
Traumatic Brain Injury in United States Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) Hispanic Veterans—A Review Using the PRISMA Method

Abstract
:1. Background and Significance
1.1. Burden of TBI
1.2. Definition of TBI

{kind=link}
| Severity | Glasgow Coma Scale Rating (GCS) | Loss of Consciousness (LOC) | Alteration of Consciousness (AOC) | Posttraumatic Amnesia (PTA) | Structural Brain Imaging |
|---|---|---|---|---|---|
| Mild | 13–15 | Up to 30 min | Up to 24 h | Up to 24 h | Normal |
| Moderate | 9–12 | 30 min to 24 h | > 24 h | 24 h to 7 days | Normal or abnormal |
| Severe | 9–8 | > 24 h | > 24 h | > 7 days | Normal or abnormal |
1.3. Comorbidities Associated with TBI
1.4. Surveillance of TBI Cases
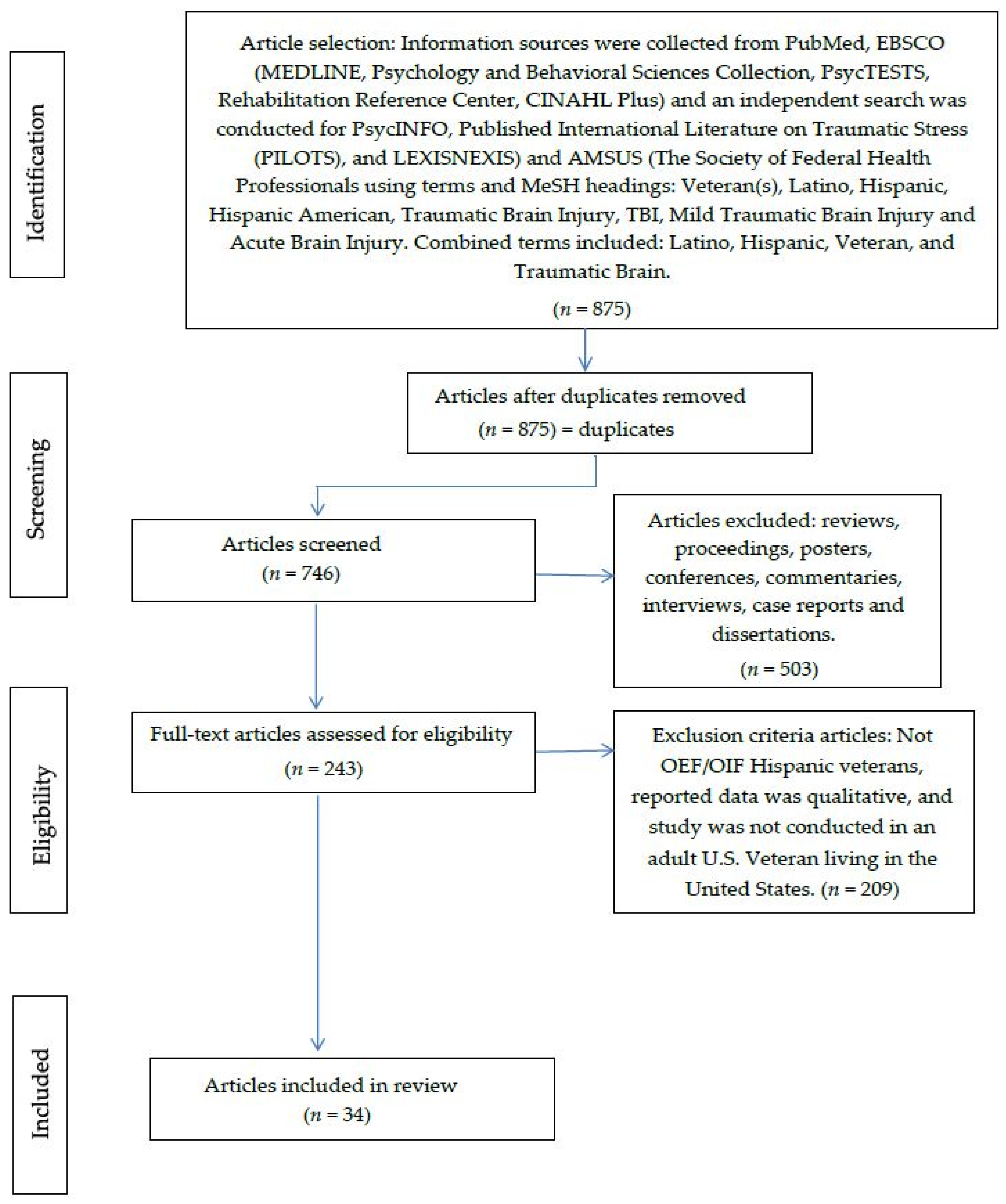
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
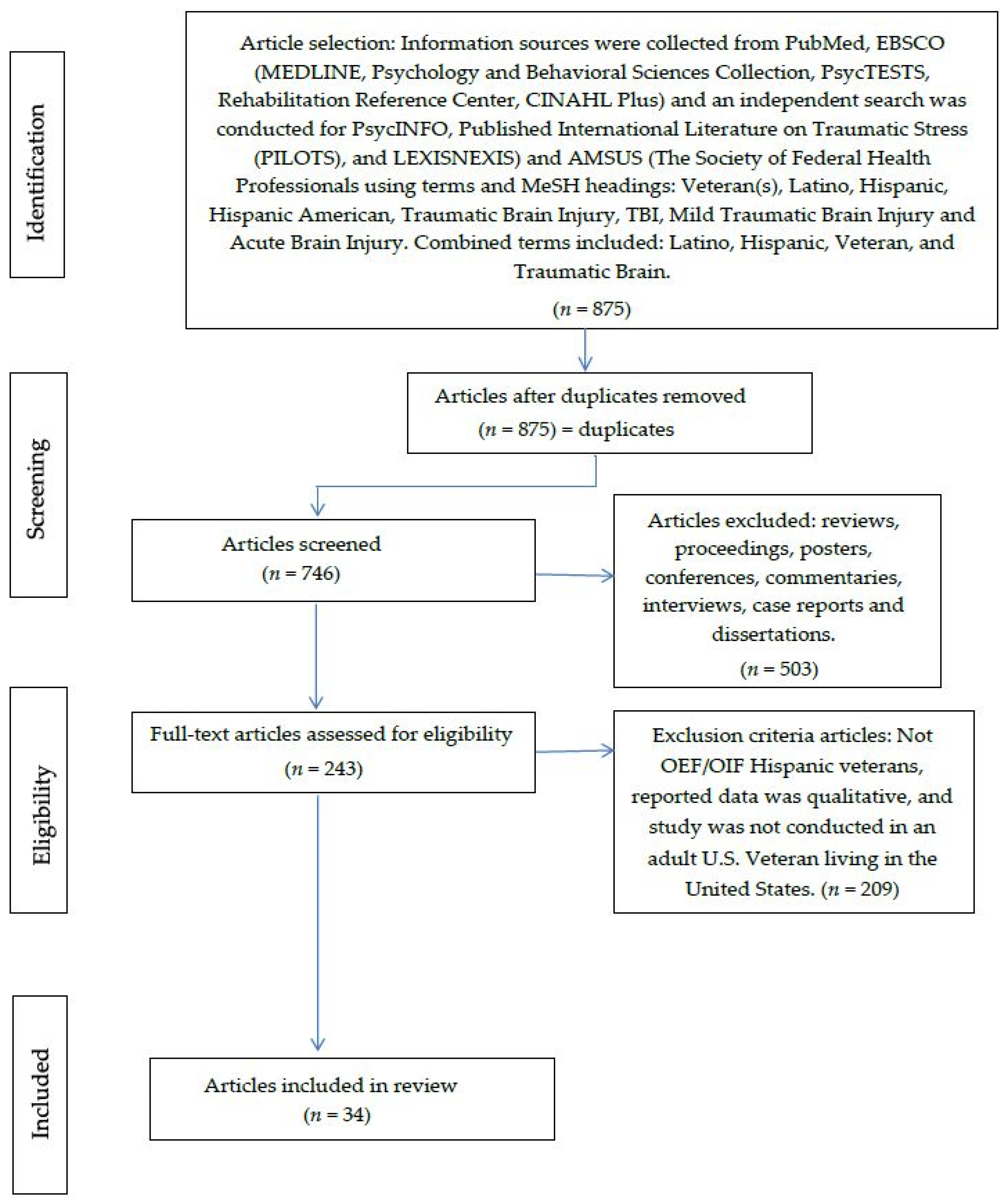
3. Results
| Study | Study Design, Population Sample | Sample Size (% Hispanic) | TBI Definition | Assessment | Outcomes | Critique |
|---|---|---|---|---|---|---|
| Patil et al. [40] | Retrospective cohort study Midwestern VA Polytrauma Network Site | 246 (19%) | VA’s TBI screening. DoD TBI’s definition | Self-reported head pain occurring 30 days prior to initial MTBI screening. Headache severity: Neurobehavioral Symptoms Inventory (0 = none; 4 = almost always) | 45% diagnosed with migraine headaches. 20% diagnosed with chronic daily headaches. 92% reported some level of sleep disturbances. Treatment: Triptan (68%) and anticonvulsant (55%), and tricyclic (40%). Headache rating did not differ by ethnicity (Hispanic/Latino vs. non-Hispanic/Latino) or marital status (married vs. unmarried) | Small sample size. Self-report data (not a valid instrument) for headaches. Low follow up (missing chart information) |
| Ettenhofer et al. [39] | Retrospective, cross-sectional design. VA Greater Los Angeles Healthcare System, GLA Polytrauma Network. | 57 (21.4%) | VA’s TBI screening. TBI’s definition. Based on LOC or PTA: 1 = mild without LOC or PTA; 2 = mild with LOC or PTA; 3 = moderate for LOC and/or PTA; 4 = severe for LOC > 24 h and/or PTA > 7 days | Medical chart review. Clinical interview. Self-report inventory of PCS (Neurobehavioral Symptom Inventory). Battery of neuropsychological test. | Post concussive symptoms = 34% of veterans self-reported (severe to very severe). Involvement in work and school (p = 0.45, p < 0.001). Housing insecurity (p = −0.34, p < 0.05). Clinical-rated DSM-IV GAF (p = 0.43, p < 0.01) | Small sample size. Generability: Only one Polytrauma Network. 89.5% individuals were diagnosed with PTSD. Other co-morbidities could affect the functional status (i.e., pain, sleep disturbances, etc.) |
| Norman et al. [37] | Retrospective, cross-sectional design | 303,716 (~12%) | VA’s TBI screening. DoD TBI’s definition Severe: Normal or abnormal imaging, LOC > 24 h; AOC > 24, PTA > 7 days. Moderate: Normal or abnormal imaging, LOC > 30 min and ≤ 24 h, AOC > 24 h, PTA > 1 day and < 7 days.Mild: Normal imaging; LOC from 0–30 min, AOC is up to 24 h and PTA is from 0–1 day and unclassifiable. | ICD-9-CM code for communications disorders (aphasia, voice disorders and, fluency) | Voice disorders (3.5 per 1000). Aphasia (1.9 per 1000). Fluency disorder (0.7 per 1000). TBI with aphasia (OR = 11.09–252.75, 95% CI = 8.78–441.52, p < 0.01). TBI with fluency disorders (OR = 3.58–10.41, 95% CI = 2.56–42.40, p < 0.01). TBI and voice disorders (OR = 1.5–6.61, 95% CI = 1.24–14.05, p < 0.01) | Diagnostic bias: some veterans were only diagnosed once with communication disorders. Diagnostic categories too broad. No clear mechanism of injury, could be associated with speech-language problems |
| Rodgers et al. [42] | Retrospective, cross-sectional design Veterans Affairs Outpatient Level 3 Polytrauma clinic | 310 (1.3%) | DoD TBI’s definition. VA’s TBI screening. Self-report TBI | Self-report of Beck Depression Inventory II (BDI-II) Score: 0 = no symptoms to 3 = severe symptoms. Total score of 21 = moderate symptoms | Mean BDI-II total score = 21.20 (SD = 11.76; range = 0–51) CFA’s models: three-factor TBI, two factor psychiatric, three-factor substance abuse, and two-factor neurorehabilitation samples. Chi-square for all models were significant (p < 0.001). Three-factor substance abuse model: reliability = 0.79 to 0.88 (best fit). | Instrument (BDI-II) was demonstrated to have a good reliability and validity in previous studies.3. Generalizability (only veterans referred to outpatient level 3polytrauma clinic. Small sample size to use CFA’s models. |
| Sozda et al. [38] | Cross-sectional study design Veterans Affairs Outpatient Level 3 Polytrauma clinic | 103 (14%) | DoD TBI’s definition VA’s TBI screening | Wechsler Adult Intelligence Scale (WAIS-III) Digit Span subset. Delis-Kaplan Executive Functioning System. Hopskins Verbal Learning Test. Brief Visuospatial Memory Test. Beck Depression Inventory. PTSD Checklist-Military Version | Non-normality of neuropsychological (Wilsoxon’s sign ranked tests to compare median z scores of interest, and Cohen’s r effect sizes; small = 0.1, medium= 0.3, large = 0.5). Visual learning and memory abilities = intact compared to verbal learning and memory performance = reduced. Verbal learning (SD = 1.1 below the mean) and verbal memory (SD = 1.4 below the mean) | All MTBI’s were self- reported during soldier’s active duty status. Lack of methodology while identification of included/excluded patients. Controlled environment setting, Causal relationship between psychiatric symptoms, MTBI, and neuropsychological performance. |
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
Appendix A: Search strategy
MeSH Headings:
- Hispanic: Cuban American, Cuban Americans, Hispanics, Latina, Latinas, Latino, Puerto Rican, Puerto Ricans, Spanish American, Spanish Americans
- Veteran: Veterans
- Traumatic Brain Injury: Acute Brain injury, brain injury, brain laceration, brain lacerations, brain trauma, contusion, contusions, encephalopathy, mild traumatic brain injury, post traumatic TBI
PubMed (Full-Text):
- ■
- Included = 556; duplicates = none; articles screened = 556; articles excluded (reviews, proceedings, posters, conferences, commentaries, interviews, case reports and dissertations) = 502
- ■
- Included for eligibility = 54
- ■
- Excluded by criteria = 50
- No OEF/OIF Hispanic veterans = 37
- Data was qualitative = 3
- Study was not conducted in an adult U.S. Veteran living in United States = 6
- ■
- Included: 4 articles
LEXISNEXIS: Accessed by the VA Librarian
- ■
- No table to import to Microsoft Access; manual entries
- ■
- Included=13 articles as 26 January 2015; duplicates= 2 by PubMed; articles screened= 11; articles excluded (reviews, proceedings, posters, conferences, commentaries, interviews, case reports and dissertations)= 0
- ■
- Included for eligibility= 11 articles
- ■
- Excluded= 11
- No OEF/OIF Hispanic veterans= 9
- Data was qualitative= 0
- Study was not conducted in an adult U.S. Veteran living in United States= 2
- ■
- Included = 0
PsycINFO:
- ■
- Exported table to Microsoft Access to access inclusion/exclusion criteria.
- ■
- Included = 171, duplicated = 21 by Refworks; articles screened = 150; articles excluded (reviews, proceedings, posters, conferences, commentaries, interviews, case reports and dissertations) = 0
- ■
- Included for eligibility = 150
- ■
- Excluded = 129
- No OEF/OIF Hispanic veterans = 120
- Data was qualitative = 9
- Study was not conducted in an adult U.S. Veteran living in United States = 0
- ■
- Included for final review = 21
PILOTS:
- ■
- Included = 8 articles; duplicated = 2; articles screened = 6; articles excluded (reviews, proceedings, posters, conferences, commentaries, interviews, case reports and dissertations) = 0
- ■
- Included for eligibility= 6
- ■
- Excluded= 3
- No OEF/OIF Hispanic veterans = 3
- Data was qualitative = 0
- Study was not conducted in an adult U.S. Veteran living in United States = 0
- ■
- Included for eligibility = 3
EBSCO-CINAHL Plus:
- ■
- Included = 95 articles; duplicated (Brain Injuries AND Hispanics AND Veterans) = 94; articles screened = 1; articles excluded (reviews, proceedings, posters, conferences, commentaries, interviews, case reports and dissertations) = 0
- ■
- Included for eligibility= 1
- ■
- Excluded: 1
- No OEF/OIF Hispanic veterans = 1
- Data was qualitative = 0
- Study was not conducted in an adult U.S. Veteran living in United States = 0
- ■
- Included for eligibility: 0
EMBASE:
- ■
- Included = 12 articles; duplicated = 5; articles screened = 7; articles excluded (reviews, proceedings, posters, conferences, commentaries, interviews, case reports and dissertations) = 0
- ■
- Included for eligibility = 7
- ■
- Excluded = 7
- No OEF/OIF Hispanic veterans = 3
- Data was qualitative = 3
- Study was not conducted in an adult U.S. Veteran living in United States = 1
- ■
- Included for eligibility = 0
AMSUS:
- ■
- Manually entered records on Access database
- ■
- Included = 20 articles; duplicated = 5 articles with LEXIS NEXIS; articles screened = 15; articles excluded (reviews, proceedings, posters, conferences, commentaries, interviews, case reports and dissertations) = 1
- ■
- Included for eligibility = 14
- ■
- Excluded = 8
- No OEF/OIF Hispanic veterans = 4
- Data was qualitative = 3
- Study was not conducted in an adult U.S. Veteran living in United States = 1
- ■
- Included for final review = 6
Data Searched: 1980–20 February 2015
Automatic updates:
- ■
- PubMed e-Alerts request on 18 January 2015
- ■
- ESCO alert on 4 March 2015
- ■
- VACO Library Literature e-Alerts Request as 27 January 2015, 3:47 PM
- ■
- Daily News Alert: Veteran/Military Suicide
- ■
- Weekly PubMed/MEDLINE Alerts: OEF/OIF Veterans, Traumatic Brain Injury o Biweekly PubMed/MEDLINE Alert: Minority Veterans
References
- Menon, D.K.; Schwab, K.; Wright, D.W.; Mass, A.I. Position statement: Definition of traumatic brain injury. Arch. Psyc. Med. Rehabil. 2010, 91, 1637–1640. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Returning Home from Iraq and Afghanistan: Preliminary Assessment of Readjustment Needs of Veterans, Service Members, and Their Families; The National Academies Press: Washington, DC, USA, 2010. [Google Scholar]
- Center for Military Health Policy Research. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery. 2008. Available online: http://www.rand.org/content/dam/rand/pubs/monographs/2008/RAND_MG720.pdf (accessed on 13 November 2015).
- Bazarian, J.J.; Blyth, B.; Mookerjee, S.; He, H.; McDermott, M.P. Sex differences in outcome after mild traumatic brain injury. J. Neurotrauma 2010, 27, 527–539. [Google Scholar] [CrossRef] [PubMed]
- Kirkness, C.J.; Burr, R.L.; Mitchell, P.H.; Newell, D.W. Is there a sex difference in the course following traumatic brain injury? Biol. Research Nurs. 2004, 5, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Arango-Lasprilla, J.C.; Rosenthal, M.; Deluca, J.; Komaroff, E.; Sherer, M.; Cifu, D.; Hanks, R. Traumatic brain injury and functional outcomes: Does minority status matter? Brain Inj. 2007, 21, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Arango-Lasprilla, J.C.; Ketchum, J.M.; Gary, K.W.; Kreutzer, J.S.; O’Neil-Pirozzi, T.M.; Wehman, P.; Marquez de la Plata, C.; Jha, A. The influence of minority status on job stability after traumatic brain injury. PM&R 2009, 1, 41–49. [Google Scholar]
- Gary, K.W.; Arango-Lasprilla, J.C.; Ketchum, J.M.; Kreutzer, J.S.; Copolillo, A.; Novack, T.A.; Jha, A. Racial differences in employment outcome after traumatic brain injury at 1, 2, and 5 years post-injury. Arch. Phys. Med. Rehabil. 2009, 90, 1699–1707. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, V.B.; Ward-Murray, E.M. Decreasing the gap in health care disparities research using novel concepts on time, trustworthiness, and education as methodological strategies. Insight 2008, 34, 8–13. [Google Scholar]
- National Institute of Minority Health and Health Disparities (NIMHD). About NIMHD. Available online: http://www.nimhd.nih.gov/about/nimhdHistory.html (accessed on 13 November 2015).
- National Institute of Health (NIH). Public Law 106-525-NOV 22, 2000. 2000. Available online: http://history.nih.gov/research/downloads/PL106-525.pdf (accessed on 13 November 2015). [Google Scholar]
- Centers for Disease Control and Prevention. CDC Health Disparities and Inequalities Report (CHDIR). 2015. Available online: http://www.cdc.gov/TraumaticBrainInjury (accessed on 13 November 2015). [Google Scholar]
- Centers for Disease Control and Prevention. CDC Health disparities and inequalities report—United States, 2011. MMWR Morb. Mortal. Wkly. Rep. 2011, 60, 1–116. [Google Scholar]
- Egede, L.E.; Dismuke, C.; Echols, C. Racial/ethnic disparities in mortality risk among US veterans with traumatic brain injury. Am. J. Public Health 2012, 102, S266–S271. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, K.T.; Donnelly, J.P.; Dunnam, M.; Warner, G.C.; Kittleson, C.J.; Constance, J.E.; Bradshaw, C.B.; Alt, M. Reliability, sensitivity, and specificity of the VA Traumatic Brain Injury Screening Tool. J. Head Trauma Rehabil. 2011, 26, 439–453. [Google Scholar] [CrossRef] [PubMed]
- Kelly, D.F.; Becker, D.P. Advances in management of neurosurgical trauma: USA and Canada. World J. Surg. 2001, 25, 1179–1185. [Google Scholar] [CrossRef] [PubMed]
- Fakhry, S.M.; Trask, A.L.; Waller, M.A.; Watts, D.D. Management of brain-injured patients by an evidence-based medicine protocol improves outcomes and decreases hospital charges. J. Trauma 2004, 56, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Traumatic Brain Injury in the United States: Fact Sheet. 2015. Available online: http://www.cdc.gov/traumaticbraininjury/get_the_facts.html (accessed on 13 November 2015). [Google Scholar]
- Terrio, H.; Brenner, L.A.; Ivins, B.J.; Cho, J.M.; Helmick, K.; Schwab, K.; Scally, K.; Bretthauer, R.; Warden, D. Traumatic brain injury screening: Preliminary findings in a US Army brigade combat team. J. Head Trauma Rehabil. 2009, 24, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Hoge, C.W.; Goldberg, H.M.; Castro, C.A. Care of war veterans with mild traumatic brain injury—Flawed perspectives. N. Engl. J. Med. 2009, 360, 1588–1591. [Google Scholar] [CrossRef] [PubMed]
- Tanielian, T.; Jaycox, L.H. (Eds.) Invisible Wounds of War: Psychological and Cognitive Injuries, their Consequences, and Services to Assist Recovery; RAND Corp: Santa Monica, CA, USA, 2008.
- Schneiderman, A.I.; Braver, E.R.; Kang, H.K. Understanding sequelae of injury mechanisms and mild traumatic brain injury incurred during the conflicts in Iraq and Afghanistan: Persistent postconcussive symptoms and posttraumatic stress disorder. Am. J. Epidemiol. 2008, 167, 1446–1452. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.T.; St. Andre, J.R.; Pape, T.L.; Steiner, M.L.; Stroupe, K.T.; Hogan, T.P.; Weaver, F.M.; Smith, B.M. An evaluation of the Veterans Affairs traumatic brain injury screening process among Operation Enduring Freedom and/or Operation Iraqi Freedom veterans. PM&R 2013, 5, 210–220. [Google Scholar]
- Veterans Health Initiative. Traumatic Brain Injury. 2010. Available online: http://www.publichealth.va.gov/docs/vhi/traumatic-brain-injury-vhi.pdf (accessed on 13 November 2015). [Google Scholar]
- Defense and Veterans Brain Injury Center (DVIC). DoD Worldwide Numbers for TBI. 2015. Available online: http://dvbic.dcoe.mil/dod-worldwide-numbers-tbi (accessed on 13 November 2015).
- Jaffee, M.S.; Meyer, K.S. A brief overview of traumatic brain injury (TBI) and posttraumatic stress disorder (PTSD) within the Department of Defense. Clin. Neuropsychol. 2009, 23, 1291–1298. [Google Scholar] [CrossRef] [PubMed]
- Bilmes, L.J.; Stiglitz, J.E. The three Trillion Dollar War: The True Cost of the Iraq Conflict; W.W. Norton & Company: New York, NY, USA, 2008. [Google Scholar]
- USA Today. VA to Increase Benefits from Mild Brain Trauma. 2008. Available online: http://usatoday30.usatoday.com/news/military/2008-09-22-tbibenefits_N.htm (accessed on 13 November 2015).
- Military.com. Traumatic Brain Injury Overview. Available online: http://www.military.com/benefits/veterans-health-care/traumatic-brain-injury-overview.html (accessed on 13 November 2015).
- National Institute of Neurological Disorders and Stroke. NINDS Traumatic Brain Injury Information Page. 2015. Available online: http://www.ninds.nih.gov/disorders/tbi/tbi.htm (accessed on 13 November 2015). [Google Scholar]
- Centers for Disease Control and Prevention. Basic Information about Traumatic Brain Injury and Concussion. 2015. Available online: http://www.cdc.gov/traumaticbraininjury/basics.html (accessed on 13 November 2015). [Google Scholar]
- Defense and Veterans Brain Injury Center (DVIC). TBI Basics. Available online: http://dvbic.dcoe.mil/about-traumatic-brain-injury/article/tbi-basics (accessed on 13 November 2015).
- Veterans Health Administration. Screening and Evaluation of Possible Traumatic Brain Injury in Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF) Veterans. 2010. Available online: http://www.va.gov/optometry/docs/vha_directive_2010-012_screening_and_evaluation_of_possible_tbi_in_oef-oif_veterans.pdf (accessed on 13 November 2015). [Google Scholar]
- Sayer, N.A.; Nelson, D.; Nugent, S. Evaluation of the Veterans Health Administration traumatic brain injury screening program in the upper Midwest. J. Head Trauma Rehabil. 2011, 26, 454–467. [Google Scholar] [CrossRef] [PubMed]
- Veteran Health Administration. Report on VA Facility Specific Operation Enduring Freedom, Operation Iraqi Freedom, and Operation New Dawn Veterans Coded with Potential PTSD, from 1st Qtr FY 2002 through 3rd Qtr FY 2012. 2012. Available online: http://www.publichealth.va.gov/docs/epidemiology/ptsd-report-fy2012-qtr3.pdf (accessed on 13 November 2015). [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Norman, R.S.; Jaramillo, C.A.; Amuan, M.; Wells, M.A.; Eapen, B.C.; Pugh, M.J. Traumatic brain injury in veterans of the wars in Iraq and Afghanistan: Communication disorders stratified by severity of brain injury. Brain Inj. 2013, 27, 1623–1630. [Google Scholar] [CrossRef] [PubMed]
- Sozda, C.N.; Muir, J.J.; Springer, U.S.; Partovi, D.; Cole, M.A. Differential learning and memory performance in OEF/OIF veterans for verbal and visual material. Neuropsychology 2014, 28, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Ettenhofer, M.L.; Melrose, R.J.; Delawalla, Z.; Castellon, S.A.; Okonek, A. Correlates of functional status among OEF-OIF veterans with a history of traumatic brain injury. Mil. Med. 2012, 177, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Patil, V.K.; St. Andre, J.R.; Crisan, E.; Smith, B.M.; Evans, C.T.; Steiner, M.L.; Pape, T.L. Prevalence and treatment of headaches in veterans with mild traumatic brain injury. Headache 2011, 51, 1112–1121. [Google Scholar] [CrossRef] [PubMed]
- Afari, N.; Pittman, J.; Floto, E.; Owen, L.; Buttner, M.; Hossain, N.; Baker, D.G.; Lindamer, L.; Lohr, J.B. Differential impact of combat on post-deployment symptoms in female and male veterans of Iraq and Afghanistan. Mil. Med. 2015, 180, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, M.; Asaria, M.; Walker, S.; McMillan, D.; Lucock, M.; Harden, M.; Palmer, S.; Eastwood, A. The clinical effectiveness and cost-effectiveness of low intensity psychological interventions for the secondary prevention of relapse after depression: A systematic review. Health Technol. Assess. 2012, 16, 1–130. [Google Scholar] [CrossRef] [PubMed]
- Wisco, B.E.; Marx, B.P.; Holowka, D.W.; Vasterling, J.J.; Han, S.C.; Chen, M.S.; Gradus, J.L.; Nock, M.K.; Rosen, R.C.; Keane, T.M. Traumatic brain injury, PTSD, and current suicidal ideation among Iraq and Afghanistan U. S. veterans. J. Trauma. Stress 2014, 27, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Olson-Madden, J.H.; Forster, J.E.; Huggins, J.; Schneider, A. Psychiatric diagnoses, mental health utilization, high-risk behaviors, and self-directed violence among veterans with comorbid history of traumatic brain injury and substance use disorders. J. Head Trauma Rehabil. 2012, 27, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Department of Defense (DoD). Section 508 Fact Sheet. Available online: http://dodcio.defense.gov/Portals/0/Documents/Section%20508/DoDS508_FactSheet_Compliant.pdf (accessed on 13 November 2015).
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arriola, V.D.; Rozelle, J.W. Traumatic Brain Injury in United States Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) Hispanic Veterans—A Review Using the PRISMA Method. Behav. Sci. 2016, 6, 3. https://doi.org/10.3390/bs6010003
Arriola VD, Rozelle JW. Traumatic Brain Injury in United States Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) Hispanic Veterans—A Review Using the PRISMA Method. Behavioral Sciences. 2016; 6(1):3. https://doi.org/10.3390/bs6010003
Chicago/Turabian StyleArriola, Vanessa D., and Jeffrey W. Rozelle. 2016. "Traumatic Brain Injury in United States Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) Hispanic Veterans—A Review Using the PRISMA Method" Behavioral Sciences 6, no. 1: 3. https://doi.org/10.3390/bs6010003