
Early Detection of Hepatocellular Carcinoma: How to Screen and Follow up Patients with Liver Cirrhosis According to the GERMAN S3 Guideline?

Abstract
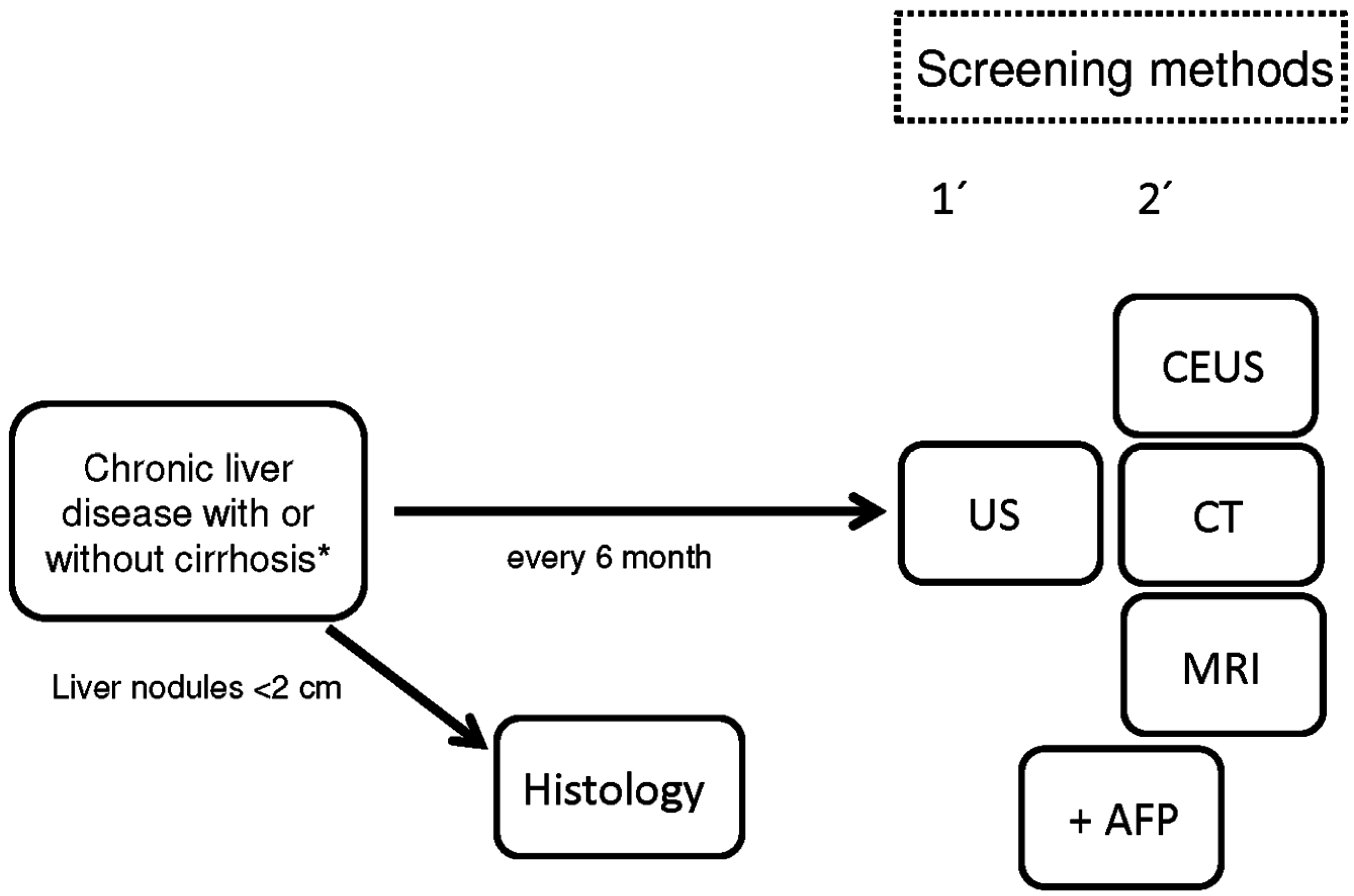
:1. Introduction

2. Imaging Techniques

{kind=link}
| Modality | Specificity | Sensitivity | Reference |
|---|---|---|---|
| US | 90% | 58%–89% | [16] |
| US | 94% | 94% | [17] |
| US | - | 89% | [30] |
| US + AFP | - | 69% | [27] |
| CEUS | - | 66.6%–97.3% | [25] |
| CT | 80% | 80% | [6,28] |
| CT | - | 56%–67% | [30] |
| MRI | - | 50%–56% | [30] |
3. Conclusions
Author Contributions
Conflicts of Interest
References
- Bruix, J.; Sherman, M. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B.; Davila, J.A.; Petersen, N.J.; McGlynn, K.A. The continuing increase in the incidence of hepatocellular carcinoma in the United States: An update. Ann. Intern. Med. 2003, 139, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Burroughs, A.; Bruix, J. Hepatocellular carcinoma. Lancet 2003, 362, 1907–1917. [Google Scholar] [CrossRef]
- Chang, M.H.; Chen, C.J.; Lai, M.S.; Hsu, H.M.; Wu, T.C.; Kong, M.S.; Liang, D.C.; Shau, W.Y.; Chen, D.S. Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children. N. Engl. J. Med. 1997, 336, 1855–1859. [Google Scholar] [CrossRef] [PubMed]
- Greten, T.F.; Malek, N.P.; Schmidt, S.; Arends, J.; Bartenstein, P.; Bechstein, W.; Bernatik, T.; Bitzer, M.; Chavan, A.; Dollinger, M.; et al. Diagnosis and therapy for hepatocellular carcinoma. Z. Gastroenterol. 2013, 51, 1269–1326. [Google Scholar] [PubMed]
- Fattovich, G.; Olivari, N.; Pasino, M.; D’Onofrio, M.; Martone, E.; Donato, F. Long-term outcome of chronic hepatitis B in Caucasian patients: Mortality after 25 years. Gut 2008, 57, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Tapias, J.M.; Costa, J.; Mas, A.; Bruquera, M.; Rodes, J. Influence of hepatitis B virus genotype on the long term outcome of chronic hepatitis B in western patients. Gastroenterology 2002, 123, 1848–1856. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Poynard, T.; Colombo, M.; Schiff, E.; Burak, K.; Heathcote, E.J.; Berg, T.; Poo, J.L.; Mello, C.B.; Guenther, R.; et al. Maintenance therapy with peginterferon alfa-2b does not prevent hepatocellular carcinoma in cirrhotic patients with chronic hepatitis C. Gastroenterology 2011, 140, 1990–1999. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.I.; Lu, S.N.; Liaw, Y.F.; You, S.L.; Sun, C.A.; Wang, L.Y.; Hsiao, C.K.; Chen, P.J.; Chen, D.S.; Chen, C.J. Hepatitis B e antigen and the risk of hepatocellular carcinoma. N. Engl. J. Med. 2002, 347, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Philippe, M.A.; Ruddell, R.G.; Ramm, G.A. Role of iron in hepatic fibrosis: One piece in the puzzle. World J. Gastroenterol. 2007, 13, 4746–4754. [Google Scholar] [CrossRef] [PubMed]
- Ascha, M.S.; Hanouneh, I.A.; Lopez, R.; Tamimi, T.A.; Feldstein, A.F.; Zein, N.N. The incidence and risk factors of hepatocellular carcinoma in patients with nonalcoholic steatohepatitis. Hepatology 2010, 51, 1972–1978. [Google Scholar] [CrossRef] [PubMed]
- Zoli, M.; Maqalotti, D.; Bianchi, G.; Gueli, C.; Marchesini, G.; Pisi, E. Efficacy of a surveillance program for early detection of hepatocellular carcinoma. Cancer 1996, 78, 977–985. [Google Scholar] [CrossRef]
- Henrion, J.; Libon, E.; de Maeght, S.; Deltenre, P.; Schapira, M.; Ghilain, J.M.; Maisin, J.M.; Heller, F.R. Screening for hepatocarcinoma in a cohort with cirrhosis mainly of alcoholic origin. Gastroenterol. Clin. Biol. 2003, 27, 534–539. [Google Scholar] [PubMed]
- Seitz, K. Quality of abdominal ultrasound. Ultraschall Med. 2006, 27, 217–219. [Google Scholar] [CrossRef] [PubMed]
- Bolondi, L. Screening for hepatocellular carcinoma in cirrhosis. J. Hepatol. 2003, 39, 1076–1084. [Google Scholar] [CrossRef]
- Singal, A.; Volk, M.L.; Waljee, A.; Salqia, R.; Higgins, P.; Rogers, M.A.; Marrero, J.A. Meta-analysis: Surveillance with ultrasound for early-stage hepatocellular carcinoma in patients with cirrhosis. Aliment. Pharmacol. Ther. 2009, 30, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Hangiandreou, N.J.; Stekel, S.F.; Tradup, D.J.; Gorny, K.R.; King, D.M. Four-year experience with a clinical ultrasound quality control program. Ultrasound Med. Biol. 2011, 37, 1350–1357. [Google Scholar] [CrossRef] [PubMed]
- Seitz, K.; Vasilakis, D.; Ziegler, M. Efficiency of a portable B-scan ultrasound device in comparison to a high-end machine in abdominal ultrasound. Results of a pilot study. Ultraschall Med. 2003, 24, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, C.M.; Seitz, K.; Leicht-Biener, U.; Mauch, M. Detection of therapeutically relevant diagnoses made by sonography of the upper abdomen: Portable versus high-end sonographic units—A prospective study. Ultraschall Med. 2004, 25, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Ueno, S.; Sakoda, M.; Kurahara, H.; Iino, S.; Minami, K.; Ando, K.; Mataki, Y.; Maemura, K.; Ishiqami, S.; Takumi, K.; et al. Preoperative segmentation of the liver, based on 3D CT images, facilitates laparoscopic anatomic hepatic resection for small nodular hepatocellular carcinoma in patients with cirrhosis. Hepatogastroenterology 2010, 57, 807–812. [Google Scholar] [PubMed]
- Seitz, K.; Bernatik, T.; Strobel, D.; Blank, W.; Friedrich-Rust, M.; Strunk, H.; Greis, C.; Kratzer, W.; Schuler, A. Contrast-enhanced ultrasound (CEUS) for the characterization of focal liver lesions in clinical practice (DEGUM Multicenter Trial): CEUS vs. MRI—A prospective comparison in 269 patients. Ultraschall Med. 2010, 31, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.J.; Xu, H.X.; Lu, M.D.; Xie, X.Y.; Xu, Z.F.; Zhenq, Y.L.; Liang, J.Y. Enhancement pattern of hepatocellular carcinoma: Comparison of real-time contrast-enhanced ultrasound and contrast-enhanced computed tomography. Clin. Imaging 2006, 30, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Tranquart, F.; Correas, J.M.; Ladam Marcus, V.; Manzoni, P.; Vilqrain, V.; Aube, C.; Elmaleh, A.; Chami, L.; Claudon, M.; Cuilleron, M.; et al. Real-time contrast-enhanced ultrasound in the evaluation of focal liver lesions: Diagnostic efficacy and economical issues from a French multicentric study. J. Radiol. 2009, 90, 109–122. [Google Scholar] [CrossRef]
- Gaiani, S.; Celli, N.; Piscaglia, F.; Cecillioni, L.; Losinno, F.; Gianqreqorio, F.; Mancini, M.; Pini, P.; Fornari, F.; Bolondi, L. Usefulness of contrast-enhanced perfusional sonography in the assessment of hepatocellular carcinoma hypervascular at spiral computed tomography. J. Hepatol. 2004, 41, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.H.; Yang, B.H.; Tang, Z.Y. Randomized controlled trial of screening for hepatocellular carcinoma. J. Cancer Res. Clin. Oncol. 2004, 130, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.G.; Parkin, D.M.; Chen, Q.G.; Lu, J.H.; Shen, Q.J.; Zhang, B.C.; Zhu, Y.R. Screening for liver cancer: Results of a randomised controlled trial in Qidong, China. J. Med. Screen. 2003, 10, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Plentz, R.R.; Boozari, B.; Malek, N.P. Guideline compliant diagnostics of hepatocellular carcinoma. Radiologe 2014, 54, 2651–2655. [Google Scholar]
- Lee, J.M.; Zech, C.J.; Bolondi, L.; Jonas, E.; Kim, M.J.; Matsui, O.; Merkle, E.M.; Sakamoto, M.; Choi, B.I. Consensus report of the 4th International Forum for Gadolinium-Ethoxybenzyl-Diethylenetriamine Pentaacetic Acid Magnetic Resonance Imaging. Korean J. Radiol. 2011, 12, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Teefey, S.A.; Hildeboldt, C.C.; Dehdashti, F.; Siegel, B.A.; Peters, M.G.; Heiken, J.P.; Brown, J.J.; McFarland, E.G.; Middleton, W.D.; Balfe, D.M. Detection of primary hepatic malignancy in liver transplant candidates: Prospective comparison of CT, MR imaging, US, and PET. Radiology 2003, 226, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Trinchet, J.C.; Chaffaut, C.; Bourcier, V.; Deqos, F.; Henrion, J.; Fontaine, H.; Roulot, D.; Mallat, A.; Hillaire, S.; Cales, P.; et al. Ultrasonographic surveillance of hepatocellular carcinoma in cirrhosis: A randomized trial comparing 3- and 6-month periodicities. Hepatology 2011, 54, 1987–1997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.E.; Kim, S.H.; Lee, S.J.; Rhim, H. Hypervascular hepatocellular carcinoma 1 cm or smaller in patients with chronic liver disease: Characterization with gadoxetic acid-enhanced MRI that includes diffusion-weighted imaging. AJR Am. J. Roentgenol. 2011, 196, 758–765. [Google Scholar] [CrossRef] [PubMed]
- Khattab, M.; Fouad, M.; Ahmed, E. Role of biomarker in the prediction and diagnosis of hepatocellular carcinoma. World J. Hepatol. 2015, 23, 2474–2481. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Plentz, R.R.; Malek, N.P. Early Detection of Hepatocellular Carcinoma: How to Screen and Follow up Patients with Liver Cirrhosis According to the GERMAN S3 Guideline? Diagnostics 2015, 5, 497-503. https://doi.org/10.3390/diagnostics5040497
Plentz RR, Malek NP. Early Detection of Hepatocellular Carcinoma: How to Screen and Follow up Patients with Liver Cirrhosis According to the GERMAN S3 Guideline? Diagnostics. 2015; 5(4):497-503. https://doi.org/10.3390/diagnostics5040497
Chicago/Turabian StylePlentz, Ruben R., and Nisar P. Malek. 2015. "Early Detection of Hepatocellular Carcinoma: How to Screen and Follow up Patients with Liver Cirrhosis According to the GERMAN S3 Guideline?" Diagnostics 5, no. 4: 497-503. https://doi.org/10.3390/diagnostics5040497