Association of TLR4 Polymorphisms, Expression, and Vitamin D with Helicobacter pylori Infection



Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Genomic DNA Extraction and Genotyping Assays
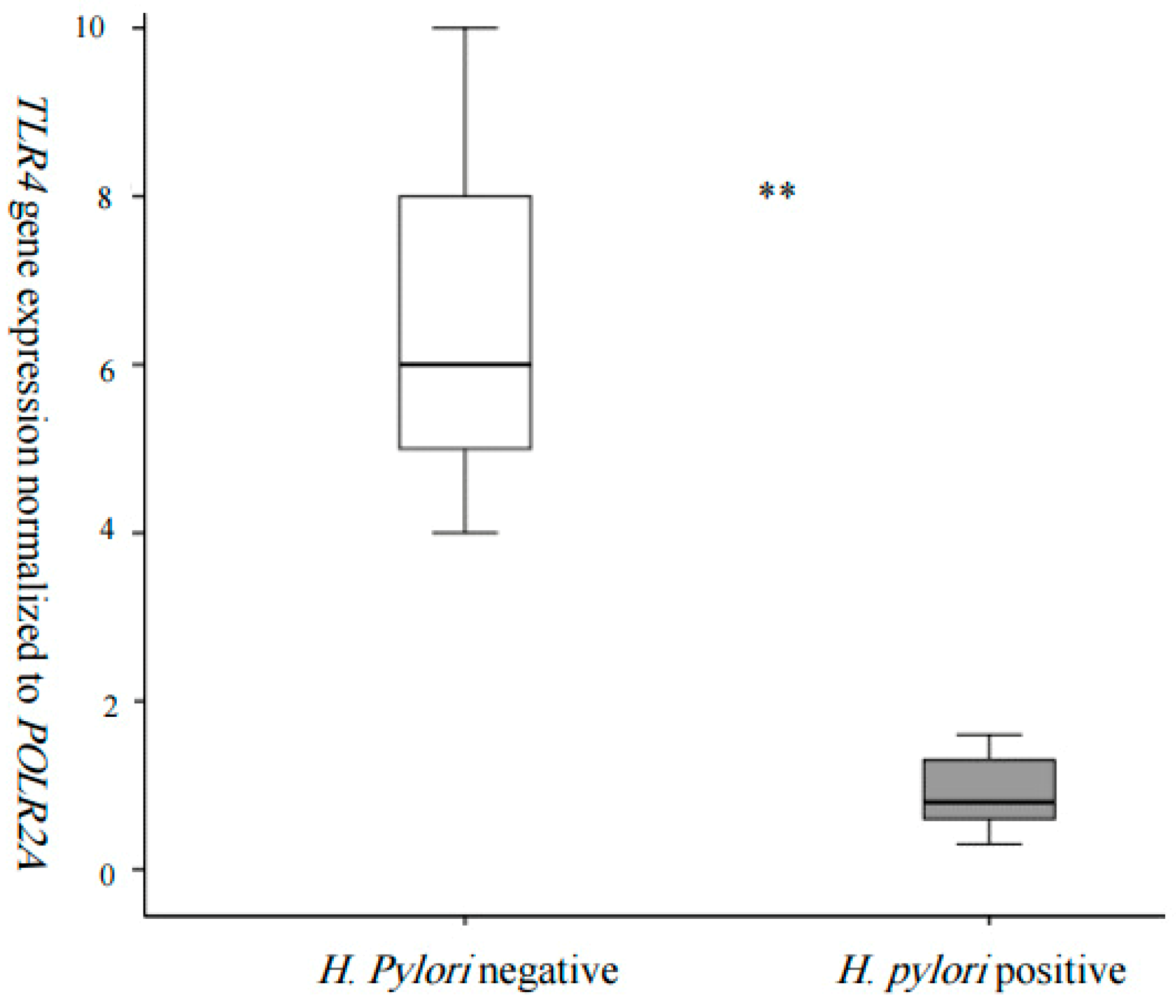
2.4. TLR4 Expression in White Blood Cells
2.5. Statistical Analyses
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Burucoa, C.; Axon, A. Epidemiology of Helicobacter pylori infection. Helicobacter 2017, 22 (Suppl. 1). [Google Scholar] [CrossRef] [PubMed]
- Naja, F.; Nasreddine, L.; Hwalla, N.; Moghames, P.; Shoaib, H.; Fatfat, M.; Sibai, A.; Gali-Muhtasib, H. Association of H. pylori infection with insulin resistance and metabolic syndrome among Lebanese adults. Helicobacter 2012, 17, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Kusters, J.G.; van Vliet, A.H.; Kuipers, E.J. Pathogenesis of Helicobacter pylori infection. Clin. Microbiol. Rev. 2006, 19, 449–490. [Google Scholar] [CrossRef]
- Pachathundikandi, S.K.; Lind, J.; Tegtmeyer, N.; El-Omar, E.M.; Backert, S. Interplay of the Gastric Pathogen Helicobacter pylori with Toll-Like Receptors. Biomed. Res. Int. 2015, 2015, 192420. [Google Scholar] [CrossRef] [PubMed]
- Tongtawee, T.; Bartpho, T.; Kaewpitoon, S.; Kaewpitoon, N.; Dechsukhum, C.; Leeanansaksiri, W.; Loyd, R.A.; Talabnin, K.; Matrakool, L.; Panpimanmas, S. Genetic polymorphisms in TLR1, TLR2, TLR4, and TLR10 of Helicobacter pylori-associated gastritis: A prospective cross-sectional study in Thailand. Eur. J. Cancer Prev. 2018, 27, 118–123. [Google Scholar] [CrossRef]
- Mayerle, J.; den Hoed, C.M.; Schurmann, C.; Stolk, L.; Homuth, G.; Peters, M.J.; Capelle, L.G.; Zimmermann, K.; Rivadeneira, F.; Gruska, S.; et al. Identification of genetic loci associated with Helicobacter pylori serologic status. JAMA 2013, 309, 1912–1920. [Google Scholar] [CrossRef]
- Hishida, A.; Matsuo, K.; Goto, Y.; Mitsuda, Y.; Naito, M.; Wakai, K.; Tajima, K.; Hamajima, N. Significant association of RUNX3 T/A polymorphism at intron 3 (rs760805) with the risk of gastric atrophy in Helicobacter pylori seropositive Japanese. J. Gastroenterol. 2009, 44, 1165–1171. [Google Scholar] [CrossRef]
- Karhukorpi, J.; Yan, Y.; Niemela, S.; Valtonen, J.; Koistinen, P.; Joensuu, T.; Saikku, P.; Karttunen, R. Effect of CD14 promoter polymorphism and H. pylori infection and its clinical outcomes on circulating CD14. Clin. Exp. Immunol. 2002, 128, 326–332. [Google Scholar] [CrossRef]
- Castano-Rodriguez, N.; Kaakoush, N.O.; Goh, K.L.; Fock, K.M.; Mitchell, H.M. The role of TLR2, TLR4 and CD14 genetic polymorphisms in gastric carcinogenesis: A case-control study and meta-analysis. PLoS ONE 2013, 8, e60327. [Google Scholar] [CrossRef]
- Kang, T.J.; Chae, G.T. Detection of Toll-like receptor 2 (TLR2) mutation in the lepromatous leprosy patients. FEMS Immunol. Med. Microbiol. 2001, 31, 53–58. [Google Scholar] [CrossRef] [Green Version]
- Du, C.; Yang, S.; Zhao, X.; Dong, H. Pathogenic roles of alterations in vitamin D and vitamin D receptor in gastric tumorigenesis. Oncotarget 2017, 8, 29474–29486. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Chen, W.; Zhu, H.; Chen, Y.; Wan, X.; Yang, N.; Xu, S.; Yu, C.; Chen, L. Helicobacter pylori induces increased expression of the vitamin D receptor in immune responses. Helicobacter 2014, 19, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.T.; Stenger, S.; Li, H.; Wenzel, L.; Tan, B.H.; Krutzik, S.R.; Ochoa, M.T.; Schauber, J.; Wu, K.; Meinken, C.; et al. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science 2006, 311, 1770–1773. [Google Scholar] [CrossRef] [PubMed]
- Assaad, S.; Chaaban, R.; Tannous, F.; Costanian, C. Dietary habits and Helicobacter pylori infection: A cross sectional study at a Lebanese hospital. BMC Gastroenterol. 2018, 18, 48. [Google Scholar] [CrossRef] [PubMed]
- Alghalyini, B.; El Shamieh, S.; Salami, A.; Visvikis Siest, S.; Fakhoury, H.M.; Fakhoury, R. Effect of SLCO1B1 gene polymorphisms and vitamin D on statin-induced myopathy. Drug Metab. Pers. Ther. 2018, 33, 41–47. [Google Scholar] [CrossRef] [PubMed]
- El Shamieh, S.; Costanian, C.; Kassir, R.; Visvkis-Siest, S.; Bissar-Tadmouri, N. Apoe genotypes in lebanon: Distribution and association with hypercholesterolemia and alzheimer’s disease. Per. Med. 2019, 16, 15–23. [Google Scholar] [CrossRef]
- Hosoda, K.; Shimomura, H.; Wanibuchi, K.; Masui, H.; Amgalanbaatar, A.; Hayashi, S.; Takahashi, T.; Hirai, Y. Identification and characterization of a vitamin D3 decomposition product bactericidal against Helicobacter pylori. Sci. Rep. 2015, 5, 8860. [Google Scholar] [CrossRef]
- Nasri, H.; Baradaran, A. The influence of serum 25-hydroxy vitamin D levels on Helicobacter pylori Infections in patients with end-stage renal failure on regular hemodialysis. Saudi J. Kidney Dis. Transplant. 2007, 18, 215–219. [Google Scholar]
- Yildirim, O.; Yildirim, T.; Seckin, Y.; Osanmaz, P.; Bilgic, Y.; Mete, R. The influence of vitamin D deficiency on eradication rates of Helicobacter pylori. Adv. Clin. Exp. Med. 2017, 26, 1377–1381. [Google Scholar] [CrossRef]
- Wanibuchi, K.; Hosoda, K.; Ihara, M.; Tajiri, K.; Sakai, Y.; Masui, H.; Takahashi, T.; Hirai, Y.; Shimomura, H. Indene Compounds Synthetically Derived from Vitamin D Have Selective Antibacterial Action on Helicobacter pylori. Lipids 2018, 53, 393–401. [Google Scholar] [CrossRef]
- Singh, K.; Gandhi, S.; Batool, R. A Case-Control Study of the Association between Vitamin D Levels and Gastric Incomplete Intestinal Metaplasia. Nutrients 2018, 10, 629. [Google Scholar] [CrossRef] [PubMed]
- Fleet, J.C.; DeSmet, M.; Johnson, R.; Li, Y. Vitamin D and cancer: A review of molecular mechanisms. Biochem. J. 2012, 441, 61–76. [Google Scholar] [CrossRef] [PubMed]
- Ren, C.; Qiu, M.Z.; Wang, D.S.; Luo, H.Y.; Zhang, D.S.; Wang, Z.Q.; Wang, F.H.; Li, Y.H.; Zhou, Z.W.; Xu, R.H. Prognostic effects of 25-hydroxyvitamin D levels in gastric cancer. J. Transl. Med. 2012, 10, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karttunen, T.J.; Niemela, S.; Kerola, T. Blood leukocyte differential in Helicobacter pylori infection. Dig. Dis. Sci. 1996, 41, 1332–1336. [Google Scholar] [CrossRef] [PubMed]
- Kondo, Y.; Joh, T.; Sasaki, M.; Oshima, T.; Itoh, K.; Tanida, S.; Kataoka, H.; Ohara, H.; Nomura, T.; Itoh, M. Helicobacter pylori eradication decreases blood neutrophil and monocyte counts. Aliment. Pharmacol. Ther. 2004, 20 (Suppl. 1), 74–79. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, S.; Rumi, M.A.; Kadowaki, Y.; Ortega-Cava, C.F.; Yuki, T.; Yoshino, N.; Miyaoka, Y.; Kazumori, H.; Ishimura, N.; Amano, Y.; et al. Essential role of MD-2 in TLR4-dependent signaling during Helicobacter pylori-associated gastritis. J. Immunol. 2004, 173, 1406–1416. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.F., Jr.; Mitchell, A.; Li, G.; Ding, S.; Fitzmaurice, A.M.; Ryan, K.; Crowe, S.; Goldberg, J.B. Toll-like receptor (TLR) 2 and TLR5, but not TLR4, are required for Helicobacter pylori-induced NF-ĸB activation and chemokine expression by epithelial cells. J. Biol. Chem. 2003, 278, 32552–32560. [Google Scholar] [CrossRef]
- Kawahara, T.; Kuwano, Y.; Teshima-Kondo, S.; Kawai, T.; Nikawa, T.; Kishi, K.; Rokutan, K. Toll-like receptor 4 regulates gastric pit cell responses to Helicobacter pylori infection. J. Med. Investig. 2001, 48, 190–197. [Google Scholar]
- Sadeghi, K.; Wessner, B.; Laggner, U.; Ploder, M.; Tamandl, D.; Friedl, J.; Zügel, U.; Steinmeyer, A.; Pollak, A.; Roth, E.; et al. Vitamin D3 down-regulates monocyte TLR expression and triggers hyporesponsiveness to pathogen-associated molecular patterns. Eur. J. Immunol. 2006, 36, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Do, J.E.; Kwon, S.Y.; Park, S.; Lee, E.S. Effects of vitamin D on expression of Toll-like receptors of monocytes from patients with Behcet’s disease. Rheumatology (Oxford) 2008, 47, 840–848. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Helicobacter pylori | |||
|---|---|---|---|
| Positive (n = 225) | Negative (n = 235) | p | |
| Mean ± SD | Mean ± SD | ||
| Age (years) | 39.28 ± 13.9 | 41.86 ± 14.26 | 0.05 |
| Gender | |||
| Males, n (%) | 88 (39.1%) | 80 (34%) | 0.25 |
| Females, n (%) | 137 (60.9%) | 155 (66%) | |
| BMI Category | |||
| Normal | 109 | 128 | 0.12 |
| Overweight and Obese | 116 | 107 | |
| Education Level | |||
| Primary | 32 | 56 | 6 × 10−3 |
| School | 52 | 57 | |
| University | 141 | 122 | |
| Marital Status | |||
| Not Married | 70 | 69 | 0.38 |
| Married | 155 | 166 | |
| Alcohol consumption | |||
| No | 145 | 153 | 0.48 |
| Yes | 80 | 82 | |
| SBP (mmHg) | 131.03 ± 1.51 | 131.37 ± 1.64 | 0.05 |
| DBP (mmHg) | 6.78 ± 0.88 | 6.78 ± 0.93 | 0.47 |
| Glycemia (mg/dL) | 121 ± 46 | 95 ± 21 | 0.18 |
| Cholesterol (mmol/L) | 1.75 ± 0.41 | 1.87 ± 0.4 | 0.009 |
| TG (mmol/L) | 1.22 ± 0.92 | 1.68 ± 1.45 | 0.001 |
| HDL (mmol/L) | 0.46 ± 0.12 | 0.44 ± 0.16 | 0.13 |
| LDL (mmol/L) | 1.14 ± 0.34 | 1.2 ± 0.32 | 0.24 |
| VitD (ng/mL) | 18.04 ± 7.16 | 30.74 ± 15.66 | <1 × 10−3 |
| Insufficiency | 133 | 12 | <1 × 10−3 |
| Deficiency | 56 | 109 | |
| Normal | 15 | 107 | |
| Helicobacter pylori | |||
|---|---|---|---|
| OR | 95% C.I. | p | |
| Age | |||
| <40 years | 1 | ||
| ≥40 years | 0.73 | (0.33–1.62) | 0.44 |
| Gender | |||
| Male | 1 | ||
| Female | 0.7 | (0.37–1.32) | 0.02 |
| BMI category | |||
| Normal | 1 | ||
| Overweight and Obese | 1.49 | (0.82–2.72) | 0.19 |
| Education Level | |||
| Primary | 1 | ||
| School | 2.46 | (0.96–6.34) | 0.06 |
| University | 4.16 | (1.52–11.4) | 0.01 |
| Marital Status | |||
| Not Married | 1 | ||
| Married | 1.03 | (0.5–2.1) | 0.93 |
| Alcohol Consumption | |||
| No | 1 | ||
| Yes | 1.42 | (0.76–2.67) | 0.27 |
| Vitamin D status | |||
| Insufficiency | 1 | ||
| Deficiency | 0.03 | (0.01–0.06) | <1 × 10−3 |
| Normal | 0.01 | (0–0.02) | <1 × 10−3 |
| Gene SNPs | |||
| rs10004195 in TLR1 | 1.23 | (0.8–1.8) | 0.29 |
| rs10759932 in TLR4 | 1.37 | (0.75–2.48) | 0.30 |
| rs10983755 in TLR4 | 0.51 | (0.05–5.44) | 0.58 |
| rs11536889 in TLR4 | 1.51 | (0.82–2.79) | 0.19 |
| rs1898830 in TLR4 | 0.84 | (0.55–1.29) | 0.44 |
| rs4986790 in TLR4 | 7.09 | (1.12–45) | 0.04 |
| rs4986791 in TLR4 | 0.14 | (0.02–0.86) | 0.03 |
| rs2569190 in CD14 | 0.74 | (0.49–1.12) | 0.15 |
| rs760805 in RUNX3 | 0.78 | (0.53–1.15) | 0.21 |
| Vitamin D | |||||||
|---|---|---|---|---|---|---|---|
| SNP ID | Gene | Chr | position | n | β [95% C.I.] | S.E | p |
| rs4986790G>A | TLR4 | 9 | 117713024 | 456 | −0.371 [−0.112, −0.63] | 0.13 | 5 × 10−3 |
| rs4986791T>C | 117713324 | 457 | −0.4 [−0.14, −0.663] | 0.13 | 1 × 10−3 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assaad, S.; Costanian, C.; Jaffal, L.; Tannous, F.; Stathopoulou, M.G.; Shamieh, S.E. Association of TLR4 Polymorphisms, Expression, and Vitamin D with Helicobacter pylori Infection. J. Pers. Med. 2019, 9, 2. https://doi.org/10.3390/jpm9010002
Assaad S, Costanian C, Jaffal L, Tannous F, Stathopoulou MG, Shamieh SE. Association of TLR4 Polymorphisms, Expression, and Vitamin D with Helicobacter pylori Infection. Journal of Personalized Medicine. 2019; 9(1):2. https://doi.org/10.3390/jpm9010002
Chicago/Turabian StyleAssaad, Shafika, Christy Costanian, Lama Jaffal, Fida Tannous, Maria G. Stathopoulou, and Said El Shamieh. 2019. "Association of TLR4 Polymorphisms, Expression, and Vitamin D with Helicobacter pylori Infection" Journal of Personalized Medicine 9, no. 1: 2. https://doi.org/10.3390/jpm9010002