1. Introduction
That human relationships play a valuable role in maintaining physical and mental wellbeing has become conventional wisdom in the interdisciplinary literature on social epidemiology. Studies show that networks are the primary channels through which, for example, behaviors such as smoking and drinking spread and are shared among close contacts (
Smith and Christakis 2008). Medical diseases and symptoms such as obesity, influenza and depression also have a network basis since they travel and grow, or become “contagious,” through human interactions (
Christakis and Fowler 2013). In addition, social networks are important because they can play a dual role of directly and indirectly protecting and improving health by transferring helpful information and resources as well as providing a buffer against stress factors (
Cohen et al. 2000). A voluminous literature exists highlighting the health benefits of social networks, ranging across a host of mental and physical categories (
Berkman et al. 2000;
Kawachi and Berkman 2001;
Uchino 2006;
Umberson et al. 2010). In particular, there is substantial evidence that social relations are critical for providing “social support” that can protect and promote psychological or subjective wellbeing (
De Silva et al. 2007). From adolescent depression (
Guan and Kamo 2016) to elderly loneliness (
Warner and Adams 2016), it has been shown time and again that interpersonal networks offer significant health benefits. According to a recent systematic review, both individual- and ecological-level social capital has the potential to reduce the risk of common mental disorders (
Eshan and De Silva 2015). In short, the message is clear: social connectedness produces healthy outcomes, while social isolation has deleterious effects. The objective of this study is to contribute to the literature by shedding additional light on the association between social networks and mental health, specifically psychological distress, in an East Asian context. It seeks to do so in following ways. First, the majority of research in the field does not systematically differentiate between types of network relations. Instead, they are usually lumped together by counting the total number of contacts to which the focal individual is connected (see e.g.,
Cornwell and Laumann 2015;
Cornwell et al. 2014). Following Granovetter’s (1973) well-known distinction between “strong” and “weak” ties (
Granovetter 1973), the current study offers a more nuanced analysis in terms of how tie strength, social networks, and mental health outcome are intertwined. Second, interpersonal networks are formed and operate in environmental settings (
Berkman et al. 2000). How social ties relate to health is thus partly shaped by the broader context in which individual actors are embedded. That is, ecology is important (
Sampson 2003). A growing number of studies have highlighted “neighborhood effects” on individual health outcomes (
Kawachi and Berkman 2001). Neighborhood characteristics can protect and promote health through various mechanisms, including the provision of, for example, collective efficacy (
Sampson 2012) and reciprocity and enforceable trust (
Alejandro and Sensenbrenner 1993). Deciphering the exact causal linkage between ecological variables and individual health outcomes has been methodologically tricky (
van Ham et al. 2012). Nevertheless, one of the main issues has been to decipher “contextual” versus “compositional” effects (
Kawachi and Berkman 2001). That is, scholars are increasingly interested in how and to what extent where people live have an independent influence on their mental and physical wellbeing independent of their individual characteristics (e.g., education, income, gender, race). Using hierarchically nested data and related analytic strategy, this study thus explicitly investigates how and the extent to which the network-health linkage is moderated by contextual (neighborhood-level) factors. Lastly, prior studies based on multilevel modeling primarily focus on the ameliorative role of “neighborhood social capital” (
Bender et al. 2015;
Lau and Ataguba 2015;
Meng and Chen 2014;
Tomita and Burns 2013). As a result, their contributions notwithstanding, we know relatively little about how neighborhood characteristics (e.g., average household income, mean age of residents) may operate as a risk factor in undermining or exacerbating individual health and wellbeing. This research incorporates official government statistics, including a measure of community ethnic heterogeneity, to probe the possible contingent associations between network size and depressive symptoms based on a probability sample from South Korea (hereafter Korea).
The bulk of existing research is rooted in empirical cases from Western developed countries (North America and Europe). How does the social capital argument apply to a non-Western (i.e., Confucian cultural) context such as Korea? Despite the growing body of research, this particular question has been understudied (
Yip et al. 2007;
Yamaoka 2008). Asian societies under the cultural tradition of Confucianism typically stress “collectivism” over “individualism,” which can lead to disparate results concerning the relationship between social capital and wellbeing (
Chang 2009). The few studies focusing on Asia have produced findings that partly support as well as challenge those based on Western populations (
Yip et al. 2007;
Chang 2009). According to an investigation using cross-national data on East Asia, cognitive (i.e., trust) but not structural (i.e., organizational) social capital was related to health and subjective wellbeing (
Yamaoka 2008). The implication is that the universality of the relationship between social capital and mental health cannot be taken for granted. Certain aspects of social capital may improve health in one setting, while another may fail to do so in a different context. A comparative study of multiple European and Asian countries further reveals that factors underlying subjective wellbeing are in fact unique across sociocultural contexts (
Jagodzinski 2010). The purpose of this paper is to increase our understanding of this variation by examining the social capital-mental health linkage in Korea.
With respect to the main theme of this paper, Korea presents itself as a compelling empirical example to be analyzed. The issue of tackling mental health problems has been precarious at best in many Asian countries (
Maramis et al. 2011). Within the Asia Pacific Rim, Korea especially remains somewhat of an enigma. Accompanied by rapid and successful economic progress during the last several decades, the country has significantly improved its national healthcare services, culminating in universal coverage for all citizens (
OECD 2012). Despite the availability of relatively affordable and quality services, however, many Koreans across different socioeconomic strata and demographic backgrounds suffer from acute mental health-related illnesses (
Park et al. 2012). The gravity of the situation is underscored by the fact that Korea has led all OECD-member countries for the last decades in terms of the highest age-standardized suicide rate (
OECD 2015), with no signs of slowing down. The dynamics of individual-level social capital and neighborhood characteristics as they relate to psychological distress among Koreans, therefore, merits systematic attention.
1.1. Mechanisms Underlying Networks and Health
Despite the voluminous findings in support of the network-health nexus, there is a shortage of theoretical explanations concerning
why networks matter (
Tsai and Papachristos 2015;
Thoits 2011). A list of alternative mechanisms has been proposed to explain the relationship between networks and health outcomes. According to one of the earliest and most oft-cited review articles, networks effect health by way of key pathways, namely social “support,” “influence,” and “engagement” (
Berkman et al. 2000). That is, networks can channel material, emotional and instrumental support to those in need. They can also influence people to be healthy through peer pressures and diffusion of norms, i.e., networks can motivate people to adopt healthy habits and to engage in health-enhancing behaviors. Another review essay classifies the health benefits of social ties in terms of behavioral, psychosocial and physiological explanations. The first has to do with dietary habits, medical regimens, exercise and other matters that can promote health or prevent illness. The second deals with social support, symbolic meaning of relationships, etc. In addition, finally, the third consists of how social processes influence physiological processes (
Umberson and Montez 2010). Yet another systematic review cites additional related factors such as social influence/social comparison, social control, role-based purpose and meaning, and belonging and companionship (
Thoits 2011).
The common thread running throughout these and other proposed mechanisms is that interpersonal networks are a main source of social (i.e., emotional and instrumental) support, which is functional for sustaining mental health and facilitating psychological wellbeing (
Kawachi and Berkman 2001). Even a cursory review of the extant scholarship reveals that most studies emphasize the role of overall, and often undifferentiated, network size (
McCarty et al. 2001) in relation to health behaviors and outcomes. In his classic work on suicide, Durkheim (
Durkheim 1951) propounds the integration-regulation dichotomy in analyzing social structural conditions under which an individual is more likely to resort to deadly self-harm. His basic thesis is that suicide varies inversely with integration, while over-regulation can intensify suicidal ideation. In a nutshell, the distinction here is largely a quantitative one. That is, Durkheim implies a kind of non-monotonic relationship where the number or level of connections plays a protective function, but only to a certain extent before turning into a risk factor. Durkheim’s monumental insights continue to inspire and influence academic research today on the importance of social relationships (
Berkman et al. 2000;
Tsai and Papachristos 2015). Not all human relations, however, are the same in terms of intimacy and duration (
Degenne and Lebeaux 2005;
Grossetti 2007;
Totterdell et al. 2008). Some are closer and more stable, as in kin relations. By contrast, others are more distant and transient, as in colleague relations. Put another way, at the risk of oversimplification, network relations are said to be “strong” or “weak” (
Granovetter 1973). This conceptual distinction, not explicitly recognized by Durkheim and even some of the more contemporary scholars, has profound implications for understanding the health-related roles and benefits of network ties.
1.2. Tie Strength and Social Provisions
As has been pointed out by
Granovetter (1973) in his seminal article, the respective quality of information that circulates through strong and weak ties is uniquely different. Information transmitted via strong networks tend to be confirmatory and redundant, while that obtained through weak channels tend to be more novel. It is in this sense that weak ties are ironically said to be “strong.” By extension, then, a piece of otherwise well-intended advice from a family member (strong tie) can turn out to be inferior to that given by an acquaintance (weak tie). This dichotomous notion is similar to the distinction made in the sociology of health literature about primary and secondary groups (
Thoits 2011). It also closely resembles Putnam’s (
Putnam 2001) discussion on bonding and bridging forms of social capital. Bonding social capital denotes resources found within similar others; bridging social capital, by contrast, signifies resources circulated among members who are relatively dissimilar. Another way of looking at this is that bonding networks (kin members and close friends) are more homogeneous, while bridging networks (acquaintances and coworkers) are more heterogeneous. As the name suggests, bridging networks can extend across different cliques, groups, institutions and communities (
Villalonga-Olives and Kawachi 2015). In comparison, bonding networks are better at providing cohesion and solidarity, if not conformity, through internal monitoring and consensus building, as articulated by
Coleman (1988) and
Portes and Sensenbrenner (1993). In short, weak ties have functional resemblance to bridging social capital, whereas strong ties are characteristic of bonding social capital.
This qualitative difference in relational types is critical because social provisions (informational advice, emotional intimacy, material support, etc.) vary according to the identity of network contacts or alters (
McPherson et al. 2006;
Perry and Pescosolido 2010;
Wellman and Frank 2001). In times of personal crisis, for instance, the ego, or the focal actor, is more likely to seek comfort from close contacts such as family and friends. When in need of obtaining valuable or scarce information to solve a particular problem, on the other hand, the person is more likely to gravitate toward, say, a friend of a friend who can bridge the informational gap. In fact, research shows that emotional and material support typically comes from strong ties, whereas weak ties are more useful in channeling information-related benefits (
Binder et al. 2012;
Burt 2005;
Weil et al. 2012;
Wellman and Wortley 1990). Since different types of interpersonal contacts deliver different kinds of assistance or support, it is important to examine how strong and weak ties differentially influence health. Unfortunately, the bulk of prior research has not fully recognized this difference. In fact, many studies rely on an undifferentiated measure of network size that consists mainly of strong ties. To great extent, this methodological tendency is rooted in the fact that the wording for the “Name Generator” question, most often used in collecting egocentric network data, is biased. Specifically, it asks respondents to name (usually up to five) close confidants with whom they can share private matters. In other words, the survey item is designed to tap what is called “core networks” (
McPherson et al. 2006;
Binder et al. 2012), which, by definition, precludes weak ties on the periphery (casual acquaintances, neighbors, co-workers, etc.).
The General Social Survey (GSS) of the National Opinion Research Center at the University of Chicago first introduced this name-generator item back in 1985, which has since been replicated and adopted by other population-based surveys including Add Health (National Longitudinal Study of Adolescent to Adult Health) and NSHAP (National Social Life, Health, and Aging Project), to name two of the most oft-cited examples. Perhaps no field of research better showcases the salutary role of social relationship than that on health and aging. There is indeed ample evidence indicating that social isolation powerfully and adversely impacts mental and physical wellbeing of, in particular, elderly populations. According to one study based on the NSHAP data, lack of proper connectedness significantly lowers subjective health status among older American adults (
Cornwell and Waite 2009). Another NSHAP-based investigation shows that the changes in core network members over time have profound implications for the wellbeing of elderly Americans (
Cornwell and Laumann 2015). These and a host of other findings using different datasets demonstrate robust associations between being “more connected” and being “healthier.” Yet, because the definition of social network is not disaggregated along the dimension of tie strength, it is not clear exactly how different social contacts (family versus acquaintances, for instance) contribute differently to individual wellbeing. That is, we do not know whether strong ties or weak ties operate according to similar or dissimilar mechanisms in affecting health outcomes. Moreover, there is lack of evidence on how such potentially distinct roles may vary across larger contextual units, or residential characteristics.
In light of the aforementioned discussion of the literature and the limitations therein, this study is informed by the following questions:
First, how do strong and weak ties separately and simultaneously relate to adult depressive symptoms in an East Asian context (i.e., Korea)? Is one type of social relation more effective than the other with respect to the status of psychological distress? Second, to what extent do neighborhood demographic factors have an impact on the outcome, above and beyond individual-level covariates? Does residence in a neighborhood community with more immigrants, for example, imply structural disadvantage and hence poorer mental health? And lastly, do contextual-level characteristics (e.g., ethnic heterogeneity) exert an indirect effect by moderating the network-health nexus that has been frequently observed in the literature based on North American and European cases?
To answer these questions, we now turn to the description of data, variables, and analytic methods.
2. Data and Methods
2.1. Sample and Setting
Data are drawn from the 2012 version of Korean General Social Survey (
Kim 2012), which is modeled after the GSS based on the US sample. KGSS is conducted annually, with a topical module implemented during specific years. In 2012, researchers in Korea, Japan, China and Taiwan collaborated to produce a cross-national dataset, the East Asian Social Survey (EASS), containing the Social Network Module, of which KGSS 2012 is a part. The Social Network Module has various questions about the survey participants’ trust levels, informal/formal organizational involvement, and network ties in each of the four countries. In short, it provides data on individual-level social capital, from which the main predictor variable for this study is constructed. KGSS 2012 also contains a wealth of information on respondents’ social and economic lives, political interests and civic engagement, cultural values and lifestyles, and physical health and subjective wellbeing, among others. Data collection was completed by the Survey Research Center at Sungkyunkwan University in Seoul, Korea. The data have since been released and are publicly available through the ICPSR (Interuniversity Consortium for Political and Social Research) of the University of Michigan (
https://www.icpsr.umich.edu) (
Kim 2012). Like GSS-type surveys, KGSS comprises a national sample drawn by full probability sampling procedures. All Korean household-dwelling adults (18 years of age and over) constituted the target universe. Three-stage area probability sampling method was used to select the initial sample size of 2500 respondents from representative residential blocks, or ward-level administrative districts in cities and rural counties throughout the country. With the response rate of 55.8%, the final sample consists of 1396 participants (individual-level N), who were interviewed face-to-face and clustered in 197 residential districts (neighborhood-level N).
2.2. Measures
The outcome variable is constructed using a battery of questions, which form a shortened version of the Center for Epidemiological Studies Depression Scale (CES-D). Using a 4-point scale (e.g., 1 = Not at all, 4 = Nearly every day), respondents were asked to answer the following question: “Over the last 2 weeks, how often have you been bothered by any of the following problems?” The list of psychological and physiological symptoms includes: “Trouble falling asleep, staying asleep, or sleeping too much,” “Feeling tired or having too little energy,” Little interest or pleasure in doing things,” “Feeling down, depressed or hopeless,” “Thinking that you would be better off dead or that you want to hurt yourself in some way,” etc. Answers to 9 such items were added to create a single index, ranging in value from 11 to 39. In models not shown, the individual answers were log-transformed and standardized (into z scores) to create alternative versions of the dependent measure (Depressive Symptoms). Doing so did not substantively or substantially alter the main findings using the original coding scheme.
At the individual-level, there are two main predictor variables, Strong Network and Weak Network. The former is based on the following survey item: “On an ordinary day, with how many family members or relatives, excluding those who live with you, do you have contact through telephone, mails, internet, or face-to-face?” The latter is measured using the following related question: “On an ordinary day, with how many people other than family members or relatives do you have contact through telephone, mails, internet, or face-to-face?” Both questions were answered based on a Richter-type scale (e.g., 1 = “0”; 2 = “1–2”; 4 = “5–9”; 6 = “20–24”; 8 = “100 or more”). Other surveys such as GSS and NSHAP place a much smaller limit on the egocentric network size, usually 5 (e.g., “Please name up to five individuals with whom you…”). As such, the information given is necessarily confined to close (i.e., strong) contacts. KGSS, on the other hand, allows for the measurement of two distinct types of network ties. Due to the right-tailed skewed distributions of data, the two independent variables take on long-transformed values. A number of confounders are adjusted for in the analysis: namely, the respondent’s age (in years), gender (male = 1), marital status (yes = 1), educational attainment coded on a 7-point scale (e.g., 1 = no formal education; 3 = high school; 5 = 4-year college; 7 = PhD), subjective social status measured on a 10-pont ladder scale (10 = “highest rung”), self-identified extroverted personality (1 = disagree strongly; 4 = neither disagree nor agree; 7 = agree strongly), and, finally, two additional measures of social capital frequently used in public health research. One is general trust, measured based on the following question: “Generally speaking, would you say that most people can be trusted?” (1 = people can almost always be trusted; 2 = people can usually be trusted; 3 = you usually can’t be too careful in dealing with people; 4 = you almost can’t be too careful in dealing with people). Answers were reversed-coded and dichotomized so that the two more affirmative categories were given the value of 1 and 0 otherwise. The other one is civic engagement. Respondents were asked, “How often have you participated in group discussions (either formal or informal discussion among 3 or more people) about the following community or local issues during the last 12 months?” There were four issue categories: environmental, educational, safety and consumer. Individual responses (e.g., 1 = never, 4 = about every week) were averaged across the four items.
In addition to individual covariates, several neighborhood-level factors were taken into account to address part of the research questions posed above. The concept of collective efficacy, or social cohesion, has been widely used as a key component of contextual or neighborhood effect (
Browning and Cagney 2002;
Halbert et al. 2014;
Sampson et al. 1997). KGSS contains two specific items to construct this variable. Respondents were asked to state their views (reverse-coded so that e.g., 1 = strongly disagree and 5 = strongly agree) regarding the following statements: “My neighbors are mutually concerned for each other” and “My neighbors are willing to provide assistance when I am in need.” Answers are first combined (Cronbach’s alpha = 0.79) and then averaged across the contextual unit, a standard practice in the literature (
Browning and Cagney 2002). To control for the socioeconomic dimension of neighborhoods individual (logged) household incomes are similarly averaged. Also included is an aggregate measure of residential urbanity based on self-reported data concerning whether one lives in an urban (yes = 1), as opposed to a suburban or a rural, area. Census data were also accessed to gauge three neighborhood-level demographic features: population size, proportion of elderly residents (aged 65 and over) and number of foreigners (per 1000 natives). Information for these variables was obtained from the Korean Statistical Information Service (KOSIS), the government body in charge of collecting, managing, and disseminating official statistics (more details can be found at
http://kosis.kr/eng) (
KOSIS 2017). Original values were converted to Z scores, with the mean of 0 and the standard deviation of 1. Based on the geocoding information available in the KGSS, the respondent-level data were merged with the KOSIS aggregate statistics to create a 2-level hierarchically nested dataset.
2.3. Analytic Approach
The multistage sampling procedure used in collecting data for KGSS poses a distinct problem in running standard ordinary least squares (OLS) regression, since it violates the basic independence of observation assumption leading to biased parameter estimates. Given this hierarchically nested data structure, multilevel models are estimated, which adjust for the clustering of individual observations (respondents) within the contextual units and allow for the examination of neighborhood-level direct and indirect effects. Following a standard procedure to avoid collinearity problems, all non-dichotomous individual-level (L-1) variables were group-mean centered; all neighborhood-level (L-2) variables were grand-mean centered. All analyses were conducted using the latest version (7.1) of HLM for Windows, the statistical software specifically designed for multilevel modeling. The two-level models are formally expressed as:
Individual-level Full Model:where Y
ij is the measure of depressive symptoms for the respondent
i in the neighborhood
j, β
0j represents the intercept,
βijs are the parameter estimates, and
rij is the individual-level random error term.
Neighborhood-level Direct Effects Model:
where γ
00 is the intercept, γ
01, γ
02,… γ
06 are the coefficients for the effects of six covariates on depressive symptoms, and
u0j is the residential-level error term.
Cross-level Moderating Effects Model: As the first step, a null model (not shown) without any of the covariates, akin to one-way random effects ANOVA, was estimated to see whether the variability in the outcome variable (depressive symptoms) across neighborhoods is significantly different from zero. The between-neighborhood cluster variance component (τ = 0.37, χ
2 = 257.33, df = 85,
p < 0.002) suggests significant variability, validating the use of hierarchical linear analysis. Three nested models were fitted to empirically test the aforementioned research questions. Model 1 includes only the level-1 control variables; Model 2 introduces the two main predictor variables (
Strong Network and
Weak Network); Models 3 incorporates the six contextual-level variables; Model 4 allows for the slope for
Weak Network to vary across neighborhoods, while others are fixed; and finally, Model 5 displays the cross-level interaction between
Weak Network and the proportion of foreign-born residents.
Table 1 summarizes the descriptive statistics. Results from running multilevel models are shown in
Table 2.
3. Result
The chi-square test (τ = 0.37, χ
2 = 257.33, df = 196,
p < 0.01) from the null model without any of the covariates showed significant variability in psychological distress across neighborhoods, confirming the validity of using hierarchical linear modeling. The intraclass correlation (ICC) indicates that about 3% of the variance is due to contextual effects. According to Model 1 in
Table 2, a number of control variables are found to be significantly related to the outcome variable. Among the sociodemographic characteristics, social status is negatively related: the higher the status, the fewer the depressive symptoms (
p < 0.05). Being married also contributes to better mental health, albeit only at a moderate level (
p < 0.1). Personality also matters, as individuals who identify themselves as being extroverted exhibit lower levels of depression (
p < 0.05). The social capital variables also emerge as protective factors. Getting involved in local community meetings is negatively associated with psychological distress (
p < 0.05), and those who are more willing to trust generalized others (strangers) are less depressed (
p < 0.01). Net of these confounders, we now turn to Model 2 to examine whether regular social interaction with strong or close ties (family and friends) and with weak or distant ties (acquaintances and coworkers) has a distinct relationship with mental health. Findings indicate that indeed this is the case. First of all, with the inclusion of these two main predictors, the relatively weak connection between depressive symptoms and marital status disappears. The size and magnitude of other background factors remain more or less the same. With respect to the main focus of this paper, the analysis shows that interaction with distant contacts (
Weak Network) is significantly and positively related to psychological wellbeing (
p < 0.05). Interacting with close contacts (
Strong Network), however, turns out to be a non-significant factor.
How do neighborhood-level characteristics affect the status of individual mental health? We turn to Model 3 to address this question. Among the six variables, only
Collective Efficacy is found to have a moderate effect (
p < 0.1). Specifically, living in a neighborhood where residents feel a greater degree of social cohesion is positively related to mental health, while controlling for a host of individual-level factors. Even after incorporating the contextual effects, the negative relationship between weak ties and depression remains robust. The last question to be explored is whether this network-health linkage is constant or shifts across neighborhood quality? To do so, the slope for
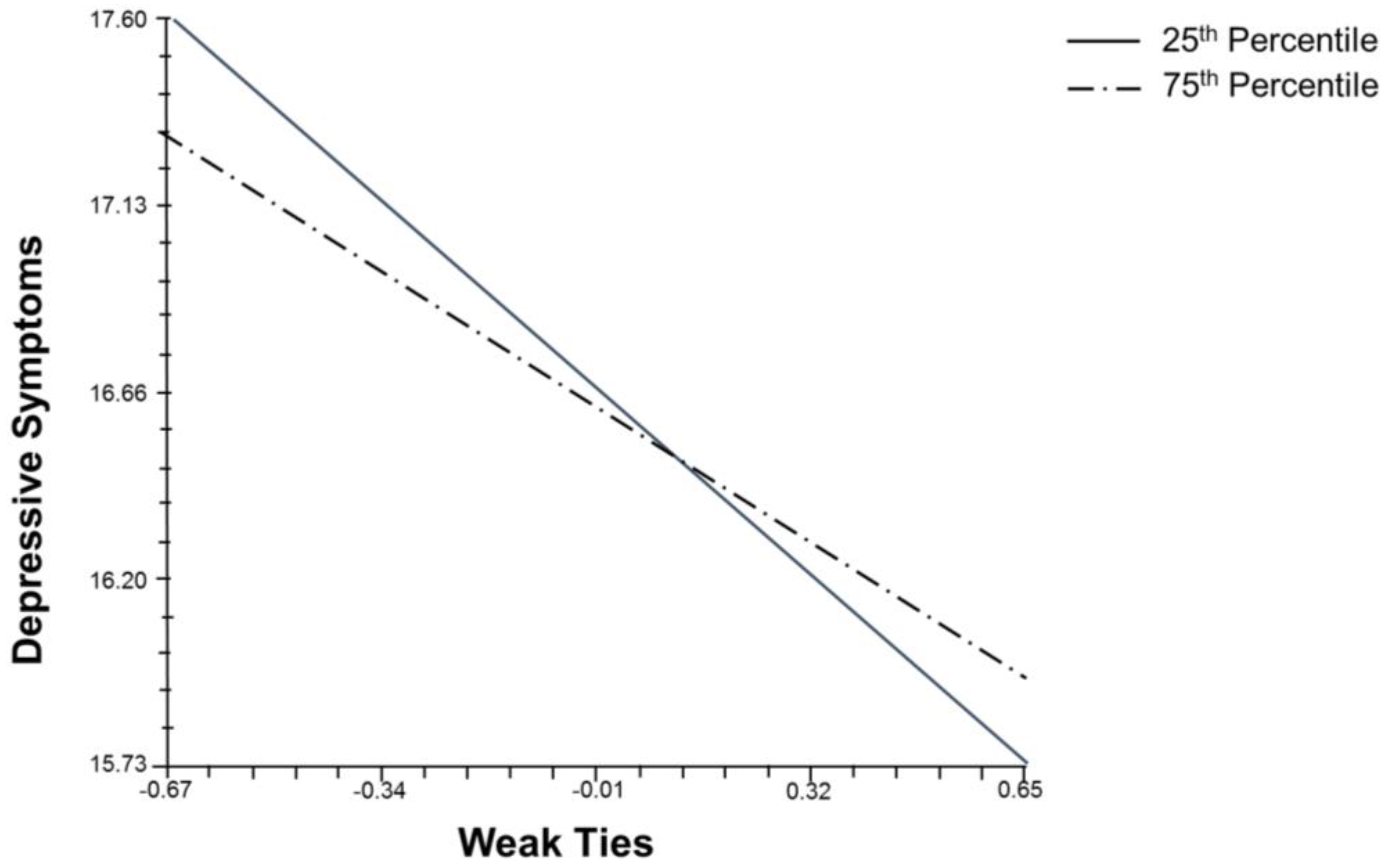
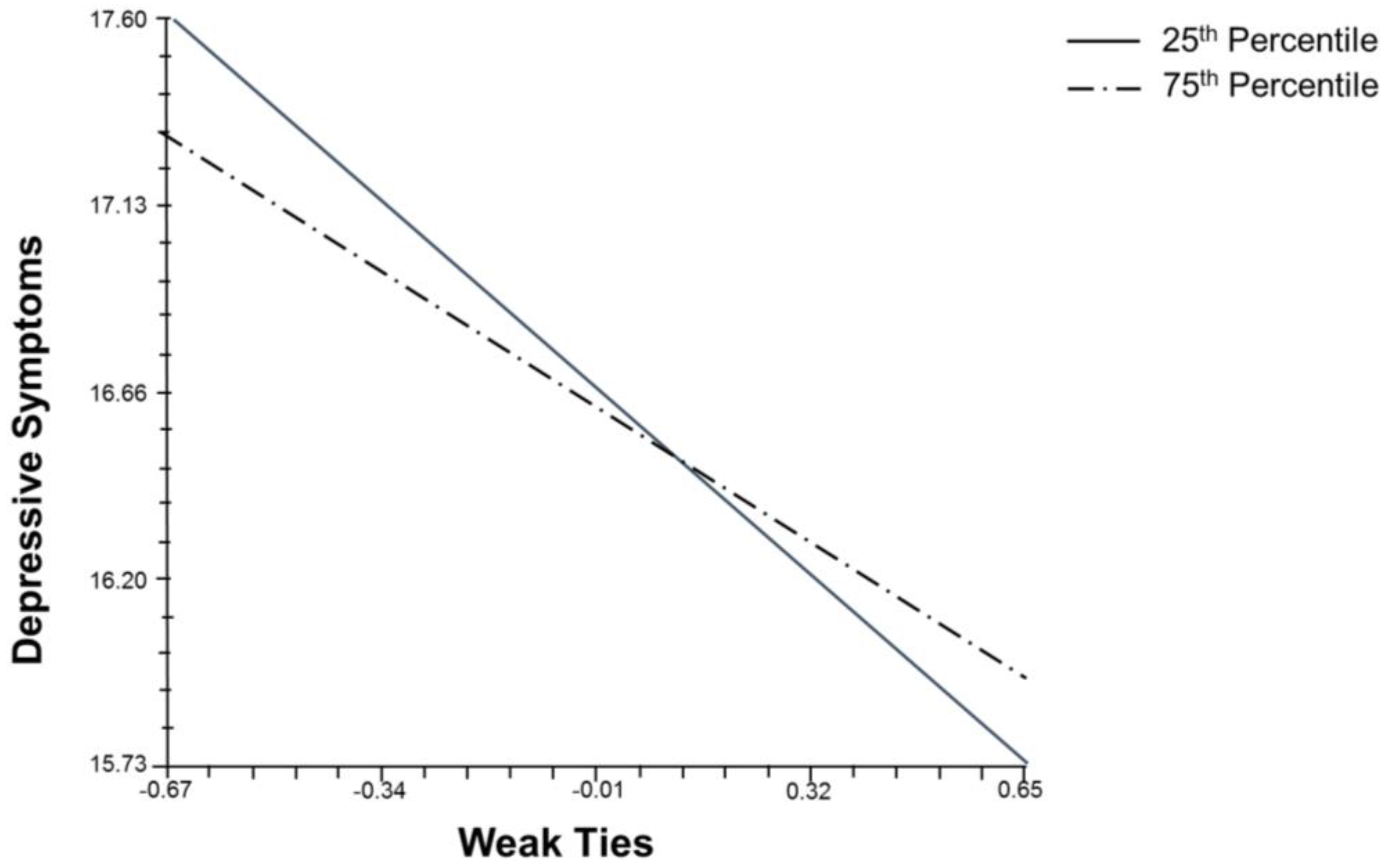
Weak Network is allowed to vary across the neighborhoods. Model 4 shows that the association between interactions with non-kin members and friends (close contacts) and depressive symptoms is partly a function of neighborhood context. To further investigate this, a series of cross-level interaction models (not shown) were estimated. Among them, only one was found to be significant, as illustrated in Model 5. According to this model, the proportion of foreigners significantly moderates the inverse association between the number of weak contacts and that of depressive symptoms. Specifically, weakly tied social networks serve a protective role. However, this role becomes less pronounced in neighborhoods with more immigrants.
Figure 1 graphically captures this contingent relationship based on results from Model 5 (while holding other variables at their means). The independent variable has been standardized, and the two lines correspond to 25th and 75th percentile scores for the proportion of foreigners. The negative slope for the higher percentile score (greater presence of foreigners) is less steep, meaning that the protective role of weak ties is diminished in a neighborhood with more non-native residents.
4. Discussion
Since Durkheim’s path-breaking analysis, there has been a substantial and growing volume of scholarly writings on the role of social ties in protecting and promoting mental health of individuals (
Berkman et al. 2000). Theoretical attempts have been made to map out “the social structure of suicide” based on Durkheim’s conceptual categories (
Bearman 1991). In addition, the empirical literature on “sociology of suicide” (
Wray et al. 2011) has a clearly recognizable Durkheimian influence. A huge interdisciplinary literature exists today based on the assumption that being socially connected has significant health benefits. Despite the overwhelming amount of findings, however, the literature on sociology of health is devoid of a clear consensus on why and how social relationships are important. This study’s primary aim was to contribute to the ongoing discourse on potential mechanisms underlying the network-health nexus. To what extent are strong and weak ties uniquely related to psychological distress and how are such associations moderated by neighborhood characteristics? By analyzing a probability sample of Korean adults nested in different neighborhood contexts, this paper sought to address these questions. Strong ties based on closeness and intimacy were hypothesized to provide more emotional support. In comparison, consistent with the general social network literature (
Granovetter 1973;
Burt 2005), weak ties were hypothesized to be more instrumental in channeling information benefits. Multilevel analysis reveals that, when it comes to the Korean adult population, social interaction with a greater number of weak, as opposed to strong, ties is associated with fewer depressive symptoms. Even after adjusting for a host of confounders, at both individual and contextual levels, this relationship holds.
How can we make sense of this core finding that points to the “strength of weak ties?” Unlike strong ties, acquaintances, neighbors, coworkers, etc. are structurally better situated to offer advice, information and tips that are fresh and therefore more valuable. This, in a nutshell, is the argument put forth by Granovetter more than four decades ago, which continues to inform research on economic sociology and beyond. In addition, it is this non-redundancy of information that ultimately translates into higher mental wellbeing, as the findings of this study demonstrate. Weak ties are akin to bridging social capital in that they can fill information and resource gaps across otherwise disconnected network contacts. An individual, in other words, is more likely to obtain the latest news and trends in healthy living from a weak tie. S/he can also access better information about seeking the right therapy when in need. The assistance flowing from a family member or a friend, though well-intended, may be old news and, as a result, limited in value. This may be one of the great ironies of social life: Those who are close to you want to help, yet it is the (often unintended) help obtained from those who are more relationally distant that really matters in the end.
There is the additional issue of obligatory reciprocity, which is absent in weak relationships. A healthy tip overheard from a friend of a friend comes “with no strings attached.” A piece of advice given by a strong tie, on the other hand, may come “with a price.” In the latter instance, the recipient is often expected to return the favor, which can be a source of burden and stress. The patterns of give-and-take interactions within close or strong networks resemble what Marcel Mauss (
Mauss 1990), incidentally Durkheim’s best-known student and nephew, refers to as the “gift exchange,” where participating members are expected to not only give and receive but also reciprocate. It is for this very reason that “social support may also entail psychological costs in the sense of indebtedness and obligations” (
Kawachi and Berkman 2001, p. 462). Put another way, in the Durkheimian language, tightly-knit social structures may produce “over-regulation” due to relational pressures to conform. In fact, studies have shown that relational embeddedness does not, by definition, imply better health outcomes (
Kawachi and Berkman 2001;
Umberson and Montez 2010). In Korea, a country steeped in the Confucian tradition that, above all else, stresses relational harmony, interaction with strong ties can impose emotional stress from having to meet the needs and demands of others. It is not surprising that in this particular Asian context, it pays to have more weak ties that can provide health benefits without the reciprocal obligations that customarily accompany familial and other strong ties. In addition, weak ties may be instrumental in providing informal psychological counseling. Traditionally, seeking professional help outside the family has been socially disapproved in Korea. Confiding in non-kin members about personal matters may thus be functionally equivalent to visiting a psychiatrist. In western societies, individuals have the freedom to seek therapy sessions in diagnosing and treating mental and emotional problems. By contrast, Koreans are much more prone to address them in a non-professional or informal context, i.e., via social interaction.
That the health benefits of weak ties fluctuate according to the size of non-native population at the neighborhood level is the other major finding in this study. For a long time, Korea was a labor-exporting country. In the wake of its rapid economic development during the past several decades, the country has increasingly become a popular destination for international migrants, especially from South East Asian countries (
Lie 2014). Given the steady rise of immigrant populations, Korea’s once ethnically monolithic residential neighborhoods have become more diverse in demographic makeup. As with other host societies, Korea now consists of neighborhoods that vary in terms of different levels of foreign-born residents. Ethnic diversity measures, such as the one used in this study, have been used in previous research to examine social cohesion and other contextual effects (
Van der Meer and Tolsma 2014). Much of this research based on Western cases rests on the assumption that the presence of ethnic and/or racial minorities (immigrants) is associated with lower-quality or more inferior residential context.
With respect to the purposes of this study, it is fair to assume that for the most part, in comparison with their native counterparts, immigrants lack some of the human capital necessary for successful socioeconomic attainment. Moreover, members of ethnic enclaves, who tend to interact with “similar others” or fellow immigrants, also lack proper networks to mainstream society required for upward mobility. In other words, all things being equal, immigrant social networks may not be as effective as native social networks in relation to, among others, maintaining and promoting health. In addition, this has critical implications for the native (i.e., “Korean’) residents living in communities characterized by high levels of ethnic heterogeneity. In contrast to someone embedded in a community consisting of predominantly natives, a person in an ethnically heterogeneous setting is, by default, more likely to meet and interact with non-natives. If so, that person would have greater chances of receiving health-related information from non-native members of community that are, on average, poorer in quality. As this study has shown, knowing and interacting with weak ties have a positive association with mental health, an association that diminishes in a neighborhood inhabited by more non-natives. This decline makes sense in light of the fact that ties to immigrants are not as helpful as (or more inferior to) those to Korean natives.
What are the implications of these findings for the general literature on “social determinants of health?” First and foremost, a main lesson is that not all social ties are the same. In fact, depending on their types (strengths), they manifest themselves differently in influencing health outcomes. The common practice of using “network size” as a general proxy for social capital, therefore, should be reexamined. The key is not how many people one is connected to but who those contacts are exactly. Specifying the identities of network alters would allow for a closer examination of why networks operate the way they do. Networks (i.e., strong ties) can, on the one hand, channel emotional support and encouragement during times of a personal crisis. On the other hand, they (i.e., weak ties) can also provide important and novel information in dealing with health-related problems. Keeping network types analytically distinct is thus critical in understanding the mechanisms underlying their health benefits. A fundamental fact of life, which has not been adequately explored in the sociology of health literature, is that human relationships are a double-edge sword characterized by both rewards/benefits and costs/liabilities. Focusing only on the quantitative aspect of network relations precludes analyzing why, how and when some relationships are salubrious while others are deleterious. Unpacking qualitative dimensions of human interactions would pave the way for researchers to probe divergent ways in which people’s respective interpersonal world affects, and is affected by, their health conditions.
It is also important to recognize that the network-health relationship is not constant but subject to vary across contextual factors. Where we live has a profound impact on our mental health and psychological wellbeing. Residential characteristics can influence our health directly, as in living in a community with fresh air, accessible medical care, low crime, helpful neighbors, etc. They can also have a more indirect effect, as the current study has demonstrated, by either strengthening or weakening the associations between social networks and health outcomes. Stress buffering has been suggested as a primary means by which “significant others” provide protection against health-damaging factors. This mechanism of influence is partly a function of broader environmental qualities and forces. Many studies in the literature overly emphasize the positive role of neighborhood social capital (collective efficacy, social cohesion, etc.). How neighborhood disadvantages (e.g., aggregate poverty, proportion of ethnic minorities) interact with individual-level networks can reveal deeper insights into the complex interplay between “micro-” “meso-” and “macro-” level variables in shaping health inequalities.
5. Conclusions
In closing, the current research demonstrates that weak ties can be strong in providing health benefits, with respect to the Korean population. Contextual moderating effect is also found, as the network-depression relationship varies according to the neighborhood ethnic makeup. This study has some limitations and, as a result, the reported findings must be interpreted with caution. As is the case with all research based on cross-sectional data, causality cannot be inferred between network measures and mental health outcome in this research. The inherent endogeneity problem suggests that the direction of causation can flow in the opposite direction: that is, healthier people are more active in social interactions, not vice versa. Another likelihood is that health conditions and social interactions mutually influence each other, a dynamic process that cannot be examined within the confines of the data analyzed herein. Unlike lab-based psychological research involving “small N,” collecting experimental data would be virtually impossible given the logistical and ethical issues involved. As the next best option, longitudinal observational surveys should be designed to minimize, though not resolve, this methodological issue. Like all general social surveys, KGSS (
Kim 2012) contains egocentric, not sociocentric, network data. As a result, the analysis is limited to the number of contacts, the frequency of interaction, etc. The availability of sociocentric data would make it possible to construct variables related to network positions and structures, which can reveal more interesting results concerning the health benefits of social networks or lack thereof.
Another limitation is that the KGSS questionnaire taps “potential,” not actualized, social capital. Network measures for this study were based on respondents’ interactions with strong and weak ties, with the assumption that health-related information and resources are channeled through them. Yet, this may or may not be the case. As has been suggested, the name-generator item about discussing “important matters” may exclude, or only partly include, health-related matters. That is, people talk to specific others about specific issues (
Perry and Pescosolido 2010). Future research would benefit from specifying the contents of network flows for a more accurate causal analysis. Finally, the concept of a “neighborhood” has been elusive, to say the least, prompting scholars to suggest multiple, often conflicting, definitions (
Sharkey and Faber 2014). One major concern here is the proper level of measurement. Previous studies have frequently relied on census tracts and other derivative concepts. The similarly conceptualized neighborhood units in the KGSS may not fully capture people’s surroundings and their impact on health. More precise measures are needed to better understand the ways in which context matters. Another related concern is the varying numbers of respondents in each cluster (neighborhood unit), which can affect the parameter estimates as reported in multilevel models. Limitations notwithstanding, the current study offers nuanced findings and raises pertinent questions about social networks and mental health in East Asia and beyond.




{kind=link}