Healthcare Waste Management: A Case Study from Sudan



1
Faculty of Arts, Science and Technology, University of Northampton, Northampton NN2 7JD, UK
2
Department of Civil, Environmental, Architectural Engineering and Mathematics, University of Brescia, via Branze 43, 25123 Brescia, Italy
*
Author to whom correspondence should be addressed.
Environments 2018, 5(8), 89; https://doi.org/10.3390/environments5080089
Submission received: 2 July 2018
/
Revised: 23 July 2018
/
Accepted: 27 July 2018
/
Published: 5 August 2018
(This article belongs to the Special Issue Innovative Processes and Technologies for the Management of Hazardous Waste)
Abstract
:Healthcare waste (HCW) represents a major public health issue, especially in developing countries. Among HCW categories, sharps waste is one of the most hazardous. Exposure to needle-stick injuries can lead to blood-borne pathogens, therefore HCW should be managed in an effective manner. The main aims of this study were to assess the current management of used needles and to suggest suitable recommendations for an improved and safer system for needle management in Khartoum, Sudan. The study showed that the management of both healthcare and home-generated HCW in Sudan is inefficient, as all wastes are mixed together and disposed of improperly, especially used needles. The study attributes this to many reasons, including lack of waste segregation at the source, lack of policies, failure of planning, inadequate training, lack of awareness of the hazardous nature of such kinds of waste, weak infrastructure, and a lack of suitable treatment technologies. The estimated average generated rate of HCW ranged from 0.38 to 0.87 kg/bed/day in 2009 and 2012, respectively. Such ineffective healthcare waste management HCWM, especially used needles, can put public health as well as the environment at risk, particularly waste workers, thus urgent action needs to be taken by all involved parties and at all levels.
1. Introduction
According to the World Health Organization [1], about 16 billion injections worldwide are administered every year. Unfortunately, not all needles and syringes are disposed of safely, potentially creating risks of injury, infection and opportunities for reuse especially in low-income countries [2]. According to Health Care without Harm [3], sharps waste is a subset of infectious waste and includes syringes, needles, lancets, broken glass and any other materials that can pierce the skin. The combination of contamination with pathogens and the ability to break through the skin’s protection makes sharps waste one of the most dangerous wastes produced in healthcare facilities (HCFs). Therefore, among healthcare waste (HCW) types, contaminated sharps represent one of the most dangerous HCW subsets [3].
Sharps injuries can transmit more than twenty pathogens [4]. A person who is exposed to needle-stick injuries (NSIs) can be at risk of immediate consequences such as trauma and long-term consequences such as blood borne pathogens (BBPs). The most serious ones are hepatitis virus B (HBV), hepatitis virus C (HCV) and human immunodeficiency virus (HIV). In 2010, unsafe injections were documented to be responsible for considerable numbers of new infections of HIV, HBV and HCV, with 33,800, 1.7 million and 315,000, respectively [5].
HCW, including contaminated needles, has a catastrophic effect on human health and the environment when managed inefficiently [6,7,8,9]. Specifically, NSIs have health, economical, personal and negative social impacts on injured workers and their families [10,11]. For example, various studies have documented that injured healthcare personnel (HCP) can suffer from physical as well as psychological health effects such as anxiety and depression [12,13,14]. HCWM procedures are also associated with many occupational safety and health (OSH) and environment hazards and risks such as biological, physical, chemical, ergonomic, and psychological [15,16,17,18,19]. Indeed, HCWM is rated as one of the most hazardous jobs [20], since the nature of this kind of work exposes workers to health and safety risks, including NSIs, musculoskeletal disorders, and exposure to toxins, viruses and bacteria, and radioactive substances [20,21,22,23].
The unsafe management of sharps, including used needles, can be seen in different ways, such as incomplete incineration, and disposal in open pits or dumping sites [24]. Such practices can lead to the reuse of needles by other people and their presence in the general waste poses a high risk to waste workers [24]. On average, waste workers who handled reused needles can get 3–5 NSIs per day [3]. For example, among collectors of recyclables in Brazil, Marinho et al. [25] reported a rate of accidental NSIs of 47.3%. Indeed, incidences of infectious diseases such as hepatitis are often higher among HCP compared to non-HCP [26,27,28,29].
Approximately 80% of HCPs have been affected by NSIs [30]. Various authors attributed the vulnerability of HCPs to BBP from NSIs to various reasons, including:
- Low vaccination rates among HCPs, lack of taking occupational precaution measurements e.g., personal protective equipment (PPE) [32];
The unsafe management of HCW is common in many regions of the world, especially in low- and middle-income countries [35]. This necessitates an urgent assessment of the HCW of HCFs to implement locally-based solutions for better HCWM [36].
Understanding the local situation is very important, especially in resource-limited countries such as Sudan. Simple interventions such as introducing safe needle containers, training and adherence to the guidelines can prevent NSIs [37,38]. Furthermore, a significant reduction of HBV among American HCPs was documented after introducing routine HBV immunisation and establishing of comprehensive OSH policies [39]. Fortunately, more than 90% of NSIs can be prevented when certain occupational preventive measures are taken like the usage of safe needle devices, worker education and work practice controls [10,40].
The main aims of this study therefore were to assess the current management of used needles and to suggest suitable and cost-effective recommendations to improve the management of used needles in Sudan with a focus on Khartoum.
The key objectives were to:
- Examine how used needles are managed including handling, storage, transportation, treatment and disposal;
- Examine the possible factors (barriers and challenges, etc.), which led to the current used needles management situation;
- Suggest practical steps for an improved and safer system of needles’ management in Khartoum.
2. The Case Study
Sudan (North Sudan) consists of fifteen states, with about 40 million people, of whom 8 million live in Khartoum State [41]. According to the annual health statistical report 2015, Khartoum State contains 49 governmental hospitals, 106 private hospitals, and 585 primary healthcare centers [42].
The projection of the increasing size of the population and urbanisation will ultimately be accompanied by an increase in the waste generated [43,44,45].
The negotiations between the government and the Sudanese People’s Liberation Army (SPLA) led in 2005 to a comprehensive peace agreement (CPA). Based on the agreement, on 9 July 2011, Sudan was separated into two parts: North Sudan (which is now called Sudan), and South Sudan [46]. Sudan has faced many humanitarian crises, including: the Darfur crisis since 2003 [47], 2011 in South Kordofan’s Nuba Mountains region, and the Blue Nile [48].
According to the United Nations Development Programme [49], the Human Development Index of Sudan is 0.490 and it is ranked 165. Minoglou et al. [50] reported that HCW generation depends on socio-economic and environmental factors. Therefore, all these socio-demographic and geopolitical factors have had a negative impact on the healthcare system in general and HCWM in particular, in Sudan.
According to various authors (e.g., [51,52,53,54]), HCWM in Khartoum’s hospitals is inefficient, due to:
- Almost all types of wastes being mixed together;
- The partial separation of wastes existing only in a few hospitals;
- Most of the workers being illiterate or having very low education levels, and there being a shortage of personal protective equipment (PPE) (e.g., boots, aprons, gloves);
- At the hospital level, no policies or rules being found except in a few centers;
- Limited training and that which is provided being inefficient;
- In the majority of the hospitals (75%), the transportation of HCW to temporary storage areas being done manually;
- A colour-coding system often not being implemented.
In addition, waste management following immunisation in the Khartoum locality is poor. For example, 75% of the safety boxes are disposed of through open burning, the remaining 25% are disposed of with other waste. Only 18% of the staff use PPE [55].
Elduma and Saeed [34] found that among 245 HCPs in three hospitals in Khartoum, only 37 (15.1%) of them attended a bio-safety training course on how to deal with high risk materials. An evaluation of the standard of laboratory bio-safety measurements among 33 laboratories in Khartoum State indicated that there was no bio-safety officer appointed, no trained personnel, and in 12 laboratories (36.4%) the removal of hazardous material waste was not done daily [56].
Outside of Khartoum State, in Port Sudan, Elya and Babiker [57] found that there was no waste segregation, sharps and general waste were disposed of together in the same container, and sometimes used needles were being reused.
Regarding HCW legislation in Sudan, there is no direct legislation related to HCW [58]. Only a few laws focus on environmental conservation, such as the Interim National Constitution [59] and the Sudan Environmental Protection Act [60]. Sudan is committed to many international conventions, such as the Stockholm Convention, the Basel Convention on the Control of Trans-Boundary Movements of Hazardous Wastes and Their Disposal [15] and the Rotterdam Convention. These conventions in one a way or another have a link to HCWM (Higher Council for Environment and Natural Resources [61]). In addition, on 2 August 2017, Sudan ratified the Paris Agreement on climate change [62].
As there is no law to control HCW at federal level, Khartoum State developed a guide to set standards for the safe management of HCW [63]. This guide notes that sharps waste should be put in safety boxes, be well labelled and be marked as hazardous.
3. Materials and Methods
Three main methods were used in this study, namely: content analyses, observations and interviews. The study was undertaken between September 2016 and December 2017.
3.1. Content Analyses
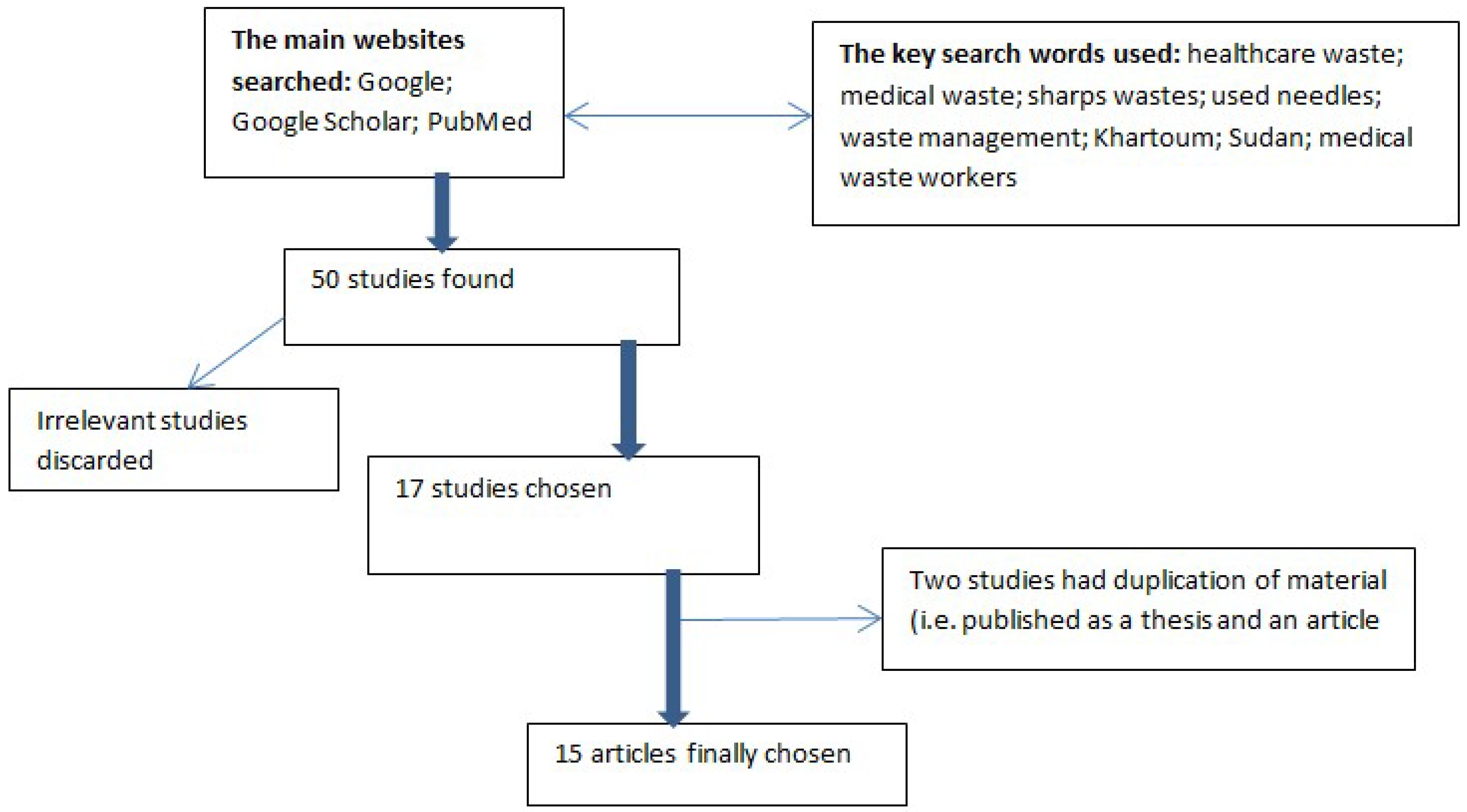
A comprehensive electronic search for the available published data was carried out. In addition, non-academic materials, for example, relevant Sudanese governmental documents were also searched. The following key search words were used: “healthcare waste”, “medical waste”, “sharps wastes”, “used needles”, “waste management”, “healthcare waste workers”, “Khartoum”, “Sudan”, using them interchangeably. Additionally, relevant references in the selected articles and article citation were traced to widen the searching scope. Any study focused on HCWM in Sudan was included in the study.
The full text and the abstract were analysed and the appropriate information (used needles management, the quantity of HCW, barriers and challenges) was extracted accordingly. In total, 15 articles were reviewed as well as some governmental documents (Figure 1).
The majority of studies were conducted in Khartoum State, apart from three studies, one of them in the Red Sea State and the remaining in the White Nile State. The search was focused on the most recently published articles from the last 10 years.
Local reports and unpublished data regarding used needles management were requested by the researcher from the authorities but there was no response. However, the websites of both the Sudan Federal Ministry of Health (SFMOH) and Khartoum State Ministry of Health (KSMOH) were searched and the available data on NSIs and the management of needles in Sudan were extracted and included in the study.
3.2. Direct Observations
The observations were carried by the authors from February 2017 to October 2017 in eight HCFs, from both the public and private sectors (five in urban areas and three in rural areas). The facilities were chosen based on accessibility. For each observation, verbal permission was obtained from the person in charge of the duty.
In addition, photos of good and bad HCW practices were taken. In each picture the practice was mentioned as well as its evaluation, i.e., good or bad based on the WHO standards [6].
The observations included the following issues regarding used needle management: where were the needles placed after use? What types of safety boxes were used, and what were they made of? What type of syringe was used (e.g. auto-retracted or other)? Where were the used needles stored, and how were they disposed of?
3.3. Interviews about Used Needles Management Issues with the HCP
Ten unstructured interviews were conducted with different HCP, such as doctors, nurses, HCPs) from both private and public HCFs. The selection process for the participants was based on their availability. The purposes of the interviews were explained to the participants and their verbal permission was obtained. All approached participants accepted the invitation.
The interviews tackled three main issues: how did they dispose of used needles? Why? And what suggestions they had to improve the current situation? In addition, three selected key phrases from HCP were mentioned. The names of the interviewees were not mentioned, only the job title was mentioned (e.g., nurse, HCP, etc.).
3.4. Data Collection and Analysis
From the content analyses, the following data were extracted:
- The published data were categorised according to the geographical area, i.e., state;
- The HCW production (kg/bed/day) was estimated;
- The main existing practices of managing used needles;
- Reporting of training, PPE, vaccination status and NSI issues;
- The key mentioned barriers and recommendations from the published research regarding used needles management in Sudan.
The interviewees’ responses were listed and similar text responses were categorised together.
Triangulation of different data sources (content analyses, observations and interviews) was carried out to develop practicable solutions for used needle management and to achieve the main goal of the study.
4. Results
4.1. Content Analyses
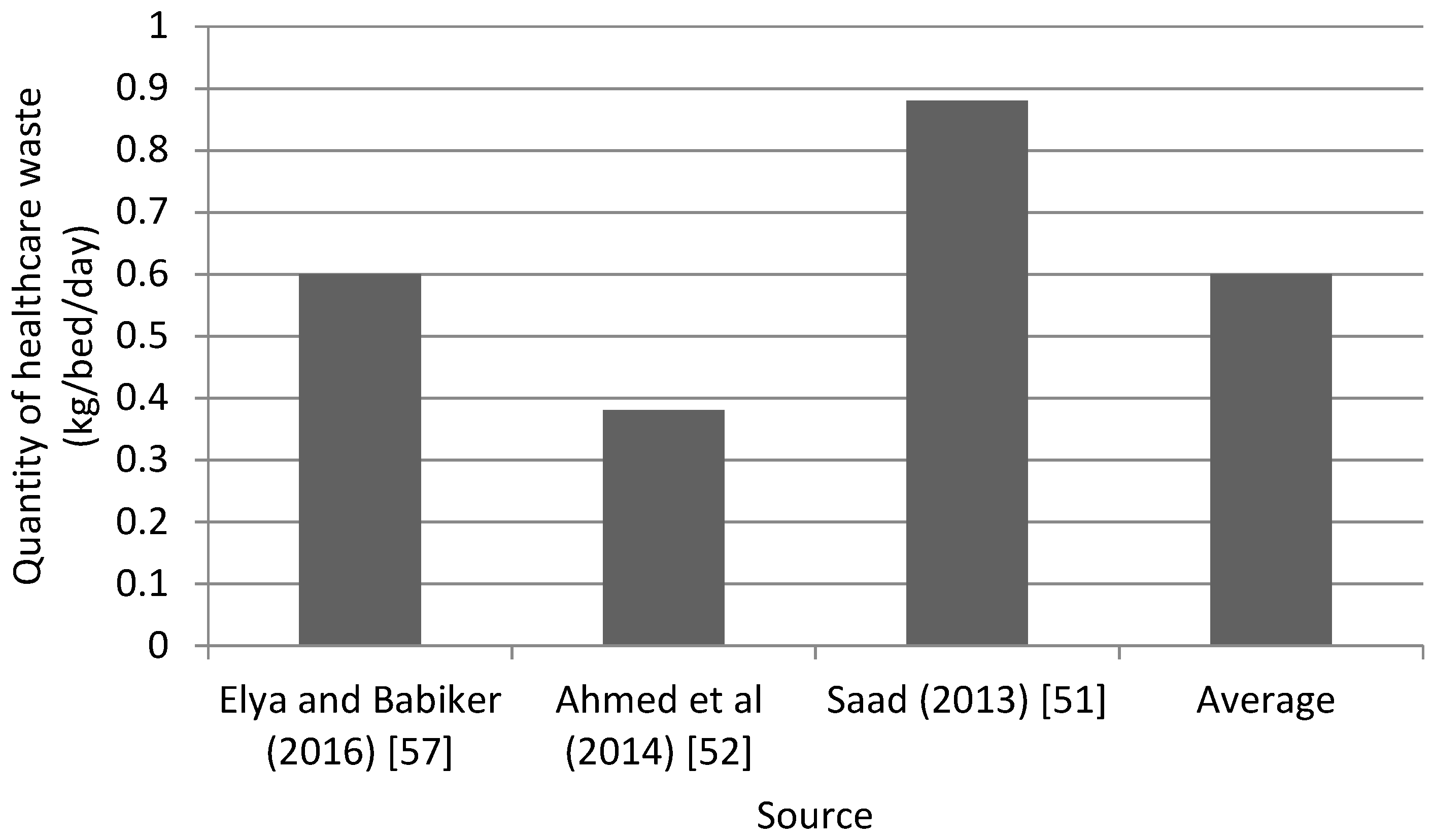
HCWM varied from one HCF to another, as well as the amount of the HCW (on average 0.6 kg/bed/day), as shown in Figure 2. It was found that the HCWM was inefficient, e.g., all wastes were mixed together, there was inadequate training, a lack of policies, a shortage or improper usage of PPE, high rates of NSIs and low vaccination rates among HCPs (Table 1).
4.1.1. NSIs Reported by SFMOH
According to the Sudan Health Observatory [70], the percentage of accidental NSIs among HCP from different governmental hospitals in Khartoum State were as follows: Khartoum North Teaching Hospitals (44%), Friendship Hospital (24%), Maternity Hospital (48%), Ibn Sina Hospital (34%) and Omdurman Hospital (39%).
According to the latest estimation, Khartoum State produced about three tons of HCW per day. The percentages of segregation of HCW were 95% and 63% in private and governmental HCFs [71]. Of this, 3% was treated as HCW. There are 22 healthcare incinerators. KSMOH stated that HCW should be burn in an incinerator with at least 1300 100 ºC temperature [70].
4.1.2. Current Used Needles Management in Sudan
It was stated in almost all the reviewed articles that sharps waste is mixed with domestic waste (e.g., [51,52,53,54]). The following outlines the key steps for used needles management in Sudan:
- Waste minimisation and segregation: there was no plan; irrational use of injections is common; lack of waste segregation.
- Waste handling: manual handling of HCW from the wards to the storage area, this increases the possibility of NSIs, especially as misuse of safety boxes is common; no or partial availability of PPE; partial segregation of waste; auto-retracted syringes are used in few of the observed hospitals.
- Storage: the storage area was not secure; there was a delay in disposing needles.
- Transportation: the vehicles (compactor, lorries, tipper, trailer) were not fulfilling the WHO standards [75]; lack of commitment to scheduling times.
- Treatment: no technologies such as autoclave or disinfection were used to treat used needles; no needle cutters; there is a possibility of the reuse of needles.
- Disposal: based on the review findings, many options are employed in Sudan to dispose of the used needles generated either in HCFs or in the home, as follows: (i) placed in a safety box or locally made sharps container (plastic bottle) and disposed of through burning in an incinerator, or buried; (ii) mixed with other HCW and disposed through a landfill site, or by burning; (iii) mixed with healthcare domestic waste and disposed of through an open dumpsite, burnt in the open environment, or a landfill site; (iv) disposed on the ground.
4.1.3. HCWM in the Rural HCFs
In the rural areas in Sudan the situation is not different from the cities, as found by Ahmed et al. [52] and Abd Elgadir [55]. Their results revealed that in the rural areas the commonly used methods for used needle management were open burning, burying without burning and encapsulation. The main reasons led to improper HCWM in the rural areas including:
- Lack of water and sanitation;
- No electricity for operations such as autoclave, steam sterilisation and incineration;
- Lack of transportation, especially in the rainy season;
- Lack of the awareness among doctors and nurses, etc.
4.2. Observations
During the observations, attention was paid to the safety boxes and their usage, as the containment of the needles and sharps was a key area of focus for the study.
4.2.1. Safety Box Usage
A shortage of safety boxes was observed in both rural and urban HCFs. Locally made safety boxes from empty plastic bottles were observed in two HCFs in rural areas. Manual handling of HCW was observed, which may lead to injuries, musculoskeletal disorders, etc. In addition, the practice of recapping needles was observed among some HCP.
4.2.2. Observation of HCWM Practices
Improper HCWM was observed at one HCF in Khartoum. During the observation, no segregation of wastes and used needles was seen. Moreover, needles were found on the floor in some hospitals and clinics in both cities and rural areas. Some HCPs were observed using latex gloves instead of heavy-duty gloves. No posters or policy regarding used needle management were found in the observed HCFs.
However, good practice was observed in some HCFs (i.e., the safety box was not overfilled, and the area was clean). The wastes should be categorised as domestic waste, biological waste and sharps wastes, as well as being well-labelled.
4.3. Interviews
Some 80% of the interviewees agreed that used needle management represents a real problem in their HCFs.
For example, a doctor said, “Waste workers are not aware about the dangerous of NSIs and this is our responsibility to take action.” Similarly, a nurse stated that, “I think, first we need to be well informed about HCWM and then we can conduct a campaign to raise the awareness about the hazards of sharps wastes.” A HCP stated that, “We are committed to our job but the non-compliance often comes from HCP as there is no segregation of wastes at source i.e., in different categories such as domestic waste and HCW e.g., sharps and non-sharps wastes.”
The interviewees attributed the practice of mixing of all types of waste together to many reasons:
- Lack of awareness regarding the danger and the long-term consequences (hepatitis and HIV) of such practices among HCP, especially those who are in direct contact with waste, such as waste workers
- No enforced policy in place, such as colour coding and labelling for waste disposal
- Lack of resources, i.e., shortage of safety boxes and insufficient budget for HCWM
- No dedicated department to deal with HCWM, i.e., that can monitor, evaluate and take appropriate actions accordingly
- Lack of training, especially among waste workers.
According to the interviewees the key reasons for limited training included:
- Limited budgets for training purposes, in addition to the inefficient management of the allocated budget
- The decisions makers are perhaps not aware of the cost effectiveness of training i.e., through training, the segregation and recycling of waste will increase
- Lack of HCWM experts.
5. Discussion
The results show that HCWM in Sudan needs to be improved, especially for used needles. All healthcare and domestic wastes were mixed together, there was no available enforced law, low vaccination rates among the HCP, PPE was unavailable or partially used, staff training was inadequate, and high rates of NSIs were reported, especially among waste workers. Similar results in terms of poor HCWM have been reported by previous studies in many African countries [76,77,78,79]. Such poor HCWM will result in serious health effects to the population and also has negative impacts on the environment [6,52]. The high rates of NSIs that were documented by the SFMOH, which in some hospitals reached up to 48% among HCPs, should raise alarm. This may be attributed to the poor working conditions and the limited precautions taken [30,31,32,34]. Although the possibilities of NSIs are high, there was no policy for injured workers. For example, the American Nurses Association [80] and the National Institute for Occupational Safety and Health (NIOSH) in the USA [81] provide some recommendations for emergency responses after NSIs, such as providing care to the wound and seeking medical help immediately. However, more labelling and categorisation of waste are needed in comparison to other countries, such as Gulf countries [82].
Although vaccination is cost effective, and the job exposed the workers to injuries, they were not vaccinated, especially against HBV. In Sudan, vaccination coverage among HCP is very low in comparison to other countries. For example, HBV vaccination rates were 4% and 82% in Eastern Sudan and the Lazio region of Italy, respectively [57,83]. Elmukashfi [84] revealed that although HBV vaccination was provided for HCP such as doctors, nurses, and laboratory technicians, none of the cleaning staff was vaccinated. Cleaning staff knew very little about hepatitis, had low vaccination rates, a low level of education or were not educated at all and none of them had been screened before. Moreover, the lack of PPE and the manual handling of HCW placed them at a higher risk of acquiring infections such as HIV and hepatitis [54,55,84]. From the above-mentioned studies, it is evident that the vaccination status (completeness and coverage) was affected by the occupational category, probably reflecting wide variations in knowledge regarding HBV infection and vaccination. Therefore, a lack of a clear policy regarding HCP vaccination is lacking in the studied HCFs. The situation needs an urgent action plan to be taken as soon as possible to ensure the safety of all employees.
Training and pre-employment examinations were not carried out for the workers and this is against the Sudan labor law [85]. The law states that workers should receive appropriate training and should not be exposed to danger. More research is needed to understand the types of work contracts, i.e., daily worker, temporary, or permanent employees. The health surveillance of workers before commencing employment is a good opportunity to check their fitness and to provide appropriate vaccinations if needed [86,87].
The key concern that was raised was the management of home-generated HCW, which was found to be mixed with the general domestic waste. Therefore, domestic waste workers are commonly at risk from the mixed waste.
By mixing HCW with municipality waste, the entire waste will become infectious and valuable resources will be lost. It is difficult to obtain a benefit from the general waste through processes such as reuse, recycling and recovery [88,89]. However, although the mixing of the waste types and limited training were mentioned in previous studies, there were no explanations provided, as in this study.
The maximum range of the average waste generation rate (0.87 kg/bed/day) [51] was lower in compared to Bangladesh (1.54 kg/bed/day) [90] and Mauritius (2 kg/bed/day) [17].
This is in contrast to the amount generated in developed countries, which a study estimated to be 0.5 kg/bed/day [24]. The variation may be due the lack of waste segregation in developing countries such as Sudan, which makes the total amount higher. Nevertheless, any unseparated waste from HCFs should be treated as hazardous. In addition, the terminology of HCW is interpreted differently and HCW depends on socio-economic and environmental factors, which vary among countries [50,91,92]. For example, CO2 emissions, life expectancy, and the Human Development Index (HDI) were found to be positively correlated with HCW generation [50]. A difference in terminologies for HCW was also observed in reviewed studies.
Most of the barriers (lack of training, low awareness, financial constraints, lack of or ineffective legislation) which led to improper HCWM have been documented in previous studies [91]. Interventional programmes based on education were found to work well in similar contexts [69,93]. For example, HCP at the main hospitals of the White Nile State in Sudan recorded a significant improvement in their knowledge and practice with regard to HCWM immediately after an educational intervention programme [69]. In addition, needles may contain toxic or radioactive substances. In such cases, more precautions should be taken when disposing of them [23]. A recent assessment of radioactive waste in two hospitals in Khartoum State showed no waste segregation, as all wastes (gloves, syringe, vials, etc.) were mixed together in a bag, as well as unsafe storage and a delay in disposal [94]. To ensure the safe disposal of such wastes, other parties, e.g., the Sudan Atomic Energy Agency, should be involved. Surprisingly, even the medical professional staff misused the safety box and dispensing of medicines [42].
Based on the analysis of current situation and the triangulation of the collected information from the review, observations and the interviews regarding used needle management in Khartoum, Sudan, the study came up with the following recommendations:
- Short-term recommendations:
- Workshops for the involved parties such as the Ministry of Health, hospital administrations, public health personnel, HCW disposal companies, physicians, nurses, researchers, pharmacists, diabetes organisations and societies, diabetes educators, etc. The materials for the workshop should be organised with the involvement of all parties
- Patients’ educational sessions about the safe disposal of sharps, especially at home
- Provision to patients of safe disposal tools, such as a safety box and a community drop safety box, this can be organised with pharmaceutical companies and non-governmental organisation (NGOs)
- Community involvement through the launching of campaigns for safe sharps disposal (posters, brochures, media sessions, etc.). Public awareness about the hazards and risks of HCW is a key of success [95]
- Knowing the main stakeholders and their influence regarding waste management
- Rapid assessment of HCW among the HCFs, including the availability of an incinerator for each HCF. For this purpose, the WHO Individualised Rapid Assessment Tool (I-RAT) can be used [96].
- Medium-term recommendations:
- Encourage the use of the available HCWM technologies
- Training and periodic updating of the staff on different aspects related to safe HCWM, such as OSH, rational usage of medicines and operation of sharps pits and incinerators. Meanwhile, the ten proposed recommendations by Laing et al. [98] to improve rational medicine usage in developing countries can be adopted in the Sudan context. Provision of training was found to be effective in reducing the rate and underreporting of NSIs [99]
- Allocation of enough resources such as budget, safety boxes, personnel, and vehicles for HCWM and PPE. However, PPE should be used as the last option of protection in the hierarchy of hazard controls [100]. The strategy for HCW should focus on the most effective control measures e.g., minimisation of needle usage, use of engineering (e.g., auto-retracting syringes, safety boxes, etc.), and administrative (e.g., setting of policies, training, etc.) [101]
- Conducting audits for HCWM
- Documentation should be encouraged to identify the amount of waste and to trace the waste from the generating facility to the end of disposal. In addition, record keeping should be introduced at all HCF levels
- Establishment of sharps pits or incinerators according to the needs based on the results of the initial survey.
- Long-term recommendations:
- Development and effective implementation of HCWM legislation
- An environmental impact assessment should be implemented for all HCFs and should be mandatory before establishing any new facility
- Alternative technologies can be used. However, before selecting any technology, basic information should be available: (a) the size of the target facility, whether it is small, medium, large, or at the national level; (b) the estimated amount of waste generated; and (c) the cost of the needed technology.
6. Conclusions
Based on the available literature, observations and the interviews with HCP, used needle management is inefficient in Khartoum, Sudan.
Such poor management of HCW can pose negative impacts (e.g., injuries, BBP, etc.) on patients and the community, as well as the environment (pollution of soil, air and water). The situation necessitates that urgent action be taken by all involved parties, such as HCF staff, decision-making staff, and at all levels of state and federal governments. Policies and initiatives should be implemented to improve HCWM:
- Policies regarding the safe handling and disposal of sharps, vaccination, OSH, reporting of NSIs, PEP, and colour coding and labelling for waste disposal;
- Initiatives to raise awareness of safe sharps disposal among HCP and the public through education, training and the launching of campaigns, i.e., posters, brochures, media sessions, etc.
In addition, the recommendations proposed above can be implemented to improve the current situation. The proposed policies, initiatives and recommendations can be applied at Khartoum sites (hospitals, clinics, etc.) and can be duplicated in others states and even Sudan generally.
The observations included the following regarding used needle management: where needles are put after use; the type of safety boxes, their use, and what are they made of; the type of syringe used (auto-retractable or not); where they store used needles; and how they dispose of them.
Author Contributions
Conceptualization, A.A.H.; Methodology, A.A.H., T.T. and M.V.; Validation, A.A.H., T.T. and M.V.; Formal Analysis, A.A.H., T.T. and M.V.; Investigation, A.A.H.; Resources, A.A.H.; Data Curation, A.A.H., T.T. and M.V.; Writing—Original Draft Preparation, A.A.H.; Writing—Review and Editing, A.A.H., T.T. and M.V.; Supervision, T.T. and M.V.; Project Administration, A.A.H.
Funding
This research received no external funding.
Acknowledgments
The authors would like to thank the hospitals and staff for consenting to and participating in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO. Injection Safety. 2012. Available online: http://www.wpro.who.int/mediacentre/factsheets/fs_20120204/en/ (accessed on 18 December 2017).
- Caniato, M.; Tudor, T.L.; Vaccari, M. Assessment of health-care waste management in a humanitarian crisis: A case study of the Gaza Strip. Waste Manage. 2016, 58, 386–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Care without Harm. Treating Sharps Waste. 2017. Available online: https://noharm-global.org/issues/global/treating-sharps-waste (accessed on 23 July 2017).
- CDC. Sharps Safety for Healthcare Settings. 2015. Available online: https://www.cdc.gov/sharpssafety/ (accessed on 30 July 2017).
- Pepin, J.; Abou Chakra, C.N.; Pépin, E.; Nault, V.; Valiquette, L. Evolution of the global burden of viral infections from unsafe medical injections, 2000-2010. PLoS ONE 2014, 9, e99677. [Google Scholar] [CrossRef] [PubMed]
- Chartier, Y.; Emmanuel, J.; Pieper, U.; Annette, P.; Rushbrook, P.; Stringer, S.; Townend, W.; Stringer, W.; Zghondi, R. Safe Management of Wastes from Health-Care Activities, 2nd ed.; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Ahmed, A.A; Awooda, E.M.; Elbeshir, E.I. Dentists knowledge, attitude and practice towards dental waste management in private clinics-Khartoum locality. Int. J. Latest Res. Sci. Technol. 2014, 3, 93–96. [Google Scholar]
- Caniato, M.; Tudor, T.; Vaccari, M. International governance structures for health-care waste management: A systematic review of scientific literature. J. Environ. Manage. 2015, 153, 93–107. [Google Scholar] [CrossRef] [PubMed]
- Vaccari, M.; Tudor, T.; Perteghella, A. Costs associated with the management of waste from healthcare facilities: An analysis at national and site level. Waste Manage. Res. 2018, 36, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Waljee, J.F.; Malay, S.; Chung, K.C. Sharps Injuries: The Risks and Relevance to Plastic Surgeons. Plast. Reconstr. Surg. 2013, 131, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Lavoie, M.C.; Verbeek, J.H.; Pahwa, M. Devices for preventing percutaneous exposure injuries caused by needles in healthcare personnel. Cochrane Db. Syst. Rev. 2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDowell, C.L. First Hand: The Surgeon and Hepatitis, C. J. Hand Surg. 2012, 37, 1693–1694. [Google Scholar] [CrossRef]
- Adib-Hajbaghery, M.; Lotfi, M.S. Behavior of Healthcare Workers after Injuries from Sharp Instruments. Trauma Mon. 2013, 18, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Naghavi, S.H.R.; Shabestari, O.; Alcolado, J. Post-traumatic stress disorder in trainee doctors with previous needlestick injuries. Occup. Med. 2013, 63, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Basel Convention. Basel Convention on the Control of Transboundary Movements of Hazardous Wastes and Their Disposal. 2011. Available online: http://www.basel.int/portals/4/basel%20convention/docs/text/baselconventiontext-e.pdf (accessed on 2 November 2016).
- Ream, P.S.; Tipple, A.F.; Barros, D.X.; Souza, A.C.; Pereira, M.S. Biological risk among hospital housekeepers. J. Arch. Environ. Occup. Health. 2014, 71, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Bokhoree, C.; Beeharry, Y.; Makoondlall-Chadee, T.; Doobah, T.; Soomary, N. Assessment of environmental and health risks associated with the management of medical waste in Mauritius. Apcbee Procedia. 2014, 9, 36–41. [Google Scholar] [CrossRef]
- Ndejjo, R.; Musinguzi, G.; Yu, X.; Buregyeya, E.; Musoke, D.; Wang, J.S.; Halage, A.A.; Whalen, C.; Bazeyo, W.; Williams, P.; et al. Occupational health hazards among healthcare workers in Kampala, Uganda. Inter. J. Env. Res. Pub. Heal. 2015. [Google Scholar] [CrossRef]
- Vaccari, M.; Perteghella, A.; Stolfini, M.; Tudor, T. Overcoming public health risks to staff during the management of waste from healthcare facilities: Case studies from Italy. Int. J. Technol. Health. Care Qual. Assess. 2018, 31. [Google Scholar] [CrossRef] [PubMed]
- Tibbetts, J. Garbage collection is one of the most hazardous jobs. Can. Med. Assoc. J. 2013, 185, 284. [Google Scholar] [CrossRef] [PubMed]
- Sefouhi, L.; Kalla, M.; Bahmed, L.; Aouragh, L. The risk assessment for the healthcare waste in the hospital of Batna city. Algeria. Inter. J. Env. Sci. Develop. 2013, 4, 442–445. [Google Scholar] [CrossRef]
- Alwabr, G.M.; Al-Mikhlafi, A.S.; Al-Hakimi, S.A.; Dughish, M.A. Risk assessment of the current handling of medical waste in hospitals of Sana’a city Yemen. Inter. J. Sci. Technol. 2017, 3, 1–9. [Google Scholar] [CrossRef]
- Biodex. Sharps Container Shields. 2017. Available online: http://m.biodex.com/nuclear-medicine/products/syringe-vial-shields/sharps-container-shields (accessed on 6 August 2017).
- WHO. WHO Guideline on the Use of Safety-Engineered Syringes for Intramuscular, Intradermal and Subcutaneous Injections in Health-Care Settings. 2015. Available online: http://apps.who.int/iris/bitstream/10665/170470/1/WHO_HIS_SDS_2015.5_eng.pdf shields (accessed on 29 July 2017).
- Marinho, T.A.; Lopes, C.L.R.; Teles, S.A.; Reis, N.R.S.; Carneiro, M.A.D.S.; Andrade, A.A.D.; Martins, R.M.B. Prevalence of hepatitis C virus infection among recyclable waste collectors in Central-West Brazil. Mem. Inst. Oswaldo Cruz. 2013, 108, 519–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majeed, A.; Batool, S.A.; Chaudhry, M.N.; Siddique, R.A. Scavenging demeanor in Bahawalpur, Pakistan: Social and health perspective. J. Mater. Cycles Waste Manag. 2017, 19, 815–826. [Google Scholar] [CrossRef]
- Alemayehu, T.; Worku, A.; Assefa, N. Medical Waste Collectors in Eastern Ethiopia are Exposed to High Sharp Injury and Blood and Body Fluids Contamination. J. Prev. Infect. Control. 2016, 2, 1–10. [Google Scholar] [CrossRef]
- Mol, M.P.; Gonçalves, J.P.; Silva, E.A.; Scarponi, C.F.; Greco, D.B.; Cairncross, S.; Heller, L. Seroprevalence of hepatitis B and C among domestic and healthcare waste handlers in Belo Horizonte, Brazil. Waste Manage. Res. 2016, 34, 875–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadesse, M.; Tadesse, T. Epidemiology of needle stick injuries among health-care workers in Awassa City, Southern Ethiopia. Trop. Doct. 2010, 40, 111–113. [Google Scholar] [CrossRef] [PubMed]
- Elseviers, M.M.; Arias-Guillén, M.; Gorke, A.; Arens, H.J. Sharps injuries amongst healthcare workers: Review of incidence, transmissions and costs. J. Ren Care. 2014, 40, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Himmelreich, H.; Rabenau, H.F.; Rindermann, M.; Stephan, C.; Bickel, M.; Marzi, I.; Wicker, S. The Management of Needle stick Injuries. Dtsch. Ärzteblatt Int. 2013, 110, 61–67. [Google Scholar]
- Westermann, C.; Peters, C.; Lisiak, B.; Lamberti, M.; Nienhaus, A. The prevalence of hepatitis C among healthcare workers: A systematic review and meta-analysis. Occup. Environ. Med. 2015, 72, 880–888. [Google Scholar] [CrossRef] [PubMed]
- Nail, A.; Eltiganni, S.; Imam, A. Seroprevalence of Hepatitis B and C among health care workers in Omdurman, Sudan. Sudan J. Med. Sci. 2008, 3, 201–206. [Google Scholar] [CrossRef]
- Elduma, A.H.; Saeed, N.S. Hepatitis B virus infection among staff in three hospitals in Khartoum, Sudan, 2006–07. East Mediterr Health J. 2011, 17, 474–478. [Google Scholar] [CrossRef]
- WHO. Health-Care Waste Fact Sheet N.°253. 2016. Available online: http://www.who.int/mediacentre/factsheets/fs253/en/ (accessed on 31 October 2016).
- Di Bella, V.; Ali, M.; Vaccari, M. Constraints to healthcare waste treatment in low-income countries-A case study from Somaliland. Waste Manage. Res. 2012, 30, 572–575. [Google Scholar] [CrossRef] [PubMed]
- Hanafi, M.I.; Mohamed, A.M.; Kassem, M.S.; Shawki, M. Needlestick injuries among health care workers of University of Alexandria Hospitals. East Mediterr Health J. 2011, 17, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Afridi, A.A.K.; Kumar, A.; Sayani, R. Needle stick injuries–risk and preventive factors: A study among health care workers in tertiary care hospitals in Pakistan. Glob. J. Health Sci. 2013, 5, 85–92. [Google Scholar] [CrossRef] [PubMed]
- MacCannell, T.; Laramie, A.K.; Gomaa, A.; Perz, J.F. Occupational exposure of health care personnel to hepatitis B and hepatitis C: Prevention and surveillance strategies. Clin. Liver. Dis. 2010, 14, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Centre for Disease Control (CDC). Evaluation of Safety Devices for Preventing Percutaneous Injuries among Healthcare Workers during Phlebotomy Procedures-Minneapolis-St. Paul, New York City, and San Francisco. Morb. Mortal Wkly. Rep. 1997, 46, 21–23. [Google Scholar]
- Sudan Central Bureau of Statistics. Censuses. 2017. Available online: http://www.cbs.gov.sd/en/files.php?id=7#&panel1-2 (accessed on 28 July 2017).
- SFMOH. Annual Health Statistical Report, 2015. 2016. Available online: http://www.fmoh.gov.sd/yearlyReports/Annual2015.pdf (accessed on 6 December 2017).
- Pai, R.; Rodrigues, L.L.; Mathew, A.O.; Hebbar, S. Impact of urbanization on municipal solid waste management: A system dynamics approach. Int. J. Renew. Energy Environ. Eng. 2014, 2, 31–37. [Google Scholar]
- Dahiya, R. Projections for the population growth and its impact on solid waste generation of medium sized north Indian city. Int. J. Tech. Res. Appl. 2015, 3, 57–61. [Google Scholar]
- Das, S.; Bhattacharyya, B.K. Estimation of municipal solid waste generation and future trends in greater metropolitan regions of Kolkata, India. J. Ind. Eng. Manag. Innovat. 2014, 1, 31–38. [Google Scholar] [CrossRef]
- UN. Independence of South Sudan. 2011. Available online: http://www.un.org/en/peacekeeping/missions/past/unmis/referendum.shtml (accessed on 18 February 2016).
- Udombana, N.J. When neutrality is a sin: The Darfur crisis and the crisis of humanitarian intervention in Sudan. Hum. Rights Q. 2005, 27, 1149–1199. [Google Scholar] [CrossRef]
- Gramizzi, C.; Tubiana, J. New War, Old Enemies: Conflict Dynamics in South Kordofan; The Small Arms Project: Geneva, Switzerland, 2013. [Google Scholar]
- UNDP. Sudan. Human Development Indicators. 2016. Available online: http://hdr.undp.org/en/countries/profiles/SDN (accessed on 29 July 2017).
- Minoglou, M.; Gerassimidou, S.; Komilis, D. Healthcare Waste Generation Worldwide and Its Dependence on Socio-Economic and Environmental Factors. Sustainability 2017, 9, 220. [Google Scholar] [CrossRef]
- Saad, S.A. Management of Hospitals Solid Waste in Khartoum State. Environ. Monit. Assess. 2013, 185, 8567–8582. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.O.; Gasmelseed, G.A.; Musa, A.E. Assessment of Medical Solid Waste Management in Khartoum State Hospitals. Jpn. J. Ind. Appl. Math. 2014, 2, 201–205. [Google Scholar]
- Idris, MGM. Medical Waste Management in Some Hospitals in Sudan. University of Khartoum, 2016. Available online: http://khartoumspace.uofk.edu/handle/123456789/20910 (accessed on 6 September 2016).
- Eltayeb, E.; Magdah, E.; Abdelelah, M.; Mohamed, E.; Khouya, K.; Benkaddour, R. Knowledge, Attitude and Practice towards Collection and Disposal of Medical Waste among Medical Waste Workers in Khartoum State Hospitals, Sudan (2013–2016). Appl. J. Environ. Eng. Sci. 2017, 3, 268–279. [Google Scholar]
- Abd Elgadir, A. Assessment of Medical Immunization Waste Management in Khartoum (Doctoral Dissertation, UOFK). Available online: http://khartoumspace.uofk.edu/handle/123456789/7628 (accessed on 13 August 2017).
- Fath, E.I.A.; Magdi, B. Evaluation of Laboratory Biosafety in Khartoum State Primary Health Care Centers, Sudan. Med. Saf. Global Health. 2016, 5, 126. [Google Scholar]
- Elya, T.B.; Babiker, A.B. Assessment of Medical Waste Management in Port Sudan Teaching Hospital, Sudan. Int. J. Sci. Res. 2016, 5, 586–589. [Google Scholar]
- Tairab, M.A.O. Knowledge, Attitudes and Practices towards Medical Waste Hazards among Health Cleaners at Bahari and Sharq Al-Neel Hospitals. Master’s Thesis, University of Khartoum, Khartoum, Sudan, June 2009. [Google Scholar]
- The Interim National Constitution of the Republic of the Sudan. 2005. Available online: http://www.refworld.org/pdfid/4ba749762.pdf (accessed on 9 November 2016).
- Environmental Protection Act 2001. Sudan Parliament. Available online: http://www.parliament.gov.sd/ar/index.php/site/LigsualtionVeiw/210 (accessed on 24 December 2014).
- Higher Council for Environment and Natural Resources. National Implementation Plan for the Stockholm Covention on POPs. 2007. Available online: http://www.pops.int/documents/implementation/nips/submissions/NIP_Sudan.pdf (accessed on 9 November 2016).
- UNEP. Sudan Ratifies Paris Climate Agreement. 2017. Available online: http://www.unep.org/disastersandconflicts/news/sudan-ratifies-paris-climate-agreement (accessed on 10 August 2017).
- KSMOH. Guideline to the Safe Disposal of Medical Waste. 2012. Available online: http://ksmoh.gov.sd/dpre.pdf (accessed on 25 July 2017).
- Abdalgadir, M.A.; Osman, F.F.A.; Bushara, M.O.E.; Alawneh, S.M.A. 2016. Knowledge Attitude and Practice of the Workers towards Health Care Waste Safety Measures in Khartoum State Governmental Hospitals. Eur. J. Pharm. Med. Res. 2015, 3, 580–584. [Google Scholar]
- Hassan, E.M.A.; Bashir, N.F. Evaluation of Medical Waste Treatment in Sudanese Hospitals. Inter. J. Env. Res. Eng. Sci. 2016, 4, 49–54. [Google Scholar]
- Yousif, M.; Elfadil, H.; Eldalo, A.; Nasr. Sudanese patients’ perception on injections. Saudi J. Health Sci. 2012, 1, 99–102. [Google Scholar] [CrossRef]
- Osman, O.B.; Osman, F.F.A.; Mohamed, M.H.; Ahmed, H.R.M. Effect of health awareness interventions on knowledge, attitudes and practices of health providers and workers involve in health care waste aspects at Khartoum North Teaching hospital. Eur. J. Pharm. Med. Res. 2015, 2, 124–132. [Google Scholar]
- Elhassan, R.M.; Ibrahim, M.A. The Effect of Handling of Laboratory Wastes on Liver Function Tests among Handlers in National Laboratory for Public Health in Khartoum State. Eur. Acad. Res. 2016, 4, 1060–1069. [Google Scholar]
- Elnour, A.M.; Moussa, M.M.R.; El-Borgy, M.D.; Fadelella, N.E.; Mahmoud, A.H. Impacts of health education on knowledge and practice of hospital staff with regard to Healthcare waste management at White Nile State main hospitals, Sudan. Int. J. Health Sci. 2015, 9, 315–331. [Google Scholar]
- SHO. Environmental Health, Category Guidelines/SOPs. 2017. Available online: http://sho.gov.sd/controller/knowledge_hub.php?mid=110&sm_id=&lid=1# (accessed on 20 August 2017).
- Alsudanalyoum. Healthcare Waste Incinerators in Khartoum State and Hepatitis. 2017. Available online: http://alsudanalyoum.com/2017/07/30/page/3/ (accessed on 8 November 2017).
- Alnilin. Healthcare Waste on the Road. 2013. Available online: http://www.alnilin.com/689461.htm (accessed on 29 September 2017).
- Sudaress. Healthcare Waste, Information and Facts. 2013. Available online: https://www.sudaress.com/rayaam/308497 (accessed on 15 October 2017).
- Seedbed. Hospital Waste. 2017. Available online: http://seedbed.nl/hospital-waste.html (accessed on 20 November 2017).
- WHO. Technologies. 2017. Available online: https://www.healthcare-waste.org/resources/technologies/ (accessed on 2 August 2017).
- Mansab, M.R. Sharp waste management at Kidongo Chekundu National Mental Hospital Zanzibar Tanzania”. Master’s Thesis, The Open University of Tanzania, Salaam, Tanzania, September 2014. Available online: http://repository.out.ac.tz/605/1/MANSAB_MANSAB_RAMADHAN_-DISSERTATION.pdf (assessed on 10 August 2017).
- Abeje, G.; Azage, M. Hepatitis B vaccine knowledge and vaccination status among health care workers of Bahir Dar City Administration, Northwest Ethiopia: A cross sectional study. BMC Infect. Dis. 2015, 15, 30. [Google Scholar] [CrossRef] [PubMed]
- Udofia, E.A.; Fobil, J.N.; Gulis, G. Solid medical waste management in Africa. Afr. J. Environ. Sci. Technol. 2015, 9, 244–254. [Google Scholar]
- Udofia, E.A.; Gulis, G.; Fobil, J. Solid medical waste: A cross sectional study of household disposal practices and reported harm in Southern Ghana. BMC Public Health 2017, 17, 464. [Google Scholar] [CrossRef] [PubMed]
- ANA. 7 Things to Do in Response to Needle Stick Injury. 2010. Available online: http://www.nursingworld.org/DocumentVault/OccupationalEnvironment/Needles/7-Responses.pdf (accessed on 22 August 2017).
- NIOSH. Emergency Sharps Information. 2016. Available online: https://www.cdc.gov/niosh/topics/bbp/emergnedl.html (accessed on 17 August 2017).
- Health Authority of Abu Dhabi. Medical Waste Management in Health Care Facilities. 2009. Available online: https://www.haad.ae/haad/Portals/0/Policies_Docs/Policy%20on%20Medical%20Waste%20Mangement%20in%20the%20HCFs.pdf (accessed on 14 November 2017).
- La Torre, G.; Scalingi, S.; Garruto, V.; Siclari, M.; Chiarini, M.; Mannocci, A. Knowledge, Attitude and Behaviours towards Recommended Vaccinations among Healthcare Workers. Healthcare (Basel) 2017, 5, E13. [Google Scholar] [CrossRef] [PubMed]
- Elmukashfi, T. Sero-Epidemiological Survey of Hepatitis B Markers among Health Care Workers in Public Hospitals in Khartoum State in the Year 2004. Ph.D. Thesis, University of Khartoum, Khartoum, Sudan, July 2015. [Google Scholar]
- Sudan Labor Law. 1997. Available online: http://www.ilo.org/dyn/natlex/docs/WEBTEXT/49122/65103/E97SDN01.htm (accessed on 1 August 2017).
- Amsalu, A.; Worku, M.; Tadesse, E.; Shimelis, T. The exposure rate to hepatitis B and C viruses among medical waste handlers in three government hospitals, southern Ethiopia. Epidemiol. Health 2016, 38, 1–8. [Google Scholar] [CrossRef]
- CDC. Recommended Vaccines for Healthcare Workers. 2017. Available online: https://www.cdc.gov/vaccines/adults/rec-vac/hcw.html (accessed on 21 August 2017).
- Tudor, T.L.; Noonan, C.L.; Jenkin, L.E.T. Healthcare waste management: A case study from the National Health Service in Cornwall, United Kingdom. Waste Manag. 2005, 25, 606–615. [Google Scholar] [CrossRef] [PubMed]
- Lavee, D. Is municipal solid waste recycling economically efficient? Environ. Manage. 2007, 40, 926–943. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.Z.; Islam, M.S.; Islam, M.R. Medical Waste Management: A Case Study on Rajshahi City Corporation in Bangladesh. J Environ Sci Nat. Resour. 2015, 6, 173–178. [Google Scholar] [CrossRef]
- Hossain, M.S.; Santhanam, A.; Norulaini, N.N.; Omar, A.M. Clinical solid waste management practices and its impact on human health and environment–A review. Waste Manage. 2011, 31, 754–766. [Google Scholar] [CrossRef] [PubMed]
- Shannon, A.L.; Woolridge, A. Medical Waste. In Waste; Michigan Department of Natural Resources and Environment: Lansing, MI, USA, 2011; pp. 329–339. [Google Scholar]
- Kumar, R.; Somrongthong, R.; Ahmed, J. Impact of waste management training intervention on knowledge, attitude and practices of teaching hospital workers in Pakistan. Pak. J. Med. Sci. 2016, 32, 705–710. [Google Scholar] [CrossRef] [PubMed]
- Almahi, A.Y.Y. Assessment of the Radioactive Waste Management in Nuclear Medicine Departments in Khartoum State Hospitals. Available online: http://repository.sustech.edu/handle/123456789/14321 (accessed on 11 August 2017).
- Kusiluka, L.J.M.; Mkhandi, D.N.H.; Hango, M. Management of Medical Wastes: Public Awareness and Associated Health Risks. J. Open Univ. Tanzan. 2013, 15, 34–51. [Google Scholar]
- WHO. Individualised Rapid Assessment Tool (I-RAT). 2009. Available online: http://www.who.int/water_sanitation_health/facilities/waste/hcwmtool/en/ (accessed on 8 October 2016).
- Dabora, M.A.M.A. Efficiency of Recombinant DNA Vaccine against Hepatitis B Virus in Health Care Workers in Some Hospital in Khartoum State. Master’s Thesis, Sudan University of Science & Technology, Khartoum, Sudan, January 2014. [Google Scholar]
- Laing, R.O.; Hogerzeil, H.V.; Ross-Degnan, D. Ten recommendations to improve use of medicines in developing countries. Health Policy Plan. 2001, 16, 13–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yilmaz, L. Effect of the Training Provided for Nurses on Sharp-Needle stick Injuries and Reporting Process. International Journal of Caring Sciences, 2016, 9, 561. Int. J. Caring Sci. 2016, 9, 561. [Google Scholar]
- NIOSH. Hierarchy of Controls. 2015. Available online: https://www.cdc.gov/niosh/topics/hierarchy/default.html (accessed on 22 September 2017).
- RCN. Sharps Safety. 2013. Available online: http://www.gla.ac.uk/media/media_511552_en.pdf (accessed on 23 August 2017).
Figure 1.
The key steps taken in the identification of the publications for the analysis.
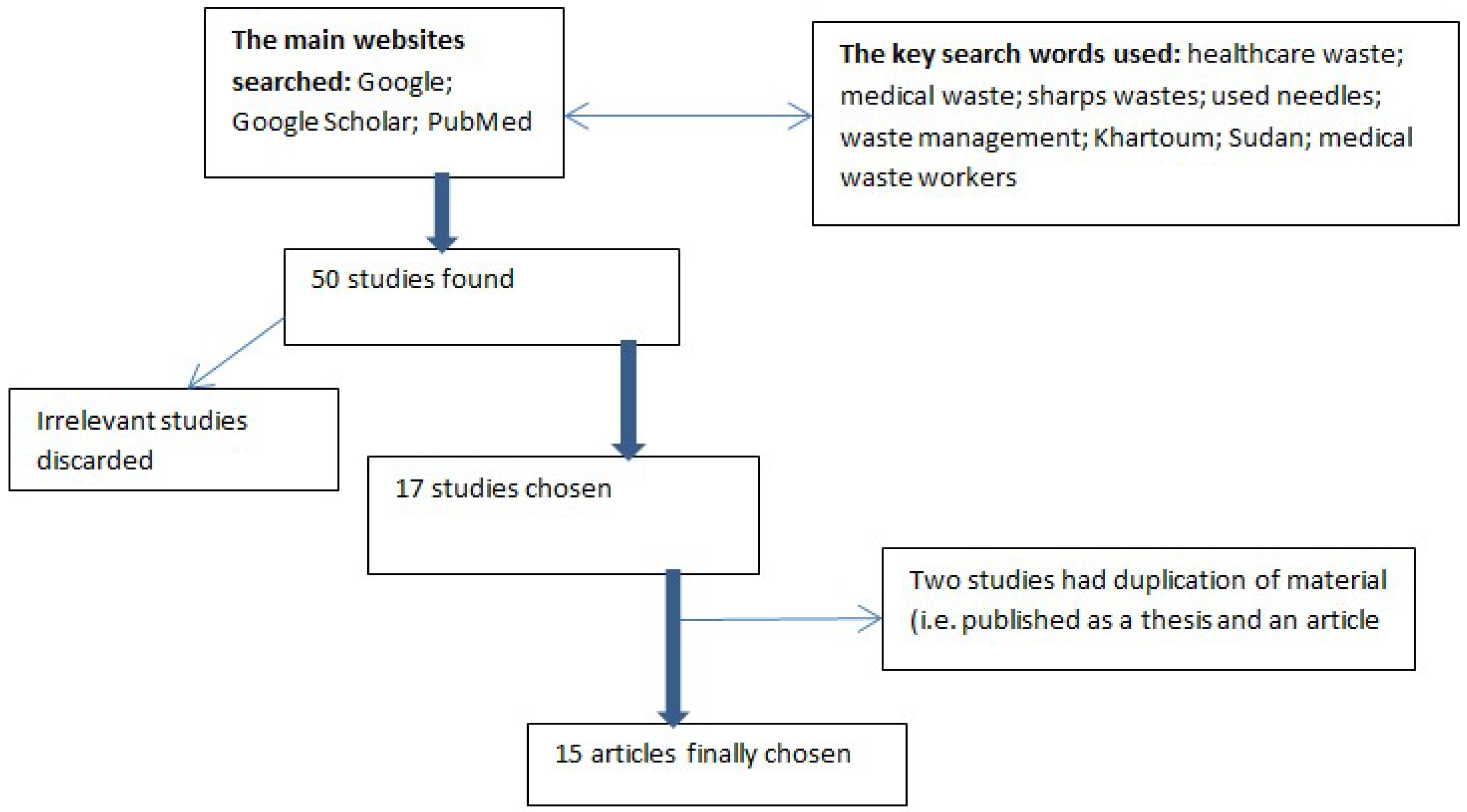
Figure 2.
Estimated healthcare waste arisings per bed per year.


{kind=link}
{kind=link}
Table 1.
A review of the provision of training, personal protective injuries and vaccination, as well as the prevalence of needle stick injuries in selected case study healthcare facilities.
Table 1.
A review of the provision of training, personal protective injuries and vaccination, as well as the prevalence of needle stick injuries in selected case study healthcare facilities.
| Reference | Issues | |||
|---|---|---|---|---|
| Training | PPE 1 | NSIs 2 | Vaccination | |
| [64] | Only 45% were trained on HCWM 3 | 46.5% of did not have PPE | 42.9% injured while working | 69% vaccinated against hepatitis |
| [57] | No hospital personnel were trained about HCWM and, infection control | Manual handling of waste without using PPE | 27% had NSIs | 4% of the HCP 4 were vaccinated |
| [7] | Training was available only in 40% of the investigated HCFs 5 | PPE only 30% in the investigated hospitals | - | - |
| [65] | Called for HCP training and education | Deficiency in protective measures | - | Recommended vaccination for workers, especially those at risk |
| [66] | - | - | Unacceptable injection disposal practices led to 26.1% NSIs | 26.3% of the injections given in the community were used for vaccination |
| [67] | After the intervention, an improvement in the knowledge, attitudes and practices regarding HCWM were reported | - | Decrease in the rate of NSIs and, HBV 6 infection | After the awareness intervention programme, the utilisation of HBV vaccination increased from 11% to 48% |
| 53] | The training programmes for HCP with respect to HCW 7 handling were not efficient | - | - | There was no recurrent medical follow-up and vaccination for HCPs |
| [68] | Recommended periodic training for HCPs | Only 62% were wearing PPE while handling HCW | Only 8% had NSIs | The study was carried on already-vaccinated HCPs |
| [58] | 61.7% do not receive any training in handling hazardous wastes | 95.8% of them used PPE | 91.3% checked with physicians after NSIs | 91.6% did not receive HBV vaccination |
| [69] | Improvement of the HCPs knowledge after educational intervention programme | More PPE were used by the staff after the programme | NSIs were more often reported by the staff | 69% of the study participants in the intervention group were not vaccinated |
| [55] | 42% of HCP were not trained. The training period was not enough for those who received training, and the provision of an education and training programme were recommended | PPE were not used properly i.e., either lack of PPE or they were not aware of its importance | Only 7.5% of HCP knew that HCW is a source of HBV | - |
1 PPE—personal protective equipment. 2 NSIs—needle stick injuries. 3 HCWM—healthcare waste management. 4 HCP—healthcare personnel. 5 HCFs means—healthcare facilities. 6 HBV—hepatitis virus B. 7 HCW—healthcare waste.
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hassan, A.A.; Tudor, T.; Vaccari, M. Healthcare Waste Management: A Case Study from Sudan. Environments 2018, 5, 89. https://doi.org/10.3390/environments5080089
AMA Style
Hassan AA, Tudor T, Vaccari M. Healthcare Waste Management: A Case Study from Sudan. Environments. 2018; 5(8):89. https://doi.org/10.3390/environments5080089
Chicago/Turabian StyleHassan, Ahmed Ali, Terry Tudor, and Mentore Vaccari. 2018. "Healthcare Waste Management: A Case Study from Sudan" Environments 5, no. 8: 89. https://doi.org/10.3390/environments5080089
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.