Hidden Cost of Drinking Water Treatment and Its Relation with Socioeconomic Status in Nepalese Urban Context

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
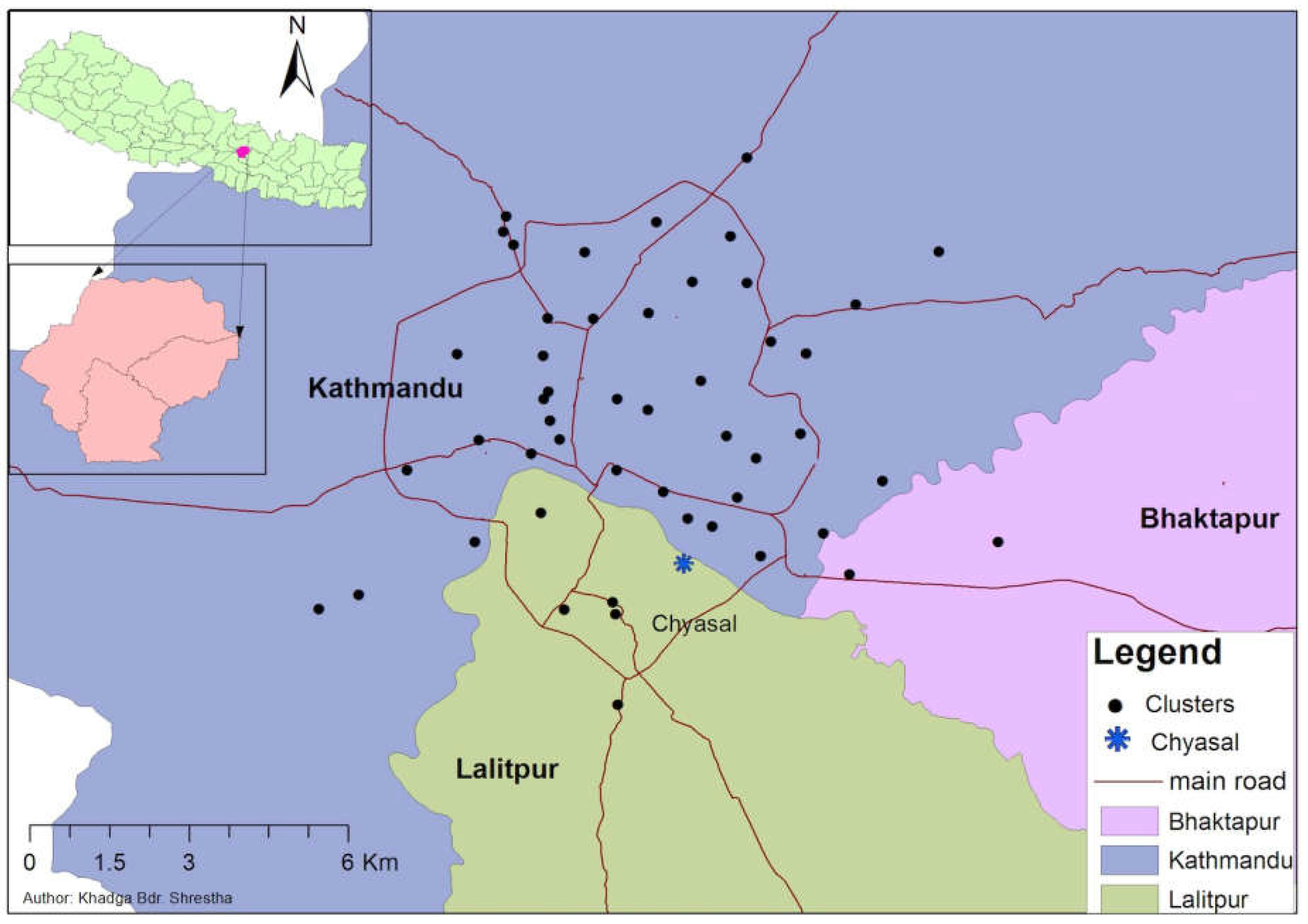
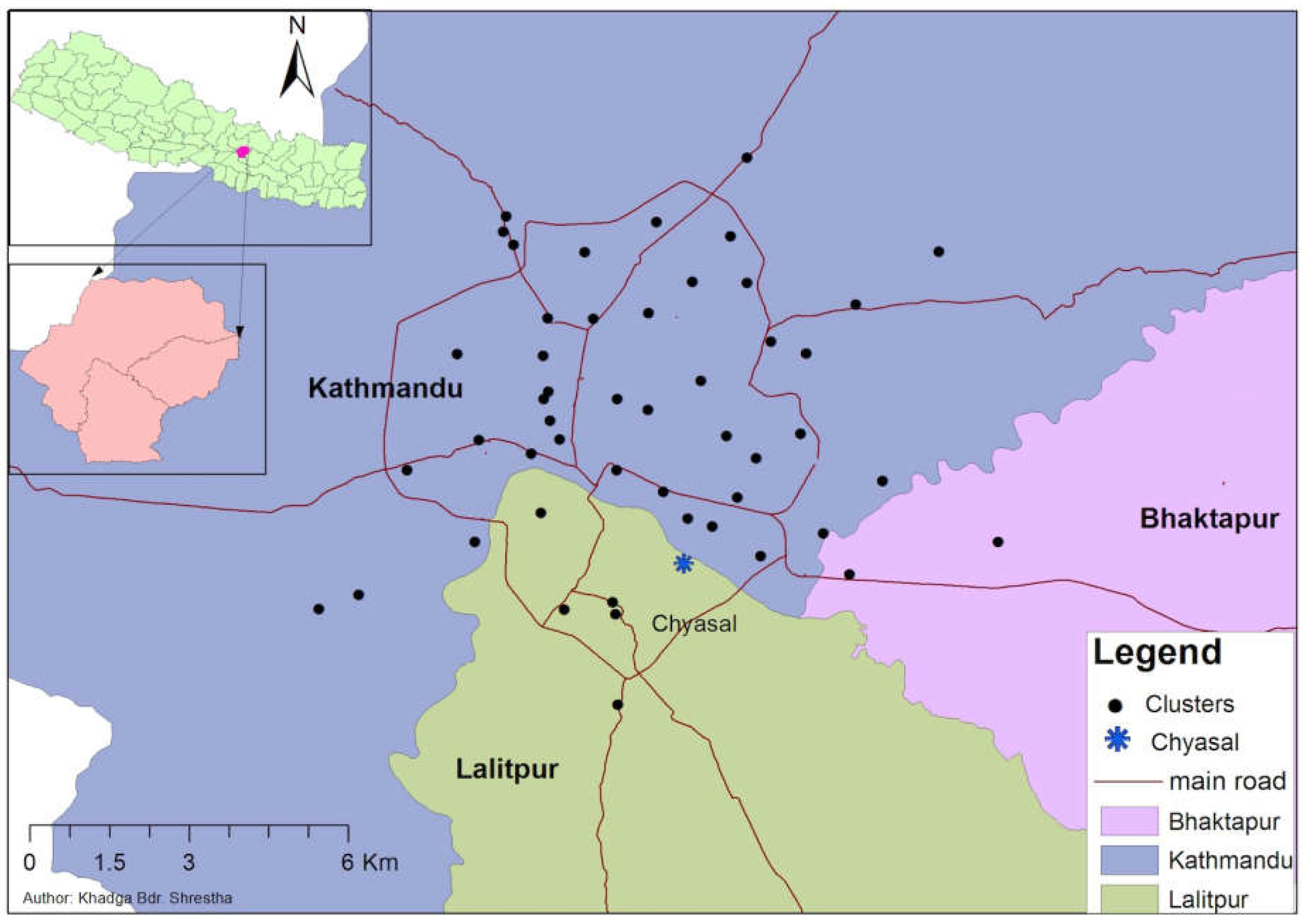
2.1. Study Area:
2.2. Methods
2.2.1. Estimation of Method-Specific Water Treatment Cost
2.2.2. Estimation of Average Monthly Treatment Cost
2.2.3. Socioeconomic Status Variables
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
3.1. Estimation of Method-Specific Cost
3.1.1. Cost for Chlorine Use
3.1.2. Cost for Ceramic Filter
3.1.3. Cost for Boiling
3.1.4. Cost for Euro-Guard
3.1.5. Cost for Domestic Treatment Plant (RO-UV)
3.2. Estimation of Average Monthly Treatment Cost in Households
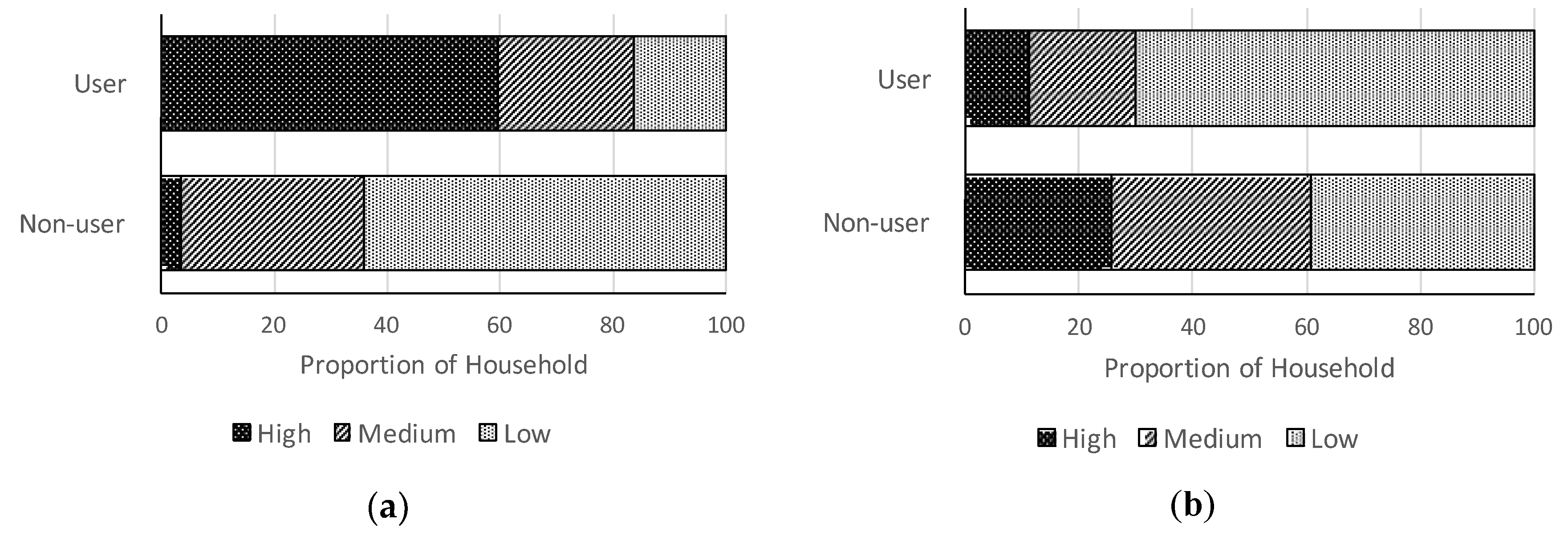
3.3. Socioeconomic Situation and Water Insecurity Perception in Surveyed Households
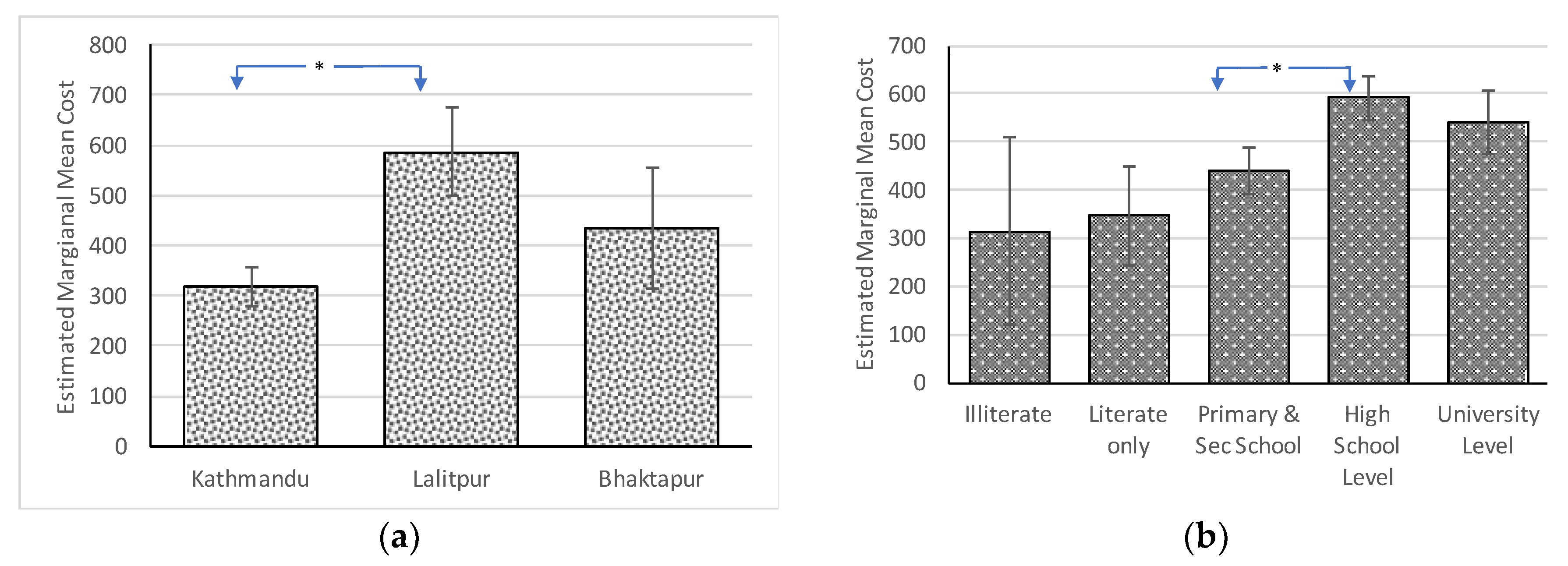
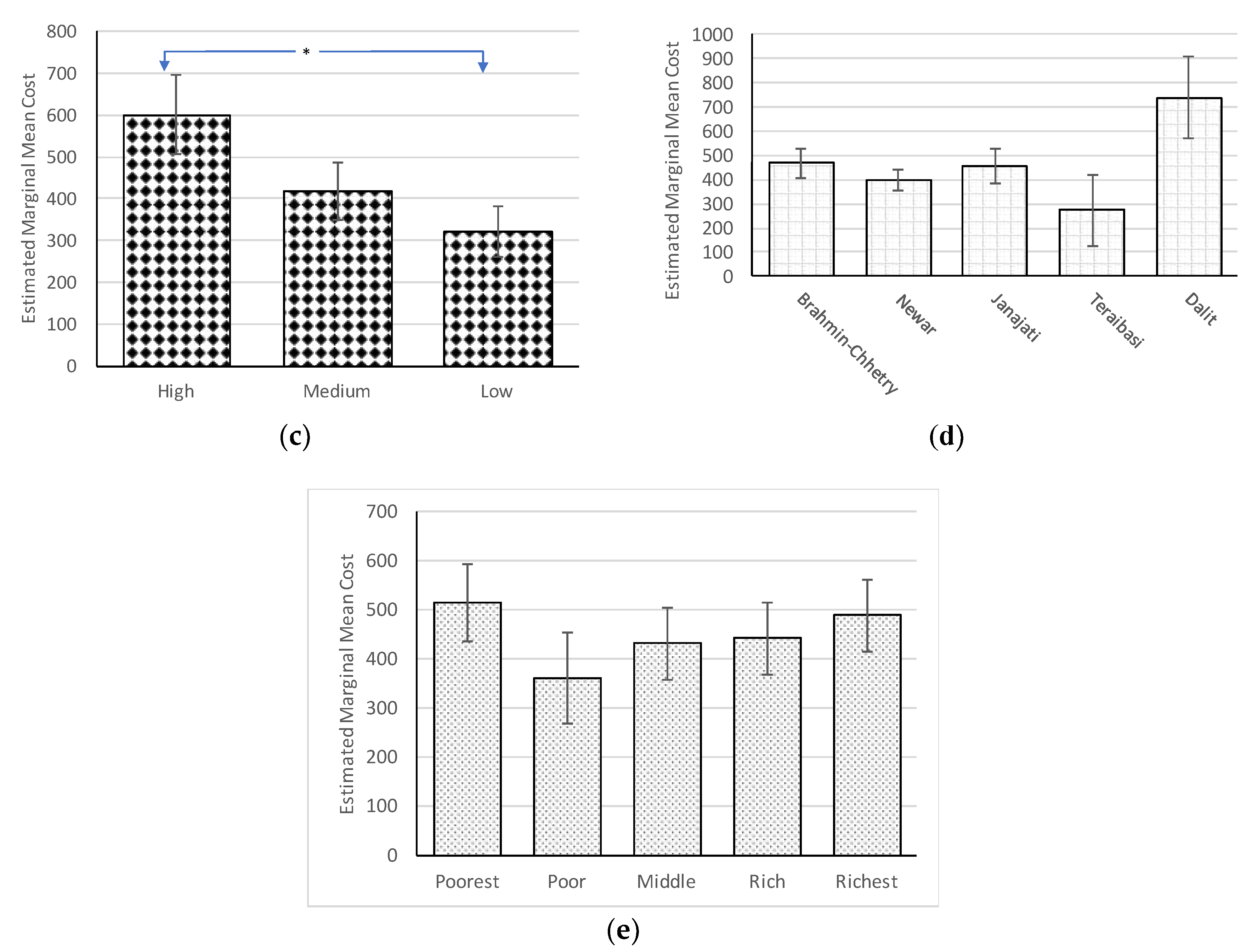
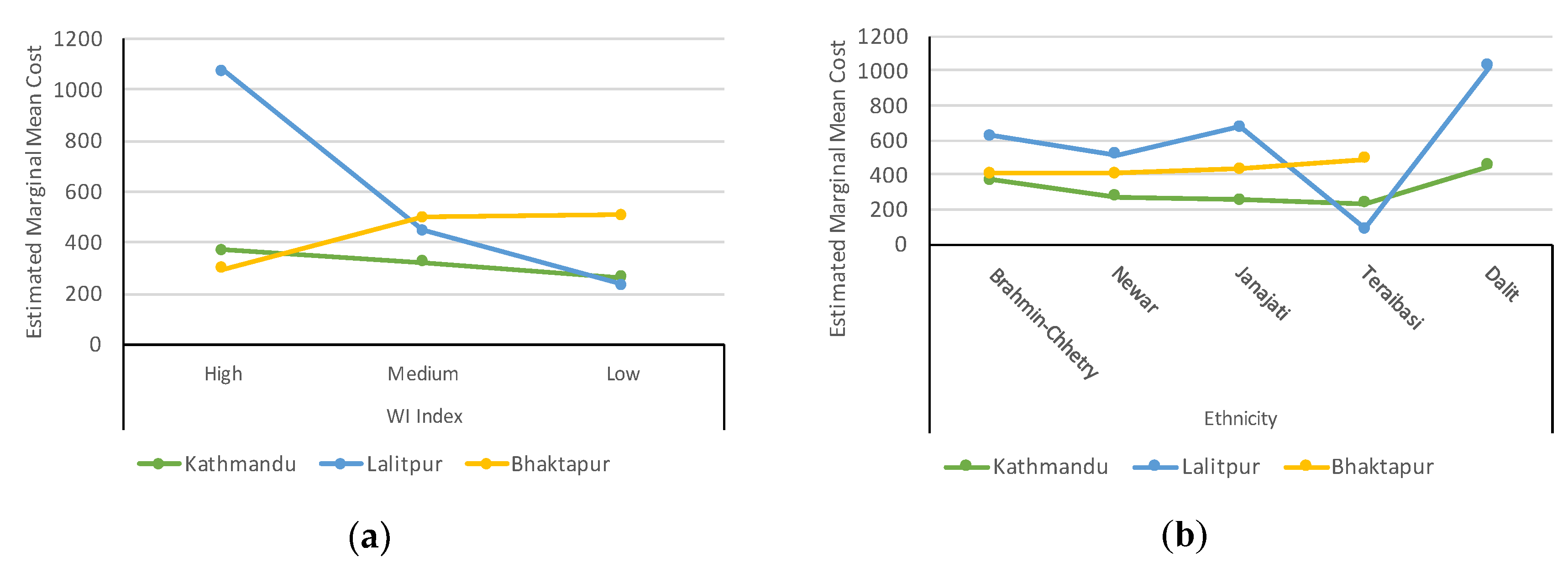
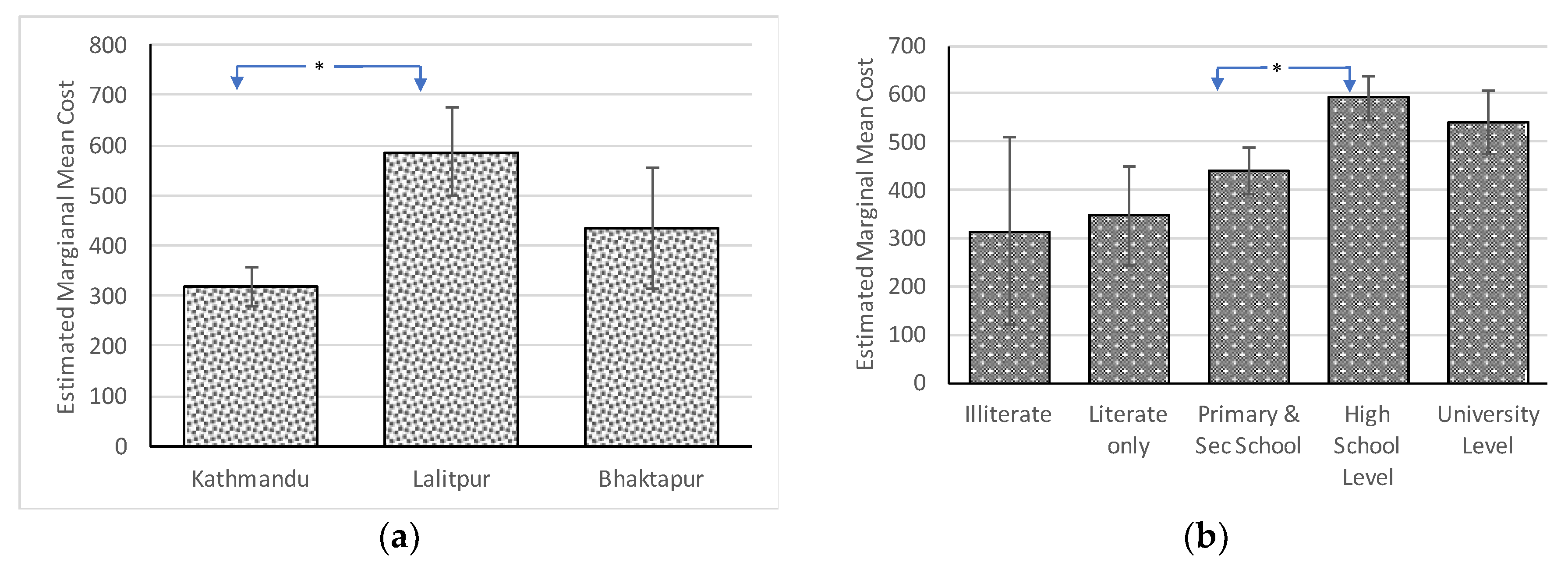
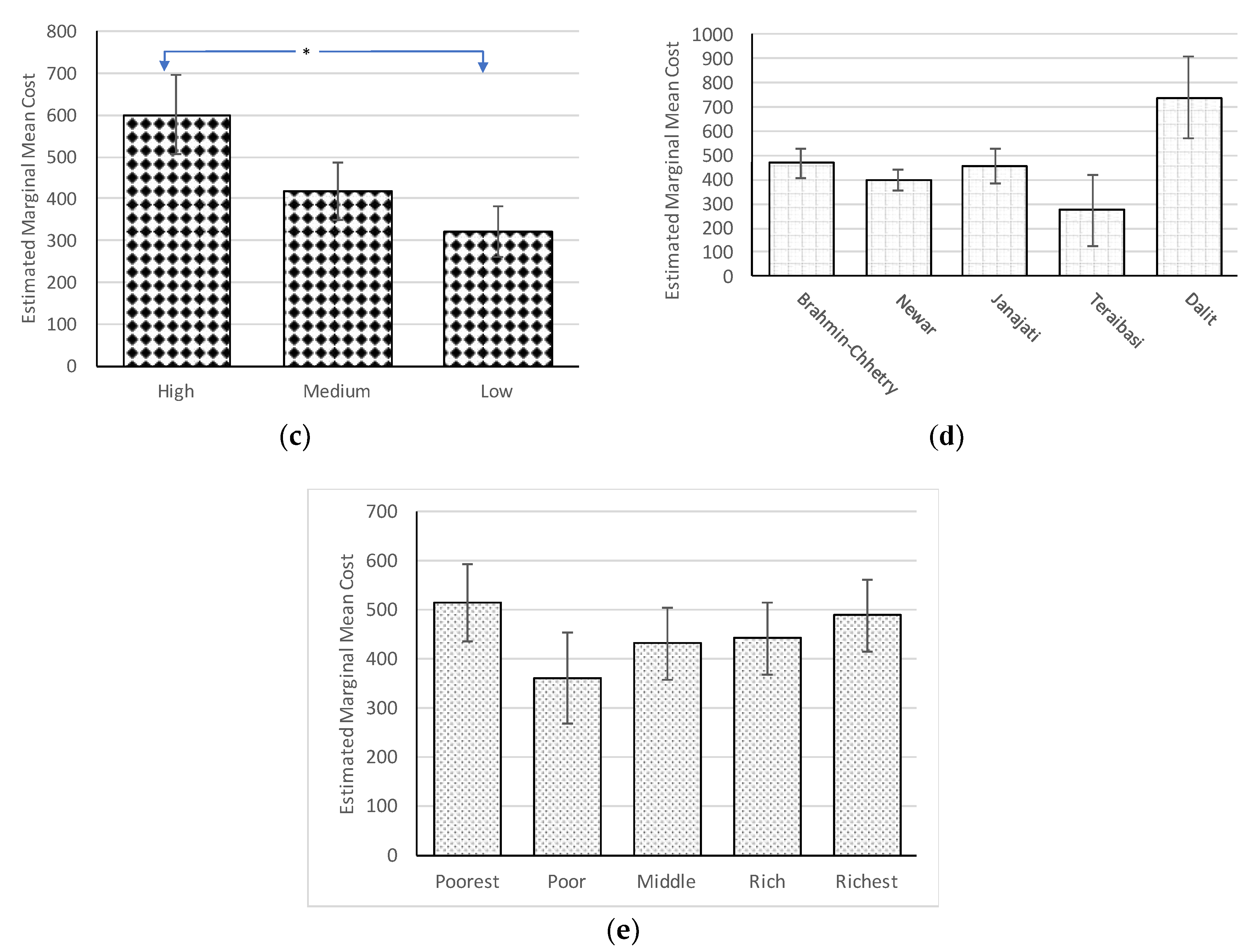
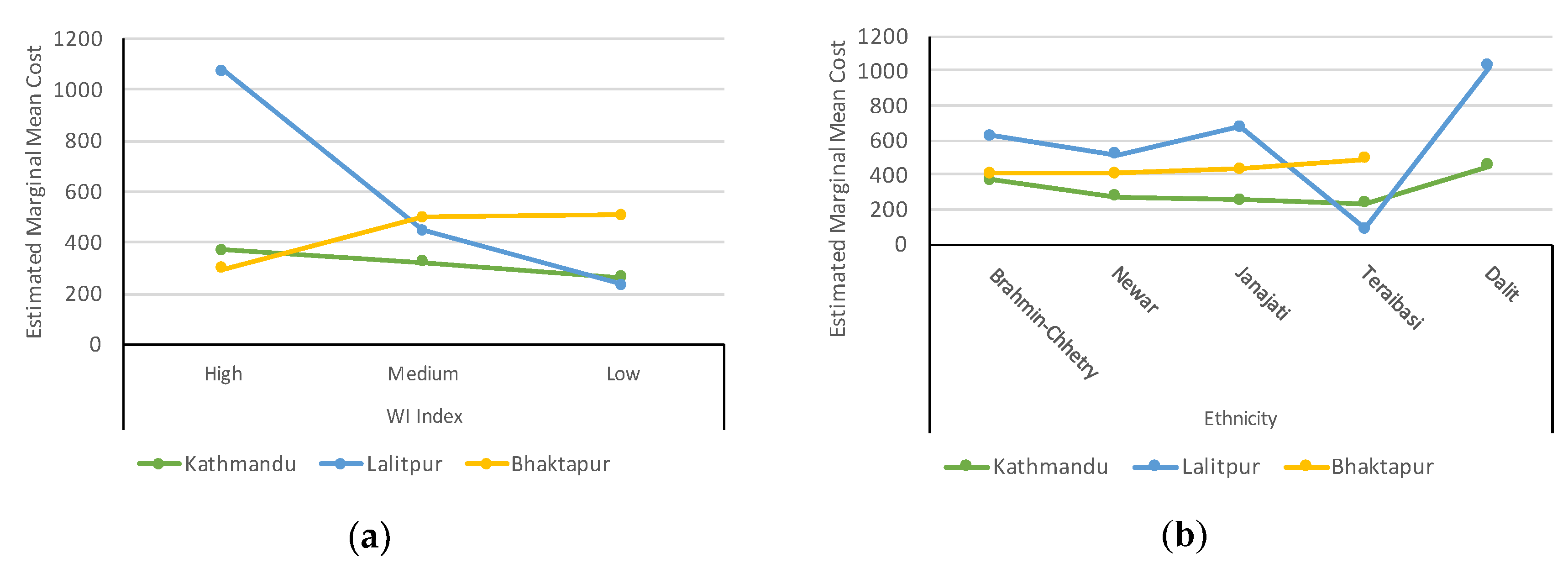
3.4. Association of Water Treatment Cost with Socioeconomic Variables
3.5. Situation of Water Treatment Cost in Alternative Sources Users
4. Discussion
5. Conclusion
Supplementary Materials
Author contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hutton, G. Global costs and benefits of reaching universal coverage of sanitation and drinking-water supply. J. Water Health 2013, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- United Nations. The Human Right to Water and Sanitation. Available online: http://www.un.org/waterforlifedecade/human_right_to_water.shtml (accessed on 29 December 2017).
- The World Bank Water Overview. Available online: http://www.worldbank.org/en/topic/water/overview (accessed on 28 December 2017).
- Brighty, P. Water Security in South Asia: Geo Factsheet. Available online: https://intranet.royalhospitalschool.org/resource.aspx?id=672068 (accessed on 9 March 2018).
- MoUD Government of Nepal. National Urban Water Supply and Sanitation Sector Policy Final Draft; MoUD Government of Nepal: Kathmandu, Nepal, 2009.
- Thapa, B.R.; Ishidaira, H.; Pandey, V.P.; Shakya, N.M. A multi-model approach for analyzing water balance dynamics in Kathmandu Valley, Nepal. J. Hydrol. Reg. Stud. 2017, 9, 149–162. [Google Scholar] [CrossRef]
- Yoden, K. Kathmandu Valley Water Distribution, Sewerage and Urban Development; ADB: Kathmandu, Nepal, 2010. [Google Scholar]
- Pant, B.R. Ground water quality in the Kathmandu valley of Nepal. Environ. Monit. Assess. 2011, 178, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Tamrakar, N.K.; Manandhar, K.C. Institutional Capacity Assessment of KUKL; Ministry of Urban Development (MoUD): Kathmandu, Nepal; Japan International Cooperation Agency (JICA): Tokyo, Japan, 2016.
- Thapa, B.R.; Ishidaira, H.; Pandey, V.P.; Bhandari, T.M.; Shakya, N.M. Evaluation of Water Security in Kathmandu Valley before and after Water Transfer from another Basin. Water 2018, 10, 24. [Google Scholar] [CrossRef]
- MWSP Melamchi Water Supply Project Description. Available online: http://www.melamchiwater.gov.np/about-us/melamchi-ws-project/project-description/ (accessed on 4 February 2018).
- Thapa, P. Delay in Melamchi Water Supply Project in Nepal: An Analysis of the Decision Making Process since 1998 under Application of Teisman’s Rounds Model. 2012. Available online: https://www.scribd.com/document/106089175/Delay-in-Melamchi-Project-in-Nepal (accessed on 5 May 2018).
- Pattanayak, S.K.; Yang, J.-C.C.; Whittington, D.; Bal Kumar, K.C. Coping with unreliable public water supplies: Averting expenditures by households in Kathmandu, Nepal. Water Resour. Res. 2005, 41, 1–11. [Google Scholar] [CrossRef]
- Warner, N.R.; Levy, J.; Harpp, K.; Farruggia, F. Drinking water quality in Nepal’s Kathmandu Valley: A survey and assessment of selected controlling site characteristics. Hydrogeol. J. 2008, 16, 321–334. [Google Scholar] [CrossRef]
- Subedi, M.; Aryal, M. Public perception about drinking jar water and its bacteriological analysis. Nepal Med. Coll. J. 2010, 12, 110–114. [Google Scholar] [PubMed]
- WHO. UNICEF Diarrhoea: Why Children Are Still Dying and What Can Be Done; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- PATH. Perspectives: Commercial Approaches to Delivering Household Water Treatment and Safe Storage Products and Solutions to Low-Income Households; PATH: Seattle, WA, USA, 2012. [Google Scholar]
- Shrestha, S.; Aihara, Y.; Kondo, N.; Rajbhandari, S.; Bhattarai, A.P.; Bista, N.; Kazama, F.; Nishida, K.; Timilsina, H.P.; Shindo, J. Household Water Use in the Kathmandu Valley: A Dry Season Survey; Interdisciplinary Center for River Basin Environment: Kofu Yamanashi, Japan, 2016. [Google Scholar]
- Lantagne, D.S.; Clasen, T.F. Use of household water treatment and safe storage methods in acute emergency response: Case study results from Nepal, Indonesia, Kenya, and Haiti. Environ. Sci. Technol. 2012, 46, 11352–11360. [Google Scholar] [CrossRef] [PubMed]
- Rojas, L.F.R.; Megerle, A.; Araral, E. Perception of Water Quality and Health Risks in the Rural Area of Medellín. Am. J. Rural Dev. 2010, 12, 106–115. [Google Scholar]
- McGarvey, S.T.; Buszin, J.; Reed, H.; Smith, D.C.; Rahman, Z.; Andrzejewski, C.; Awusabo-Asare, K.; White, M.J. Community and household determinants of water quality in coastal Ghana. J. Water Health 2008, 6, 339–349. [Google Scholar] [CrossRef] [PubMed]
- ICIMOD. Kathmandu Valley Environment Outlook; International Centre for Integrated Mountain Development: Kathmandu, Nepal, 2007. [Google Scholar]
- Adhikari, A. Towards Developing Indicators of Environmental Sustainability for Kathmandu, Nepal. Int. J. Humanit. Soc. Sci. 2012, 2, 192–196. [Google Scholar]
- Gohil, P.P.; Channiwala, S.A. Experimental Investigation of Performance of Conventional Lpg Cooking Stove. Fundam. J. Therm. Sci. Eng. 2011, 1, 25–34. [Google Scholar]
- Waters, T.; Waters, D. Are the terms “socio-economic status” and “class status” a warped form of reasoning for Max Weber? Palgrave Commun. 2016, 2, 16002. [Google Scholar] [CrossRef]
- Vyas, S.; Kumaranayake, L. Constructing socio-economic status indices: How to use principal components analysis. Health Policy Plan. 2006, 21, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Allison, P.D. Fixed Effects Regression Models (Quantitative Applications in the Social Sciences), 1st ed.; Sage Publications Inc.: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Armstrong, R.A. When to use the Bonferroni correction. Ophthalmic Physiol. Opt. 2014, 34, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Rosa, G.; Clasen, T. Estimating the scope of household water treatment in low- and medium-income countries. Am. J. Trop. Med. Hyg. 2010, 82, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Ramshah Path; New ERA; ICF DHS Program. Nepal Demographic and Health Survey 2016; Ministry of Health Ramshah Path: Kathmandu, Nepal; New ERA: Kathmandu, Nepal; The DHS Program ICF: Rockville, MD, USA, 2017; pp. 9–10. Available online: https://www.dhsprogram.com/pubs/pdf/fr336/fr336.pdf (accessed on 5 May 2018).
- Nepal Rastra Bank. Fifth Household Budget Survey Nepal 2014/15; Nepal Rastra Bank: Kathmandu, Nepal, 2016. [Google Scholar]
- Irianti, S.; Prasetyoputra, P.; Sasimartoyo, T.P. Determinants of household drinking-water source in Indonesia: An analysis of the 2007 Indonesian family life survey. Cogent Med. 2016, 3, 1–13. [Google Scholar] [CrossRef]
- Shrestha, S.; Aihara, Y.; Bhattarai, A.P.; Bista, N.; Rajbhandari, S.; Kondo, N.; Kazama, F.; Nishida, K.; Shindo, J. Dynamics of Domestic Water Consumption in the Urban Area of the Kathmandu Valley: Situation Analysis Pre and Post 2015 Gorkha Earthquake. Water 2017, 9, 222. [Google Scholar] [CrossRef]
- McLennan, J.D. To boil or not: Drinking water for children in a periurban barrio. Soc. Sci. Med. 2000, 51, 1211–1220. [Google Scholar] [CrossRef]
- Farzin, Y.H.; Grogan, K.A. Socioeconomic factors and water quality in California. Environ. Econ. Policy Stud. 2013, 15, 1–37. [Google Scholar] [CrossRef]
- Clasen, T.F. Household Water Treatment and the Millennium Development Goals: Keeping the Focus on Health. Environ. Sci. Technol. 2010, 44, 7357–7360. [Google Scholar] [CrossRef] [PubMed]
- Clasen, T.F.; Cairncross, S. Household water management: Refining the dominant paradigm. Trop. Med. Int. Health 2004, 9, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Whiteford, L.M.; Vindrola-Padros, C. Water, Health and Social Inequality. In International Encyclopedia of the Social & Behavioral Sciences; Elsevier Ltd.: New York, NY, USA, 2015; Volume 25, pp. 428–436. ISBN 9780080970875. [Google Scholar]
- Johns, H. Stigmatization of Dalits in Access to Water and Sanitation in India; National Campaign on Dalit Human Rights (NCDHR): New Delhi, India, 2012. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SN | Method | Initial Cost | Operating Cost | Maintenance Cost | Total Cost | Summary Base Data for Cost Calculation |
|---|---|---|---|---|---|---|
| 1 | Chemical | 0.0 | 22.5 | 0.0 | 22.5 | Operating cost: Cost for chlorine (Piyush) = NRs 25/60 mL bottle (used for 300 L of water) |
| 2 | Ceramic Filter | 13.3 | 0.0 | 43.4 | 56.7 | Initial cost: Filter = NRs 800; Average Life = 5 years (2–8). Maintenance cost: Candles (2) = NRs 260 × 2 times (change 3–12 months). |
| 3 | Boiling (Gas) | 7.5 | 283.04 | 50.0 | 340.5 | Initial cost: Gas stove = NRs 1500; Average Life = 5 years; 30% used for boiling. Operating cost: Thermal efficiency = 0.66; Unit Cost for gas = 0.008648 NRs/kcal Maintenance cost: Boiling pot = NRs 600; Average life = 1 year. |
| Boiling (Electricity) | 16.7 | 354.4 | 140.0 | 511.1 | Initial cost: Electric heater = NRs 200; Average Life = 1 year. Operating cost: Thermal efficiency = 0.85 Unit Cost for electricity = 12 NRs/kWh Maintenance cost: Heater coil = NRs 90 (1 coil per month), Boiling pot = NRs 600 for 1 year. | |
| 4 | Euro-Guard | 333.3 | 250 | 2.7 | 586.0 | Initial cost: Euro-Guard = NRs 20,000; Average Life = 5 years; Operating cost: Wattage = 28 W, Average operation time = 16 min/day, Unit Cost for electricity = NRs 12/kWh Maintenance cost: Filter = NRs 1000 per year; Lamp + technician = NRs 4000 per 2 years. |
| 5 | Domestic Treatment Plant (RO-UV) | 357.1 | 25.6 | 416.6 | 799.3 | Initial cost: Treatment plant = NRs 30,000; Average Life = 7 years Operating cost: Wattage 60 W for RO and 11 W for UV, Average operation time = 60 min/day, Unit Cost for electricity = NRs 12/kWh Maintenance cost: Filter + technician = NRs 5000 per year. |
| Water Treatment Method | Frequency | Percentage of HH | Method-Specific Cost (NRs) | Total Monthly Cost (NRs) # |
|---|---|---|---|---|
| Chemicals (Chlorine) | 59 | 3.9 | 22.5 | 1327.5 |
| Ceramic filter | 956 | 63.9 | 56.7 | 54,173.3 |
| Boiling | 893 | 59.7 | 391.7 | 349,788.1 |
| Euro-Guard | 197 | 13.2 | 586.0 | 115,442.0 |
| Domestic RO-UV treatment | 49 | 3.3 | 799.4 | 39,170.6 |
| No treatment | 366 | 24.5 | 0.0 | 0.0 |
| Per household cost (All HH) | 379.7 (393.1) | |||
| Per household cost (Treatment method applied HH only) | 502.8 (377.8) | |||
| Average water expenditure | (Piped water, Bottle/Jar, Tanker/Vendor water) | 496.0 (909.4) | ||
| Variables | Categories | Frequency | Percentage |
|---|---|---|---|
| District (n = 1495) | Kathmandu | 1228 | 82.1 |
| Lalitpur | 178 | 11.9 | |
| Bhaktapur | 89 | 6.0 | |
| Ethnicity (n = 1495) | Brahmin/Chhetri | 640 | 42.8 |
| Newar | 551 | 36.9 | |
| Janajati | 200 | 13.4 | |
| Teraibasi | 63 | 4.2 | |
| Dalit | 41 | 2.7 | |
| Higher Education (n = 1483) | Illiterate | 45 | 3.0 |
| Literate only | 104 | 7.0 | |
| Primary and Secondary School | 600 | 40.5 | |
| High school (+2 level) | 348 | 23.5 | |
| University Level | 386 | 26.0 | |
| Occupation of HH head (n = 1475) | Unemployed | 248 | 16.8 |
| Daily employed | 105 | 7.1 | |
| Students | 102 | 6.9 | |
| Business | 623 | 42.2 | |
| Service | 397 | 26.9 | |
| Wealth Quintile (n = 1495) | Poorest | 299 | 20.0 |
| Poor | 308 | 20.6 | |
| Middle | 295 | 19.7 | |
| Rich | 289 | 19.3 | |
| Richest | 304 | 20.3 | |
| Water Insecurity Index (n = 1493) | High (>45) | 389 | 26.1 |
| Medium (30–45) | 477 | 31.9 | |
| Low (<30) | 627 | 42.0 |
| Parameter | Numerator Df | Denominator Df | F (Statistics) | p Value |
|---|---|---|---|---|
| Intercept | 1 | 1366 | 57.58 | 0.00 |
| DISTRICT | 2 | 1366 | 6.04 | 0.00 |
| Ethnicity | 4 | 1366 | 1.68 | 0.15 |
| EduHigher | 4 | 1366 | 2.93 | 0.02 |
| WQuin | 4 | 1366 | 0.56 | 0.69 |
| WIIndex | 2 | 1366 | 3.67 | 0.03 |
| DISTRICT × Ethnicity | 7 | 1366 | 2.28 | 0.03 |
| DISTRICT × EduHigher | 8 | 1366 | 1.10 | 0.36 |
| DISTRICT × WQuin | 8 | 1366 | 1.53 | 0.14 |
| DISTRICT × WIIndex | 4 | 1366 | 16.38 | 0.00 |
| Ethnicity × EduHigher | 16 | 1366 | 0.87 | 0.61 |
| Ethnicity × WQuin | 16 | 1366 | 0.88 | 0.59 |
| Ethnicity × WIIndex | 8 | 1366 | 1.18 | 0.31 |
| EduHigher × WQuin | 16 | 1366 | 1.09 | 0.36 |
| EduHigher × WIIndex | 8 | 1366 | 1.50 | 0.15 |
| WQuin × WIIndex | 8 | 1366 | 1.51 | 0.15 |
| Water Sources | Kathmandu (n = 1228) | Lalitpur (n = 178) | ||||||
|---|---|---|---|---|---|---|---|---|
| User | Non-User | User | Non-User | |||||
| HH (%) | ATC (sd) | HH (%) | ATC (sd) | HH (%) | ATC (sd) | HH (%) | ATC (sd) | |
| Ground water | 20 (1.6) | 489.4 (286.9) | 1208 (98.4) | 364.1 (373.2) | 13 (7.3) | 1340.3 (670.2) | 165 (92.7) | 368.8 (511.2) |
| Tanker/ Vendor | 60 (4.9) | 488.3 (378.6) | 1168 (95.1) | 359.9 (370.9) | 34 (19.1) | 1288.7 (669.5) | 144 (80.9) | 239.3 (319.0) |
| Ground or Tanker water | 80 (6.5) | 488.6 (356.2) | 1148 (93.5) | 357.6 (371.9) | 37 (20.8) | 1224.9 (687.9) | 141 (79.2) | 233.8 (314.0) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shrestha, K.B.; Thapa, B.R.; Aihara, Y.; Shrestha, S.; Bhattarai, A.P.; Bista, N.; Kazama, F.; Shindo, J. Hidden Cost of Drinking Water Treatment and Its Relation with Socioeconomic Status in Nepalese Urban Context. Water 2018, 10, 607. https://doi.org/10.3390/w10050607
Shrestha KB, Thapa BR, Aihara Y, Shrestha S, Bhattarai AP, Bista N, Kazama F, Shindo J. Hidden Cost of Drinking Water Treatment and Its Relation with Socioeconomic Status in Nepalese Urban Context. Water. 2018; 10(5):607. https://doi.org/10.3390/w10050607
Chicago/Turabian StyleShrestha, Khadga Bahadur, Bhesh Raj Thapa, Yoko Aihara, Sadhana Shrestha, Arun P. Bhattarai, Niranjan Bista, Futaba Kazama, and Junko Shindo. 2018. "Hidden Cost of Drinking Water Treatment and Its Relation with Socioeconomic Status in Nepalese Urban Context" Water 10, no. 5: 607. https://doi.org/10.3390/w10050607