1. Background
The Nd:YAG Laser has become indispensable in lung surgery procedures [
1]. It is used mainly in the context of open surgical procedures for the resection of lung metastases. After opening the thorax, the entire non-ventilated lung is examined by palpation. The aim is to perform a non-anatomic resection of all palpable lung metastases in order to preserve the largest possible amount of lung parenchyma [
2]. Anatomical lung resections are only carried out when the metastases are located more centrally or have reached a certain size [
1]. If the branch of the lobar bronchus exhibits infiltration it even becomes necessary to perform sleeve lobectomy. The laser method is an excellent method for removing lung metastases with a safety distance of 5 mm [
3]. The lung metastasis is felt by palpation, after which the lung parenchyma surrounding the lesion is separated. An advantage of this method is that the resection surface is coagulated at the same time. It is thus possible for the surgeon to work without any blood loss. In addition, the lung can be inspected for further lesions [
4]. In our clinic we use the diode-pumped Nd:YAG Laser LIMAX
® 120 (wavelength: 1318 nm) (Gebrüder Martin GmbH & Co KG, Tuttlingen, Germany). The advantage of a diode-pumped Nd:YAG laser in comparison to a Nd:YAG laser is, that a higher rate of electric energy will be transformed into laser light. So the diode-pumped Nd:YAG laser is more efficient. As a rule, we work with a focusing handpiece without contact to the tissue and a laser power of 80 to 100 W. The maximum focus of the laser beam is achieved at a distance of 30 mm to the lung surface, where it exerts the maximum effect. Lung parenchyma is continuously cut and simultaneously coagulated by moving the handpiece. Smoke evacuation is required due to the development of smoke during the procedure.
As an alternative to the focusing handpiece, a laser fiber of a so-called bare fiber can also be used. A 600 µm bare fiber is currently available for applications involving the lung parenchyma. The separation of the lung parenchyma is performed through direct contact with the laser fiber, which is moved forward. Similar to a scalpel, the surgeon is able to precisely cut through the tissue with the laser. The laser fiber is held by hand with a laser fiber holder. The laser fiber is guided along the intended resection line with permanent contact to the lung parenchyma. If tissue particles adhere to the laser fiber, there is always the risk of spontaneous ignition and burning of the laser fiber, which must then be prepared again for further use. Unfortunately, there are no data available on the extent of the local effect of this bare fiber on the lung parenchyma depending on the operating speed and laser power. We would like to study this question using a specially developed experimental design.
2. Material and Methodology
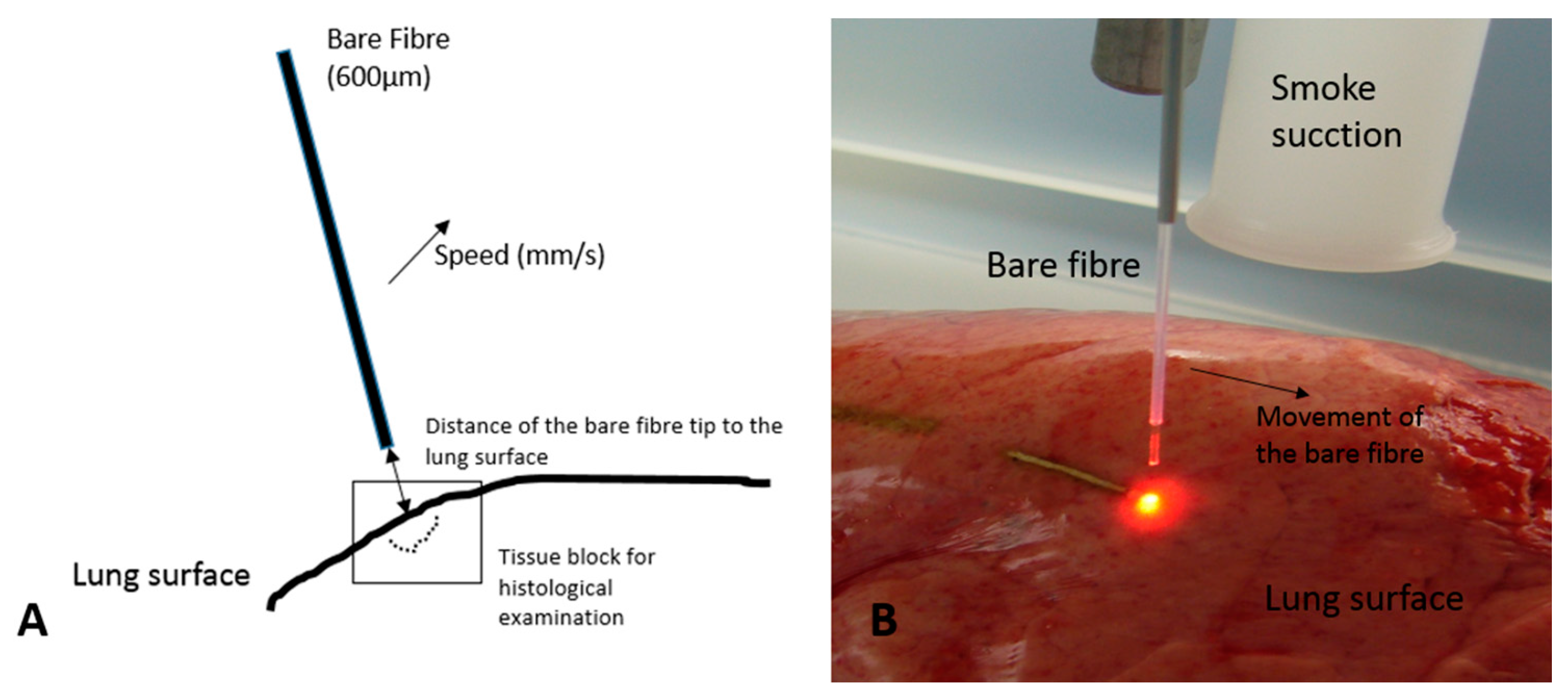
Lungs from recently slaughtered pigs were removed at the abattoir (weight EU standard: 90 kg). After exsanguination and death of the animals, they were transported to a water vapor instillation to remove all the bristles from their skin. No hot water bath was used, therefore the risk of hot water aspiration is negligible. After opening of the thorax by the butcher no lung edema was seen. Anyway we controlled all lungs for signs of lung edema or other pathological changes before immediate transportation to our laboratory. As soon as the lungs arrived in our laboratory they were laid on a flat table such that the surface of the lungs was parallel to the table. The lung surface was then visually inspected for damage. A 600 µm bare fiber was then precisely positioned vertically above the surface of the lungs using a mounting bracket. After that, the bare fiber was connected to the Nd:YAG Laser LIMAX
® 120 (Gebrüder Martin GmbH & Co KG, Tuttlingen, Germany). The laser power on the Nd:YAG Laser can be continuously adjusted from 0 to 120 W. The mounting bracket was connected to a hydraulic device which can be used to move it either forward or backward over a certain distance at a selectable, consistent motion speed. This construction can thus be used to feed the bare fiber forward in a precisely vertical position at a defined speed and a specific distance to the lung surface (see
Figure 1). A straight groove can then be seen on the lung surface. Depending on the laser power, only coagulation or opening of the lung parenchyma can be observed. For the study we assessed the effect of the bare fiber at three different laser powers: 20 W, 60 W, and 120 W. For each power we conducted out the tests at three different distances of the bare fiber to the lung surface: 10 mm, 5 mm, or direct contact. The bare fiber was moved across the surface of the lungs at three different speeds: 5 mm/s, 10 mm/s, and 20 mm/s. Each experiment was repeated three times.
The areas of the lung surface treated by laser were resected and sent in for histological analysis. The tissue blocks were fixed and then cut precisely vertically to the lesions. These sections were then stained with eosin and hematoxylin. The depth of the vaporization and of the coagulation zone were measured using multiple histological sections (each group n = 12). The program Image G (Version 1.49v, National Institute of Health, Bethesda, MD, USA) was used for this. After that, the mean values and the standard deviation of each group were calculated. For this we used the statistics program Graph Prism 6 (La Jolla, CA, USA).
Figure 1.
(A) Experimental design (illustration); (B) Image of the experimental design.
Figure 1.
(A) Experimental design (illustration); (B) Image of the experimental design.
3. Results
3.1. Depth of the Vaporization and Coagulation Zone at a Laser Power of 20 W
At a motion speed of 5 mm/s and contact of the tip of the bare fiber to the lung surface, we measured a depth of the vaporization zone of 756.4 ± 1.2 µm and of the coagulation zone of 221.8 ± 2.9 µm. When the distance of the tip of the bare fiber was increased to 5 mm, there was no more vaporization effect, and the coagulation depth was 143.9 ± 1.7 µm. At a distance of one centimetre, the coagulation depth decreased to 72.6 ± 1.4 µm. This was equivalent to a mean decrease in coagulation depth of 67.2%. When the motion speed was doubled and there was contact with the bare fiber, the mean depth of the vaporization zone was 436.0 ± 0.8 µm. This was equivalent to a mean decrease of 42.3%. The coagulation zone decreased to 145.0 ± 3.3 µm. This was equivalent to a mean decrease of 34.6%. At a greater distance of 5 mm or 10 mm of the tip of the bare fiber, the depth of the coagulation zone was reduced to 68.6 ± 2.0 µm and 28.08 ± 1.1 µm, respectively. When the motion speed was set to 20 mm/s, with contact of the bare fiber we measured a vaporization zone of 246.3 ± 1.4 µm and a coagulation zone of 67.45 ± 1.5 µm. This was equivalent to a decrease of 67.4% and 69.6%, respectively, compared to the tests conducted at a motion speed of 5 mm/s. At a distance of the tip of the bare fiber to the lung surface of 5 mm and 10 mm, mean depths of the coagulation zones of 38.4 ± 1.2 µm and 13.73 ± 0.4 µm were measured, respectively (see
Table 1).
Table 1.
Depth of the vaporization and coagulation zone (µm) at a laser power of 20 W of the 600 µm bare fiber.
Table 1.
Depth of the vaporization and coagulation zone (µm) at a laser power of 20 W of the 600 µm bare fiber.
| Motion Speed (mm/s)/Distance of the Bare Fiber to the Lung Surface (mm) | Vaporization Zone (µm) | Coagulation Zone (µm) |
|---|
| 5/0 | 756.4 ± 1.2 | 221.8 ± 2.9 |
| 5/5 | 0 | 143.9 ± 1.7 |
| 5/10 | 0 | 72.6 ± 1.4 |
| 10/0 | 436.0 ± 0.8 | 145.0 ± 3.3 |
| 10/5 | 0 | 68.6 ± 2.0 |
| 10/10 | 0 | 28.08 ± 1.1 |
| 20/0 | 246.3 ± 1.4 | 67.45 ± 1.5 |
| 20/5 | 0 | 38.4 ± 1.2 |
| 20/10 | 0 | 13.73 ± 0.43 |
3.2. Depth of the Vaporization and Coagulation Zone at a Laser Power of 60 W
When the bare fiber had direct contact to the lung surface at a motion speed of 5 mm/s, we measured a depth of the vaporization zone of 1411.0 ± 2.3 µm and of the coagulation zone of 324.3 ± 1.8 µm. This was equivalent to a mean increase in the vaporization zone of 46.4% compared to the previous tests performed at 20 W. The mean depth of the coagulation zone increased by 32% compared to the tests performed at 20 W. When the distance of the tip of the bare fiber to the lung surface was increased to 5 mm and 10 mm, the mean depth of the coagulation zone decreased to 164.9 ± 1.6 µm and 49.0 ± 1.6 µm, respectively. We did not observe a quantifiable vaporization effect on the lung surface. At a motion speed of 10 mm/s we measured a mean depth of the vaporization zone of 777.0 ± 0.9 µm and of the coagulation zone of 211.3 ± 1.7 µm. No vaporization effect was observed at a distance of the tip of the bare fiber to the lung surface of 5 mm and 10 mm. At these distances we measured a mean size of the coagulation zone of 101.5 ± 1.3 µm (5 mm) and 51.65 ± 1.6 µm. When the motion speed was increased to 20 mm/s, with direct contact of the bare fiber to the lung surface we measured a mean vaporization zone of 431.7 ± 2.0 µm and a coagulation zone of 78.6 ± 1.4 µm. As with the other motion speeds, we observed no vaporization effect at a distance of the tip of the bare fiber to the lung surface of 5 mm and 10 mm. The depth of the coagulation border created was measured at 45.8 ± 1.3 µm (5 mm) and 28.5 ± 1.6 µm (10 mm) (see
Table 2).
Table 2.
Depth of the vaporization and coagulation zone (µm) at a laser power of 60 W of the 600 µm bare fiber.
Table 2.
Depth of the vaporization and coagulation zone (µm) at a laser power of 60 W of the 600 µm bare fiber.
| Motion Speed (mm/s)/Distance of the Bare Fiber to the Lung Surface (mm) | Vaporization Zone (µm) | Coagulation Zone (µm) |
|---|
| 5/0 | 1411.0 ± 2.3 | 324.3 ± 1.8 |
| 5/5 | 0 | 164.9 ± 1.6 |
| 5/10 | 0 | 49.0 ± 1.6 |
| 10/0 | 777.0 ± 0.9 | 211.3 ± 1.7 |
| 10/5 | 0 | 101.5 ± 1.3 |
| 10/10 | 0 | 51.65 ± 1.6 |
| 20/0 | 431.7 ± 2 | 78.6 ± 1.4 |
| 20/5 | 0 | 45.8 ± 1.3 |
| 20/10 | 0 | 28.5 ± 1.6 |
3.3. Depth of the Mean Vaporization and Coagulation Zone at a Laser Power of 120 W
With direct contact to the lung and a motion speed of 5 mm/s, a mean depth of the vaporization zone of 2126.0 ± 1.4 µm and 450.5 ± 1.8 µm was determined. At a distance of 5 mm of the tip of the bare fiber to the lung we measured a vaporization zone of 994.7 ± 1.8 µm and a coagulation zone of 223.2 ± 2.1 µm. When the distance was doubled to 10 mm, the size of the vaporization zone was 408.0 ± 1.2 µm and the depth of the coagulation zone was 66.96 ± 2.4 µm. When increasing the motion speed to 10 mm/s, with direct contact of the bare fiber with the lung, the mean depth of the vaporization zone was 1514.0 ± 1.7 µm and that of the coagulation zone was 263.1 ± 2.8 µm. When the distance of the tip of the bare fiber was increased to 5 mm, the mean depth of the vaporization zone was measured as 764.5 ± 0.6 µm and that of the coagulation zone as 126.5 ± 2.2 µm. At a distance of 10 mm we measured a mean depth of the vaporization zone of 287.8 ± 0.7 µm and a depth of the coagulation zone of 63.7 ± 2.4 µm.
After further increasing the motion speed to 20 mm/s, with direct contact of the tip of the bare fiber, we measured a mean depth of the vaporization zone of 863.1 ± 1.7 µm and a mean depth of the coagulation zone of 102.2 ± 2.4 µm. When the distance of the tip of the bare fiber was increased to 5 mm, the depth of the vaporization zone was decreased to 425.9 ± 1.3 µm and that of the coagulation zone to 64.2 ± 2.3 µm. At a distance of 10 mm, the depth of the vaporization zone was decreased to 182.9 ± 1.5 µm and that of the coagulation zone was decreased to 38.3 ± 1.3 µm (see
Table 3).
In summary the
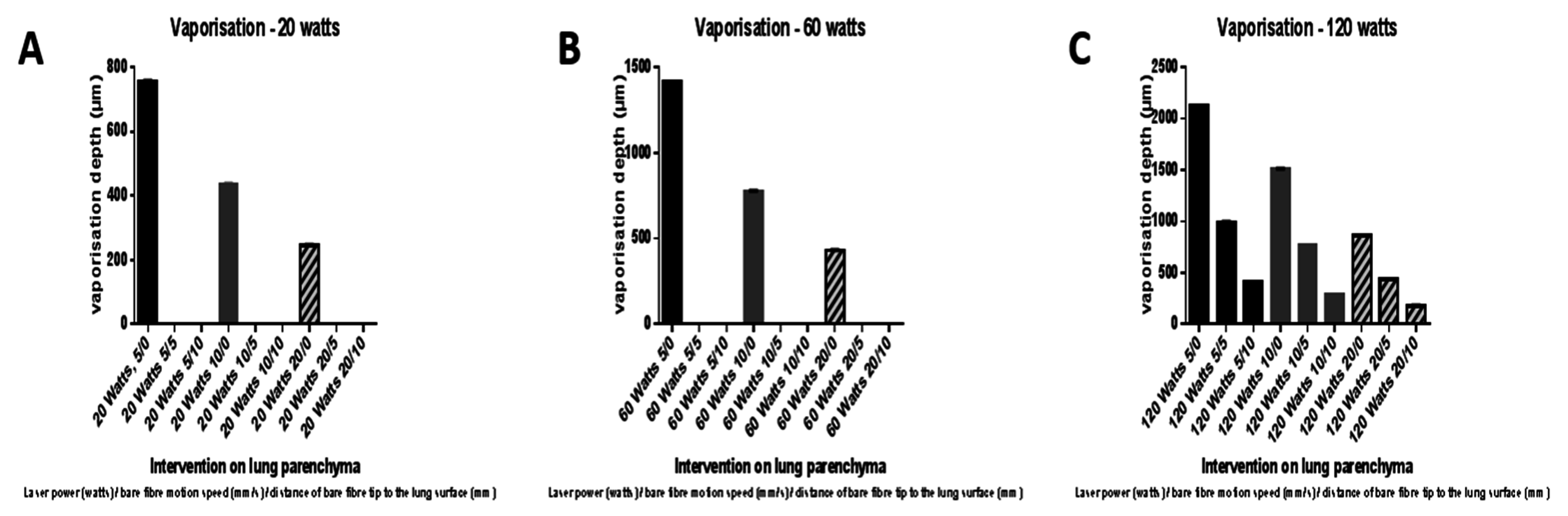
Figure 2 and
Figure 3 will show the comparison of the depths of vaporization and coagulation zones at various laser powers, motion speeds and distances of the tip of the bare fibre to the lung surface.
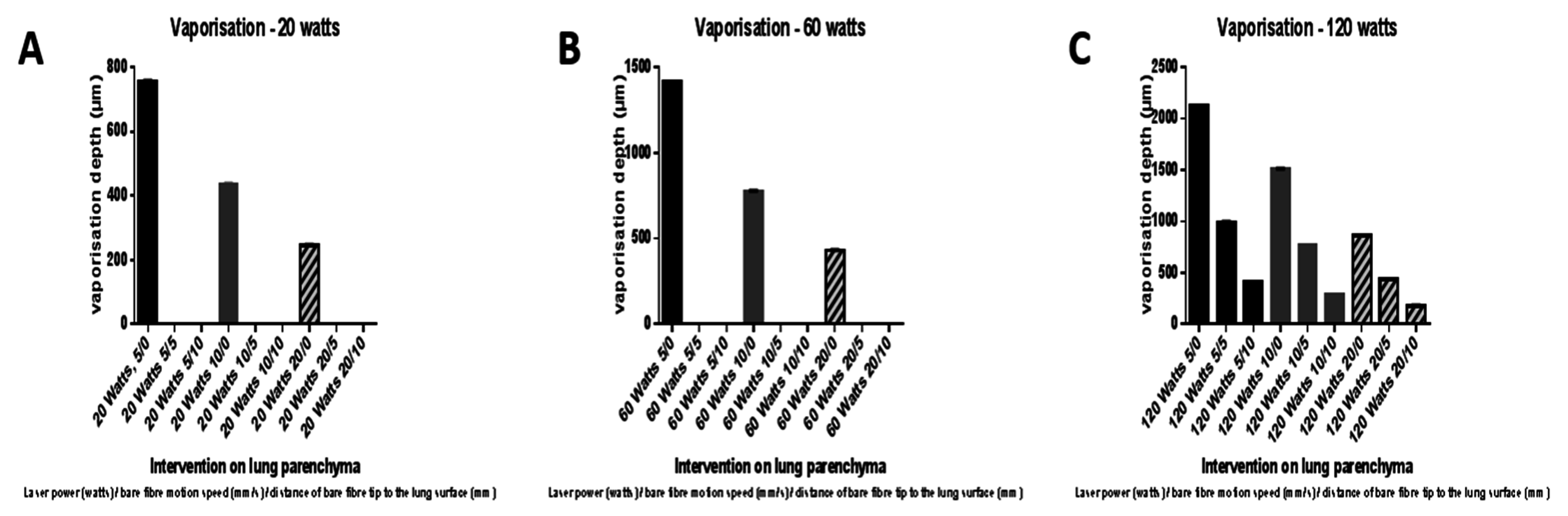
Figure 2.
Comparison of the depth of the vaporization zone (in µm) at the various laser powers (A: 20 W, B: 60 W, C: 120 W), motion speeds (5 mm/s, 10 mm/s, 20 mm/s) and distances of the tip of the bare fiber to the lung surface (0, 5 mm and 10 mm).
Figure 2.
Comparison of the depth of the vaporization zone (in µm) at the various laser powers (A: 20 W, B: 60 W, C: 120 W), motion speeds (5 mm/s, 10 mm/s, 20 mm/s) and distances of the tip of the bare fiber to the lung surface (0, 5 mm and 10 mm).
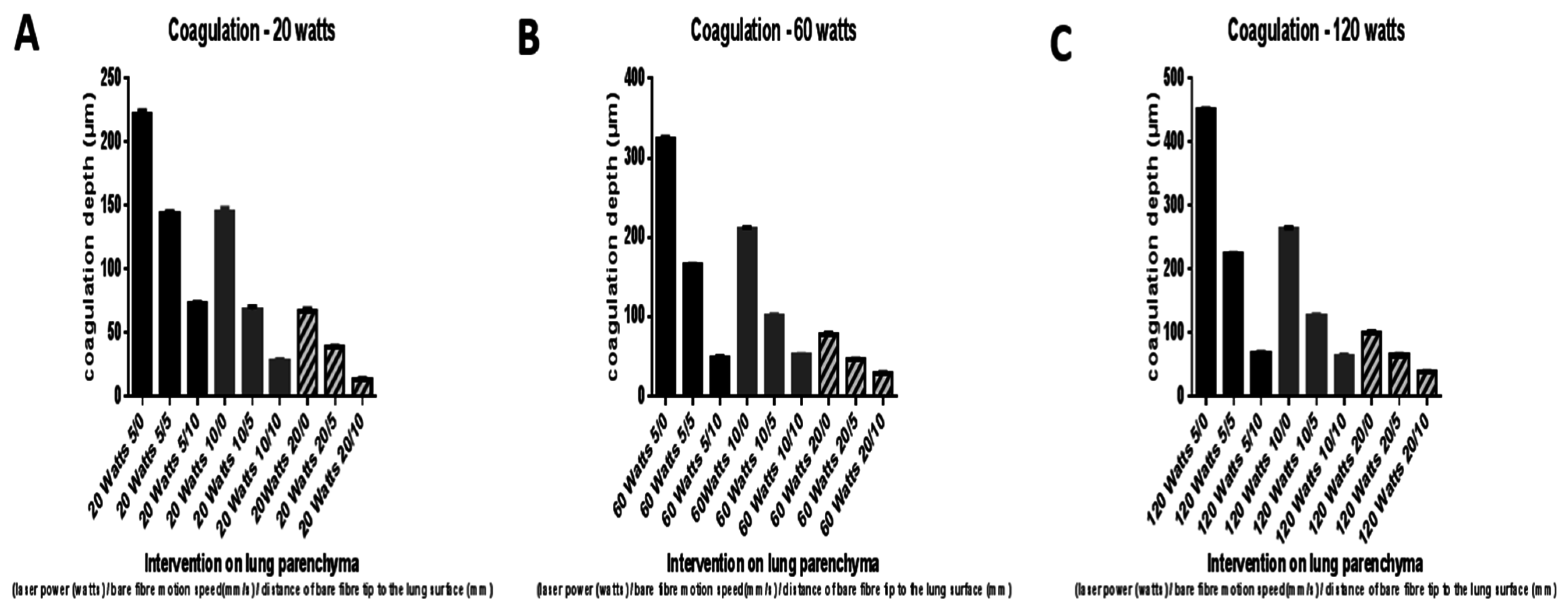
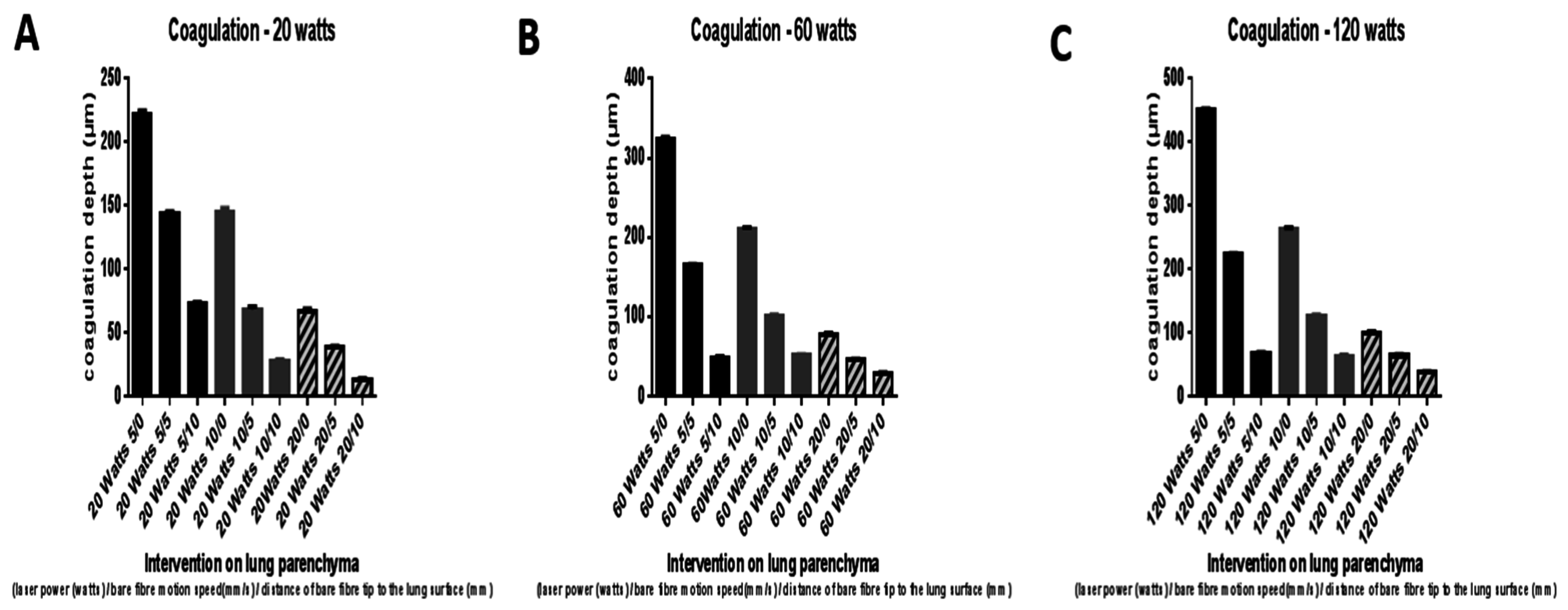
Figure 3.
Comparison of the depth of the coagulation zone (in µm) at the various laser powers (A: 20 W, B: 60 W, C: 120 W), motion speeds (5 mm/s, 10 mm/s, and 20 mm/s) and distances of the tip of the bare fiber to the lung surface (0, 5 mm and 10 mm).
Figure 3.
Comparison of the depth of the coagulation zone (in µm) at the various laser powers (A: 20 W, B: 60 W, C: 120 W), motion speeds (5 mm/s, 10 mm/s, and 20 mm/s) and distances of the tip of the bare fiber to the lung surface (0, 5 mm and 10 mm).
Table 3.
Depth of the vaporization and coagulation zone (µm) at a laser power of 120 W of the 600 µm bare fiber.
Table 3.
Depth of the vaporization and coagulation zone (µm) at a laser power of 120 W of the 600 µm bare fiber.
| Motion Speed (mm/s)/Distance of the Bare Fiber to the Lung Surface (mm) | Vaporization Zone (µm) | Coagulation Zone (µm) |
|---|
| 5/0 | 2126.0 ± 1.4 | 450.5 ± 1.8 |
| 5/5 | 994.7 ± 1.8 | 223.2 ± 2.1 |
| 5/10 | 408.0 ± 1.2 | 66.96 ± 2.4 |
| 10/0 | 1514.0 ± 1.7 | 263.1 ± 2.8 |
| 10/5 | 764.5 ± 0.6 | 126.5 ± 2.2 |
| 10/10 | 287.8 ± 0.7 | 63.7 ± 2.4 |
| 20/0 | 863.1 ± 1.7 | 102.2 ± 2.4 |
| 20/5 | 435.9 ± 1.3 | 64.2 ± 2.3 |
| 20/10 | 182.0 ± 1.5 | 38.3 ± 1.3 |
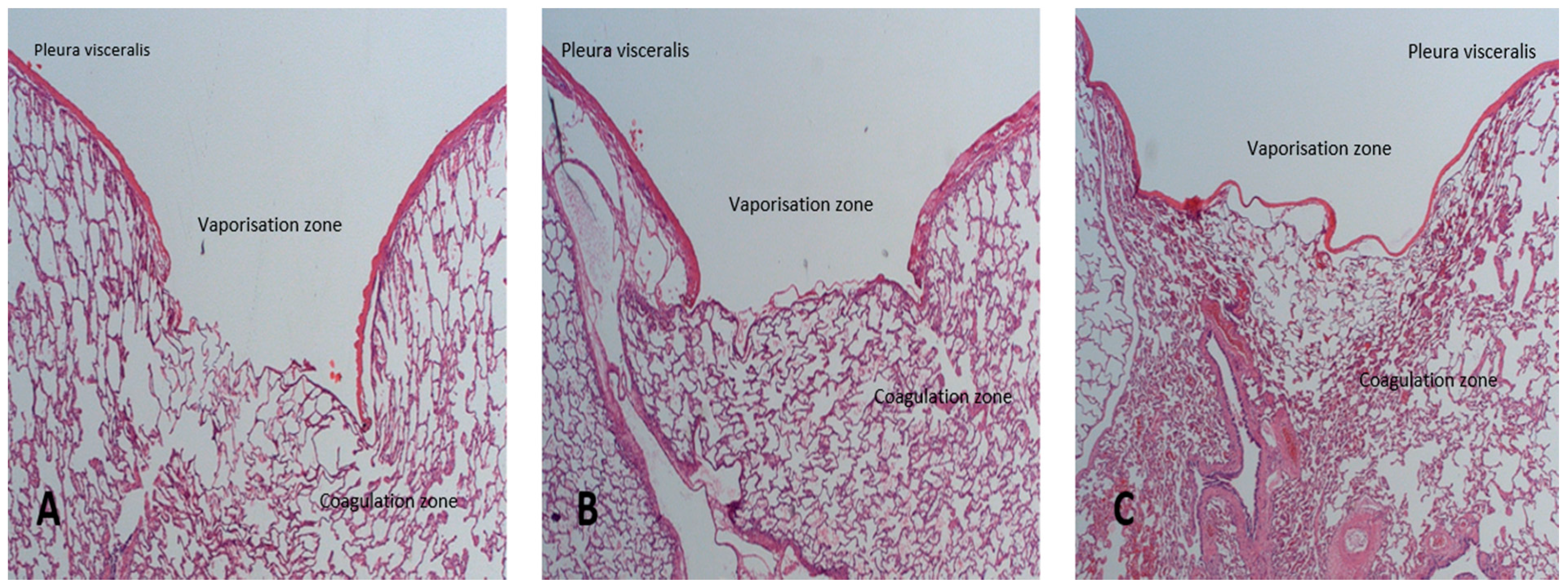
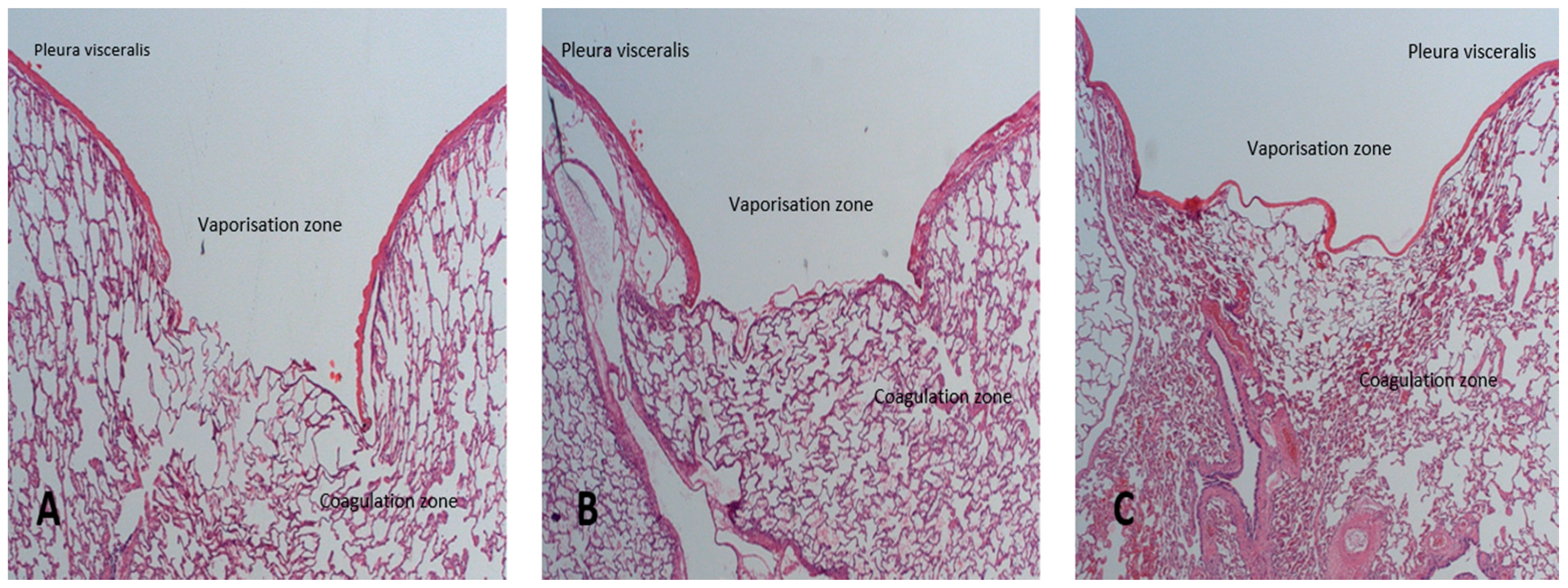
The histological analysis of the resected preparations exhibited the vaporization effects on the one hand, with varying intensities of the bordering coagulation zones. The surrounding lung parenchyma exhibited no changes owing to the laser. In
Figure 4, we show examples of three histological sections in which the effect of increasing the distance of the tip of the bare fiber to the lung surface is easy to recognize. In spite of a consistently high laser power of 120 W, we observed a marked reduction in the vaporization and coagulation zone simply by increasing the distance of the tip of the bare fiber from 5 mm to 10 mm.
Figure 4.
Histological presentation of the size of the vaporization and coagulation zone in the histological section (haematoxylin and eosin stain, magnification 12.5): (A) Laser power 120 W, motion speed 5 mm/s, direct contact of the tip of the bare fiber with the lung surface; (B) Laser power 120 W, motion speed 5 mm/s, distance of the tip of the bare fiber to the lung surface 5 mm; (C) Laser power 120 W, motion speed 5 mm/s, distance of the tip of the bare fiber to the lung surface: 10 mm.
Figure 4.
Histological presentation of the size of the vaporization and coagulation zone in the histological section (haematoxylin and eosin stain, magnification 12.5): (A) Laser power 120 W, motion speed 5 mm/s, direct contact of the tip of the bare fiber with the lung surface; (B) Laser power 120 W, motion speed 5 mm/s, distance of the tip of the bare fiber to the lung surface 5 mm; (C) Laser power 120 W, motion speed 5 mm/s, distance of the tip of the bare fiber to the lung surface: 10 mm.
4. Discussion
Lung parenchyma can be separated either by means of a laser without tissue contact using a focusing handpiece or by means of a laser fiber with direct tissue contact (so-called bare fiber). The laser fiber is guided across the lung parenchyma like a scalpel under visual control. Due to the strong development of local heat, a part of the lung parenchyma is vaporized, and the resection edges are coagulated. A hollow is thus created at the cut lung parenchyma, which is coagulated along the edge. It is therefore possible to work completely without blood loss. The laser fiber is thus not only suitable for open, but also for minimally invasive surgical procedures. As a general rule, thicker bare fibers are used for applications involving the lung parenchyma, like the 600 µm fiber we used in our study. The aim of our study was to assess the local effects of the bare fiber on the lung parenchyma at various laser powers, operating speeds and distances of the tip of the bare fiber to the surface of the lungs. The greatest effect in terms of the size of the vaporization and coagulation zone was observed at a maximum laser power of 120 W, at a low operating speed of 5 mm/s and with direct tissue contact. The lowest effect was observed at a motion speed of 20 mm/s, with direct tissue contact and a laser power of 20 Watt. The fact that a vaporization effect was no longer detectable at distances of 5 mm and 10 mm of the tip of the bare fiber to the lung surface was interesting. With increasing operating speeds and unchanged laser power, the effect of the laser on the lung parenchyma is markedly reduced. This is logical, as less thermal energy per unit of time is lost to the lung parenchyma. At a constant operating speed, an increase of the laser energy leads to an increase in both the cutting and the coagulation effect. This effect can be further optimised by using a slower operating speed.
As a fact the depth of the coagulation zone is responsible for the air tightness of the lung parenchyma after laser resection.
Compared to our own studies, it was shown that—at a consistent energy level—the depth of the vaporization zone and of the coagulation zone is nearly twice as wide using the bare fiber with direct contact to the lung parenchyma compared to the focusing handpiece [
5].
Therefore as a conclusion for clinical practice our work indicates that it is possible to cut deeper into the lung parenchyma with the bare fiber without the need for suture.
This aspect has to be proven in an experimental setting with living animals, which we have planned to do in a further study. It is possible that both direct contact of the laser fiber with the lung parenchyma and the consistent mechanical forward feed of the fiber play a role. The strong effect of the laser fiber on the lung parenchyma is absolutely desirable when peripheral lung resections are to be performed. The amount of time needed to remove a lesion in the lung can be markedly reduced. However, if more central areas of the lungs are involved in which the density of larger vessels and bronchi increases, there is an increased risk of damaging these structures. This can lead to considerable local bleeding. Due to the scalpel-like character of the laser fiber, there is also the risk of small segmental bronchi being cut unnoticed. This would result in persistent air leakages from the lungs, which in the worst case would have to be closed in a separate surgical procedure. Our experience has shown that, whenever lasers are used in these parts of the lungs, the laser power should be markedly reduced to 20 W.
The use of laser fibers in our tests was unproblematic. There is generally the risk of tissue adhering to the tip of the fiber, which could lead to self-ignition and destruction thereof. In this case the laser fiber would have to be prepared again, which is time-consuming in practice. However, the bare fibers can be rapidly and easily used. The slightly thicker 600 µm fibers have become established in clinical practice, as they bend less during use. Our experimental data (albeit collected using pig lungs) demonstrate how effectively the laser fiber can be used in applications involving lung parenchyma. The latest-generation laser fibers even allow for use of very high laser energies, which significantly reduces the application time. No fiber problems occurred in any of the applications despite unusually high laser energies of 120 W.
As a trend towards open surgery to minimally invasive surgical procedures can be seen in thoracic surgery [
6,
7], laser fibers are extremely interesting, especially in minimally invasive surgeries [
8]. In these procedures, probe-like instruments are advanced into the thorax using trocars. The lung parenchyma can be cut (like with a scalpel) and coagulated using a thoracoscope for visual control [
9,
10]. For superficial defects, closure of the lung parenchyma by sutures is not required [
11]. In addition, adhesions of the lungs with the thoracic wall can be safely separated with the laser fiber. In contrast, the focusing handpiece is too short and too thick to be effectively used within the scope of minimally invasive surgical procedures. In the field of minimally invasive thoracic surgery, the future belongs to laser fibers thanks to their range of possible applications.
5. Conclusions
The 600 µm bare fiber exerts its maximum effect when in direct contact with the lung parenchyma at a laser power of 120 W and an operating speed of 5 mm/s. Both the depth of the cutting effect achieved and the width of the coagulation zone are greatest at these settings. These settings are suitable for applications involving peripheral lung segments. If the laser fiber is used in parts of the lungs close to the hilus, the laser power absolutely has to be considerably reduced in order to prevent unintended damage of important structures.




{kind=link}
{kind=link}
{kind=link}
{kind=link}