Community Engagement for Big Epidemiology: Deliberative Democracy as a Tool

Abstract
:1. Introduction
1.1. Why Is There a Demand for New Methodology in Community Engagement?
1.2. What is Deliberative Democracy?
1.3. Why Tasmania?
2. Methods
2.1. Recruitment

{kind=link}
{kind=link}
{kind=link}
| Demographic | Required | Achieved Stage 1 | Achieved Stage 2 | Selected | Participated in Event | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | Category | F | M | F | M | F | M | F | M | F | M |
| Location | Hobart | 2 | 2 | 19 | 9 | 6 | 4 | 9 | 5 | 8 | 3 |
| Other towns | 2 | 2 | 13 | 9 | 1 | 1 | 5 | 7 | 4 | 5 | |
| Rural | 2 | 2 | 21 | 7 | 0 | 0 | 5 | 5 | 4 | 1 | |
| Age | ≤30 years | 1 | 1 | 3 | 1 | 1 | 4 | 4 | 2 | 3 | 1 |
| >30 years | 1 | 1 | 50 | 24 | 6 | 1 | 15 | 15 | 13 | 8 | |
| Education | No university | 1 | 1 | 38 | 18 | 5 | 5 | 14 | 12 | 12 | 5 |
| University | 1 | 1 | 15 | 7 | 2 | 0 | 5 | 5 | 4 | 4 | |
| Employed | Yes | 1 | 1 | 17 | 8 | 7 | 3 | 11 | 11 | 9 | 6 |
| No | 1 | 1 | 36 | 17 | 0 | 2 | 8 | 6 | 7 | 3 | |
| Born in Australia | Yes | 1 | 1 | 40 | 21 | 6 | 3 | 13 | 12 | 11 | 6 |
| No | 1 | 1 | 13 | 4 | 1 | 2 | 6 | 5 | 5 | 3 | |
| Indigenous | Yes | 1 | 1 | 2 | 1 | 0 | 0 | 2 | 1 | 2 | 0 |
| No | 1 | 1 | 51 | 24 | 7 | 5 | 17 | 16 | 14 | 9 | |
| Genetic or serious medical condition | Yes | 1 | 1 | 24 | 14 | 0 | 0 | 7 | 10 | 7 | 5 |
| No | 1 | 1 | 29 | 11 | 7 | 5 | 12 | 7 | 9 | 4 | |
2.2. Information Provision
- Prior to the event
- (i)
- an information booklet mailed to participants (detailed [44]);
- (ii)
- a website (with links to relevant external websites);
- (iii)
- an invitation to participants to independently seek out information, and to discuss issues with their friends and family.
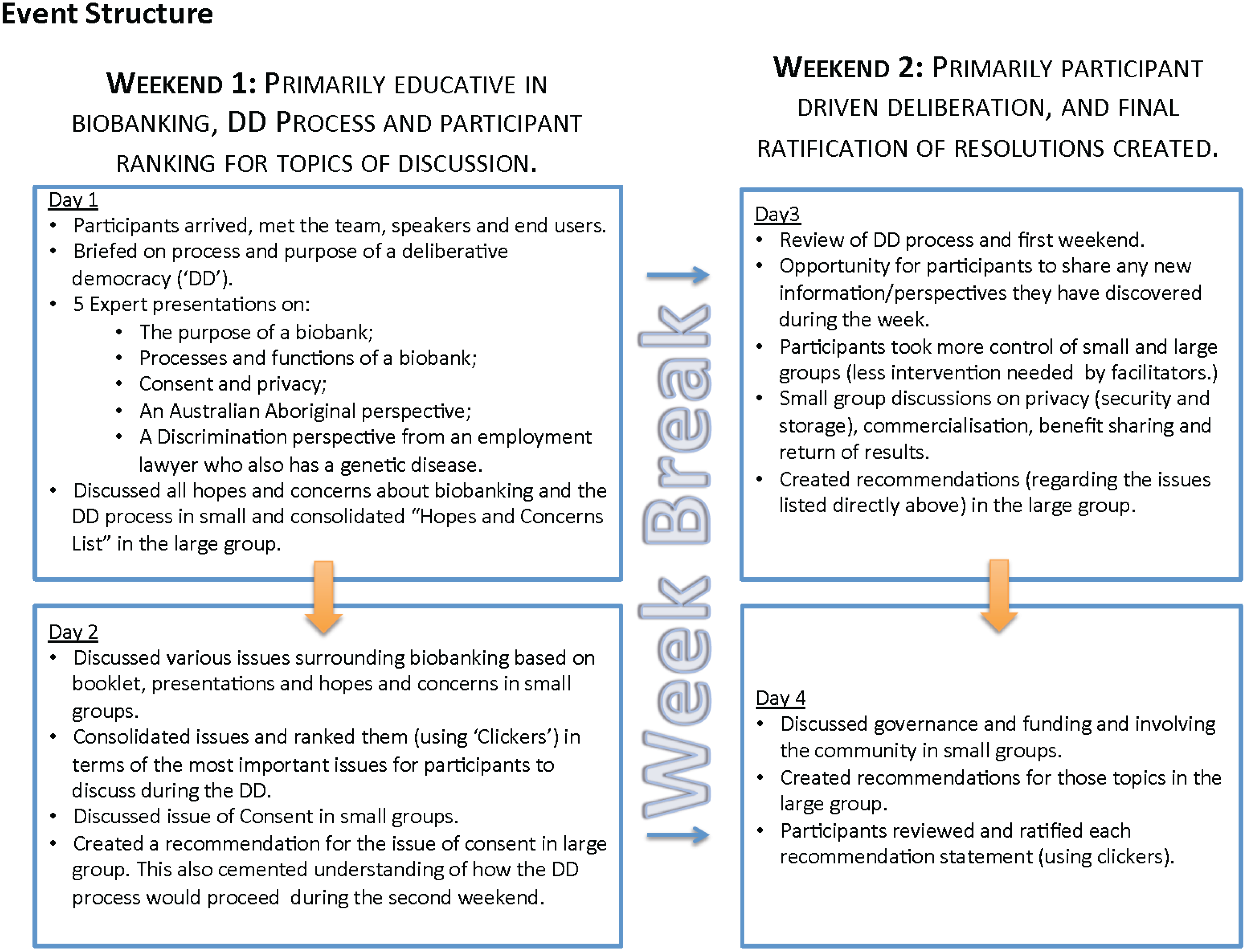
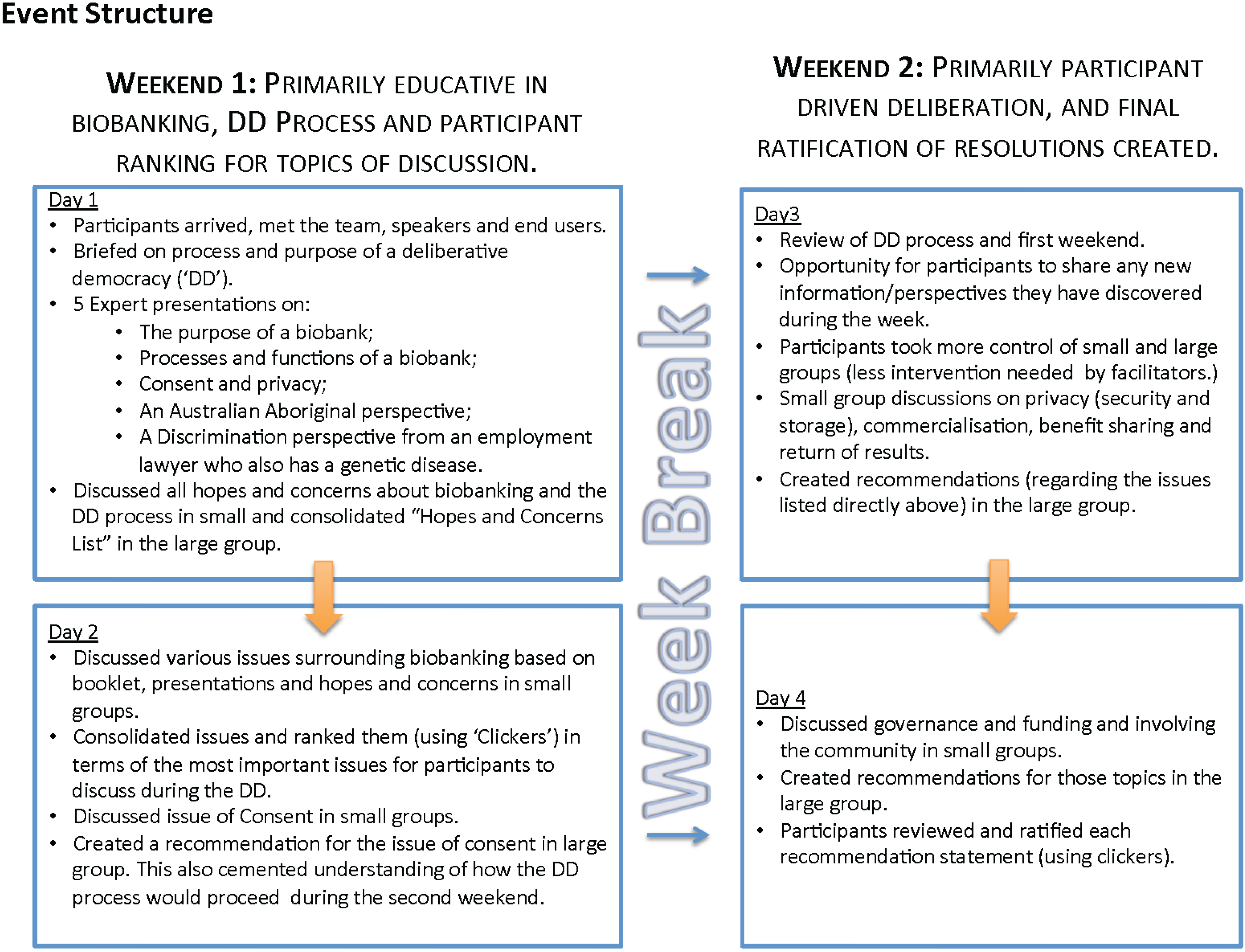
- During the event
- (i)
- informative presentations by five expert speakers representing the diverse perspectives of researchers (what is a biobank and the value of biobanks to genetic research), lawyers (presenting issues of privacy, consent and conflicts of interest), the indigenous community (autonomy and ethical issues) and those affected with a genetic disease (autonomy, genetic discrimination and other ethical issues); and
- (ii)
- a panel Q&A session, which included end users such as a representative from the Department of Health and Ageing and experts in genetics, law and biobanking [45].
2.3. Small and Large Group Format
2.4. End Users and Observers
2.5. Participant Satisfaction Surveys
2.6. Statistical Analyses Method
3. Results
3.1. Participants
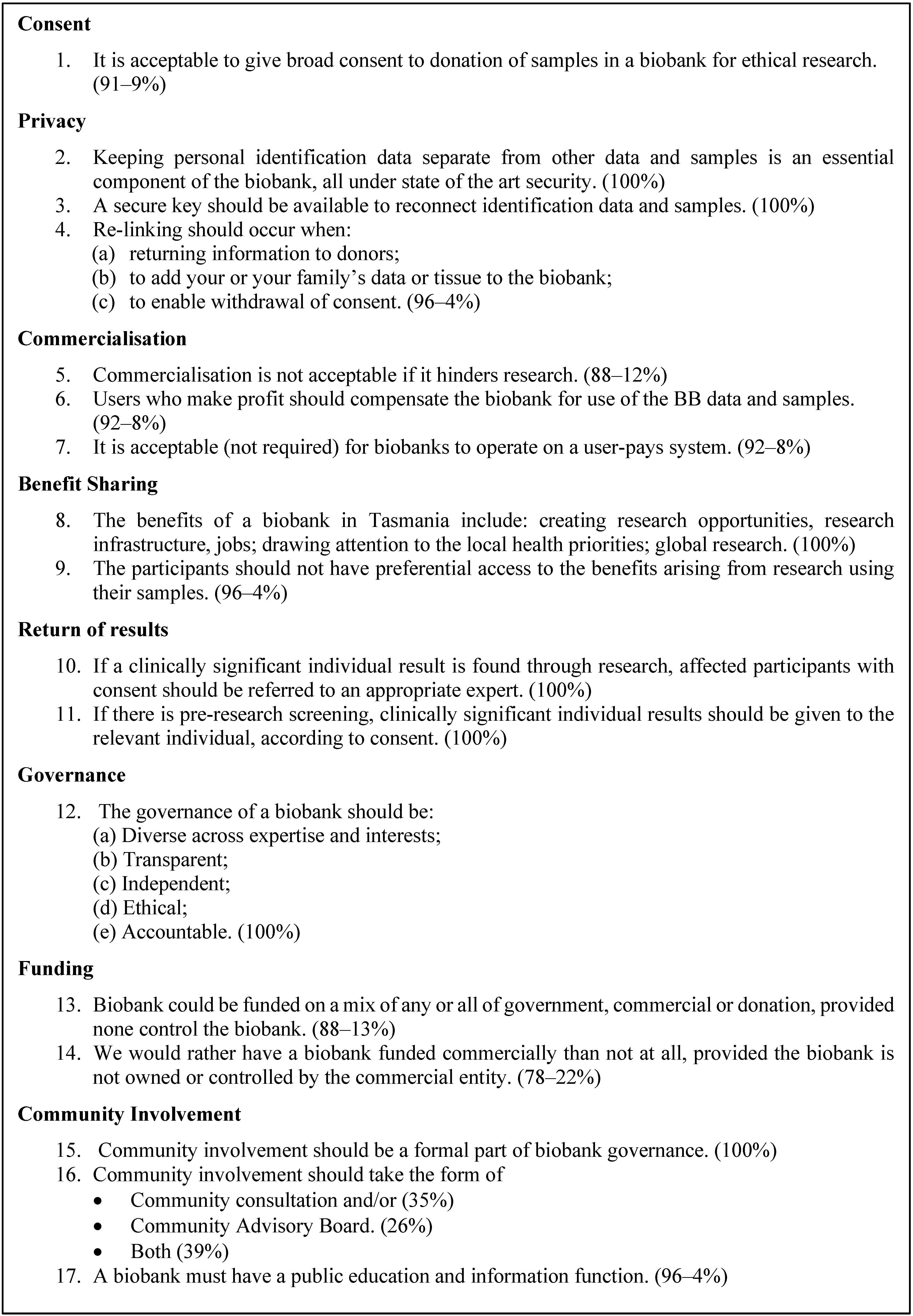
3.2. Outcomes
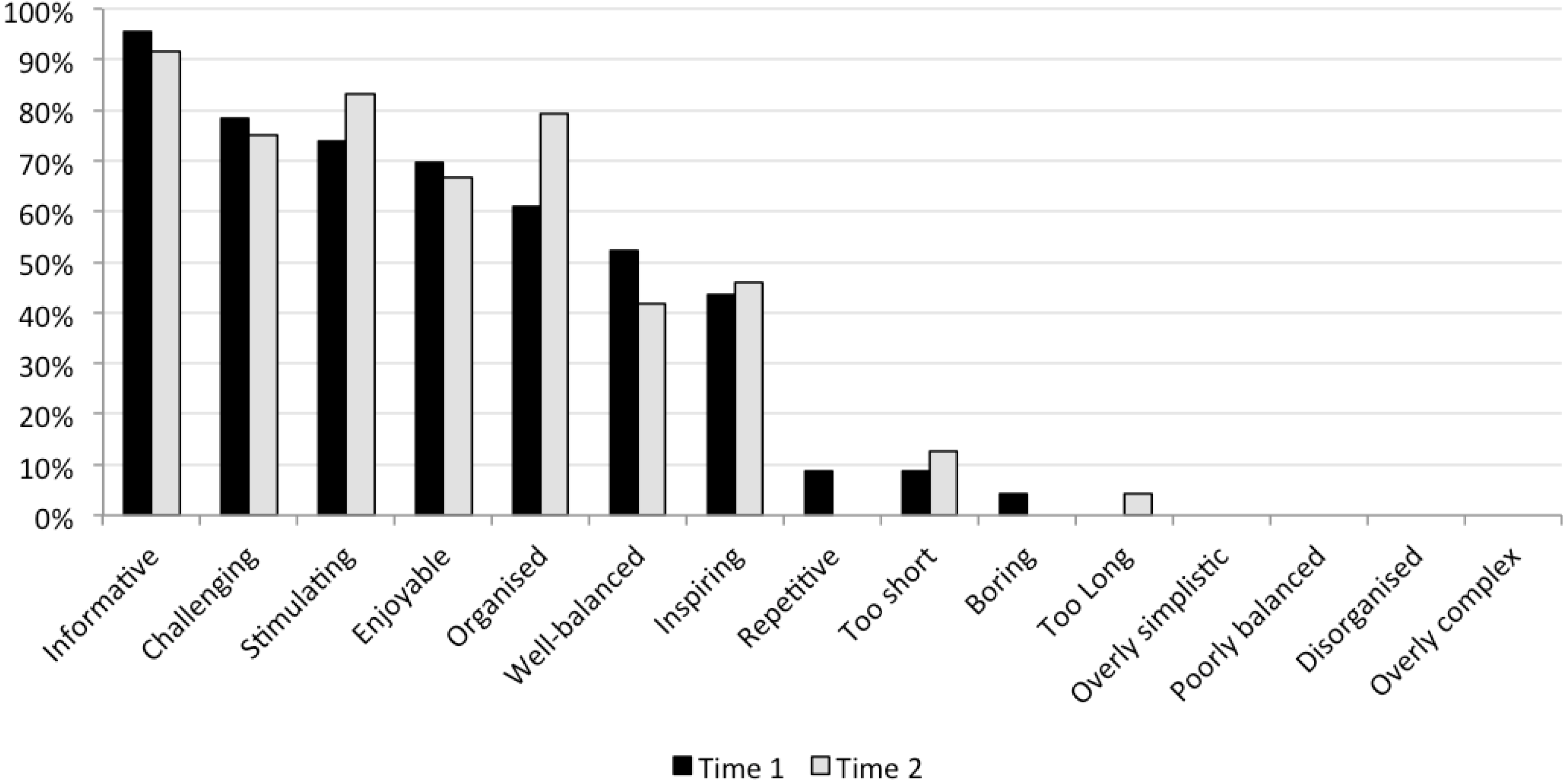
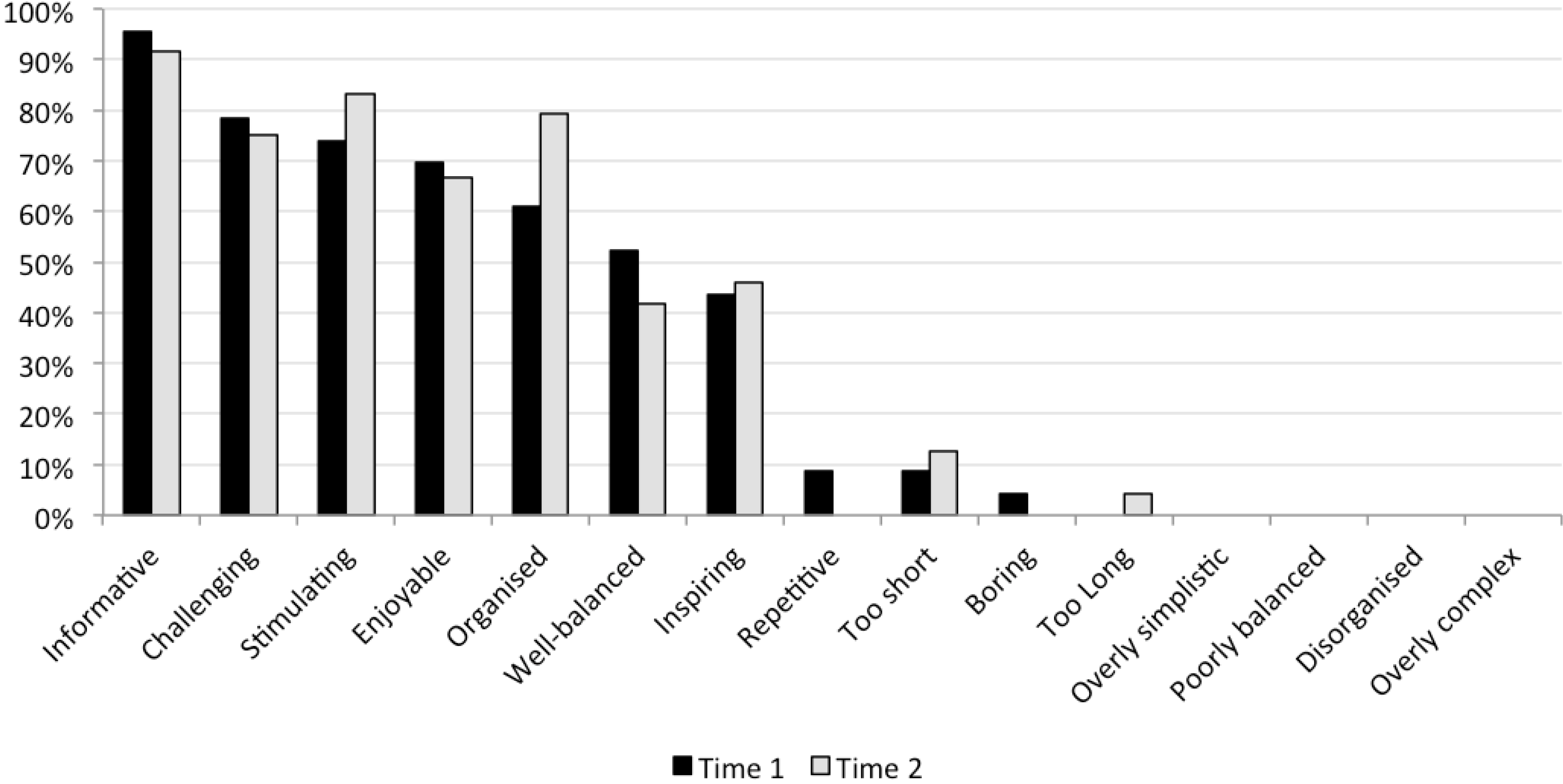
3.3. Participant Satisfaction Survey
| Trust | Time 1 | Time 2 | ||
|---|---|---|---|---|
| Median | Range | Median | Range | |
| Did you feel heard/listened to during the deliberation? a | 4 | (3–4) | 4 | (4–4) |
| Did you feel respected during the deliberation? a | 4 | (3–4) | 4 | (3–4) |
| Were the processes that led to the group’s recommendations fair? a | 4 | (2–4) | 4 | (3–4) |
| Were the processes that led to the group’s recommendations trustworthy? a | 4 | (3–4) | 4 | (3–4) |
| In your opinion, is it sensible for researchers to rely on a deliberative event like this when trying to develop Australian policy? e | 95.7% Yes | 4.3% No | 91.7% Yes | 4.2% No/ 4.2% DK |
| Outcomes | ||||
| How willing are you to abide by the group’s final position, even if you personally hold a different view? a | 4 | (2–4) | 4 | (3–4) |
| The group’s final recommendations addressed all issues considered important by participant s c | 3 | (1–4) | 3 | (1–4) |
| Intentions and Evaluation | ||||
| How likely is it that you would attend an event like this again in the future? d | 4 | (3–4) | 4 | (3–4) |
| How would you rate this deliberative event overall? b | 5 | (4–5) | 5 | (4–5) |
4. Discussion
5. Conclusions and Implications
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Rychetnik, L.; Carter, S.M.; Abelson, J.; Thornton, H.; Barratt, A.; Entwistle, V.A.; Mackenzie, G.; Salkeld, G.; Glasziou, P. Enhancing citizen engagement in cancer screening through deliberative democracy. J. Natl. Cancer Inst. 2013, 105, 380–386. [Google Scholar] [PubMed]
- Awadalla, P.; Boileau, C.; Payette, Y.; Idaghdour, Y.; Goulet, J.P.; Knoppers, B.; Hamet, P.; Laberge, C. Cohort profile of the CARTaGENE study: Quebec’s population-based biobank for public health and personalized genomics. Int. J. Epidemiol. 2013, 42, 1285–1299. [Google Scholar] [CrossRef] [PubMed]
- Manolio, T.A.; Collins, R. Vehement agreement on new models? Am. J. Epidemiol. 2013, 177, 290–291. [Google Scholar] [CrossRef] [PubMed]
- Toh, S.; Platt, R. Is size the next big thing in epidemiology? Epidemiology 2013, 24, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Hoeyer, K. The ethics of research biobanking: A critical review of the literature. Biotechnol. Genet. Eng. Rev. 2008, 25, 429–452. [Google Scholar]
- Hansson, M.G. Ethics and biobanks. Br. J. Cancer 2008, 100, 8–12. [Google Scholar] [CrossRef]
- Knoppers, B.M.; Zawati, M.H.; Kirby, E.S. Sampling populations of humans across the world: ELSI issues. Annu. Rev. Genomics Hum. Genet. 2012, 13, 395–413. [Google Scholar] [CrossRef] [PubMed]
- Bracken, M.B.; Baker, D.; Cauley, J.A.; Chambers, C.; Culhane, J.; Dabelea, D.; Dearborn, D.; Drews-Botsch, C.D.; Dudley, D.J.; Durkin, M.; et al. New models for large prospective studies: Is there a risk of throwing out the baby with the bathwater? Am. J. Epidemiol. 2013, 177, 285–289. [Google Scholar] [CrossRef]
- Marx, V. Biology: The big challenges of big data. Nature 2013, 498, 255–260. [Google Scholar] [CrossRef]
- Hernán, M.A.; Savitz, D.A. From “Big Epidemiology” to “Colossal Epidemiology”: When all eggs are in one basket. Epidemiology 2013, 24, 344–345. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, G.A. How big is big enough for epidemiology? Epidemiology 2007, 18, 18–20. [Google Scholar] [CrossRef] [PubMed]
- Burton, P.R.; Hansell, A.L.; Fortier, I.; Manolio, T.A.; Khoury, M.J.; Little, J.; Elliott, P. Size matters: Just how big is BIG? Quantifying realistic sample size requirements for human genome epidemiology. Int. J. Epidemiol. 2009, 38, 263–273. [Google Scholar] [CrossRef]
- Kohane, I.S.; Altman, R.B. Health-information altruists—A potentially critical resource. N. Engl. J. Med. 2005, 353, 2074–2077. [Google Scholar] [CrossRef] [PubMed]
- Winickoff, D.E. Genome and nation: Iceland’s health sector database and its legacy. Innovations 2006, 1, 80–105. [Google Scholar] [CrossRef]
- Gottweis, H.; Chen, H.; Starkbaum, J. Biobanks and the phantom public. Hum. Genet. 2011, 130, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, D.J.; Murphy-Bollinger, J.; Scott, J.; Hudson, K.L. Public opinion about the importance of privacy in biobank research. Am. J. Hum. Genet. 2009, 85, 643–654. [Google Scholar] [CrossRef] [PubMed]
- Lemke, A.A.; Wolf, W.A.; Hebert-Beirne, J.; Smith, M.E. Public and biobank participant attitudes toward genetic research participation and data sharing. Public Health Genomics 2010, 13, 368–377. [Google Scholar]
- Godard, B.; Marshall, J.; Laberge, C.; Knoppers, B.M. Strategies for consulting with the community: The cases of four large-scale genetic databases. Sci. Eng. Eth. 2004, 10, 457–477. [Google Scholar] [CrossRef]
- Chalmers, D.; Nicol, D.; Otlowski, M.; Critchley, C. Personalised medicine in the genome era. J. Law Med. 2013, 20, 577–594. [Google Scholar] [PubMed]
- Avard, D.; Bucci, L.M.; Burgess, M.M.; Kaye, J.; Heeney, C.; Farmer, Y.; Cambon-Thomsen, A. Public Health Genomics (PHG) and public participation: Points to consider. J. Public Delib. 2009, 5, 1–21. [Google Scholar]
- Wallace, H.M. The development of the UK biobank: Excluding scientific controversy from ethical debate. Crit. Public Health 2005, 15, 323–333. [Google Scholar] [CrossRef]
- Petersen, A. “Biobanks” “Engagements”: Engendering trust or engineering consent? Genomics Soc. Policy 2007, 3, 31–43. [Google Scholar] [CrossRef]
- Hoeyer, K.L.; Tutton, R. “Ethics was here”: Studying the language-games of ethics in the case of UK biobank. Crit. Public Health 2005, 15, 385–397. [Google Scholar] [CrossRef]
- O’Doherty, K.C.; Hawkins, A.K.; Burgess, M.M. Involving citizens in the ethics of biobank research: Informing institutional policy through structured public deliberation. Soc. Sci. Med. 2012, 75, 1604–1611. [Google Scholar] [CrossRef] [PubMed]
- Laws, R.; King, L.; Hardy, L.L.; Milat, A.; Rissel, C.; Newson, R.; Rychetnik, L.; Bauman, A.E. Utilization of a population health survey in policy and practice: A case study. Health Res. Policy Syst. 2013, 11, 1–11. [Google Scholar] [CrossRef] [PubMed]
- McWhirter, R.E.; Mununggirritj, D.; Marika, D.; Dickinson, L.J.; Condon, J.R. Ethical genetic research in indiginous communities: Challenges and successdul approaches. Trends Mol. Med. 2012, 18, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Dickert, N.; Sugarman, J. Ethical goals of community consultation in research. Am. J. Public Health 2005, 95, 1123–1127. [Google Scholar] [CrossRef]
- Chambers, S. Deliberative democracy theory. Annu. Rev. Polit. Sci. 2003, 6, 307–326. [Google Scholar] [CrossRef]
- Burgess, M.; O’Doherty, K.; Secko, D. Biobanking in British Columbia: A discussion of the future of personalized medicine through deliberative public engagement. Pers. Med. 2008, 5, 285–296. [Google Scholar] [CrossRef]
- Clayton, E.W.; Smith, M.; Fullerton, S.M.; Burke, W.; McCarty, C.A.; Koenig, B.A.; McGuire, A.L.; Beskow, L.M.; Dressler, L.; Lemke, A.A.; et al. Consent and community consultation working group of the eMERGE consortium. Confronting real time ethical, legal and social issues in the eMERGE (electonic Medical Records and Genomics) consortium. Genet. Med. 2010, 12, 616–620. [Google Scholar] [CrossRef]
- Molster, C.; Maxwell, S.; Youngs, L.; Kyme, G.; Hope, F.; Dawkins, H.; O’Leary, P. Blueprint for a deliberative public forum on biobanking policy: Were theoretical principles achievable in practice? Health Expect. 2013, 16, 211–224. [Google Scholar] [CrossRef]
- Secko, D.M.; Burgess, M.; O’Doherty, K. Perspectives on engaging the public in the ethics of emerging biotechnologies: From salmon to biobanks to neuroethics. Acc. Res. 2008, 15, 283–302. [Google Scholar] [CrossRef]
- Niemeyer, S. The emancipatory effect of deliberations: Empirical lessons from mini publics. Polit. Soc. 2011, 39, 103–140. [Google Scholar] [CrossRef]
- Longstaff, H.; Burgess, M.M. Recruiting for representation in public deliberation on the ethics of biobanks. Public Underst. Sci. 2010, 19, 212–224. [Google Scholar] [CrossRef] [PubMed]
- O’Doherty, K.C.; Burgess, M. Engaging the public on biobanks: Outcomes of the BC biobank deliberation. Public Health Genomics 2008, 12, 203–215. [Google Scholar]
- Rychetnik, L.; Carter, S.M.; Barratt, A.; Irwig, L. Expanding the evidence on cancer screening: The value of scientific, social and ethical perspectives. Med. J. Aust. 2013, 198, 536–539. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council (NHMRC). National Biobanking Strategy; NHMRC: Canberra, Australia, 2012. [Google Scholar]
- Gaskell, G.; Gottweis, H. Biobanks need publicity. Nature 2011, 471, 159–160. [Google Scholar] [CrossRef] [PubMed]
- FitzGerald, L.M.; Patterson, B.; Thomson, R.; Polanowski, A.; Quinn, S.; Brohede, J.; Thornton, T.; Challis, D.; Mackey, D.A.; Dwyer, T.; et al. Identification of a prostate cancer susceptibility gene on chromosome 5p13q12 associated with risk of both familial and sporadic disease. Eur. J. Hum. Genet. 2008, 17, 368–377. [Google Scholar]
- Mackey, D.A. Genetic eye research in tasmania: A historical overview. Clin. Exp. Ophthalmol. 2012, 40, 205–210. [Google Scholar] [CrossRef]
- Rubio, J.P.; Bahlo, M.; Butzkueven, H.; van der Mai, I.A.F.; Sale, M.M.; Dickinson, J.L.; Groom, P.; Johnson, L.J.; Simmons, R.D.; Tait, B.; et al. Genetic dissection of the human leukocyte antigen region by use od haplotypes of Tasmanians with multiple sclerosis. Am. J. Hum. Genet. 2002, 70, 1125–1137. [Google Scholar] [CrossRef] [PubMed]
- Brothers, C.R.D. Huntington’s chorea in Victoria and Tasmania. J. Neurol. Sci. 1964, 1, 405–420. [Google Scholar] [CrossRef] [PubMed]
- O’Doherty, K.C.; Hawkins, A. Structuring public engagement for effective input in policy development on human tissue biobanking. Public Health Genom. 2010, 13, 197–206. [Google Scholar] [CrossRef]
- Biobank Tasmania. Available online: http://www.tasbiobankproject.com (accessed on 1 November 2014).
- Chalmers, D.; McWhirter, R.E.; Nicol, D.; Whitton, T.; Otlowski, M.; Burgess, M.; Foote, S.J.; Critchley, C.; Dickinson, J.L. New avenues within community engagement: Addressing the ingenuity gap in our approch to health reserch and future provision of health care. J. Responsib. Innov. 2014. [Google Scholar] [CrossRef]
- O’Doherty, K.C.; Burgess, M.M.; Edwards, K.; Gallagher, R.P.; Hawkins, A.K.; Kaye, J.; McCaffrey, V.; Winickoff, D.E. From consent to institutions: Designing adaptive governance for genomic biobanks. Soc. Sci. Med. 2011, 73, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Molster, C.; Maxwell, S.; Youngs, L.; Potts, A.; Kyne, G.; Hope, F.; Dawkins, H.; O’Leary, P. An Australian approach to the policy translation of deliberated citizen perspectives on biobanking. Public Health Genomics 2012, 15, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Molster, C.; Potts, A.; Hope, F.; McNamara, B.; Youngs, L.; Maxwell, S.; Dawkins, H.; O’Leary, P. Informing public health policy through deliberative public engagement: Perceived impact on participants and citizen-government relations. Genet. Test. Mol. Biomark. 2013, 17, 713–718. [Google Scholar] [CrossRef]
- Street, J.; Duszynski, K.; Krawczuk, S.; Braunack-Mayer, A. The use of citizens’ juries in health policy decision-making: A systematic review. Soc. Sci. Med. 2014, 109, 1–9. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McWhirter, R.E.; Critchley, C.R.; Nicol, D.; Chalmers, D.; Whitton, T.; Otlowski, M.; Burgess, M.M.; Dickinson, J.L. Community Engagement for Big Epidemiology: Deliberative Democracy as a Tool. J. Pers. Med. 2014, 4, 459-474. https://doi.org/10.3390/jpm4040459
McWhirter RE, Critchley CR, Nicol D, Chalmers D, Whitton T, Otlowski M, Burgess MM, Dickinson JL. Community Engagement for Big Epidemiology: Deliberative Democracy as a Tool. Journal of Personalized Medicine. 2014; 4(4):459-474. https://doi.org/10.3390/jpm4040459
Chicago/Turabian StyleMcWhirter, Rebekah E., Christine R. Critchley, Dianne Nicol, Don Chalmers, Tess Whitton, Margaret Otlowski, Michael M. Burgess, and Joanne L. Dickinson. 2014. "Community Engagement for Big Epidemiology: Deliberative Democracy as a Tool" Journal of Personalized Medicine 4, no. 4: 459-474. https://doi.org/10.3390/jpm4040459