
A Possible Association between Melanoma and Prostate Cancer. Results from a Case-Control-Study

Abstract
:1. Introduction
2. Results and Discussion
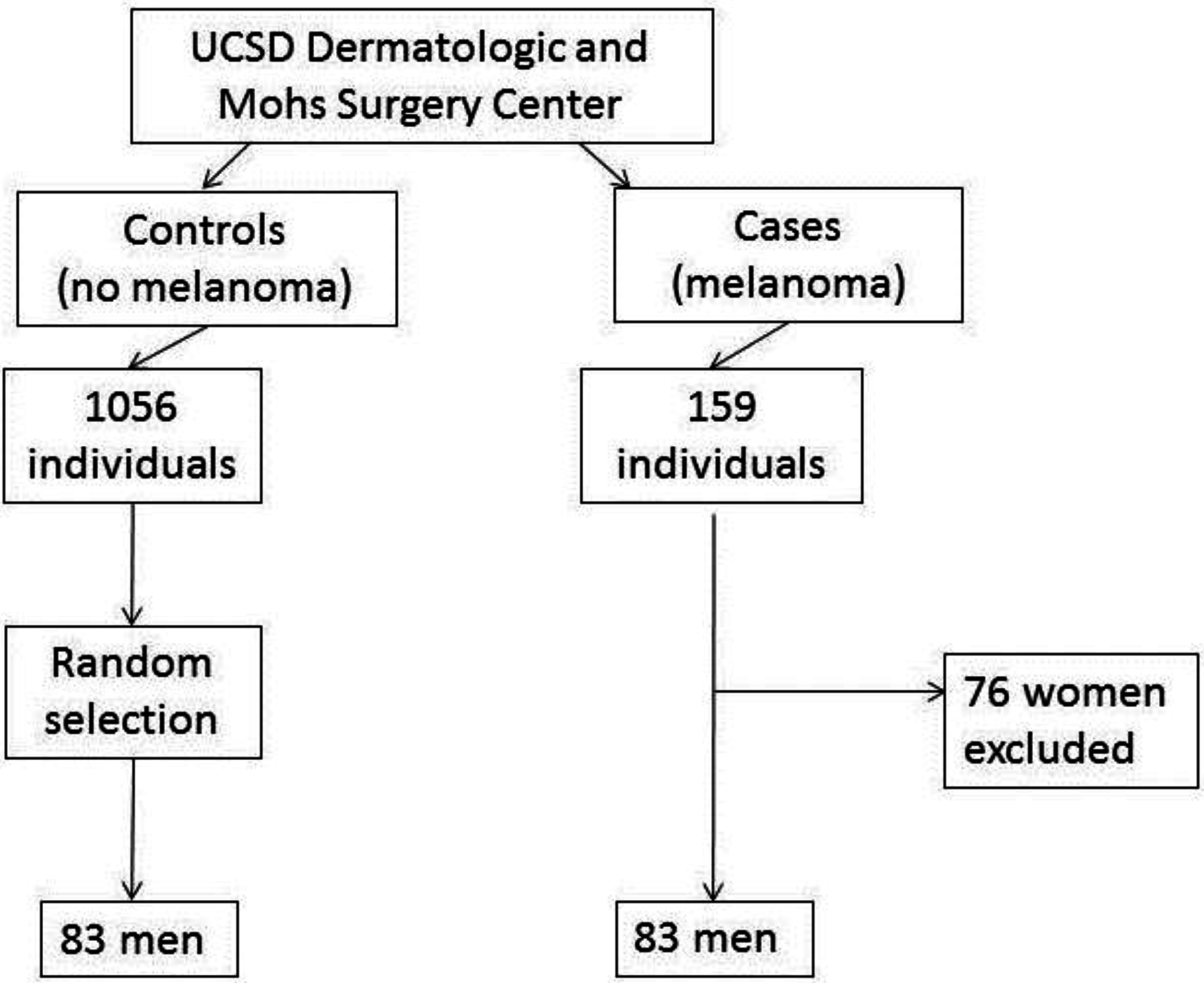
2.1. Results


{kind=link}
| Variable | Subvariable | Melanoma Cases N = 83 | Non-Melanoma Controls a N = 83 | OR | CI | p |
|---|---|---|---|---|---|---|
| Age (mean, SD) | 67 (13) | 69 (13.8) | 0.332 | |||
| Skin type N (%) | I | 6 (7.2) | 10 (12.7) | 0.57 | 0.2, 1.6 | 0.431 |
| II | 73 (88) | 58 (73.4) | 3.1 | 1.4, 7 | 0.007 | |
| III | 3 (3.6) | 11(13.9) | 0.24 | 0.07, 0.9 | 0.047 | |
| IV | 1 (1.2) | – | – | – | – | |
| BMI | 27.5 (4) | 25.9 (3.8) | 0.018 | |||
| Cigarette use | 22 (26.8) | 16 (20.3) | 1.4 | 0.7, 3 | 0.358 | |
| Pack years | 20 (11.6) | 28 (20) | 0.174 | |||
| Any alcohol use | 50 (61) | 27 (32.5) | 3.2 | 1.7, 6.1 | <0.001 | |
| BPH medications | 18 (22) | 10 (12.3) | 2 | 0.9, 4.6 | 0.145 | |
| Immunosuppression | Total | 5 (6.4) | 23 (29.1) | 0.17 | 0.06, 0.47 | <0.001 |
| HIV | 4 | 7 | ||||
| Lymphoma | 1 | 5 | ||||
| SOTR | – | 12 | ||||
| Duration of immunosuppression | Mean years (SD) | 11.6 (8.7) | 1.9 (1) | <0.001 | ||
| Prostate Cancer | 9 (10.8) | 2 (2.4) | 4.9 | 1, 23.5 | 0.057 | |
| Prostate Cancer Treatment | No treatment | 2 | – | |||
| Radical prostatectomy | 3 | 2 | ||||
| Brachytherapy | 1 | – | ||||
| XRT | 3 | – | ||||
| PSA | 2.0 (2.2) | 2.1 (2.8) | 0.902 |
| Variable | p-value | OR | 95% CI |
|---|---|---|---|
| Age | 0.052 | 1 | 0.94, 1 |
| BMI | 0.011 | 1.15 | 1, 1.3 |
| Alcohol use | 0.005 | 3.17 | 1.4, 7 |
| Skin type II | 0.025 | 1.9 | 1.1, 3.3 |
| Immunosuppression | 0.002 | 0.127 | 0.03, 0.5 |
| History of prostate cancer | 0.042 | 11.8 | 1.1, 129 |
2.2. Discussion
3. Experimental Section
4. Conclusions
Author Contributions
Conflicts of Interest
References
- Ingraffea, A. Melanoma. Facial Plast. Surg. Clin. N. Am. 2013, 21, 33–42. [Google Scholar] [CrossRef]
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics. Cancer J. Clin. 2013, 63, 11–30. [Google Scholar] [CrossRef]
- Elwood, J.M.; Jopson, J. Melanoma and sun exposure: An overview of published studies. Int. J. Cancer 1997, 3, 198–203. [Google Scholar] [CrossRef]
- Veierod, M.B.; Weiderpass, E.; Thorn, M.; Hansson, J.; Lund, E.; Armstrong, B.; Adami, H. A prospective study of pigmentation, sun exposure, and risk of cutaneous malignant melanoma in women. J. Natl. Cancer Inst. 2003, 95, 1530–1538. [Google Scholar] [CrossRef] [PubMed]
- Titus-Ernstoff, L.; Perry, A.E.; Spencer, S.K.; Gibson, J.J.; Cole, B.J.; Ernstoff, M.S. Pigmentary characteristics and moles in relation to melanoma risk. Int. J. Cancer 2005, 116, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.B.; Barnholtz-Sloan, J.S.; Chen, Y.; Bordeaux, J.S. Risk and survival of cutaneous melanoma diagnosed subsequent to a previous cancer. Arch. Dermatol. 2011, 147, 1395–1402. [Google Scholar] [CrossRef] [PubMed]
- Braisch, U.; Meyer, M.; Radespiel-Troger, M. Risk of subsequent primary cancer among prostate cancer patients in Bavaria, Germany. Eur. J. Cancer Prev. 2012, 21, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Li, W.-Q.; Qureshi, A.A.; Ma, J.; Goldstein, A.M.; Giovannucci, E.L.; Stampfer, M.J.; Han, J. Personal history of prostate cancer and increased risk of incident melanoma in the United States. J. Clin. Oncol. 2013, 31, 4394–4395. [Google Scholar] [CrossRef] [PubMed]
- Sergentanis, T.N.; Antoniadis, A.G.; Gogas, H.J.; Antonopoulos, C.N.; Adami, H.; Ekbom, A.; Petridou, E.T. Obesity and risk of malignant melanoma: A meta-analysis of cohort and case-control studies. Eur. J. Cancer 2013, 49, 642–657. [Google Scholar] [CrossRef] [PubMed]
- Rota, M.; Pasquali, E.; Bellocco, R.; Bagnardi, V.; Scotti, L.; Islami, F.; Negri, E.; Boffetta, P.; Pelucchi, C.; Corrao, G.; et al. Alcohol drinking and cutaneous melanoma risk—A systematic review and dose-risk meta-analysis. Br. J. Dermatol. 2014, 170, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Olsen, C.M.; Carroll, H.J.; Whiteman, D.C. Estimating the attributable fraction for melanoma: A meta-analysis of pigmentary characteristics and freckling. Int. J. Cancer 2010, 127, 2430–2445. [Google Scholar] [CrossRef] [PubMed]
- Dahlke, E.; Murray, C.A.; Kitchen, J.; Chan, A.W. Systematic review of melanoma incidence and prognosis in solid organ transplant recipients. Transpl. Res. 2014. [Google Scholar] [CrossRef]
- Dinh, Q.Q.; Chong, A.H. Melanoma in organ transplant recipients: The old enemy finds a new battleground. Australas. J. Dermatol. 2007, 48, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Penn, I. Malignant melanoma in organ allograft recipients. Transplantation 1996, 61, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Bosland, M.C. The role of steroid hormones in prostate carcinogenesis (Chapter 2). J. Natl. Cancer Inst. Monogr. 2000, 27, 39–66. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, P.L.; Je, Y.; Schutz, F.A.; Hoffman, K.E.; Hu, J.C.; Parekh, A.; Beckman, J.A.; Choueiri, T.K. Association of androgen deprivation therapy with cardiovascular death in patients with prostate cancer: A meta-analysis of randomized trials. JAMA 2011, 306, 2359–2366. [Google Scholar] [CrossRef] [PubMed]
- Hyde, Z.; Flicker, L.; McCaul, K.A.; Almeida, O.P.; Hankey, G.J.; Chubb, S.A.P.; Yeap, B.B. Associations between testosterone levels and incident prostate, lung, and colorectal cancer: A population based study. Cancer Epidemiol. Biomark. Prev. 2012, 21, 1319–1329. [Google Scholar] [CrossRef]
- Gann, P.H.; Hennekens, C.H.; Ma, J.; Longcope, C.; Stampfer, M.J. Prospective study of sex hormone levels and risk of prostate cancer. J. Natl. Cancer Inst. 1996, 88, 1118–1126. [Google Scholar] [CrossRef] [PubMed]
- Sutcliffe, S.; Giovannucci, E.; Isaacs, W.B.; Willett, W.C.; Platz, E.A. Acne and risk of prostate cancer. Int. J. Cancer 2007, 121, 2688–2692. [Google Scholar] [CrossRef] [PubMed]
- Cohen, P.R. Melanoma of non-sun exposed skin in a man with previous prostate cancer: Recognition of a recently confirmed association. Dermatol. Ther. (Heidelb) 2014, 4, 125–129. [Google Scholar] [CrossRef]
- Rampen, F.H.; Mulder, J.H. Malignant melanoma: An androgen-dependent tumour? Lancet 1980, 1, 562–564. [Google Scholar] [CrossRef] [PubMed]
- Slominski, A.; Tbin, D.J.; Shibahara, S.; Wortsman, J. Melanin pigmentation in mammalian skin and its hormonal regulation. Physiol. Rev. 2004, 84, 1155–1228. [Google Scholar] [CrossRef] [PubMed]
- Allil, P.A.; Visconti, M.A.; Castrucci, A.M.; Isoldi, M.C. Photoperiod and testosterone modulate growth and melanogenesis of S91 murine melanoma. Med. Chem. 2008, 4, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Richardson, M.; Reddy, V.; Menon, M.; Barrack, E.R.; Reddy, G.P.; Kim, S. Structural and functional association of androgen receptor with telomeres in prostate cancer cells. Aging 2013, 5, 3–17. [Google Scholar] [PubMed]
- Kim, S.H.; Richardson, M.; Chinnakannu, K.; Bai, V.U.; Menon, M.; Barrack, E.R.; Reddy, G.P. Androgen receptor interacts with telomeric proteins in prostate cancer cells. J. Biol. Chem. 2010, 285, 10472–10476. [Google Scholar] [CrossRef] [PubMed]
- Nan, H.; Du, M.; de Vivo, I.; Manson, J.E.; Liu, S.; McTiernan, A.; Curb, J.D.; Lessin, L.S.; Bonner, M.R.; Guo, Q.; et al. Shorter telomeres associate with a reduced risk of melanoma development. Cancer Res. 2011, 71, 6758–6763. [Google Scholar] [CrossRef] [PubMed]
- Hsueh, E.C.; Gupta, R.K.; Lefor, A.; Reyzin, G.; Ye, W.; Morton, D.L. Androgen blockade enhances response to melanoma vaccine. J. Surg. Res. 2003, 110, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Lenth, R.V. Java Applets for Power and Sample Size (Computer Software). Available online: http://www.stat.uiowa.edu/~rlenth/Power (accessed on 4 February 2015).
- Fitzpatrick, T.B. Soleil et peau (Sun and skin). J. Méd. Esthét. 1975, 2, 33–34. (in French). [Google Scholar]
- Balch, C.M.; Soong, S.J.; Gershenwald, J.E.; Thompson, J.F.; Reintgen, D.S.; Cascinelli, N.; Urist, M.; McMasters, K.M.; Ross, M.I.; Kirkwood, J.M.; et al. Prognostic factors analysis of 17,600 melanoma patients: Validation of the American Joint Committee on Cancer melanoma staging system. J. Clin. Oncol. 2001, 19, 3622–3634. [Google Scholar] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goldenberg, A.; Jiang, S.I.B.; Cohen, P.R. A Possible Association between Melanoma and Prostate Cancer. Results from a Case-Control-Study. Cancers 2015, 7, 670-678. https://doi.org/10.3390/cancers7020670
Goldenberg A, Jiang SIB, Cohen PR. A Possible Association between Melanoma and Prostate Cancer. Results from a Case-Control-Study. Cancers. 2015; 7(2):670-678. https://doi.org/10.3390/cancers7020670
Chicago/Turabian StyleGoldenberg, Alina, Shang I. Brian Jiang, and Philip R. Cohen. 2015. "A Possible Association between Melanoma and Prostate Cancer. Results from a Case-Control-Study" Cancers 7, no. 2: 670-678. https://doi.org/10.3390/cancers7020670