proposed in this study. In addition, the proposed method does not require measuring MVC tasks that are dangerous for pregnant women to perform. Therefore, the proposed method provides an effective and safe way to manage LPP during pregnancy.
There were several limitations in the current study. First, the study used data from one person, rather than many participants. Therefore, further research is needed to investigate the versatility of the relationships observed in the study. Moreover, the model was made for Japanese women because the participant was Japanese. It would be ideal to construct various models using databases for women in other countries. Second, WBB only measures the vertical ground force. Consequently, some missing force from movement along the sagittal and lateral side cannot be denied. The results from muscle torque might be estimated as less than the actual values in this case. Although sagittal and lateral side motion is not especially important when sitting and standing, this limitation needs to be considered, especially when participant performs big motion at the sagittal and lateral side. Third, there are simplifications and assumptions for the musculoskeletal model, such as the size and mass of the segments of the body, using averaged values from the database. As a result, the values of muscle torque from this model cannot show the exact real values, although this model can reflect some individual features of muscle activation patterns using individual EMG data. On the other hand, the tendency for motion patterns to generate considerable muscle stress can be demonstrated. Thus, the results of the proposal method can be used to check for this tendency, and they can be used as a target indication in remedial therapy. Finally, the relationship between muscle stress and LPP in pregnant women was not evaluated. That is, it is unclear how the body should move and how the muscles should be used during pregnancy. Despite these limitations, however, the findings of the study and the proposed method will help to encourage assessments of muscle stress in the trunk muscles of pregnant women, which may in turn help to manage LPP.
4. Conclusions
The methodology for constructing a musculoskeletal model for pregnant women and estimating the co-contraction activation of muscles was presented in this paper. First, motion analysis was conducted for a pregnant woman to obtain motion, force, and EMG data during sit-to-stand motions. Then, a musculoskeletal model of a pregnant woman was developed, which considered the stretched rectus abdominis and weight gained during pregnancy. From the results of this evaluation, weakened abdominal muscle torque in pregnant women was observed using the model. Finally, the co-contraction activation of trunk muscles was estimated using a genetic algorithm, in an effort to remedy a defect in the musculoskeletal model. This proposed method enables us to assess muscle torque in a safe manner, without imposing added burdens on pregnant women. Future research on a diverse set of women—with varying body features from different ethnic backgrounds—will extend the application of the proposed method in the clinical field.
Acknowledgments
This work was supported by JSPS KAKENHI Grant Number 15J07748 and JKA’s promotion funds from KEIRIN RACE Grant Number 28-143. We are especially grateful to the participant for her willingness to participate.
Author Contributions
Saori Morino and Masaki Takahashi conceived and designed the experiments; Saori Morino performed the experiments and analyzed the data; Masaki Takahashi contributed analysis tools; Saori Morino wrote the paper.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Borg-Stein, J.; Dugan, S.A. Musculoskeletal disorders of pregnancy, delivery and postpartum. Phys. Med. Rehabil. Clin. N. Am. 2007, 18, 459–476. [Google Scholar] [CrossRef]
- Fast, A.; Weiss, L.; Ducommun, E.J.; Medina, E.; Butler, J.G. Low-back-pain in pregnancy—Abdominal muscles, sit-up performance, and back pain. Spine 1990, 15, 28–30. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.S.; Yu, W.W.; Lao, T.T.; Chow, D.H.; Chung, J.W.; Li, Y. Effectiveness of maternity support belts in reducing low back pain during pregnancy: A review. J. Clin. Nurs. 2009, 18, 1523–1532. [Google Scholar] [CrossRef] [PubMed]
- Sneag, D.B.; Bendo, J.A. Pregnancy-related low back pain. Orthopedics 2007, 30, 839–845, quiz 846–7. [Google Scholar] [PubMed]
- Casagrande, D.; Gugala, Z.; Clark, S.M.; Lindsey, R.W. Low back pain and pelvic girdle pain in pregnancy. J. Am. Acad. Orthop. Surg. 2015, 23, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.H.; Meijer, O.G.; Uegaki, K.; Mens, J.M.; van Dieen, J.H.; Wuisman, P.I.; Ostgaard, H.C. Pregnancy-related pelvic girdle pain (PPP), I: Terminology, clinical presentation, and prevalence. Eur. Spine J. 2004, 13, 575–589. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.H.; Meijer, O.G.; Bruijn, S.M.; Hu, H.; van Dieen, J.H.; Lamoth, C.J.; van Royen, B.J.; Beek, P.J. Gait in pregnancy-related pelvic girdle pain: Amplitudes, timing, and coordination of horizontal trunk rotations. Eur. Spine J. 2008, 17, 1160–1169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lund, T.; Nydegger, T.; Schlenzka, D.; Oxland, T.R. Three-dimensional motion patterns during active bending in patients with chronic low back pain. Spine 2002, 27, 1865–1874. [Google Scholar] [CrossRef] [PubMed]
- Al-Eisa, E.; Egan, D.; Deluzio, K.; Wassersug, R. Effects of pelvic asymmetry and low back pain on trunk kinematics during sitting: A comparison with standing. Spine 2006, 31, E135–E143. [Google Scholar] [CrossRef] [PubMed]
- Borg-Stein, J.; Dugan, S.A.; Gruber, J. Musculoskeletal aspects of pregnancy. Am. J. Phys. Med. Rehabil. 2005, 84, 180–192. [Google Scholar] [CrossRef] [PubMed]
- Doorenbosch, C.A.; Harlaar, J.; Roebroeck, M.E.; Lankhorst, G.J. Two strategies of transferring from sit-to-stand; the activation of monoarticular and biarticular muscles. J. Biomech. 1994, 27, 1299–1307. [Google Scholar] [CrossRef]
- Falconer, K.; Winter, D.A. Quantitative assessment of co-contraction at the ankle joint in walking. Electromyogr. Clin. Neurophysiol. 1985, 25, 135–149. [Google Scholar] [PubMed]
- Dounskaia, N. The internal model and the leading joint hypothesis: Implications for control of multi-joint movements. Exp. Brain Res. 2005, 166, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Langholz, J.B.; Westman, G.; Karlsteen, M. Musculoskeletal modelling in sports—Evaluation of different software tools with focus on swimming. Procedia Eng. 2016, 147, 281–287. [Google Scholar] [CrossRef]
- Blache, Y.; Begon, M. Influence of shoulder kinematic estimate on joint and muscle mechanics predicted by musculoskeletal model. IEEE Trans. Biomed. Eng. 2017. [Google Scholar] [CrossRef] [PubMed]
- Rajagopal, A.; Dembia, C.L.; DeMers, M.S.; Delp, D.D.; Hicks, J.L.; Delp, S.L. Full-body musculoskeletal model for muscle-driven simulation of human gait. IEEE Trans. Biomed. Eng. 2016, 63, 2068–2079. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, M.; Komura, T. An analysis of muscle load on the erector spinae of a pregnant woman. J. Biomech. Sci. Eng. 2010, 5, 357–367. [Google Scholar] [CrossRef]
- Wagner, D.W.; Stepanyan, V.; Shippen, J.M.; DeMers, M.S.; Gibbons, R.S.; Andrews, B.J.; Creasey, G.H.; Beaupre, G.S. Consistency among musculoskeletal models: Caveat utilitor. Ann. Biomed. Eng. 2013, 41, 1787–1799. [Google Scholar] [CrossRef] [PubMed]
- Cholewicki, J.; Mcgill, S.M. Emg assisted optimization—A hybrid approach for estimating muscle forces in an indeterminate biomechanical model. J. Biomech. 1994, 27, 1287–1289. [Google Scholar] [CrossRef]
- Gagnon, D.; Plamondon, A.; Lariviere, C. A biomechanical comparison between expert and novice manual materials handlers using a multi-joint emg-assisted optimization musculoskeletal model of the lumbar spine. J. Biomech. 2016, 49, 2938–2945. [Google Scholar] [CrossRef] [PubMed]
- Oyong, A.W.; Parasuraman, S.; Jauw, V.L. Robot assisted stroke rehabilitation: Estimation of muscle force /joint torque from EMG using GA. In Proceedings of the 2010 IEEE EMBS Conference on Biomedical Engineering and Sciences, Kuala Lumpur, Malaysia, 30 November–2 December 2010; pp. 341–347. [Google Scholar]
- Cheng, P.T.; Chen, C.L.; Wang, C.M.; Hong, W.H. Leg muscle activation patterns of sit-to-stand movement in stroke patients. Am. J. Phys. Med. Rehabil. 2004, 83, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.K.F.; Kippers, V.; Parnianpour, M.; Richardson, C.A. EMG activity normalization for trunk muscles in subjects with and without back pain. Med. Sci. Sport Exerc. 2002, 34, 1082–1086. [Google Scholar] [CrossRef]
- Shippen, J.; May, B. Bob—Biomechanics in matlab. In Proceedings of the 11th International Conference BIOMDOLE 2016, Druskininkai, Lithuania, 20–22 October 2016. [Google Scholar]
- Shippen, J.; May, B. Teaching Biomechanical Analysis Using Matlab/Simulink; Coventry University: Coventry, UK, 2013. [Google Scholar]
- Life and Welfare Technology Center. “Human Characteristics Database”, Human Characteristics Database. Available online: http://www.tech.nite.go.jp/human/indexeng.html (accessed on 6 June 2017).
- Matsuo, A.; Fukunaga, T.; Funato, K.; Asami, T.; Yamaguchi, T. Examination of mass and location of the center of gravity of segment of the body in Japanese women. Proc. Dep. Sports Sci. Coll. Arts Sci Univ. Tokyo 1990, 24, 37–54. [Google Scholar]
- Kioka, E.; Mori, Y. Basic study on designing maternity wear corresponding to change of body form in the later stage of pregnancy (Part 1): Experimental study on suitability of maternity dress. J. Home Econ. Jpn. 1994, 45, 137–146. [Google Scholar]
- Sunaga, Y.; Kanemura, N.; Anan, M.; Takahashi, M.; Shinkoda, K. Estimation of inertial parameters of the lower trunk in pregnant japanese women: A longitudinal comparative study and application to motion analysis. Appl. Ergon. 2016, 55, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Madgwick, S.O.H.; Harrison, A.J.L.; Vaidyanathan, R. Estimation of imu and marg orientation using a gradient descent algorithm. Int. Conf. Rehabil. Robot. 2011. [Google Scholar] [CrossRef]
- Hall, H.; Cramer, H.; Sundberg, T.; Ward, L.; Adams, J.; Moore, C.; Sibbritt, D.; Lauche, R. Theeffectiveness of complementary manual therapies for pregnancy-related back and pelvic pain: A systematic review with meta-analysis. Medicine 2016, 95, e4723. [Google Scholar] [CrossRef] [PubMed]
- Goulart, F.R.; Valls-Sole, J. Patterned electromyographic activity in the sit-to-stand movement. Clin. Neurophysiol. 1999, 110, 1634–1640. [Google Scholar] [CrossRef]
Figure 1.
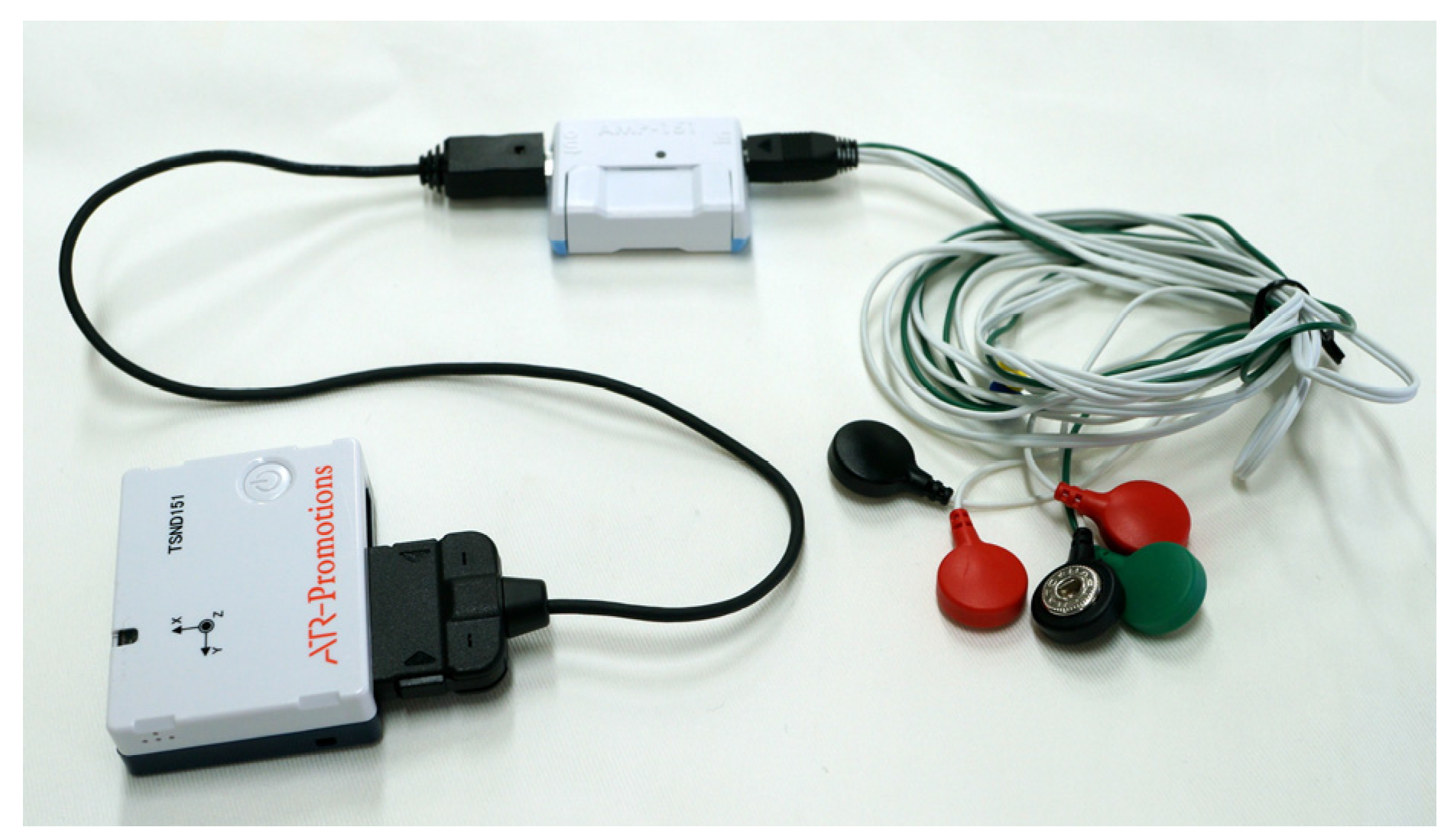
Appearance of sensors for motion analysis. The box on the left is the inertial measurement unit (IMU) (TSND151, ATR-Promotions Co., Ltd., Kyoto, Japan). The box in the middle is the electromuscular amplifier unit (AMP-151 ATR-Promotions Co., Ltd., Kyoto, Japan), and the cables on the right are surface electrodes (SE-C-AMP-H100, ATR-Promotions Co., Ltd., Kyoto, Japan) for measuring electromyography.
Figure 1.
Appearance of sensors for motion analysis. The box on the left is the inertial measurement unit (IMU) (TSND151, ATR-Promotions Co., Ltd., Kyoto, Japan). The box in the middle is the electromuscular amplifier unit (AMP-151 ATR-Promotions Co., Ltd., Kyoto, Japan), and the cables on the right are surface electrodes (SE-C-AMP-H100, ATR-Promotions Co., Ltd., Kyoto, Japan) for measuring electromyography.
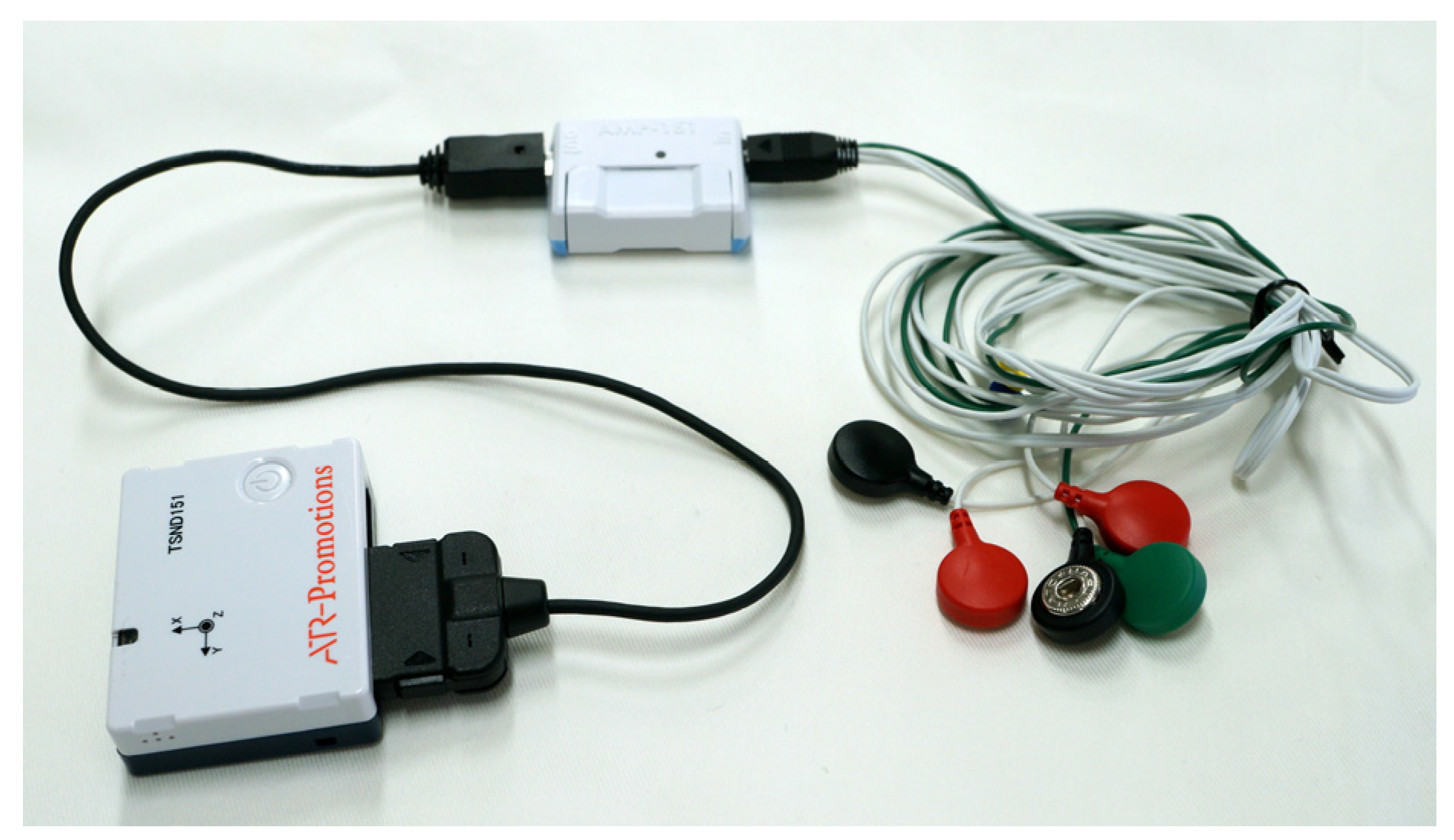
Figure 2.
Position of the IMUs and surface electrodes. The surface electrodes were placed on the right and left side of the body.
Figure 2.
Position of the IMUs and surface electrodes. The surface electrodes were placed on the right and left side of the body.
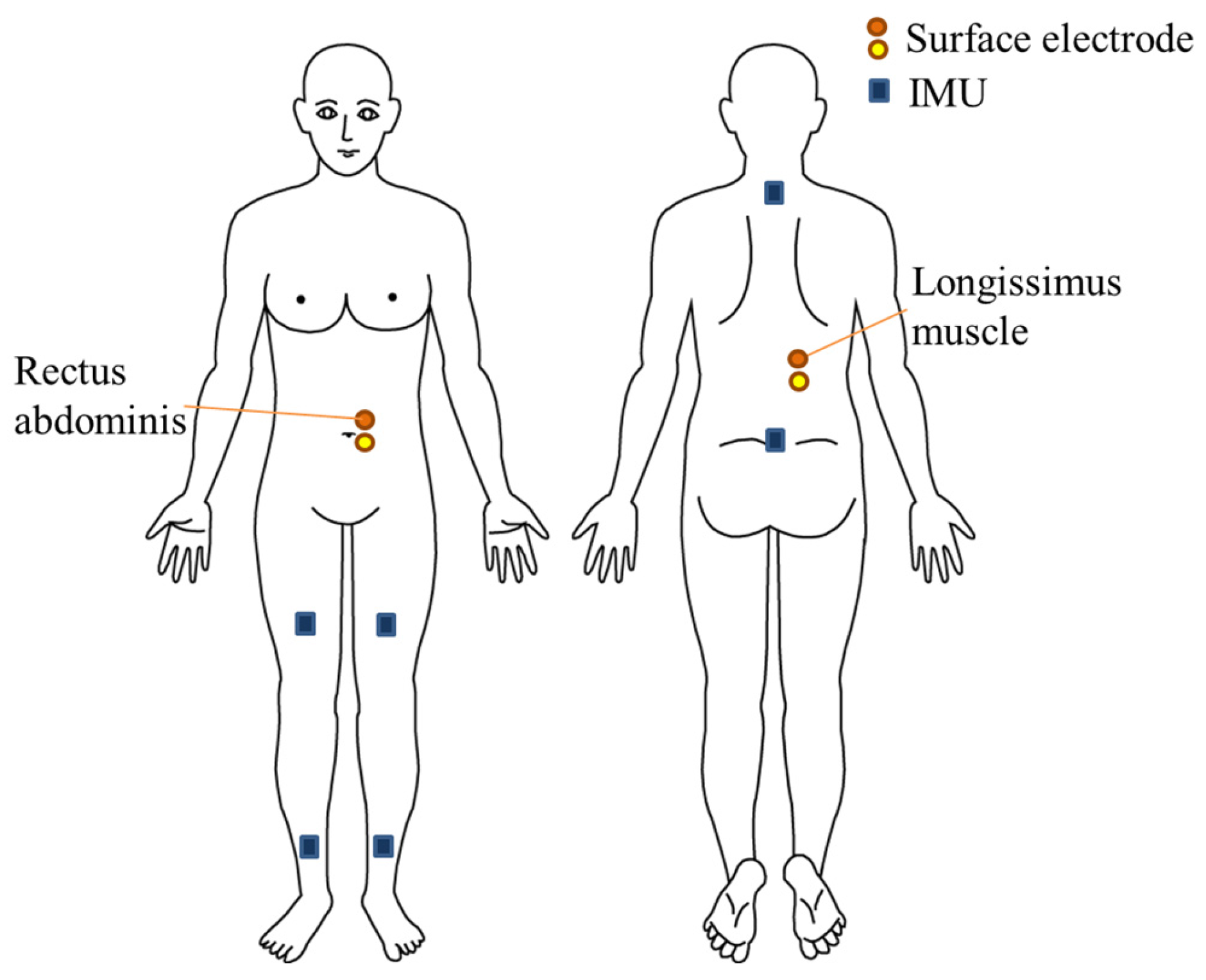
Figure 3.
Experimental setting.

Figure 4.
Musculoskeletal model of an average woman (a) and a pregnant woman (b). (A)–(C) express the points that were used to decide the wrapping points of the rectus abdominis and are correspondence to the (A)–(C) in Table 2.
Figure 4.
Musculoskeletal model of an average woman (a) and a pregnant woman (b). (A)–(C) express the points that were used to decide the wrapping points of the rectus abdominis and are correspondence to the (A)–(C) in Table 2.
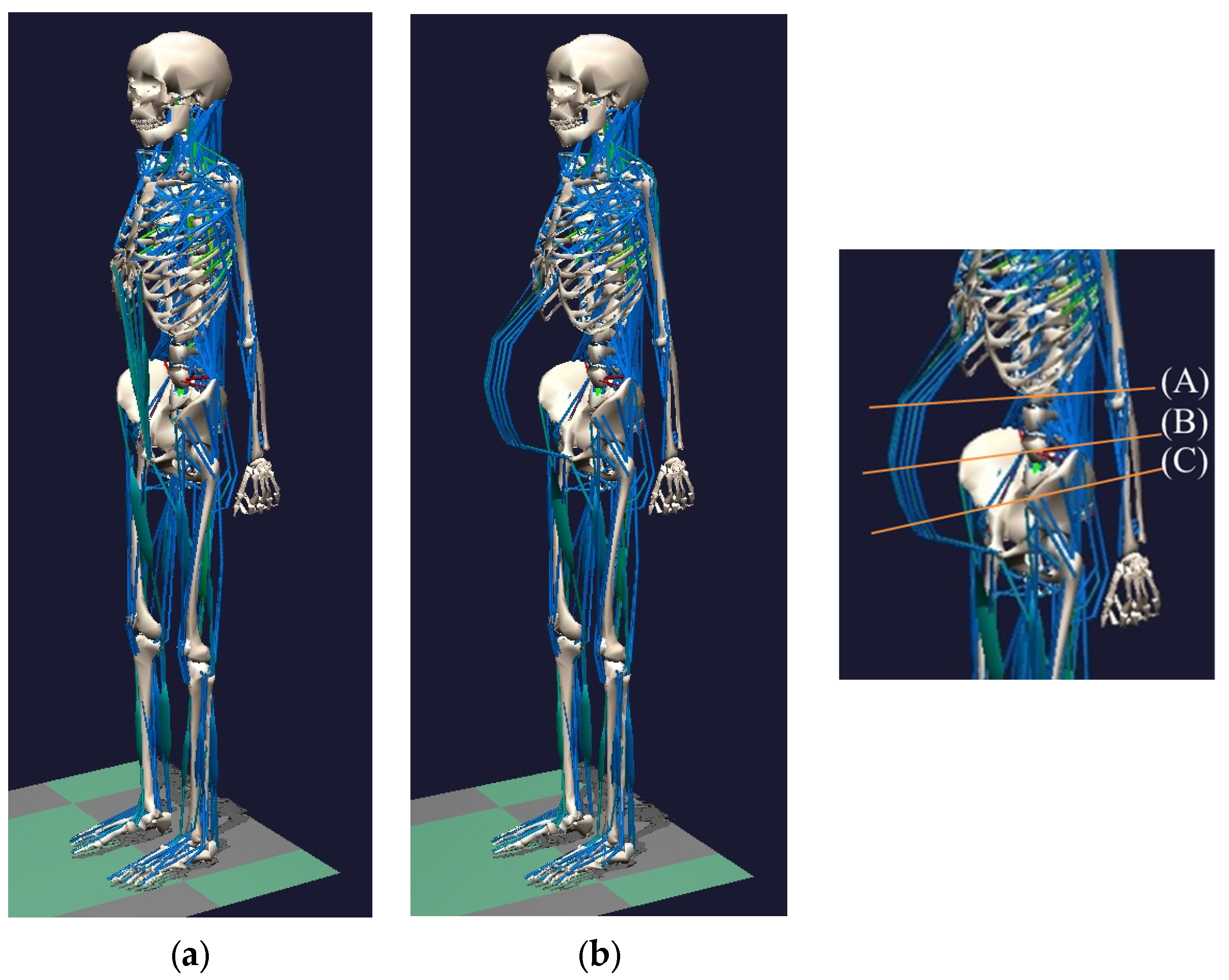
Figure 5.
Points of additional mass for the musculoskeletal model for pregnant women. The red circles indicate the points where there is increased mass.
Figure 5.
Points of additional mass for the musculoskeletal model for pregnant women. The red circles indicate the points where there is increased mass.

Figure 6.
Coordinate system and definition of angles in the study.
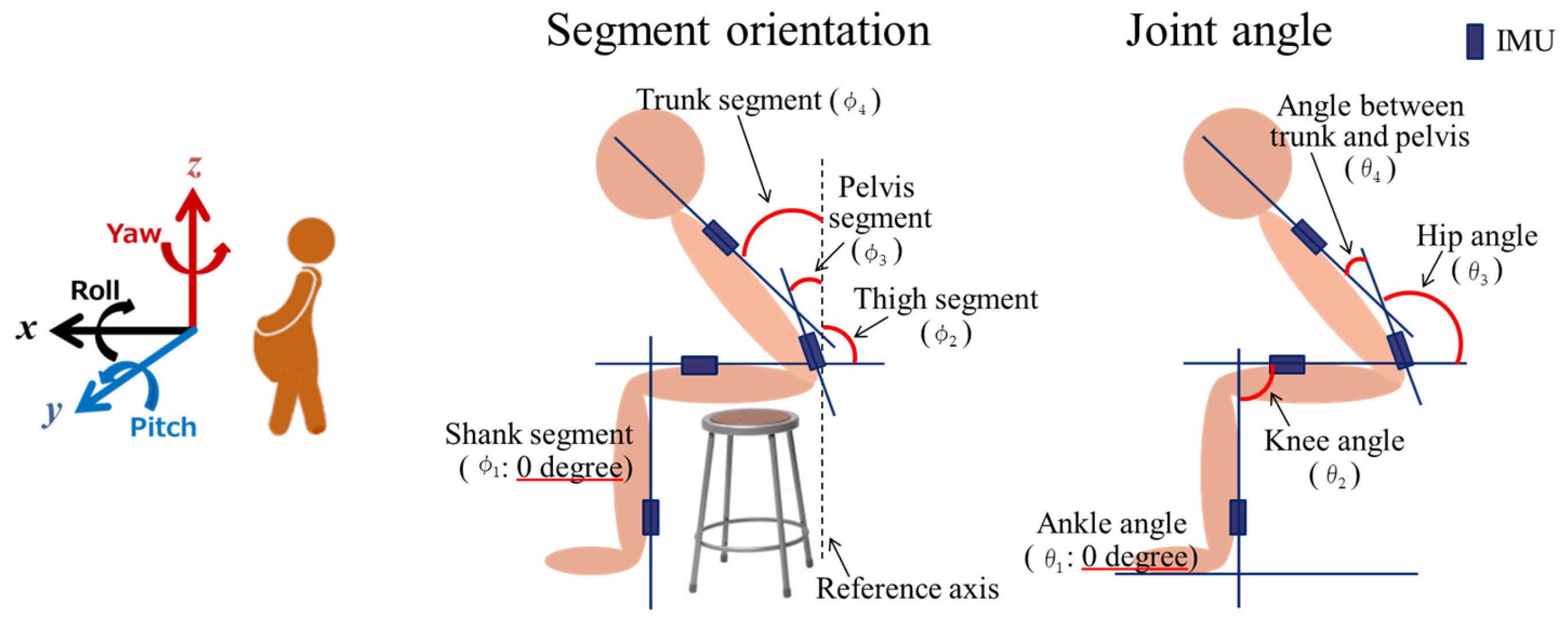
Figure 7.
System overview. EMG: electromyography. GA: genetic algorithm. IMU: Inertial measurement unit.
Figure 7.
System overview. EMG: electromyography. GA: genetic algorithm. IMU: Inertial measurement unit.
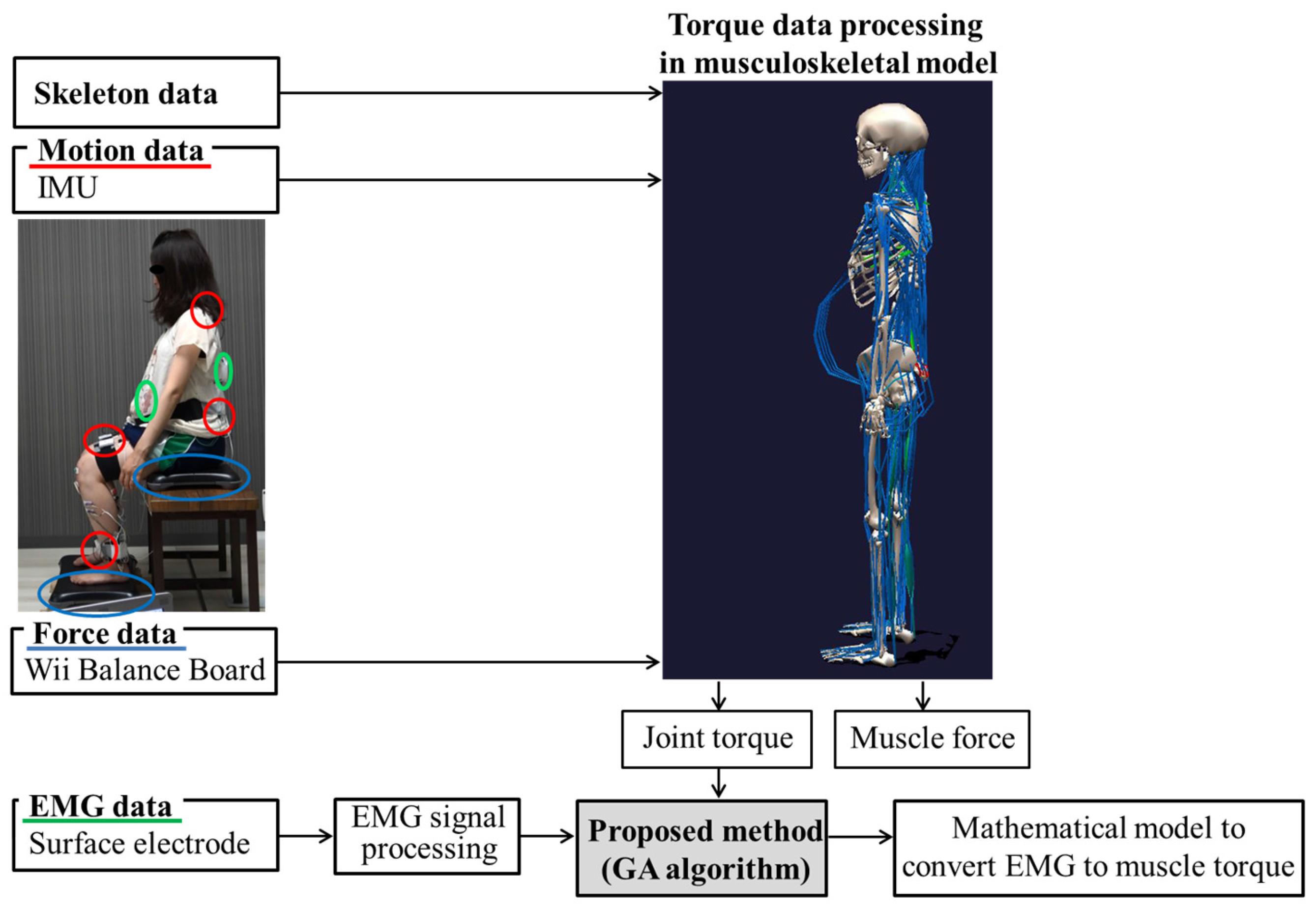
Figure 8.
Muscle torque of the rectus abdominal (left) and erector spinae (right) comparing a pregnant woman and a non-pregnant woman during the sit-to-stand (STS) motions according to the musculoskeletal model.
Figure 8.
Muscle torque of the rectus abdominal (left) and erector spinae (right) comparing a pregnant woman and a non-pregnant woman during the sit-to-stand (STS) motions according to the musculoskeletal model.

Figure 9.
Results of muscle activation patterns of the rectus abdominis with EMG.

Figure 10.
Results from estimating the muscle torque of the rectus abdominis and erector spinae with the musculoskeletal model.
Figure 10.
Results from estimating the muscle torque of the rectus abdominis and erector spinae with the musculoskeletal model.
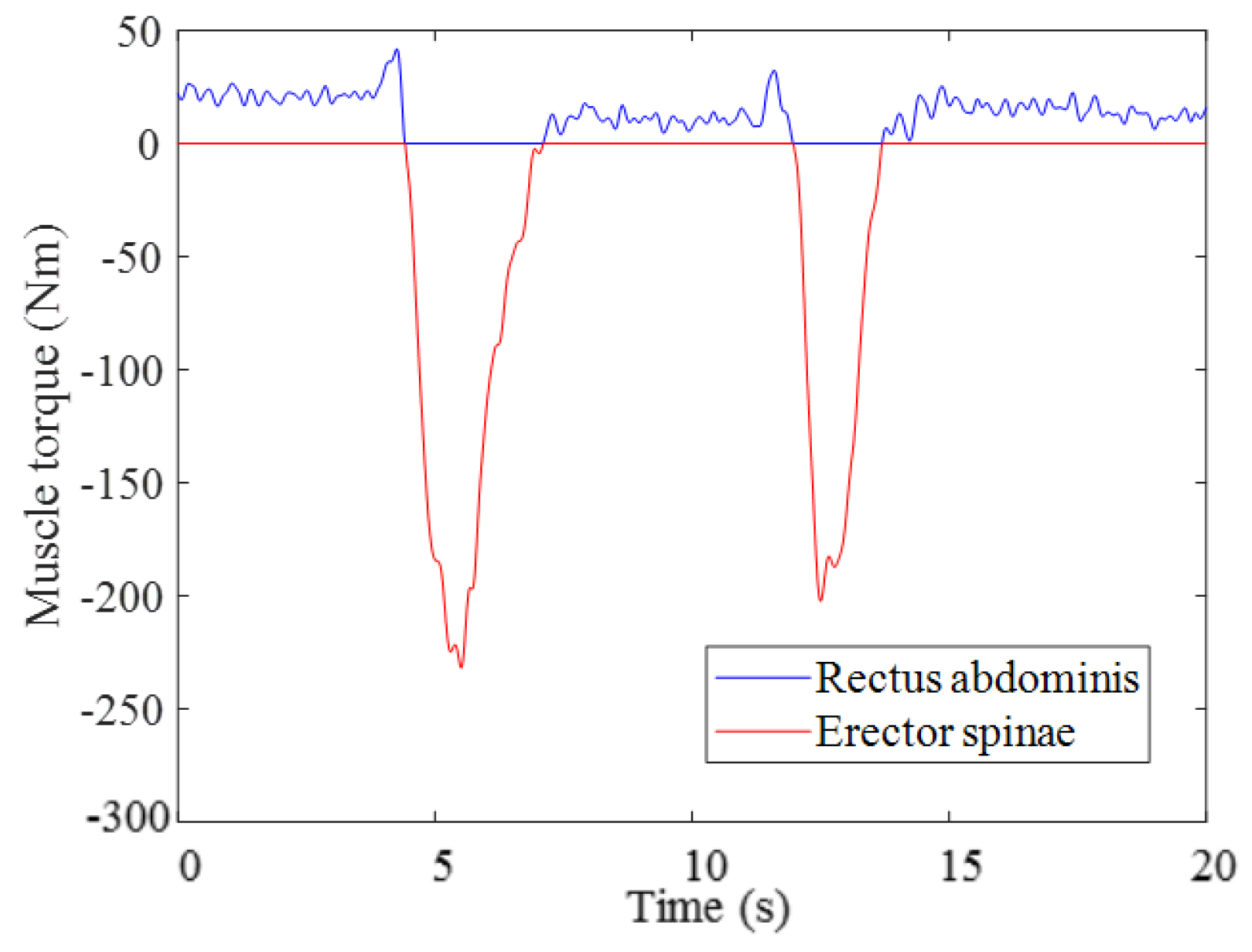
Figure 11.
Results from estimating muscle torque using the GA in Trial 2.
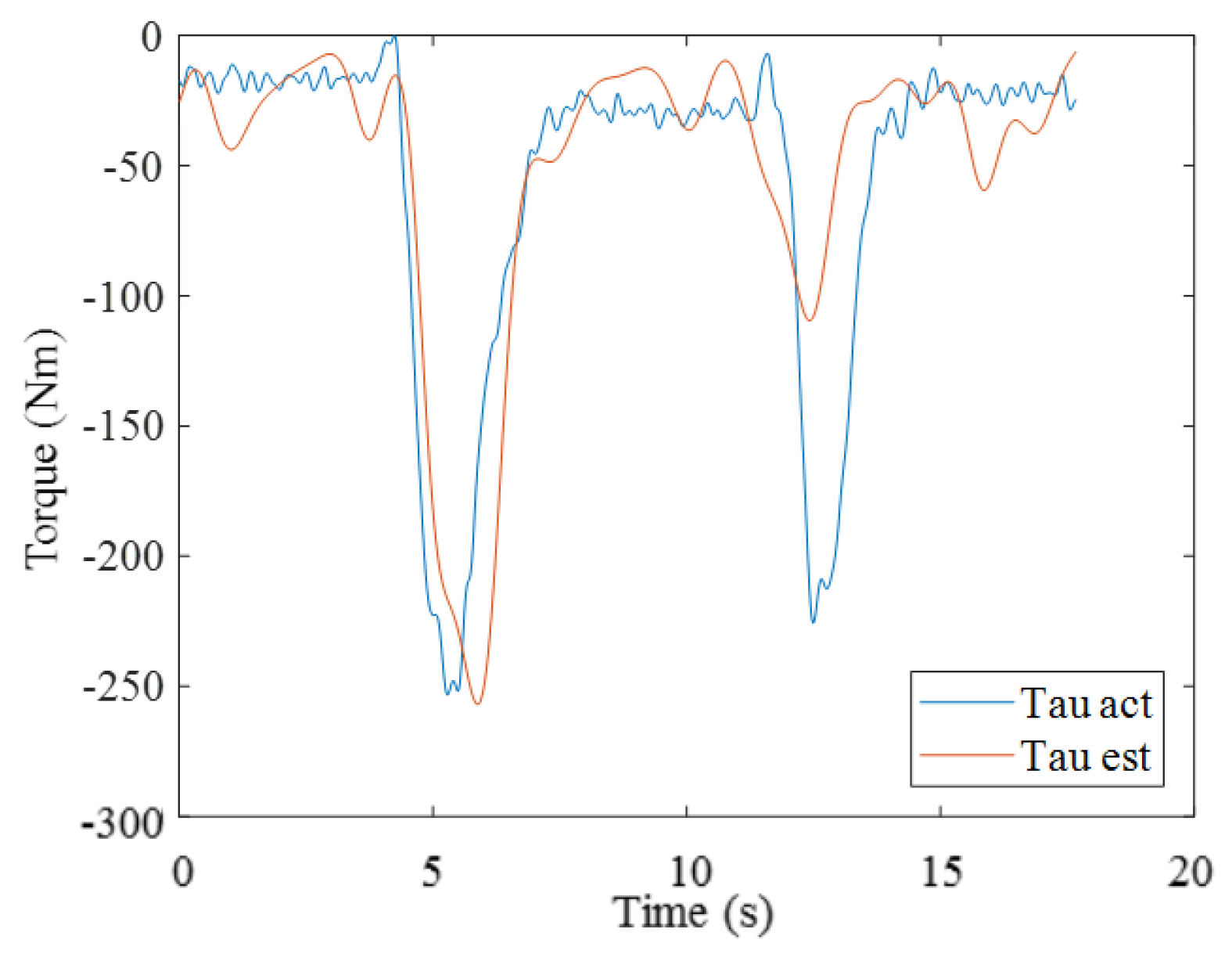
Figure 12.
Results from estimating muscle torque of the rectus abdominis and erector spinae using the GA in Trial 2.
Figure 12.
Results from estimating muscle torque of the rectus abdominis and erector spinae using the GA in Trial 2.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Physical characteristics of the participant.
| Age (years) | Duration of Pregnancy (weeks) | Height (cm) | Mass (at the Experiment) (kg) | Mass (before Pregnancy) (kg) | Experience of Childbirth |
|---|---|---|---|---|---|
| 24 | 36 | 153 | 50 | 41 | none |
Table 2.
Values used to determine enlarged rectus abdominis.
| Spinal Level | Data from Previous Research [28] | Data from a Participant of This Study | ||
|---|---|---|---|---|
| Girth (m) (Measured Value) | Depth (m) (Measured Value) | Girth (m) (Measured Value) | Depth (m) (Calculated Value) | |
| L2 (A) † | 0.865 | 0.266 | 0.840 | 0.258 |
| L4 (B) | 0.936 | 0.289 | 0.905 | 0.279 |
| L5 (C) | 0.938 | 0.290 | 0.910 | 0.281 |
† (A)–(C) are correspondence to the (A)–(C) in Figure 4.
Table 3.
Results of estimations using the genetic algorithm (GA). RMSE: root-mean-square error.
| Associated Model Parameters | RMSEl | RMSEv | ||||
|---|---|---|---|---|---|---|
| Trial 1 | x1 = 5008.0 | x2 = 1.8 | x3 = 1010.0 | x4 = 2.2 | 59.1027 | 69.0343 |
| x5 = 282.4 | x6 = 0.5 | x7 = 1092.2 | x8 = 75.7 | |||
| Trial 2 | x1 = 1560.2 | x2 = 2.1 | x3 = 1200.0 | x4 = 1.9 | 59.0246 | 39.0054 |
| x5 = −197.0 | x6 = 6.4 | x7 = 2550.1 | x8 = 1.4 | |||
| Trial 3 | x1 = 1666.3 | x2 = 2.0 | x3 = 2187.1 | x4 = 1.8 | 74.3103 | 57.0290 |
| x5 = 2180.7 | x6 = 1.2 | x7 = 2998.5 | x8 = 8.9 | |||
| Trial 4 | x1 = 302.5 | x2 = 2.0 | x3 = 1670.2 | x4 = 1.8 | 76.7090 | 54.4272 |
| x5 = 3980.9 | x6 = 7.2 | x7 = 2999.3 | x8 = 1.4 | |||
| Trial 5 | x1 = 613.1 | x2 = 2.0 | x3 = 826.6 | x4 = 2.0 | 66.0801 | 59.7488 |
| x5 = 1906.3 | x6 = 1.3 | x7 = −1397.6 | x8 = 3.4 | |||
| Trial 6 | x1 = 895.3 | x2 = 1.8 | x3 = 737.4 | x4 = 1.7 | 74.1615 | 58.9333 |
| x5 = 2006.8 | x6 = 1.7 | x7 = 1555.1 | x8 = 1.3 | |||
| Trial 7 | x1 = 5002.0 | x2 = 1.4 | x3 = 1012.0 | x4 = 2.1 | 60.4983 | 61.6914 |
| x5 = −801.5 | x6 = 1.1 | x7 = 1051.2 | x8 = 0.8 | |||
| Trial 8 | x1 = 787.4 | x2 = 2.0 | x3 = 539.7 | x4 = 2.0 | 72.2385 | 53.9310 |
| x5 = 1925.0 | x6 = 8.1 | x7 = 4619.7 | x8 = 1.6 | |||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Morino, S.; Takahashi, M. Estimating Co-Contraction Activation of Trunk Muscles Using a Novel Musculoskeletal Model for Pregnant Women. Appl. Sci. 2017, 7, 1067. https://doi.org/10.3390/app7101067
AMA Style
Morino S, Takahashi M. Estimating Co-Contraction Activation of Trunk Muscles Using a Novel Musculoskeletal Model for Pregnant Women. Applied Sciences. 2017; 7(10):1067. https://doi.org/10.3390/app7101067
Chicago/Turabian StyleMorino, Saori, and Masaki Takahashi. 2017. "Estimating Co-Contraction Activation of Trunk Muscles Using a Novel Musculoskeletal Model for Pregnant Women" Applied Sciences 7, no. 10: 1067. https://doi.org/10.3390/app7101067
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.